Embed Size (px)
Citation preview
Nurse-Directed Care Model ina Psychiatric Hospital
A Model for Clinical Accountability
MARLENE E-MORRIS, MSN, APRN, BC;
BARBARA CALDWELL, PhD, APRN, BC;
KATHLEEN J. MENCHER, MSN, APRN, BC;
KIMBERLY GROGAN, RN, NACC;
MARGARET JUDGE-GORNY, MSN, APRN, BC;
ZELDA PATTERSON, MSN, PMHCNS-BC;
TERRIAN CHRISTOPHER, MSN, APRN-BC;
RUSSELL C. SMITH, MS, LPC; TERESA MCQUAIDE, MSN, APRN, BC
Purpose: The focus on recovery for persons with severe and persistent mental illness isleading state psychiatric hospitals to transform their method of care delivery. This article
describes a quality improvement project involving a hospital’s administration and multi-
disciplinary state-university affiliation that collaborated in the development and implementa-
tion of a nursing care delivery model in a state psychiatric hospital. Description of theProject: The quality improvement project team instituted a new model to promote the hospital’s
vision of wellness and recovery through utilization of the therapeutic relationship and greater
clinical accountability. Implementation of the model was accomplished in 2 phases: first, the
establishment of a structure to lay the groundwork for accountability and, second, thedevelopment of a mechanism to provide a clinical supervision process for staff in their work with
clients. Effectiveness of the model was assessed by surveys conducted at baseline and after
implementation. Outcome: Results indicated improvement in clinical practices and client living
environment. As a secondary outcome, these improvements appeared to be associated with
increased safety on the units evidenced by reduction in incidents of seclusion and restraint.
Conclusions: Restructuring of the service delivery system of care so that clients are the center
of clinical focus improves safety and can enhance the staff’s attention to work with clients on
their recovery. Implications: The role of the advanced practice nurse can influence the recovery
f e a t u r e a r t i c l e
CL IN ICAL NURSE SPEC IAL I STA154
Clinical Nurse SpecialistA Copyright B 2010 Wolters Kluwer Health | Lippincott Williams & Wilkins
Author Affiliations: University of Medicine and Dentistry of New Jersey–School of Nursing, Newark (Ms
E-Morris, Dr Caldwell, andMsMencher); Greystone Park Psychiatric Hospital, Greystone Park (MssGrogan,
Judge-Gorny, Patterson, and Christopher); Department of Psychiatric Rehabilitation, University of
Medicine andDentistry of New Jersey, Scotch Plains (Mr Smith); and Trenton Psychiatric Hospital,West
Trenton (Ms McQuaide), New Jersey.
Correspondence:Marlene E-Morris, MSN, APRN, BC, Greystone Park Psychiatric Hospital, Greystone Park,
NJ 07950 ([email protected]).
Copyright @ 20 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.10

of clients in state psychiatric hospitals. Future research shouldconsider the impact on clients and their perceptions of the new
service models.
KEY WORDS: nursing practice, psychiatric hospital, recovery
S tate psychiatric hospitals continue to provide residentialand medical services to a significant number of people
with severe and persistent mental illness. Despite the 89%reduction in census due to deinstitutionalizations since 1950,approximately 60,000 individuals with severe and persistentmental illness remain hospitalized in US state psychiatricfacilities.1 Although there has been a nationwide commit-ment to community mental health, many people who residein state hospitals have difficulty accessing services because ofchronic substance abuse, dual diagnosis, forensic history, orissues of noncompliance.2 The challenge to hospitals is toprovide exemplary psychiatric services to individuals witha complex array of issues, while adhering to prevailing re-covery principles that focus on rehabilitation leading to alife in the community.3 The purpose of this article was todescribe a quality improvement project focusing on theprocess of implementing a new nursing model in 1 buildingof the hospital to increase the accountability for person-centered interventions. The person-centered interventions arefocused on establishing a system of individual supports thatstrives to assist each person’s effort to recover from the effectsof mental illness. Also included are outcome data that showclinical, environmental, and safety improvements that resultedfrom the facilitation of a therapeutic staff-client relationship.
