Embed Size (px)
Citation preview
JAUNDICEBYDr
HAYDER M. ABDULNABICABS
Jaundice – Classification
Normal Serum Bilirubin (SB) is 0.3 to 1.0 mg%
Jaundice is increased levels of SB > 1.0 mg%
Over production of Bilirubin (Hemolytic)
From hemolysis of RBC
Impaired hepatic function (Hepatitic)
Hepatocellular dysfunction in handling bilirubin
Uptake, Metabolism and Excretion of bilirubin
Obstruction to bile flow (Obstructive)
Intrahepatic cholestasis
Extrahepatic Obstruction (Surgical Jaundice)
2www.drsarma.in
Clinical Aspects of Jaundice
Clinically detectable if SB is >3 mg%
With edema and dark skin – Jaundice is masked
What is special about the sclera ? – Rich Elastin
Darkening of the urine – Differential Diagnosis
Skin discoloration – Yellowish, - Carotinemia – Eyes N
Mucosa – hard palate (in dark skinned)
Greenish hue of skin and sclera - due Biliverdin – indicates
long standing jaundice ( CA head pancreas )
Generalized Pruritus – Obstructive Jaundice – Why ?
3www.drsarma.in
Clinical History – Imp cluesDuration of jaundice – Acute / ChronicAbdominal pain v/s painless jaundiceFever – Viral / bacteria /sepsisScraches-Pruritus - obstructiveAppetite – Hepatocellular / MalignancyWeight loss – Malignancy Colour of stools –chalky white –obstructiveFamily history – Hemolytic – Inherited dis.H/o transfusionAlcohol abuse, Medications – INH, EM, Largactil
