Embed Size (px)
Citation preview

[CANCER RESEARCH 37, 2348-2353, July 1977]
electrolytes. This relationship forms the basis of specificnutritional therapies to combat the changes in basic bodynutrients that influence carcinogenesis.
Electrolytes and Minerals
Thus far, no abnormalities in electrolyte and mineral metabolism of tumors or host can be generalized to all types ofcancer. Therefore specific anomalies will be reported whenthey exist, but we emphasize cautious interpretation ofthese preliminary data.
Sodium and Potassium. Hypokalemia often accompaniesmucin-secreting , potassium-losing adenocarcinomas of thecolon. Weight loss and catabolism also result in potassiumand sodium losses in the urine (33). As the lean body massis restored, potassium requirements increase; a rise in thetotal body potassium is an excellent indicator of an anabolicstate (33, 40). Other alterations in potassium metabolismare noted as an indirect effect of tumors causing hypoglycemia, namely, insulinomas and retroperitoneal tumors.
The effects of cancer on sodium metabolism are nonspecific. Alterations are an indirect effect such as those observed in oat-cell carcinomas of the lung and hypothalamictumors, both of which result in inappropriate antidiuretichormone secretion, water retention, and hyponatremia.Tumors that produce adrenocorticotropic hormone also resuit in water and electrolyte abnormalities.
Calcium. Changes in calcium metabolism are secondaryto hormonal changes or are a consequence of bone destruction. Hypercalcemia is associated with parathyroid tumors, cancer metastatic to bone with primaries in the breastand thyroid, and with multiple endocrine adenomatosis.Hypocalcemia occurs as a sequela of malnutrition and isassociated with hypoalbuminemia.
Magnesium. The role of magnesium in cancer is obscure.The regression of malignant tumors with hypomagnesemiaand hypokalemia secondary to long-term dialysis in renalfailure has been observed (38). The association remainsoccult. Breast cancer specimens have contained high levelsof magnesium, the significance of which is not known (42).
Iron. Sideropenic anemia with visceral lesions, e.g., brittie nails, koilonychia, glossitis, papillary atrophy of thetongue, oral fissures, a small mouth with narrow lips, asmooth facial skin, atrophic gastritis, achlorhydria, andpostcricoid dysphagia as seen in the Plummer-Vinson syndrome, is causally related to iron deficiency. The incidenceof hypopharyngeal cancer in women in northern Sweden isinfluenced by the presence of Plummer-Vinson syndrome;
Summary
The metabolic relationships between electrolytes, mmerals, and cancer show no general abnormalities. Specificdisorders of metabolism may be produced by hormonesecreting tumors, and an increased utilization or excretionof minerals and electrolytes may result. Patients with cance.r
@ndmalnutrition lose significant amounts of nitrogen and4at. The attrition of visceral protein represents the mostclinically significant tissue loss. The resulting nutritionalconditions of marasmus and kwashiorkor account in partfor the marked impairment of cell-mediated immunity. Basalenergy expenditure in patients is not inordinately high, nordo different tumor groups need classification according toenergy expenditure in the patients. Patients require an intake of 30 to 35 kcal/kg to meet their energy requirements.Protein intake, the most important factor in effecting weightgain, is effective when 1.5 to 2.0 g/kg are supplied daily.This represents about 16 to 20% of the total energy expenditure.
Forced feeding programs, e.g. , total parenteral nutritionor enteral hyperalimentation, are often required to overcome anorexia. Response to therapy takes several weeks. Apositive or successful response includes the closure of fistulae, completion of radiotherapy or chemotherapy, recovery from anorexia or stomatitis, a subjective feeling of wellbeing, and an improvement in the quality of life. Failure torespond by these objective criteria is associated with a poorprognosis in the experience of the nutrition support service.
Introduction
In the past few years medicine has made significant advances in understanding the pathogenesis of cancer. Alongwith a more complete picture of tumor metabolism hascome a greater therapeutic sophistication; surgery, radiotherapy, chemotherapy, and immunotherapy give the pa
4 tient a better prognosis. Recently, the nutritional aspects of
cancer metabolism and therapy have been appreciated,stimulating new research in this direction. The purpose ofthis paper is to present the relationship between cancer andthe basic body nutrients including nitrogen, minerals, and
I Presented at the Conference on Nutrition and Cancer Therapy, Novem
bar 29 to December 1, 1976, Key Biscayne, Fla. Supported in part by NIHResearch Grant GM22691. Data analysis was performed on PROPHET andwas sponsored by the Chemical/Biological Information Handling Program ofthe Division of Research Resources, NIH (RR-76). This is Paper 586 fromthe Cancer Research Institute of the New England Deaconess Hospital.
2 Presenter. To whom requests for reprints should be addressed.
2348 CANCERRESEARCHVOL. 37
The Effect of Cancer on Nitrogen, Electrolyte, and MineralMetabolism1
George L. Blackburn,2Baltej S. Maini, BruceR. Bistrian,and WilliamV. McDermott,Jr.Nutrition/Metabolic Laboratory, Cancer Research Institute, New England Deaconess Hospital/Harvard Medical School, Boston, and Sidney Farber CancerInstitute, Boston, Massachusetts 02215
on April 25, 2019. © 1977 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from
Daily mineral requirements(parenteraluse)MineralDose/dayaSodium60-80
mEqPotassium60-100mEqMagnesium8-16mEqCalcium9-18mEqPhosphorus25-35mMIron1Zinc2Manganese0.4Copper1Chromium10
@gCobalt(asVitamin B12)[email protected]
Dose in mg unless otherwise noted.