HISTORICAL BACKGROUND OF SERVICEDELIVERY IN STATE PSYCHIATRIC HOSPITALS
Many psychiatric hospitals have found that implementingprogramming that is genuinely therapeutic with an em-phasis on preparation for living in the community has notbeen sustainable and has led to low morale among serviceproviders.4,5
In addition, the flow of resources toward the communityhas resulted in overcrowding, poorly trained staff, and sub-standard programming that has threatened the overall stan-dards of hospital care.6 State institutions, where care isprimarily custodial, often have staffing patterns on the unitswith a high ratio of unlicensed-to-licensed staff. A largeportion of the care activities in these hospitals is carried out byunlicensed, untrained, or uncertified personnel. In comparingprivate with state and county hospitals, nondegree or para-professional staff comprised 8.7% of mental health workers,whereas in state hospitals the proportion was 40.9%.7
In 1998, the state of New Jersey, in an effort to respondto the emerging focus on recovery for clients with mentalillness, formed a multidisciplinary state-university affilia-tion to improve the quality of care at the state psychiatrichospitals.8 The multidisciplinary team included advancedpractice psychiatric nurses (APNs), psychiatric rehabilita-tion instructors, and psychiatrists. From the state universityschool of nursing, there were 4 APNs, hired as consultants,who worked collaboratively with 4 APNs from the statehospital on new projects. Using multiple approaches, thegoal of the affiliation is to improve the quality of care by
replacing the custodial model of care delivery with one thatis collaborative, person centered, and recovery based. In2006, a formal expression of such a goal was presented bythe New Jersey Department of Human Services Division ofMental Health Services. The plan outlines a 3-phase pro-cess that guides the state system as it embarks on a trans-formation process toward wellness and recovery.9 Recoveryis defined as ‘‘a journey of healing and transformation forpersons with mental health disability to be able to live ameaningful life in communities of his or her choice whilestriving to achieve the full human potential of personhood.’’6
This paradigm has at its core a vision that recovery frommental illness is possible and that much of the care nowbeing provided in the inpatient setting can be provided inthe community.
This new vision has encouraged the mental healthsystem to assess prevailing practices and attitudes in lightof client-identified themes that promote hope and a morepositive self-identity. State hospitals are also consideringhow the implications of recovery concepts can be understoodand blended into acute medical and psychiatric services.3
Numerous studies have reported that clients who are suc-cessfully recovering from the effects of a long-term mentalillness cite the presence of an individual in their life who is aconsistent and a reliable source of emotional support.10 Thismore personal ‘‘therapeutic alliance’’ has been shown to bean integral component of successful clinical interventions.11
In hospital settings, it is often the case that although pro-fessional support is ubiquitous, this more personal connec-tion can be lost. In fact, the clients who are most likely tohave formal counseling are only those who are immediatelyproblematic.
THE MODEL
In the development of the nursing model, several keyfactors were considered. First, the therapeutic nurse-clientrelationship would be the vehicle by which the trans-formation in care delivery would take place. This requiredthe establishment and maintenance of a primary relation-ship between the staff and the clients that would remainconsistent. Second, the APNs could focus their expertise intheir established role as change agent, educators, and theprofessional who interfaces with the treatment team. TheAPNs, bridging communication to and from the team andother nursing staff, would play a key role in assisting staffto develop and sustain a therapeutic relationship as theywork with clients. Third, the model had to effectively in-corporate the high ratio of paraprofessional to professionalstaff found on the units. This required a push to utilize theparaprofessional staff in a more effective and efficientmanner and to reestablish the professional nurse as the onewho assesses, plans, directs, and evaluates the nursing carebeing provided. To emphasize this point, the model wasentitled the ‘‘Nurse-Directed Care Model’’ (NDCM).
The NDCM combines components from primary nursingand team nursing models. It provides structure, account-ability, coordination, and communication between the client,significant others, and paraprofessional and professionalstaff. In addition, the NDCM provides for ongoing clini-cal supervision by the unit APN to help staff link the day-to-day interventions to the client’s treatment plan goals.