www.drsarma.in 4

Coloured Urine – Differ. Diagnosis
Bilirubin in urine due to Jaundice (CB)Concentrated urine in dehydration Sulfasalazine use – for Ulcerative colitisRifampicin, Pyridium and Thiamine useRed urine – Porphyria, Hemoglobin & Myoglobinuria, HematuriaMelanin excretion from Melanoma-blackfood
www.drsarma.in 5
Fate of RBC
6
• RBC life span in blood stream is 90-120 days
• Old RBCs are phagocytosed and/or lysed
• Lysis occurs extravascularly in the RE system subsequent to RBC phagocytosis
• Intravascular Hemolysis of young RBC
• This is due to hemolytic diseases of RBC
www.drsarma.in
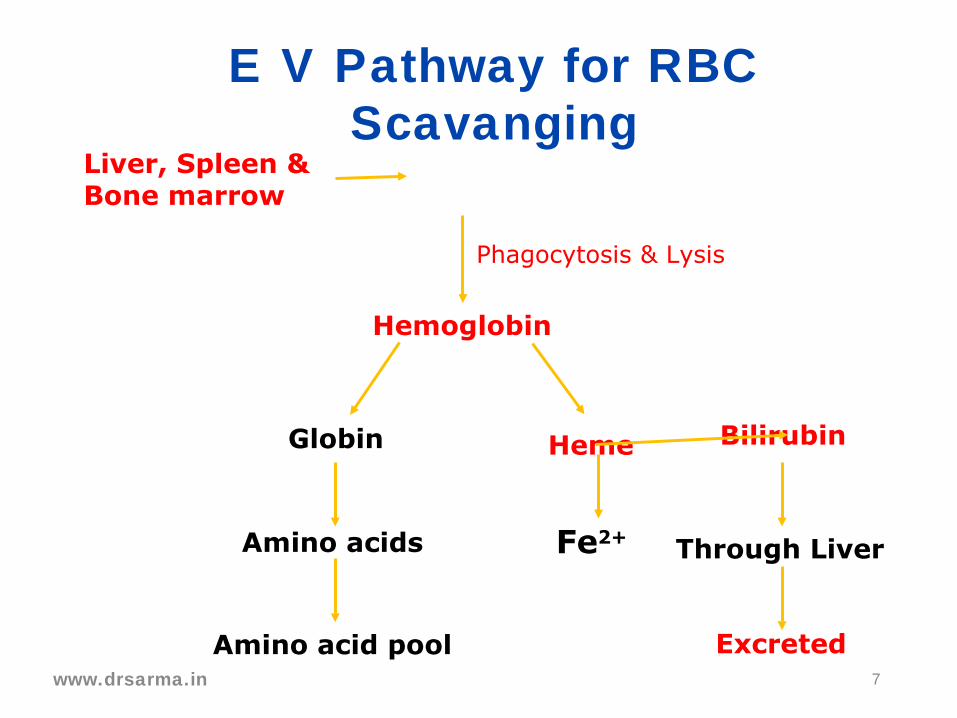
E V Pathway for RBC Scavanging
Liver, Spleen & Bone marrow
Hemoglobin
Globin
Amino acids
Amino acid pool
Heme Bilirubin
Fe2+
Excreted
Phagocytosis & Lysis
Through Liver
7www.drsarma.in
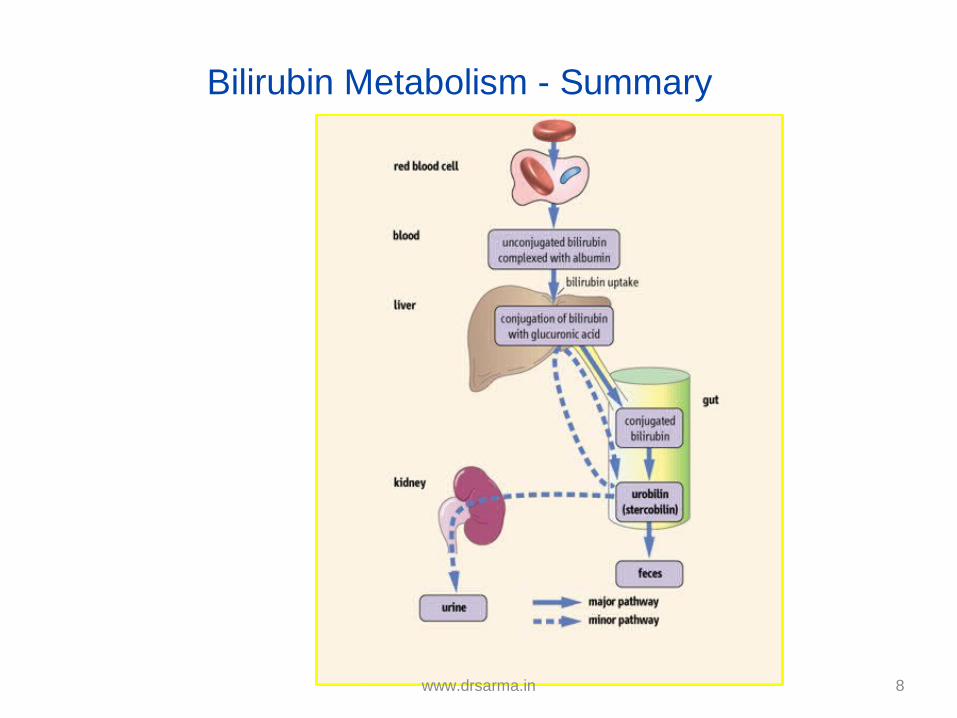
Bilirubin Metabolism - Summary
8www.drsarma.in
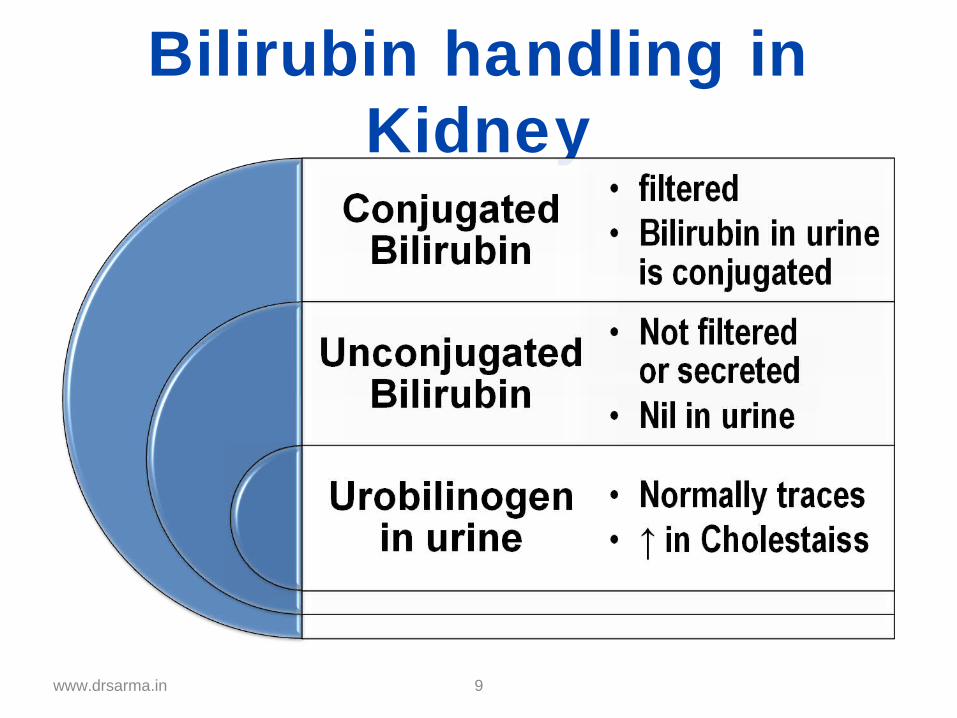
Bilirubin handling in Kidney
www.drsarma.in 9
How to clinically evaluate the patient ?
What tests will help us in D.D ?
What imaging modalities will be useful ?
How to monitor the progress ?