I. Improvedmetabohcfunctiona immunestatus
@ plasmaproteins2.Improvedworkperformance3. Improvedqualityof life4. Improved response to therapy
Chart 1. Interrelationships of cancer and nutrition.
Nitrogen , Electro!ytes, and Minerals in Cancer
both these conditions have decreased in prevalence sincenutritional repletion , specifically including iron , becamewidespread (28). Also, in areas of the world where irondeficiency is common, the incidence of gastric carcinoma is5 times as common as that in the United States; othervariables may play a role (52). Vitale (53) has pointed out theinteraction between immunodeficiency and iron depletion;the relationship between immunodeficient mechanisms iniron deficiency and carcinogenesis remains as an interesting area of research.
Trace Minerals. Numerous suggestions have been advanced and studies carried out regarding the role traceminerals might play in cancer metabolism (2, 15, 18). Ofinterest is the postulation that mineral deficiency may activate certain procarcinogens and thereby influence oncogenesis (53). Elevated zinc levels have been observed in bronchogenic and colonic cancer. In contrast, lowering of zinclevels is seen in a variety of infective and other diseasestates (35, 51).
Extensive studies investigating the role of copper in cancer have been carried out (25, 34). Copper levels are elevated in Hodgkin's disease; a fall was noted in patients whoresponded to therapy (24). Copper levels have been foundto be elevated in several types of tumors, and the significance is at present unknown. Correlation of nickel levelswith oral cancer, arsenic with laryngeal carcinoma, andlead with leukemia, lymphomas, and ovarian cancer hasbeen attempted in order to define the role of these tracemetals in oncogenesis and diagnosis (2, 35). An excellentreview of this subject has been provided by Schwartz (43).
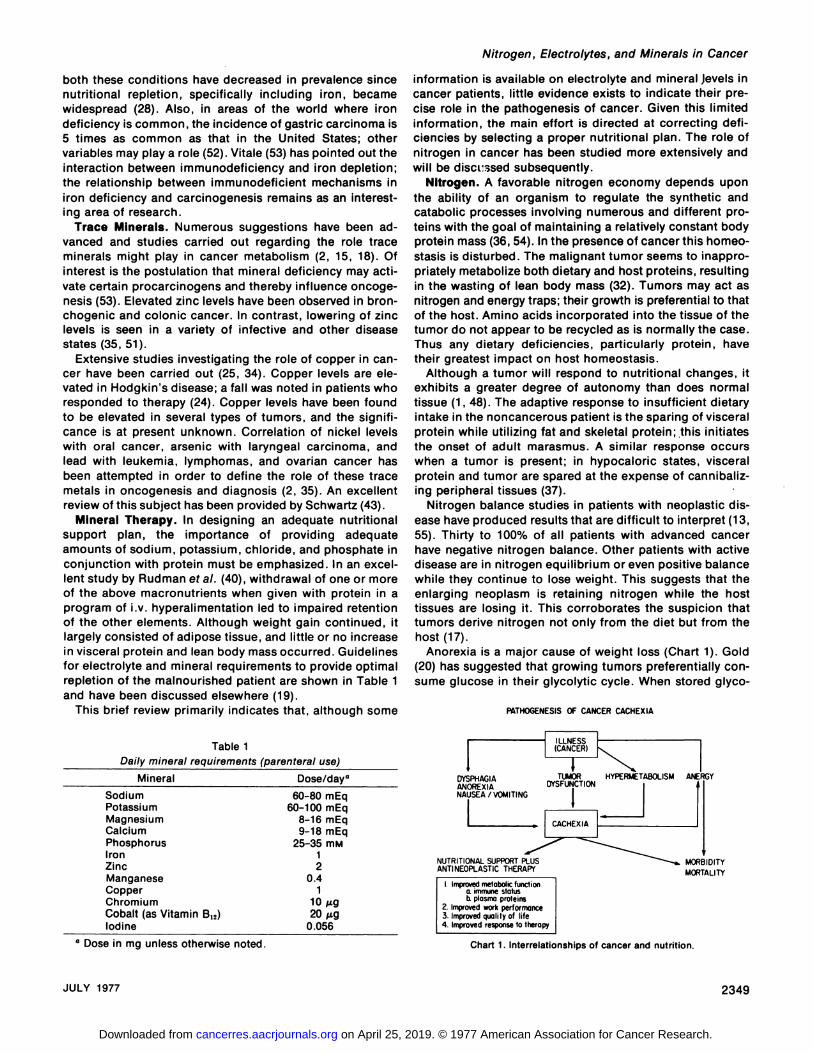
Mineral Therapy. In designing an adequate nutritionalsupport plan, the importance of providing adequateamounts of sodium, potassium, chloride, and phosphate inconjunction with protein must be emphasized. In an excellent study by Rudman et a!. (40), withdrawal of one or moreof the above macronutrients when given with protein in aprogram of i.v. hyperalimentation led to impaired retentionof the other elements. Although weight gain continued, itlargely consisted of adipose tissue, and little or no increasein visceral protein and lean body mass occurred. Guidelinesfor electrolyte and mineral requirements to provide optimalrepletion of the malnourished patient are shown in Table 1and have been discussed elsewhere (19).