VOLUME 24 | NUMBER 3 155
Copyright @ 20 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.10

The theoretical framework of the model is based onDorothea Orem’s Self-care Deficit Theory in which nurses’actions focus on health restorative functions and clients play amajor role in collaborating and partnering with staff.12
Orem’s general theory integrates other related theories suchas ‘‘self-care,’’ ‘‘self-care deficit,’’ and ‘‘nursing systems.’’Both the client and the nurse collaborate to assess the indi-vidual’s self-care deficit to determine the types of inter-vention that are needed to promote health and wellness.12
Nursing as a clinically focused discipline must advocate forclient autonomy and work collaboratively with clients indeveloping realistic and attainable recovery goals. Thistheoretical framework is applicable to psychiatric settingsand the NDCM, in that it fosters the collaboration ofclients and staff in the process of restoring health. It alsoprovides guidelines to help nurses determine in partnershipwith the clients their recovery and self-care needs to main-tain their optimum level of functioning and autonomy.13
Clients need to be involved in their own goal develop-ment. The guiding principles of the NDCM are centered onspecific roles and establishment of key personnel. The APNfunctions as the clinical expert who participates in allaspects of the therapeutic milieu providing education andclinical supervision to all levels of nursing staff. The reg-istered nurse, in addition to providing recovery orientednursing care, focuses on directing, supervising, and evaluatingthe care provided to clients by the paraprofessional staff. Theparaprofessional staff functions as care extenders.
The structure of the model is as follows:
& All clients and staff on the units are divided into 2NDCM teams.
& Registered nurses (RNs) are assigned as NDCM teamleaders.
& Licensed practical nurses (LPNs), under the direction ofan RN, function as assistant team leader.
& Each paraprofessional staff is assigned to a group of 4 to6 clients (subteams), with a focus on clinical, environmen-tal, and behavioral aspects of care and receives clinicalsupervision from the RN and unit APN.
& The NDCM assignment sheets, which include team listand subteams, are developed and are used daily.
& Team lists are posted on the wards visible to everyone,including clients.
& Medications and treatments are administered by the RNor LPN of their team.
& Daily work sheets for paraprofessionals outline prioritiesof observational and direct care.
This structure makes it possible for the same groups ofclients and staff to consistently work together across all 3shifts and thereby facilitate the development of a therapeu-tic bond and a good working alliance between clients andstaff. Because the units are divided into 2 teams, each teamleader is in charge of a smaller group of clients and canplan and direct the care for the same group each day. Thisfosters a working relationship where (1) staff has knowl-edge of the treatment goals for the clients over time, (2)there is consistency in client-staff assignment, and (3) thereis improved communication between clients and staff, andamong staff. The goal is that nursing care would progressbeyond custodial care to a more recovery-focused ap-proach in which each client is known and valued for his/her
uniqueness and individualized strengths and is given anopportunity to partner with staff in the achievement of his/her recovery goals.14 It is through knowing each client asan individual that appropriate interventions can be devel-oped and behavioral change can take place.
The NDCM expands the parameters of the current roleand function of each level of staff, particularly the LPN andparaprofessional. The LPN, formerly utilized primarily as amedication nurse, is now expected to function in the role ofteam leader, in the absence of the RN. The paraprofessionalstaff’s role is also pushed beyond the limits of assistingprimarily with activities related to daily hygiene to one wherethey are expected to become more involved in all aspects ofthe care for their core group of clients. They will be expectedto participate in their assigned clients’ treatment team meet-ings and know the client’s discharge goals and barriers andpartner with clients to teach skills necessary to overcomethose barriers. They will also be expected to utilize specificinterventions to help clients maintain or regain control.
Morris and Stuart,7 in their outline of the educationalneeds of frontline staff in behavioral health practices, statesthat ‘‘Learning should not take place in a vacuum.’’(p398)
For mastery to occur, staff must be given the opportunityto practice and apply what they are being taught in actualclinical settings. In this model, the integration of informa-tion into clinical practice takes place in the formal clinicalsupervision meetings led by the APN and client care man-ager on each unit. In these meetings, team leaders andparaprofessional staff discuss care delivery issues and eval-uate clinical intervention for their clients. Typically, duringthese meetings, there are didactic instructions, discussion ofspecific client care issues, and issues related tomanagement ofthe milieu. Interventions are developed and linked to theoverall treatment plan, and recommendations are made onhow to assist clients through the use of the therapeuticrelationship as a vehicle to bring about behavior change.Although the unit APN is available to assist staff individuallyas he/she works with their clients, these formal groupsupervision meetings provide an opportunity for other mem-bers of the team to be part of the discussion and thedevelopment of interventions for a particular client.