10
ALGORITHMIC APPROACH FOR JAUNDICE
www.drsarma.in
First Step
11www.drsarma.in
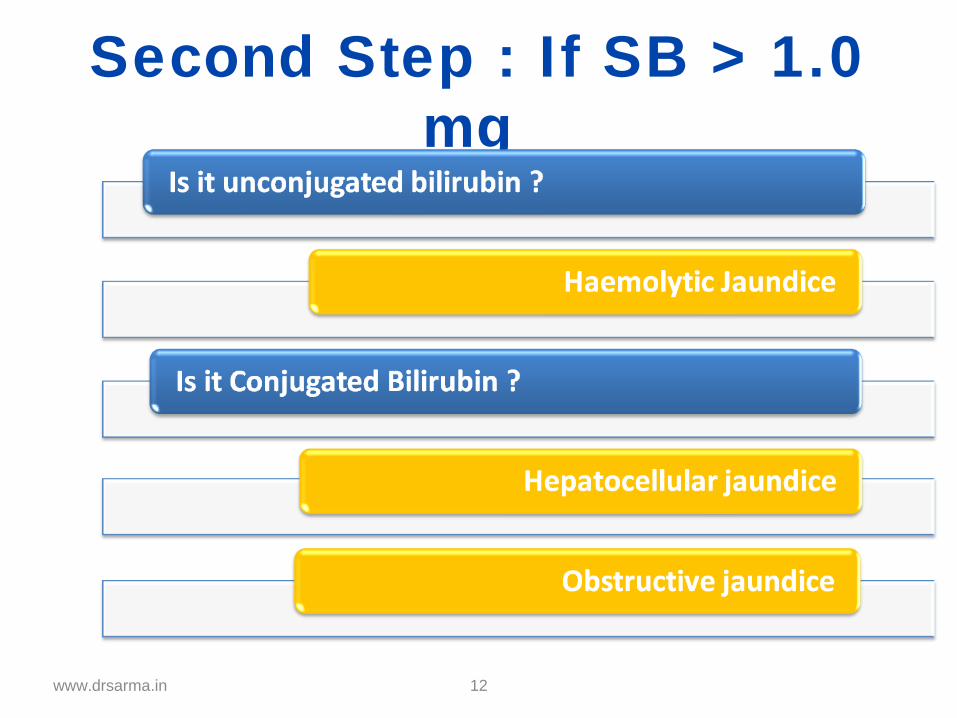
Second Step : If SB > 1.0 mg
12www.drsarma.in
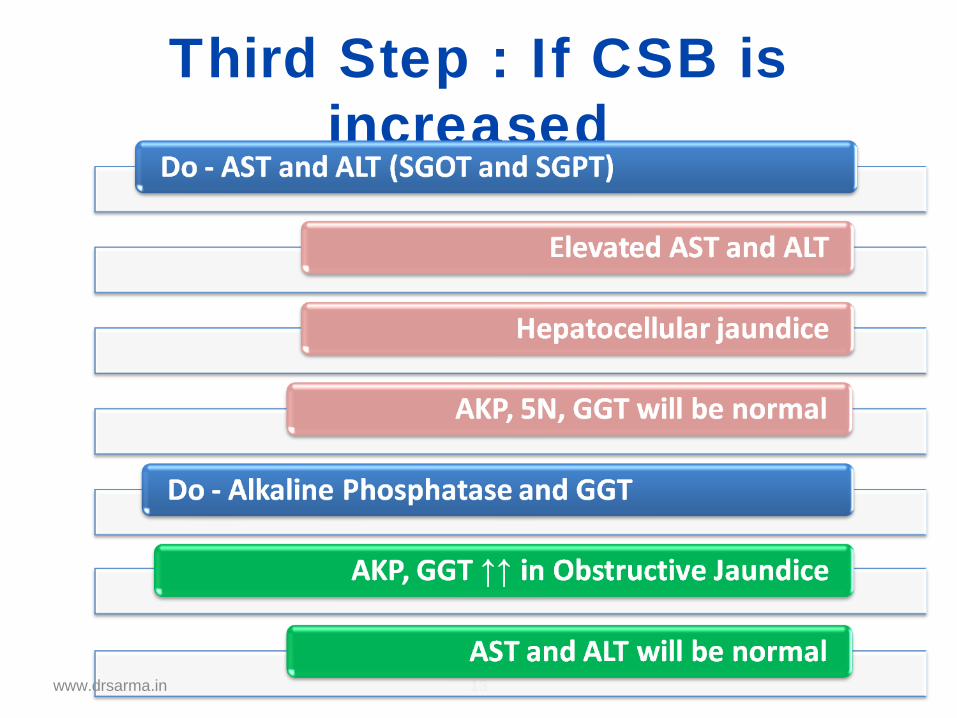
Third Step : If CSB is increased
13www.drsarma.in
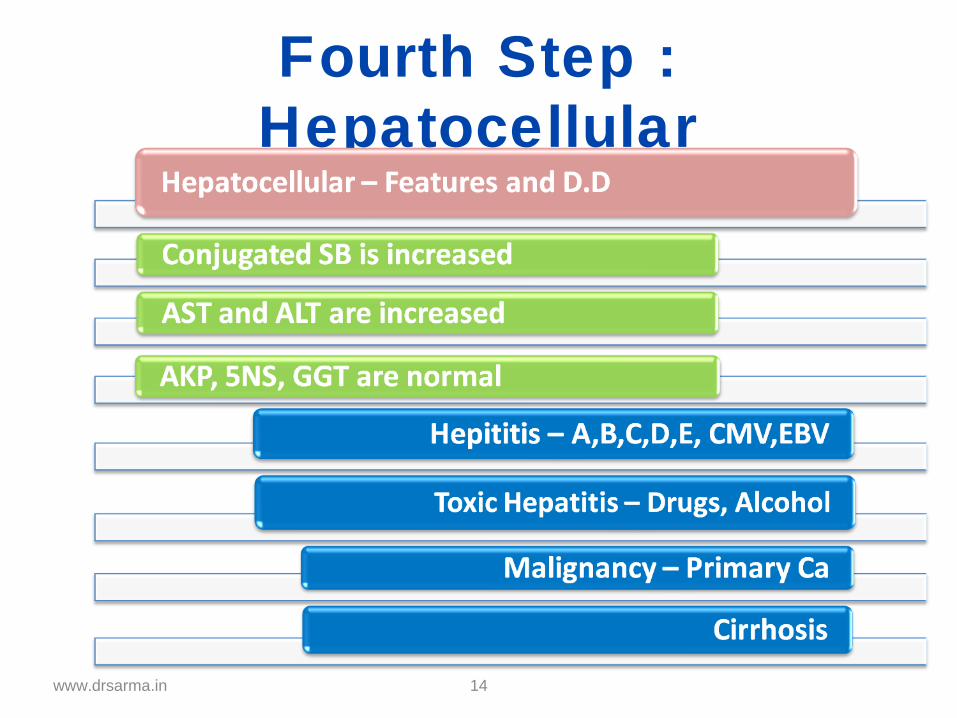
Fourth Step : Hepatocellular
14www.drsarma.in
What imaging we need
• Ultrasonography – 98% Sp, 90% Sen.