This brief review primarily indicates that, although some
information is available on electrolyte and mineral Jevels incancer patients, little evidence exists to indicate their precise role in the pathogenesis of cancer. Given this limitedinformation, the main effort is directed at correcting deficiencies by selecting a proper nutritional plan. The role ofnitrogen in cancer has been studied more extensively andwill be discussed subsequently.
Nitrogen. A favorable nitrogen economy depends uponthe ability of an organism to regulate the synthetic andcatabolic processes involving numerous and different proteins with the goal of maintaining a relatively constant bodyprotein mass (36, 54). In the presence of cancer this homeostasis is disturbed. The malignant tumor seems to inappropriately metabolize both dietary and host proteins, resultingin the wasting of lean body mass (32). Tumors may act asnitrogen and energy traps; their growth is preferential to thatof the host. Amino acids incorporated into the tissue of thetumor do not appear to be recycled as is normally the case.Thus any dietary deficiencies, particularly protein, havetheir greatest impact on host homeostasis.
Although a tumor will respond to nutritional changes, itexhibits a greater degree of autonomy than does normaltissue (1, 48). The adaptive response to insufficient dietaryintake in the noncancerous patient is the sparing of visceralprotein while utilizing fat and skeletal protein;.this initiatesthe onset of adult marasmus. A similar response occurswhen a tumor is present; in hypocaloric states, visceralprotein and tumor are spared at the expense of cannibalizing peripheral tissues (37).
Nitrogen balance studies in patients with neoplastic disease have produced results that are difficult to interpret (13,55). Thirty to 100% of all patients with advanced cancerhave negative nitrogen balance. Other patients with activedisease are in nitrogen equilibrium or even positive balancewhile they continue to lose weight. This suggests that theenlarging neoplasm is retaining nitrogen while the hosttissues are losing it. This corroborates the suspicion thattumors derive nitrogen not only from the diet but from thehost (17).
Anorexia is a major cause of weight loss (Chart 1). Gold(20) has suggested that growing tumors preferentially consume glucose in their glycolytic cycle. When stored glyco
PATHOGENESISOFCANCERCACHEXIA
Table 1
JULY 1977 2349
ILLNESSI@ (CANCER)1N@TUMOR HYPERMETABOLISMANERGYDYSPHAGIA
I PPORT@'@M
ANOREXIA DYSFUNCTIONNAUSEA/VOMITING
NUTRITIONALSU MORBIDITYANTINEOPLASTICTHERA@ MORTALITY
on April 25, 2019. © 1977 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from

PARENTERALENTERALHOMEDIScHARGED@!DISCHARGEDDISCHARGEDII301310010210142222II0008410I6310II000I38000
6336—9162 48—745732—781315
941—186414201167—17011375970—168518±620±726±66.2
0—1714 10—23
G. L. Blackburn et al.
gen and dietary carbohydrate cannot meet this requirement, a considerable loss of amino acid would occur forgluconeogenesis to provide fuel for this low-energy-yieldinganaerobic cycle. Weight loss has been correlated tohigh Con cycle activity (23); the extra energy expended isbut a small fraction of the total energy expenditure. Thistumor metabolism cannot account for the observed weightloss and malnutrition. Clearly, the important factor is toovercome anorexia by providing an adequate diet of proteinand calories.
NUTRITIONALSUPPORTOFCANCERPATIENTS
171A&W&@JP.•_____ _____Neckendmoo'
Esophoqus
Lymphosorco@rto
Lurtq8,'ecsi
6U/8/odderPoncrecs/81//cry
Uterus/Cervix
Co/ce—Rectc/
TOTAL• 27 22 8 2 7Diet
The 3 energy-containing dietary components are carbohydrate, fat, and amino acids. The 1st 2 provide nonproteinenergy. The latter is necessary if there is to be protein synthesis. Three hundred to 400 g of body protein are brokendown each day. The reutilization rate of amino acids available from the normal degradation of body protein is between70 and 80%. Those tissues in which turnover rates are high(e.g., gut and liver) are at a greater advantage whencompeting for a limited amount of amino acid compared tothe less labile proteins (7). Given the limited repair of bodycell mass (150 g/day), this process takes considerable timeto produce significant changes.
Hyperalimentation, whether it is provided enterally orparenterally, can replete most malnourished cancer patients,given adequate time. We recently studied 66 adult patientswith advanced solid tumors who were referred to the Nutrition Support Service at the New England Deaconess Hospital (8). The purpose of the study was to categorize thenature and degree of malnutrition, formulate an optimalnutritional therapy plan for each patient, and to identify thefactors preventing an adequate response to both cancerand nutritional therapy (31, 44, 48).
Patient Assessment. The patients were classified according to a number of criteria. Tumor types are listed inChart 2. The basal energy expenditure was calculated usingthe Harris-Benedict formula which takes into account age,sex, height, and weight (41). Anthropometric measurements which included triceps skinfold (an estimator of fatreserves), arm muscle circumference, and creatinine/height ratio (independent estimators of body cell mass)were recorded (4). Serum transferrin and albumin levels aswell as total lymphocyte counts were used to assess visceralproteinfunction(3,4,6).Immunological statuswas evaluated by delayed hypersensitivity skin testing with Candida,streptokinase-streptodornase, and mumps antigens (5, 29,46).