METHODS
This quality improvement project implementation phaselasted about 9 months and was first piloted in 1 building,with the plan to extend the use of the model hospitalwide.To ensure success, the APNs, client care managers, andassistant directors of nursing from the designated buildingand the state-university affiliation APNs formed a leader-ship group to oversee the implementation plan for thebuilding. To ensure standardization across units, this nurs-ing leadership group developed a manual that outlined allaspects of the model, including role, function, and expec-tation of each level of staff. The manuals were distributedto all units to be used as a resource. The nursing leadershipgroup also collaborated with the licensed staff in thedevelopment of shift-specific NDCM daily assignmentsheets. Each assignment sheet lists the team leaders forthe shift and the client-staff subteams. The leadership groupmet weekly to coordinate the process, problem solve asbarriers emerged, and to plan and conduct ongoing training.
CL IN ICAL NURSE SPEC IAL I STA156
Copyright @ 20 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.10
Each step of implementation was done simultaneously oneach unit in the building.
All staff training was provided by members of the lead-ership group. For the licensed professional staff, educationincluded topics such as leadership skills, characteristics ofeffective team leaders, effective communication techniques,and components of delegation responsibilities. For the para-professional staff, training topics included components of ahelping relationship, therapeutic communication, and roleexpectations for the direct care provider with a focus onrecovery-oriented behaviors.
Because this is a quality improvement demonstrationproject, several clinical and environmental indicators wereidentified to measure changes resulting from the implemen-tation of the NDCM. Baseline measures were obtained atthe initial phase of the implementation process, and follow-up measures were done 9 months later. The members of thenursing leadership group interviewed staff and clients toassess their knowledge of treatment plan goals and otherclinical issues and to observe the condition of the clients’living environment. Responses to the surveys were chartcongruent in that the information was verified for accuracyby reviewing the medical record and posted NDCM masterlist and assignment sheets. A total of 141 staff on the dayand evening shifts were targeted for the evaluation process.This included 32 RNs, 17 LPNs, and 92 paraprofessionalstaff. Premeasures were completed on 32 staff (23%). Atotal of 53 staff (37.5%) and 19 of their clients were inter-viewed for the postmeasures. The original survey containedan 8-item questionnaire. The postmeasures included an ex-panded version of the original survey, to include questionsto assess the staff’s knowledge of their assigned clients dis-charge goals, level of supervision, and their attendance intheir treatment team meetings.
RESULTS