• For GB stones USG better than CT
• For duct stones –only 40% seen in USG
• PTC – Extrahepatic obstr. – drainage
• ERCP – Distal biliary obstruction Dx.Rx.
• MRCP – Most useful for duct stoneswww.drsarma.in 15
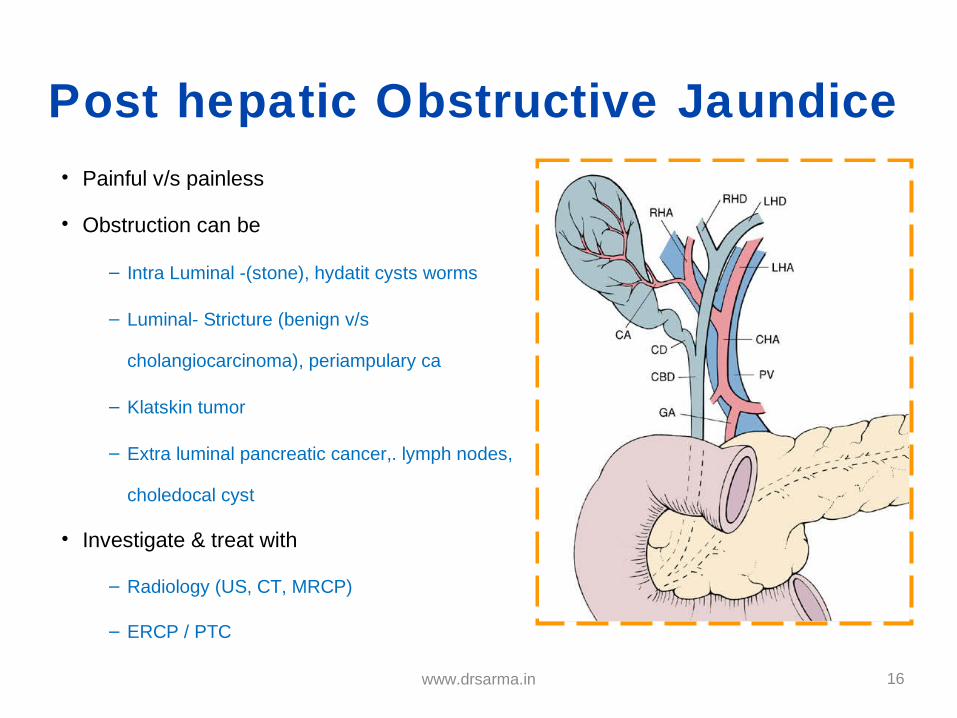
Post hepatic Obstructive Jaundice• Painful v/s painless
• Obstruction can be
– Intra Luminal -(stone), hydatit cysts worms
– Luminal- Stricture (benign v/s
cholangiocarcinoma), periampulary ca
– Klatskin tumor
– Extra luminal pancreatic cancer,. lymph nodes,
choledocal cyst
• Investigate & treat with
– Radiology (US, CT, MRCP)
– ERCP / PTC
16www.drsarma.in
• A Klatskin tumor (or hilar cholangiocarcinoma) is a cholangiocarcinoma (cancer of the biliary tree) occurring at the confluence of the right and left hepatic bile ducts. It is named after Dr. Gerald Klatskin, an American physician working at Yale.