A wide variety of tumors were present. All patients hadlost at least 10% of their usual weight. Chart 2 shows thedegree of weight loss. In addition, no significant hypermetabolism was present, and nitrogen loss could not be categorized according to tumor type. These patients were seenat all phases of their cancer treatment programs, whethersurgery, chemotherapy, or radiotherapy. These observations suggest that some generalizations and nutritionalguidelines for protein and calorie therapy are possible.
Using these aforementioned techniques of nutritional as
AGE MecnRcnge
BEE.mon/itinqe
x WeightLoss
WEIGHT64/N Macn@c@@nqe
Chart 2. Patient distribution in various tumor groups. Basal energy cxpenditure (BEE) calculated on the basis of height, weight, age, and sex. GU,genitourinary.
sessment, an objective classification of malnutrition can bemade. Chart 3 characterizes these patients according to keynutritional criteria. Substantial losses of fat mass were observed; fewer than 25% of the patients had a normal tricepsskinfold (12.5 mm). Deficits in lean body mass were considerable, although not as widespread as adipose tissue loss.The most physiologically significant tissue losses were fromthe viscera, indicated by the low albumin, transferrin, andtotal lymphocyte count, a finding seen in advanced states ofmalnutrition. A combined marasmus and kwashiorkor-likesyndrome characterizes this population (3). Poor visceralfunction, the most serious consequence of protein-caloriemalnutrition, is accompanied by the marked impairment ofcell-mediated immunity as demonstrated by the measurement of delayed hypersensitivity skin tests (Table 2; Refs. 5,45,and 46).
Biochemical Assessment. A record of blood sugar, ureanitrogen , creatinine, sodium , potassium , chloride, bicarbonate, and magnesium was kept. Liver function tests wereperformed weekly; this included albumin and transferrin.Complete blood counts were done daily, and lymphocytelevels were checked weekly. Cultures were done when necessary, and clinical charts recording weight, subjective responses to therapy, and significant events were maintained.Forty-eight-hr nitrogen balance studies were performedweekly, and skin testing was done at 3-week intervals.
The criteria for a successful response to therapy were: (a)completion of oncological therapy, (b) weight gain, (C)discharge from hospital, (d) improvements in visceral proteinstatus parameters , (e) preservation or restoration of mmU-nological response as measured by skin testing, (f) subjective improvements in symptoms, and (g) closure of fistulae.
All patients were followed closely by the members of theNutrition Support Service. This team consists of a thera
2350 CANCERRESEARCHVOL. 37
on April 25, 2019. © 1977 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from

Control patientsCancerpatientsCandidaSKSD@CandidaSKSD(mm)(mm)(mm)(mm)05b000150011121044100818035165100103000847051610101256010Mean
7.416.53.85.5
Nitrogen, Electrolytes, and Minerals in Cancer
tam anabolism and positive nitrogen balance was (1.7 xbasal energy expenditure) for i.v. hyperalimentation and(1.54 x basal energy expenditure) for enteral hyperalimentation (9, 21). The difference in these 2 groups is dueto the continuous infusion of hypertonic glucose in theparenteral case, which results in an obligate conversion ofsome of the administered glucose to fat (30. 41).
Responseto NutritionalTherapy
Chart 4 shows the responses to the different types ofnutritional therapy in surviving patients. Due to the underweight and marasmic nature of these patients, weight gainwas an important indicator of a positive response to therapy. The most significant changes during the 1st 3 weeks oftherapy appeared in the visceral compartment. Perhaps themost important result was that an average of 3.5 weeks wasrequired before a positive response demonstrated itself. No@changes were seen in the 1st week of therapy. Given thatlength of therapy, patients gained an average of 6.2 pounds,with a range of no weight change up to +17. There were nodifferences in results between the enteral and parenteralgroups; the responses to anorexia, dysphagia, stomatitis,and weight loss were similar.
Successful surgery occurred in 3 of 12 patients wherefistulae closed despite tumor in the anastomotic line. Response to chemotherapy was poor (40%) owing to the advanced nature of the disease. Radiotherapy was more successful, particularly when compared to a 25% positive response in nonhyperalimented patients requiring 4000 rads(11). Patients receiving total parenteral nutrition were in anadvanced stage of illness as reflected by a higher mortalityrate. Two episodes of catheter-related sepsis occurred inthe series, necessitating the removal of the catheter. Nofurther septic problem developed, but both patients hadadvanced cancer, were anergic, and soon succumbed totumor-related problems.
. SKIN-FOLD
@ THICKNESSARM-MUSCLE.@ - TOTAL
CIRCUMFERENCEALBUMIN TRANSFERIN@ LYMPHOCYTEL COUNT
100
@ 80
I..‘ 60
@>or@ @Q%% @A>ar.to75%but<90% •>ar'Ia6O%but<75%
S •S of Standard
Chart 3. Nutritional characterization emphasizes the physiologically significant loss of visceral protein (transferrin and total lymphocyte count) inpatients with loss of 15 to 25% of body weight.