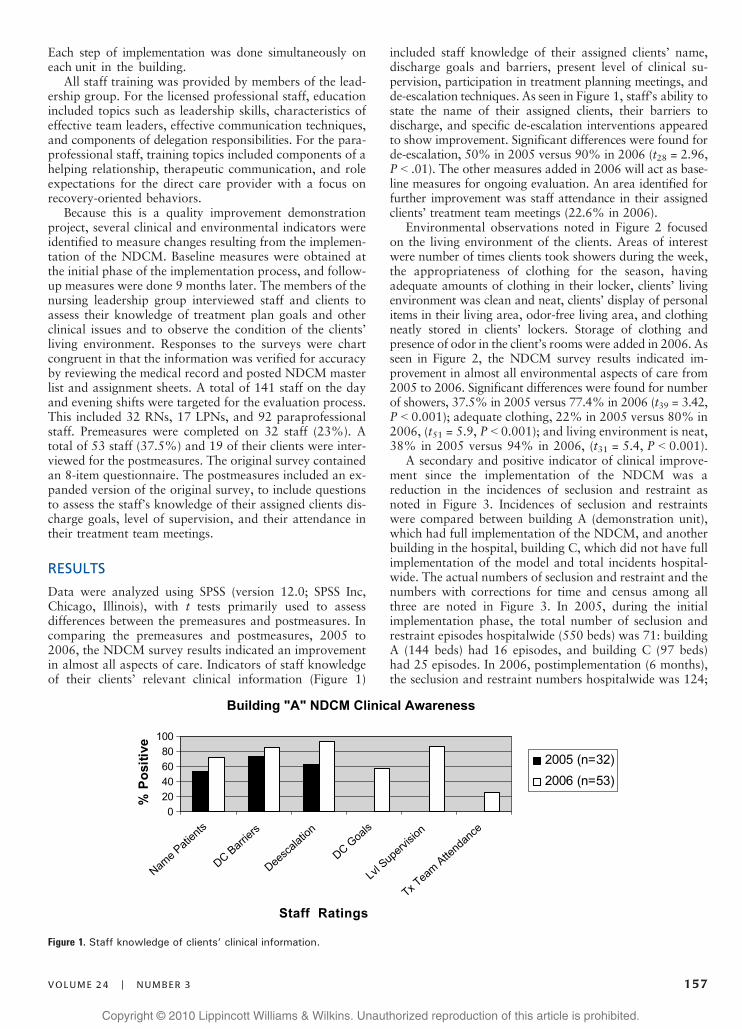
Data were analyzed using SPSS (version 12.0; SPSS Inc,Chicago, Illinois), with t tests primarily used to assessdifferences between the premeasures and postmeasures. Incomparing the premeasures and postmeasures, 2005 to2006, the NDCM survey results indicated an improvementin almost all aspects of care. Indicators of staff knowledgeof their clients’ relevant clinical information (Figure 1)
included staff knowledge of their assigned clients’ name,discharge goals and barriers, present level of clinical su-pervision, participation in treatment planning meetings, andde-escalation techniques. As seen in Figure 1, staff’s ability tostate the name of their assigned clients, their barriers todischarge, and specific de-escalation interventions appearedto show improvement. Significant differences were found forde-escalation, 50% in 2005 versus 90% in 2006 (t28 = 2.96,P G .01). The other measures added in 2006 will act as base-line measures for ongoing evaluation. An area identified forfurther improvement was staff attendance in their assignedclients’ treatment team meetings (22.6% in 2006).
Environmental observations noted in Figure 2 focusedon the living environment of the clients. Areas of interestwere number of times clients took showers during the week,the appropriateness of clothing for the season, havingadequate amounts of clothing in their locker, clients’ livingenvironment was clean and neat, clients’ display of personalitems in their living area, odor-free living area, and clothingneatly stored in clients’ lockers. Storage of clothing andpresence of odor in the client’s rooms were added in 2006. Asseen in Figure 2, the NDCM survey results indicated im-provement in almost all environmental aspects of care from2005 to 2006. Significant differences were found for numberof showers, 37.5% in 2005 versus 77.4% in 2006 (t39 = 3.42,P G 0.001); adequate clothing, 22% in 2005 versus 80% in2006, (t51 = 5.9, P G 0.001); and living environment is neat,38% in 2005 versus 94% in 2006, (t31 = 5.4, P G 0.001).
A secondary and positive indicator of clinical improve-ment since the implementation of the NDCM was areduction in the incidences of seclusion and restraint asnoted in Figure 3. Incidences of seclusion and restraintswere compared between building A (demonstration unit),which had full implementation of the NDCM, and anotherbuilding in the hospital, building C, which did not have fullimplementation of the model and total incidents hospital-wide. The actual numbers of seclusion and restraint and thenumbers with corrections for time and census among allthree are noted in Figure 3. In 2005, during the initialimplementation phase, the total number of seclusion andrestraint episodes hospitalwide (550 beds) was 71: buildingA (144 beds) had 16 episodes, and building C (97 beds)had 25 episodes. In 2006, postimplementation (6 months),the seclusion and restraint numbers hospitalwide was 124;
Figure 1. Staff knowledge of clients’ clinical information.