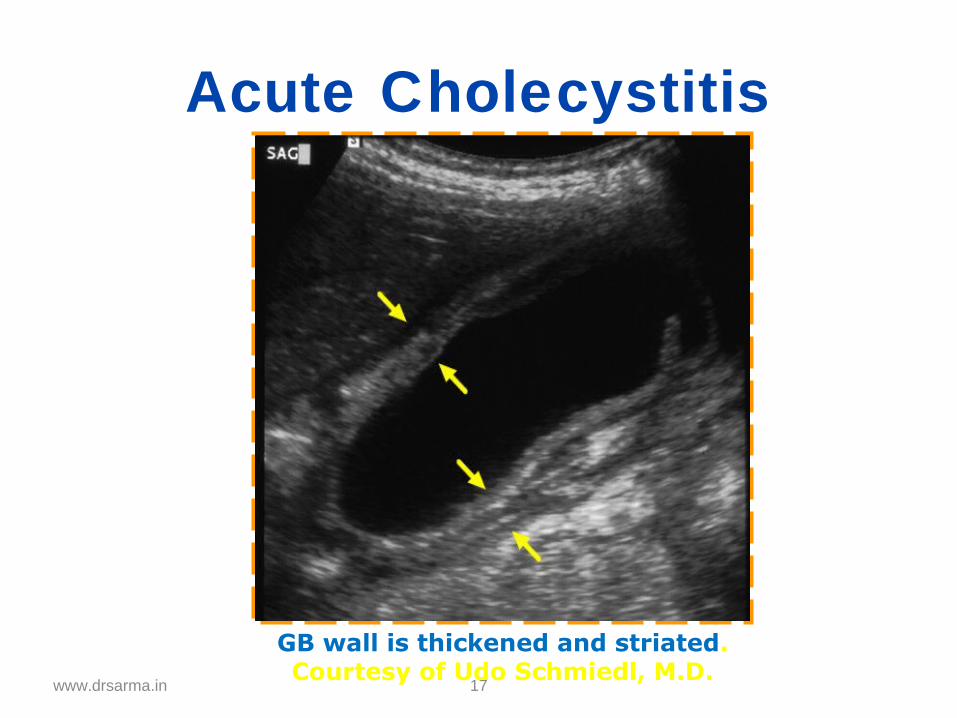
Acute Cholecystitis
17
GB wall is thickened and striated.Courtesy of Udo Schmiedl, M.D.
www.drsarma.in
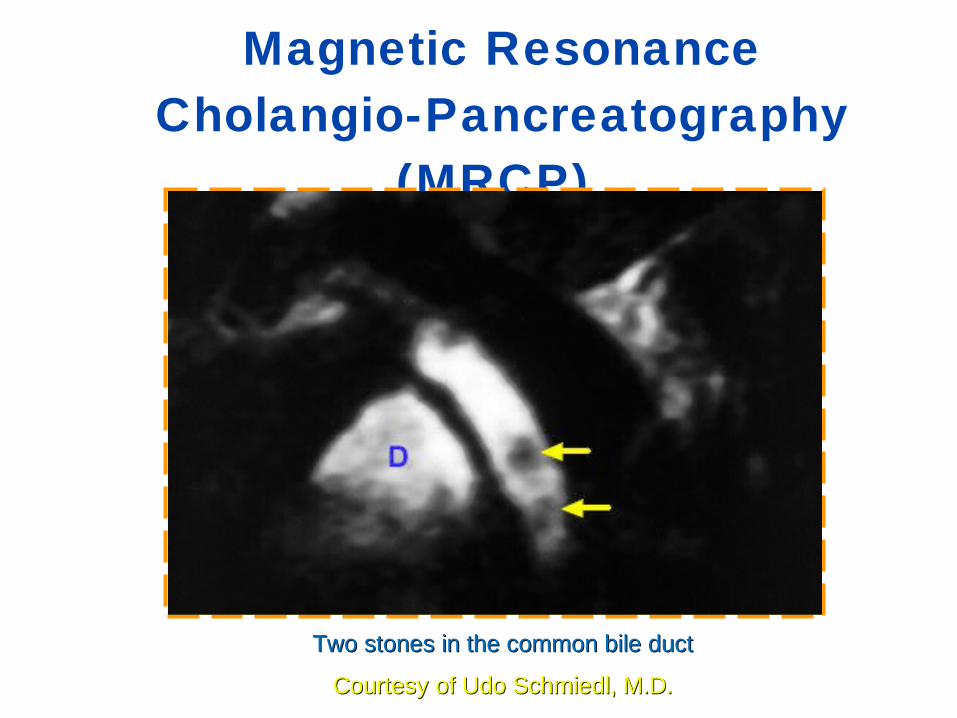
Magnetic Resonance Cholangio-Pancreatography
(MRCP)
Two stones in the common bile ductTwo stones in the common bile duct
Courtesy of Udo Schmiedl, M.D.Courtesy of Udo Schmiedl, M.D.