Table2
Delayedhypersensitivityskin testing
a SKSD, streptokinase-streptodornase.
b p < 0.005 (x2 test) for number of positive skin tests.
peutic dietitian, a hyperalimentation nurse, a pharmacist,and a psychologist. Ambulatory patients were maintainedon nutritional support (enteral) at home. These 7 patientswere followed closely through weekly visits to the nutritionclinic.
On the basis of their nutritional profile, a nutritional support plan was designed for each patient. The type of nutritional therapy was dictated by the severity of malnutritionand the presence of a functional gastrointestinal tract.When enteral hyperalimentation was indicated, a continuous drip through a mercury-tipped Silastic tube (KeofeedStomach Tube; Hedeco, Palo Alto, Calif.) was used. Definedformula diets (Precision LR®,Doyle Pharmaceutical, Mmneapolis, Minn.; Vivonex HN®,Eaton Laboratories, Norwich, N. V.; Isocal®,Mead Johnson & Co., Evansville, md.;and Ensure®, Ross Laboratories, Columbus, Ohio) weresupplemented with protein (SCM®, Control Drug, PortReading, N. J.) or calories (Polycose®, Ross Laboratories;medium-chain triglyceride caloric supplement, Eaton Laboratories), as necessary. Hyperalimentation i.v. (25% dextrose and 4.25% Fre-Amine; McGaw Laboratories, Irvine,Calif.) was carried out under standard guidelines. Tracemineral supplements were provided as shown in Table 1.The exact amount of calories and protein delivered to ob
@E/6HTGA/N LYMPHOCYTESI:, (@) @7L 2000
0@ .@ 1600
:@•@ 0 1 0 @!O
ALBUM/NLEVELS SERUMTRANSFERRIN40@@ 1mg/lOCal) 265
32 . 245
:L@@@
WEEKS
Chart 4. Response to nutritional support in surviving patients. Significant(p < 0.05) results except for albumin occurred by the 2nd to 3rd week oftherapy.
JULY 1977 2351
on April 25, 2019. © 1977 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from

G. L. Blackburn et al.
Caloric requirements confirmed the fact that energy expenditures were similar to those observed in patients undergoing elective surgery (41). Optimal nutritional supportbased on nitrogen balance showed caloric intake requirements to be 130 to 150% of basal energy expenditure inenterally fed patients and 175% of that in parenterally fedpatients (4, 21). After meeting the caloric requirements,weight gain is largely dependent upon the level of proteinintake. The best results in terms of weight gain occurredwhen an intake of 90 to 100 g of protein (1.5 to 2.0 g/kg/day)accompanied a caloric intake of 40 to 45 kcal/kg/day.
NitrogenMetabolisminCancer
Cheraskin (11) studied the effect of diet on the responseof cervical carcinoma to [email protected] this randomized studyinvolving54 patients,a high-protein,low-refinedcarbohydrate diet was compared to standard nutritional support.Radiation response was significantly higher in those sustamed by the high-proteindiet.In addition,the radiationresponse of the control group was progressively worse withmore advanced stages of uterine cancer, whereas the highprotein group continued to respond favorably. Jewell andHunter (27) noted depleted protein pools and net catabolism of labile and stable protein. These conditions presumably favor tumor growth by making amino acids and energyavailable in abundance to the tumor. The studies by Jewelland Hunter regarding the growth of 150-g female rats demonstrated accelerated rates of albumin catabolism and decreased levels of serum albumin. High-protein diets improved albumin synthesis, although net catabolism persisted. Thus tumor and visceral protein, which have higherrates of protein turnover and higher metabolic rates at rest,survive longer or in preference to muscle. In cancer (37) orin mild trauma (10), normal liver protein function and weightare maintained. Only the secretory proteins of the liveralbumin, transferrin, lipoproteins become depleted. Forthese proteins there is a lower priority for synthesis whencompared to structural proteins and enzymes competing foravailable amino acid substrates. After the depletion of muscle protein, the patient progresses to the advanced stagesof marasmus, and the loss of visceral protein and immunecompetence becomes more obvious.
In injury, a loss of skeletal muscle protein is a physiological response to injury, favoring the mobilization of labileprotein pools to support visceral protein synthesis (10). Thisresponse, primarily sympathetic mediated, is communicated in part by active polypeptides found in plasma duringinjury (12). Similarly, in cancer, tumors might produce orinitiate similar kinds of polypeptides that are responsible forthe protein depletion observed in advanced cancer patients.Theologides (50) has proposed that cancer produces lowmolecular metabolites which render host metabolism chaotic by affecting important allosteric transitions, activations, and inactivation of control mechanisms in varioustissues.
In small animal tumors, the glycolytic rate and Con cycleactivity have been measured in a “fed―group, a “fasted―group, and a “fastedplus protein―group. The fasted ani
mals exhibit a decreased tumor growth with a parallel dedine in body growth. This correlation demonstrates thesimilar effect of fasting on generalized host and tumormetabolism. The modification of fasting by protein resultsin tumor growth as well as preservation of animal growth(48).
Regardless of the mechanism, protein-calorie malnutrition does develop in a large number of cancer patients (14).The degree of imbalance between synthesis and catabolismis dependent upon: (a) extent of nutritional depletion, (b)total body protein mass, (c) rate of protein turnover, and (d)alterations produced by cancer tissue.