VOLUME 24 | NUMBER 3 157
Copyright @ 20 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.10
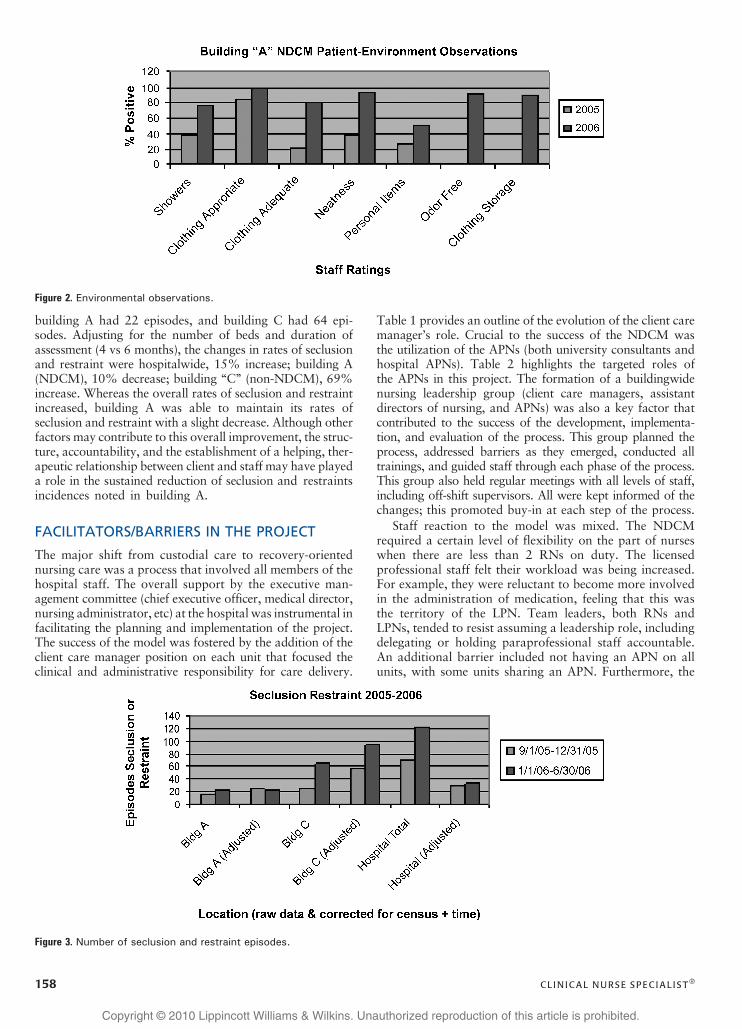
building A had 22 episodes, and building C had 64 epi-sodes. Adjusting for the number of beds and duration ofassessment (4 vs 6 months), the changes in rates of seclusionand restraint were hospitalwide, 15% increase; building A(NDCM), 10% decrease; building ‘‘C’’ (non-NDCM), 69%increase. Whereas the overall rates of seclusion and restraintincreased, building A was able to maintain its rates ofseclusion and restraint with a slight decrease. Although otherfactors may contribute to this overall improvement, the struc-ture, accountability, and the establishment of a helping, ther-apeutic relationship between client and staff may have playeda role in the sustained reduction of seclusion and restraintsincidences noted in building A.
FACILITATORS/BARRIERS IN THE PROJECT
The major shift from custodial care to recovery-orientednursing care was a process that involved all members of thehospital staff. The overall support by the executive man-agement committee (chief executive officer, medical director,nursing administrator, etc) at the hospital was instrumental infacilitating the planning and implementation of the project.The success of the model was fostered by the addition of theclient care manager position on each unit that focused theclinical and administrative responsibility for care delivery.
Table 1 provides an outline of the evolution of the client caremanager’s role. Crucial to the success of the NDCM wasthe utilization of the APNs (both university consultants andhospital APNs). Table 2 highlights the targeted roles ofthe APNs in this project. The formation of a buildingwidenursing leadership group (client care managers, assistantdirectors of nursing, and APNs) was also a key factor thatcontributed to the success of the development, implementa-tion, and evaluation of the process. This group planned theprocess, addressed barriers as they emerged, conducted alltrainings, and guided staff through each phase of the process.This group also held regular meetings with all levels of staff,including off-shift supervisors. All were kept informed of thechanges; this promoted buy-in at each step of the process.
Staff reaction to the model was mixed. The NDCMrequired a certain level of flexibility on the part of nurseswhen there are less than 2 RNs on duty. The licensedprofessional staff felt their workload was being increased.For example, they were reluctant to become more involvedin the administration of medication, feeling that this wasthe territory of the LPN. Team leaders, both RNs andLPNs, tended to resist assuming a leadership role, includingdelegating or holding paraprofessional staff accountable.An additional barrier included not having an APN on allunits, with some units sharing an APN. Furthermore, the
Figure 3. Number of seclusion and restraint episodes.
Figure 2. Environmental observations.
CL IN ICAL NURSE SPEC IAL I STA158
Copyright @ 20 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.10

inconsistency in staffing due to ‘‘floating’’ practices under-mined the principle of a consistent client-staff assignment.Finally, high census and acuity levels would often derail thefunctioning of the model, leaving the units unable to movebeyond the usual mode of operating.