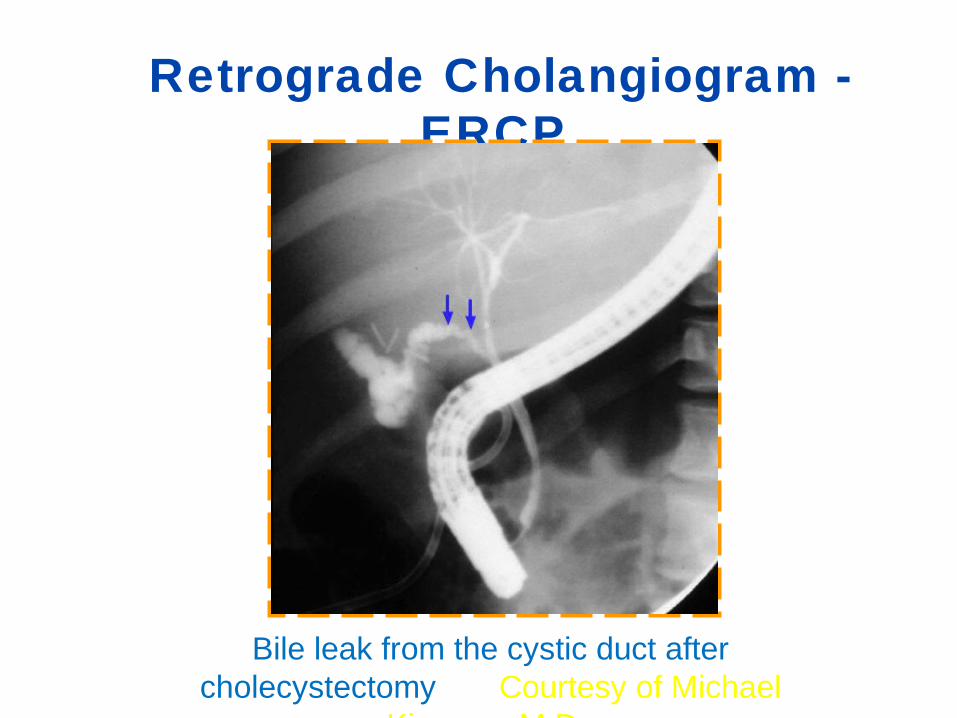
Retrograde Cholangiogram - ERCP
Bile leak from the cystic duct after cholecystectomy Courtesy of Michael
Kimmey, M.D.
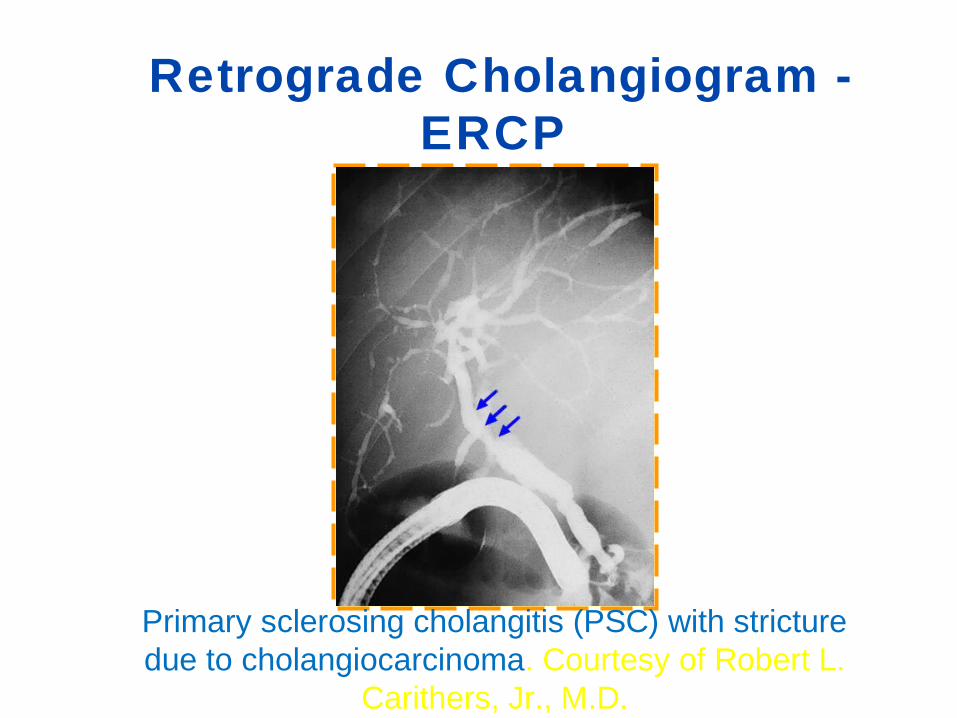
Primary sclerosing cholangitis (PSC) with stricture due to cholangiocarcinoma. Courtesy of Robert L.
Carithers, Jr., M.D.