Terepka and Waterhouse (49) have questioned the beneficial effects of forced feeding . Although effective over theshort term, these therapies could not be maintained forprolonged periods of time. Feedings p.o. lasted 10 days andresulted in positive nitrogen balance accompanied by theretention of phosphate, calcium, sodium, and chloride. Inthe postsupplemental period , however, these returned toequilibrium and finally became negative. Although the patients were encouraged by their weight gain, only 1 patientcontinued his effort successfully after the study. Nutritionsupport programs should and must be continued on anoutpatient basis in order that the patients can be maintainedin the “fed―state. Frequent monitoring and counseling, inaddition to individual alteration in feeding regimens to caterto changing behavior patterns and taste sensations, areessential.
Immunological alteration has been established as animportant mechanism in the pathogenesis of cancer(39). Lymphocytic activity and reactivity to skin antigenscorrelate well with prognosis and response to therapy inleukemia (22), Hodgkin's disease (47), lung cancer (26), andother tumors (16). It is well known that, in children andadults, the nutritional status can influence immunologicalactivity (29, 45). This can be reversed by adequate nutritional replenishment (17). This method remains an important parameter of measuring visceral protein status; all patients who failed to respond to nutritional support wereanergic and subsequently died in hospital (24 of 66 patients).
There is inadequate evidence that specific deficiencies ofelectrolytes and minerals exist in cancer. However, deficiences are part of the total picture of malnutrition, and allnutrients including trace minerals must be administered toproduce an optimal utilization and retention. The currentstatus of nitrogen, electrolyte, and mineral therapy dictatesnutrition prescriptions to contain a nitrogen/calorie ratio of1/150 with 2000 to 2500 kcal/day. With appropriate electrolyte and mineral intake, this therapy can, in 2 to 3 weeks,result in a positive objective response in the absence of anoverwhelming tumor burden. In this study, no evidence ofselective stimulation of tumor growth in any patient wasfound by any criteria available to us. The paralleled increased tumor cell mitosis produced by adequate nutritionmay be a desirable effect to maximize the efficacy of chemotherapeutic programs. In contrast, malnutrition-induceddepression of cell-mediated immunity can be expected tohave an adverse effect on cancer therapy. Optimal resultsoccurred with delivery of adequate nutrition as described
2352 CANCER RESEARCH VOL. 37
on April 25, 2019. © 1977 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from
Nitrogen, Electrolytes, and Minerals in Cancer
Cancer in Relation to the Results of Preoperative Tuberculin Skin Test.Biomed.,19:68-72,1973.
27. Jewell, W. R., and Hunter, L. The Effect of Adrenalectomy and HighProtein Diet on Tumor-altered Albumin Metabolism. Cancer Res., 31:257-259,1971.
28. Larsson, L-G., 5andstrom, A. , and Westling, P. Relationship of Plummer-Vinson Disease to Cancer of the Upper Alimentary Tract in Sweden.Cancer Res., 35: 3308-3316, 1975.
29. Law, D. K., Dudrick, S. J., and Abdou, N. I. Immunocompetence ofPatients with Protein-Calorie Malnutrition. Ann. Internal Med. , 79: 545-550, 1973.
30. Maini, B., Blackburn, G. L., Bistrian, B. R., Flatt, J. P., Page, J. G.,Bothe, A., Benotti, P., and Rienhoff, H. V. Cyclic Hyperalimentation: AnOptimal Technique for Preservation of Visceral Protein. J. Surg. Res.,20: 515-525,1976.
31. Meyer, J. A. Potentiation of Solid-Tumor Chemotherapy by MetabolicAlteration. Ann. Surg., 179: 88-93, 1974.
32. Mider, G. B. Some Aspects of Nitrogen and Energy Metabolism inCancerous Subjects: A Review. Cancer Res., 11: 821-829, 1951.
33. Moore, F. D. Metabolic Care of the Surgical Patient. Philadelphia: W. B.SaundersCo., 1959.
34. Mortazavi, S. H., Bani-Hashemi, A., Mozafari, M., and Raffi, A. Value ofSerum Copper Measurements in Lymphomas and Several Other Malignancies. Cancer, 29: 1193-1198, 1972.
35. Mulay, I. L., Roy, R., Knox, B. E., Suhr, M. H., Delaney, W. E.Trace MetalAnalysis of Cancerous and Non-cancerous Human Tissues. J. NatI. Cancer Inst., 47: 1-13, 1971.
36. Munro, H. N. Regulation Mechanisms in Protein Metabolism. In: H. N.Munro (ed), Mammalian Protein Metabolism, Vol. 4, pp. 3-108. NewYork: Academic Press, Inc., 1970.
37. Munro, H. N. A General Survey of Pathological Changes in ProteinMetabolism. In: H. N. Munro and J. B. Allison (eds.), Mammalian ProteinMetabolism, Vol. 2, pp. 267-311. New York: Academic Press, Inc., 1964.
38. Parsons, F. M., Edwards, G. F., Anderson, C. K., Ahmad, S., Clark, P. B.,Hetherington, C., and Young, G. A. Regression of Malignant Tumors inMagnesium and Potassium Depletion Induced by Diet and Hemodialysis.Lancet, 1: 243-244, 1974.