The paraprofessional staff was open to the NDCM;however, they voiced concern that other assignments suchas more task-related activities, such as transporting clientsfrequently, kept them away from fully participating. Therealso exist some resistances by staff to engage in meaningfulone-on-one conversation with clients. Some staff who hadworked for many years in the state system found it difficult toembrace this new model of care delivery, and many trans-ferred out of the building. Many of the new staff assigned tothe building was accepting of the added role expectations.
The following quotes from staff will highlight improvedstaff morale after implementation of the model:
Nurses: Does this model promote quality patient care?
I am more able to focus on the patients. . .. I am morefamiliar with their diagnosis and treatment. . . more ableto track them.
I ammore familiarwith theirmedications and their behaviors. . .more able to prevent escalation [of problem behaviors].
Direct care provider (paraprofessional): What do you likeabout the model?
I know my patients’ needs. When I come in, I knowwhat kind of help each of my patients needs. . . If theyneed assistance with their laundry. . . what groups they
are assigned. . . do they need to be encouraged to attendgroup. I know my patients.
Despite the success of the NDCM, the sustainability ofthe gains will require a considerable effort, constant vigi-lance, guidance, and support at the unit level to prevent areversal to ‘‘business as usual.’’
CONCLUSIONS
In a large state psychiatric facility that is attempting to shiftfrom a custodial to recovery model, we found that progresscan occur with a firm commitment from the administrativeand management group. We implemented a model of caredelivery that promotes recovery through enhanced client-staff relationship. This model can be generalized to otherhospitals, and plans are being made to adopt the model toother psychiatric facilities in the state. Further refinement ofthe NDCM could include an expansion beyond the disciplineof nursing to include, for example, the assignment of a socialworker on each team who will participate in the clinicalsupervisionmeetings and impart information about dischargeplans for clients and the skills needed to achieve successfulcommunity placement.
Preimplementation and postimplementation measuressuggest that the NDCM successfully improved staff’sknowledge of relevant clinical information about theirclients, including specific de-escalation interventions. Therewas also improvement in client living environment andoverall unit safety evidenced by reduction in incidences ofseclusion and restraint. This reduction could be a combinedresult of the established therapeutic alliances and theimprovement in staff knowledge on helping their clientsmaintain and regain control through the use of de-escalation techniques. This echoes Delaney and Johnson’s15
findings that a key factor in creating and maintaining a safemilieu was the ‘‘connections formed with client, an attune-ment with their affect, and an understanding of what theyneed and how that need was being expressed.’’15(p204)
The journey toward recovery takes place in an environ-ment where people feel safe and are able to be involved in atrusting relationship with another person. The inpatientsetting can be a place to begin the process of creating newmeaningful connections, or it can reinforce a sense of iso-lation, fear, and mistrust. Recovery often takes place througha helping relationship where hope is nurtured and peoplelearn to value themselves. The NDCM that was institutedin this state hospital was an attempt to foster and nurture atherapeutic alliance where healing can take place.
Table 2. Role of the Advanced PracticeNurse (Both UniversityConsultants and HospitalAdvanced Practice Nurses)
& Change agent: custodial care to recovery service delivery
& Educator: curricular development, implementation, and ongoingevaluation of a recovery-oriented system of care
& Individual and formal group clinical supervision meetings
& Facilitating therapeutic relationships between ancillary staffand patients
& Support structures for team such as routine team-buildingmeetings, changes in 24-h reporting forms to document patientassessments, interventions, and evaluations
& Integrate day-to-day interventions with patients based ontreatment plans and recovery goals
Table 1. Changes to Role of Client Care Manager in Nurse-Directed Care Model
Area of Change Traditional Nurse-Directed Care Model
Role of registered nurse manager Hospital supervisor several units (8-h responsibility) Client care manager (24-h responsibility)
Leadership No consistent accountability and leadership Formal leadership every day for unit functioning
Focus of role Administrative role Clinical and administrative role
Delivery of care Unstructured Team based with ancillary staff reporting to team leaders
Accountability Assistant director of nursing (ADN) Treatment team member and ADN
Client reporting Only shift Reports on past 24-h assessment of patients
VOLUME 24 | NUMBER 3 159
Copyright @ 20 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.10
ACKNOWLEDGMENT
The authors would like to acknowledge Nurse ManagersToni Battick, Patricia Billett, and clinical support of ElaineFitzgerald consulting APN. We would also like to thank Dr.Steven J. Schleifer who assistedwith editing and data analysis.