Retrograde Cholangiogram - ERCP
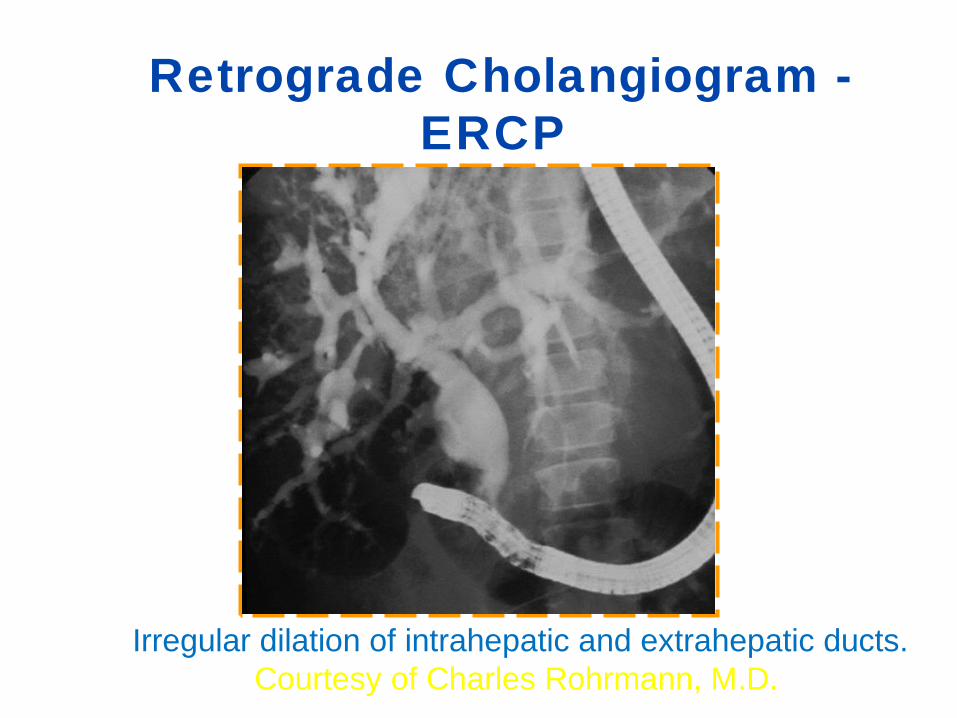
Irregular dilation of intrahepatic and extrahepatic ducts.Courtesy of Charles Rohrmann, M.D.
Retrograde Cholangiogram - ERCP
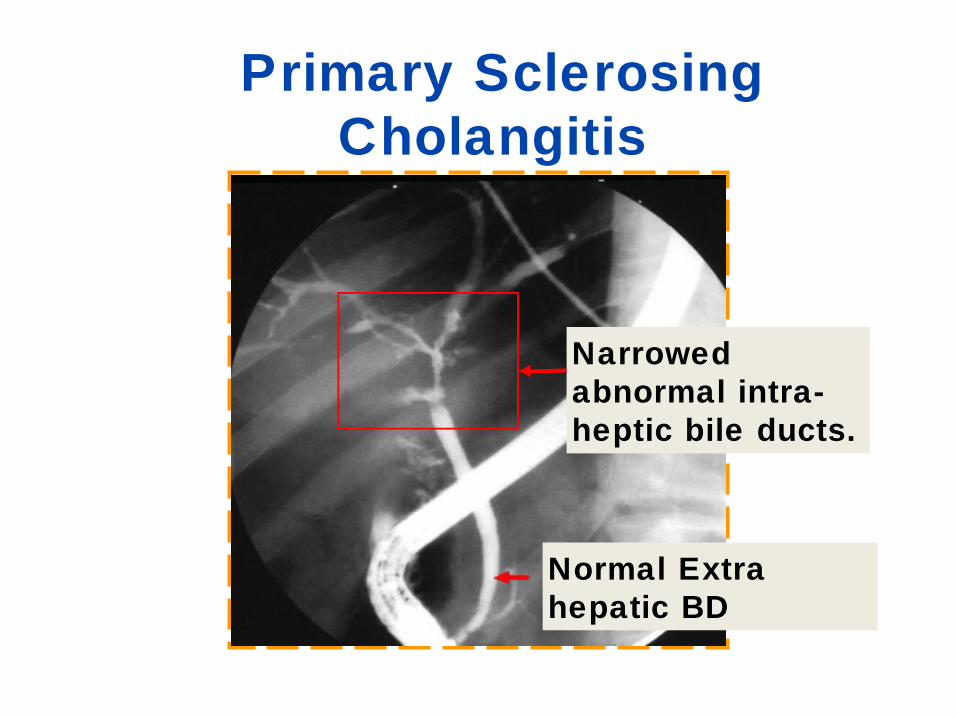
Primary Sclerosing Cholangitis
Normal Extra hepatic BD
Narrowed abnormal intra-heptic bile ducts.