39. Reif, A. E. (ed.) Immunity and Cancer in Man. New York: Marcel Dekker,Inc., 1975.
40. Rudman, D., Millikan, W. J. , Richardson, T. J. , Bixler, T. J. II, Stackhouse, W. J. , and McGarrity, W. C. Elemental Balances during lntravenous Hyperalimentation of Underweight Adult Subjects. J. Clin. Invest.,55: 94-104, 1975.
41. Rutten, P., Blackburn, G. L., Flatt, J. P., Hailowell, E., and Cochran, D.Determination of Optimal Hyperalimentation Infusion Rate. J. Surg.Res.,18:477-483,1975.
42. Santoliquido, P. M., Southwick, H. W., and Olwin, J. H. Trace MetalLevels in Cancer of the Breast. Surg. Gynecol. Obstet., 142: 65-70, 1976.
43. Schwartz, M. K. Role of Trace Elements in Cancer. Cancer Res. , 35:3481-3487, 1975.
44. Schwartz, G. F. , Green, H. L. , Bendon, M. L. , Graham, W. P. Ill, and
Blakemore, W. S. Combined Parenteral Hyperalimentation and Chemotherapy in the Treatment of Disseminated Solid Tumors. Am. J. Surg.,121:169-173,1971.
45. Smythe, P., Schonland, M.. Brereton-Stiles, G., Coovadia, H. M., Grace,H., Loening, W. E. K., Parent, M. A., and Vos, G. H. ThymolymphaticDeficiency and Depression of Cell-mediated Immunity in Protein CalorieMalnutrition. Lancet, 2: 939—944,1971.
46. Sokal, J. E. Measurement of Delayed Skin-Test Responses. New EngI. J.Med.,293:501-503,1975.
47. Sokal, J. E., and Aungst, C. W. Response to BCG vaccination andSurvival in Advanced Hodgkin's Disease. Cancer, 24: 128-134, 1969.
48. Steiger, E., Oram-Smith, J., Miller, E., Kuo, L., and vars, H. Effects ofNutrition on Tumor Growth and Tolerance to Chemotherapy. J. Surg.Res.,18:455-461,1975.
49. Terepka, A. R., and Waterhouse, C. Metabolic Observations during theForced Feeding of Patients with Cancer. Am.J. Med., 20: 225-238, 1956.
50. Theologldes, A. Pathogenesis of Cachexia in Cancer. Cancer, 29: 484-488,1972.
51. Varsieck, J., Barbier, F., Speecko, A., and Hoste, J. Manganese, Copperand zinc Concentrations in Serum and Packed Blood Cells During AcuteHepatitis, Chronic Hepatitis and Post-hepatitic Cirrhosis. Clin. Chem.,20: 1141-1145,1974.
52. Vitale, J. J. Deficiency Diseases. In: 5. L. Robbins (ed.), Pathologic Basisof Disease, Ed. 1, pp. 475-508. Philadelphia: W. B. Saunders Co., 1974.
53. Vitale, J. J. Possible Role of Nutrients In Neoplasia. Cancer Res. , 35:3320-3325, 1975.
.54. Wannemacher, R. W., Jr. Protein Metabolism. In: H. Ghadimi (ed.),Total Parenteral Nutrition: Premises and Promises, pp. 85-107. NewYork: John Wiley and Sons, 1975.
55. Watkin, D. M. Nitrogen Balance as Affected by Neoplastic Disease and ItsTherapy. Am. J. Clin. Nutr., 9: 446-460, 1961.
JULY 1977 2353
herein. The delivery of a high concentration of nutrientsthrough forced feeding programs, either by the gastrointestinal tract or by total parenteral nutrition, results in improved organ function.
References1. Amino Acid Manipulation in Cancer. Lancet, 1: 303-304, 1973.2. Berg, J. W., and Burbank, F. Correlations between Carcinogenic Trace
Metals in Water Supplies and Cancer Mortality. Ann N. Y. Acad. Sci.,199: 249-264, 1972.
3. Bistrian, B. R., Blackburn, G. L., Hallowell, E., and Heddle, R. ProteinStatus of General Surgical Patients. J. Am. Med. Assoc., 230: 858-860,1974.
4. Bistrian, B. R., Blackburn, G. L., Sherman, M., and Scrimshaw, N. S.Therapeutic Index of Nutritional Depletion in Hospitalized Patients.Surg. Gynecol. Obstet., 141: 512-516, 1975.
5. Bistrian, B. R., Blackburn, G. L. , Scrimshaw, N. S., and Flatt, J. P.Cellular Immunity in Semi-Starved States in Hospitalized Adults. Am. J.Clin. Nutr., 28: 1148-1155, 1975.
6. Bistrian, B. R., Blackburn, G. L., Vitale, J. J. , Cochran, D. , and Naylor, J.Prevalence of Malnutrition in General Medical Patients. J. Am. Med.Assoc., 235: 1567-1570, 1976.
7. Blackburn, G. L. Nitrogen Metabolism after Surgical Trauma. Physiologyin Medicine. New EngI. J. Med., in press.
8. Blackburn, G. L., and Bistrian, B. A. Nutritional Counselling: Role of aNutrition Support Service. In: H. Schneider (ed), Nutritional Support ofMedical Practice. Hagerstown, Md.: Harper and Row, in press.