References1. Geller JL. The last half-century of psychiatric services as re-
flected in psychiatric services. Psychiatr Serv. 2000;51(1):41–67.2. Lamb HR. A century and a half of psychiatric rehabilitation
in theUnited States.Hosp Community Psychiatry. 1994;45(10):1015–1020.
3. Smith RC, Bartholomew T. Will hospitals recover? The im-plications of a recovery orientation. Am J Psychiatr Rehabil.2006;9(2):85–100.
4. Corrigan PW,McCracken SG. Interactive Staff Training: Reha-bilitation Teams That Work. New York: Plenum Press; 1997.
5. Birkmann JC, Sperduto JS, Smith RC, Gill KJ. A collaborativeapproach to the improvement of in client treatment for per-sons with psychiatric disability. Psychiatr Rehabil J. 2006;29(3):157–165.
6. Hogan MF. Interim Report of the president’s New FreedomCommission on Mental Health; 2002. http://www.MentalHealth.SAMSA.gov/publications/allpubs/government/default.asp. Accessed March 3, 2007.
7. Morris JA, Stuart GW. Training and education needs of
consumers, families, and front-line staff in behavioral healthpractice. Adm Policy Ment Health. 2002;29(4/5):377–402.
8. Fitzgerald E, Caldwell B, McQuaide T. Working together toimprove care: collaboration between a state psychiatric hospitaland an academic institution. J Psychosoc Nurs. 2005;43(7):31–36.
9. New Jersey Department of Human Services, Division ofMental Health Services wellness and recovery transformationstatement. Quarterly Newsletter. June 2006:1–3.
10. Deegan PE. Recovery and the conspiracy of hope. Transcriptof a presentation given at the 6th Annual Mental Health Ser-vices Conference, Australia, New Zealand, August 1996.
11. Lambert MJ, Barker DE. Research summary on the thera-peutic relationship and psychotherapeutic outcome. PsychotherTheory Res Pract Train. 1997;38:357–361.
12. Eben JD, Gashti NN, Nation MJ, Marriner-Tomey A,Nordmeyer SB, Dorothea E. Orem self-care deficit theory ofnursing. In:Marriner-Tomey A, ed.Nursing Theorist and TheirWork. St Louis, MO: CV Mosby Co; 1989:118–132.
13. Davis AJ, Underwood PR. The competency quagmire: clari-fication of the nursing perspective concerning the issues of com-petence and informed consent. Int J Nurs Stud. 1989;26(3):271–279.
14. Patrick V, Smith R, Schleifer S, Morris M, McClennan K.Facilitating discharge in psychiatric state institutions: a groupintervention strategy.Psychiatr Rehabil J. 2006;29(3):183–188.
15. Delaney KR, Johnson ME. Keeping the unit safe: mappingpsychiatric nursing skills. J Am Psychiatr Nurses Assoc. 2006;12(4):198–207.
Explore the views of the most provocative thinkers in nursing
with Advances in Nursing Science, the journal that pushes the boundaries of nursing scholarship. This thoughtful and thought-provoking journal offers a forum for critical analysis of nursing and healthcare and a stimulating challenge to everyday thinking.
• A single, timely theme across several articles in each issue
• The latest conceptual and theoretical thinking in nursing
• How social, cultural, and political issues andtrends influence healthcare
Consistently ranked one of the most read and most assigned journals by faculties of doctoral programs in nursingEditor: Peggy L. Chinn, PhD, RN, FAAN, Professor Emerita, University of Connecticut School of Nursing
© Wolters Kluwer Health/Lippincott Williams & Wilkins F7NIK175 A7K175ZZ
To subscribe, call TOLL FREE 1-800-638-3030 or go toNursingCenter.com or LWW.com/nursing.
CL IN ICAL NURSE SPEC IAL I STA160
Copyright @ 20 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.10





