23
PRE-OPERATIVE MANAGEMENT OF OBSTRUCTIVE JAUNDICE
1. HIGH INTAKE OF GLUCOSE (BUILD UP LIVER GLYCOGEN STORE)2. VITAMIN K (FAT SOLUBLE), 10mg IV OR IM3. ANTIBIOTICS (BROAD SPECTURUM)4. HYDRATION (PREVENT RENAL FAILURE) (5% DEXTROSE TO ENSURE 30 ml/HOUR URINE FLOW)5. DIURESIS – MANNITOL- 200ML REGIMEN
24
SURGICAL PROCDURES1. ENDOSCOPIC PAPILLOTOMY (DORMIA BASKET, BALLOON CATHETER)(STENT TO RELIEVE SYMPTOMS)2. PERCUTANEOUS REMOVAL OF STONES BY BURHENNE METHOD (T- TUBE LEFT FOR SIX WEEKS AND THEN REMOVED, DILATION OF THE MATURE TRACT, STEERABLE CATHETER, AND THEN STONE BASKET)3. PERCUTANEOUS BILIARY DRAINAGE (PTC), IN THE VERY ILL4. SUPRADUODENAL CHOLEDOCHOTOMY WITH OR WITH OUT TRANSDUODENAL SPHINCTEROTOMY OR CHOLEDOCHODUODENOSTOMY5. STENTING

25
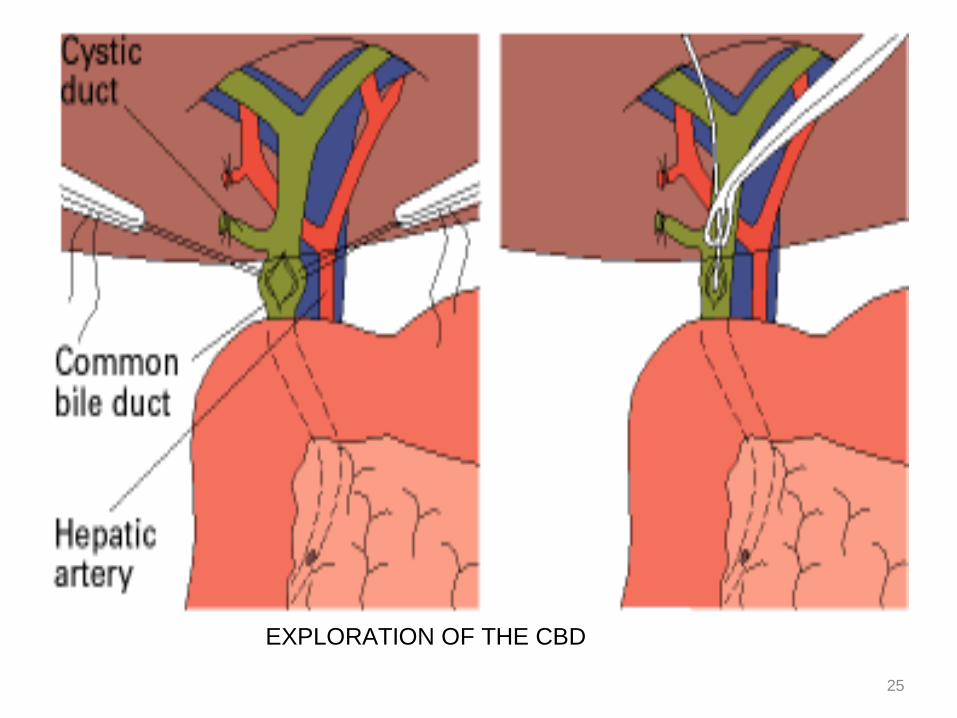
EXPLORATION OF THE CBD
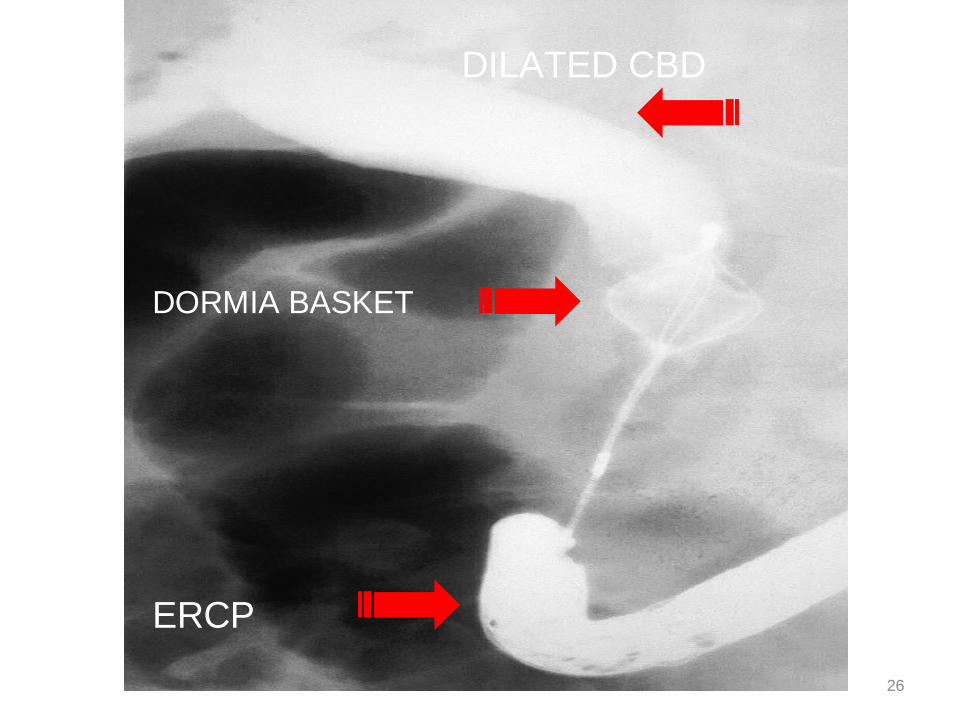
26
DORMIA BASKET
ERCP
DILATED CBD
Ascending cholangitis
• Physical examination findings typically include jaundice and right upper quadrant tenderness.
• Charcot's triad is a set of three common findings in cholangitis: abdominal pain, jaundice, and fever.
Causes•OBSTRUCTION
•GALL STONES 10-30% of cases•CA•TRAUMATIC-- ERCP
• TESTS
• MANAGEMENT