9. Blackburn, G. L., and Bistrian, B. R. Protein Calorie Curative Therapy.In: H. Schneider (ed), Nutritional Support of Medical Practice. Hagerstown, Md.: Harper and Row, in press.
10. Blackburn, G. L., Flail, J. P., and Hensie, T. Peripheral Amino AcidInfusions. In: J. E. Fischer (ed), Total Parenteral Nutrition, pp. 363-394.Boston: Little, Brown and Co., 1976.
11. Cheraskin,E.,Ringsdorf,W. M.,Hutchins,K.,Setyaadmadja,A.T. S.H.,and Wideman, G. L. Effect of Diet upon Radiation Response in CervicalCarcinoma of the Uterus. Acta Cytol., 12: 433-438, 1968.
12. Clowes, G. H. A., Farrington, G. M., Zuschneid, W., Cossette, G. R., andSaravis, C. Circulation Factors in the Etiology of Pulmonary Insufficiencies and Right Heart Failure Accompanying Severe Sepsis (Peritonitis).Ann. Surg., 171: 663—678,1970.
13.Ce,T.,Kuo,N.H.,Chuachiaco,M.,Rosh,R.,andMulholland,J.H.Protein Nutrition in Cancer. Surg. Clin. North Am. 29: 449—472,1949.
14. Copeland, E. M., MacFayden, B. V., Lanzotti, V. J., and Dudrick, S. J.Nutritional Care of the Cancer Patient. In: C. E. Howe (ed), CancerPatient Care at M. D. Anderson Hospital and Tumor Institute. Chicago:Year Book Medical Publishers, 1976.
15. Dixon,J. R., Lowe,D. B., Richards,0. E.,Cralley,L. J., andStockinger,H. E. The Role of Trace Metals in Chemical Carcinogenesis. AsbestosCancers. Cancer Res., 30: 1068-1075, 1970.
16. Eiiber, E. R., and Morton, D. L. Impaired Immunologic Reactivity andRecurrence following Cancer Surgery. Cancer, 25: 362-367, 1970.
17. Fenninger, L. D., Waterhouse, C., and Keutmann, E. H. The Interrelationship of Nitrogen and Phosphorus in Patients with Certain NeoplasticDiseases. Cancer, 6: 930-941 , 1953.
18. Furst, A. Chelation and Cancer: A Speculative Review. In: M. J. Sevenand L. A. Johnson (eds.), Metal Binding in Medicine, pp. 336-343.Philadelphia: J. B. Lippincott Co., 1960.
19. Giovanoni, R. The Manufacturing Pharmacy Solutions and Incompatibilities. In: J. E. Fischer(ed.), Total Parenteral Nutrition, pp. 27-53. Boston:Little, Brown and Co. , 1976.
20. Gold, J. Proposed Treatment of Cancer by Inhibition of Gluconeogenesis. Oncology, 22: 185-207, 1968.
21. Hallowell, E., Sasvary, D., Bistrian, B. R., Soroff, H. S., and Blackburn,G. L. Factors Determining Optimal Nutritional Support in Defined Formuia (Elemental) Diet Therapy (Abstract). Clin. Rca., 23: 591, 1975.
22. Hersh, E. M., Gutterman, J. U., Mavligit, G. M., McCredie, K. B.,Burgess, M. A., Matthews, A., and Freireich, E. J. Serial Studies ofImmunocompetence of Patients Undergoing Chemotherapy for AcuteLeukemia. J. Clin. Invest., 54: 401-408, 1974.
23. Holroyde,C. P., Gabuzda,T. G., Putnam,A. C., Paul,P., and Reichard,G. A. Altered Glucose Metabolism in Metastatic Carcinoma. Cancer Res.,35: 3710-3714, 1975.
24. Hrgovcic, M., Tessmer, C. F., Thomas, F. B., Fuller, L. M., Gamble, J. F.,and Schullenberger, C. C. Significance of Serum Copper Levels in AdultPatients with Hodgkin's Disease. Cancer, 31: 1337-1345, 1973.
25. Ilicin,G.SerumCopperandMagnesiumLevelsin LeukemiaandMalignant Lymphoma. Lancet, 2: 1036-1037, 1971.
26. Israel, L., Mugica, J., and Chahinian, P. Prognosis of Early BronchogenicCarcinoma. Survival Curves of 451 Patients after Resection of Lung
on April 25, 2019. © 1977 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from
1977;37:2348-2353. Cancer Res George L. Blackburn, Baltej S. Maini, Bruce R. Bistrian, et al. MetabolismThe Effect of Cancer on Nitrogen, Electrolyte, and Mineral
Updated version
http://cancerres.aacrjournals.org/content/37/7_Part_2/2348
Access the most recent version of this article at:
E-mail alerts related to this article or journal.Sign up to receive free email-alerts
Subscriptions
Reprints and
To order reprints of this article or to subscribe to the journal, contact the AACR Publications
Permissions
Rightslink site. Click on "Request Permissions" which will take you to the Copyright Clearance Center's (CCC)
.http://cancerres.aacrjournals.org/content/37/7_Part_2/2348To request permission to re-use all or part of this article, use this link
on April 25, 2019. © 1977 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from





























