Embed Size (px)
Citation preview

ACTA
UNIVERSITATIS
UPSALIENSIS
UPPSALA
2008
Digital Comprehensive Summaries of Uppsala Dissertationsfrom the Faculty of Medicine 326
Compulsory Psychiatric Care:Perspectives from the SwedishCoercion Study
Patient Experiences, Documented Measures, Nextof Kins’ Attitudes and Outcome
TUULA WALLSTEN
ISSN 1651-6206ISBN 978-91-554-7149-1urn:nbn:se:uu:diva-8607

���������� �������� �� ������ �������� � �� �������� ������� � ���������������������������� ��� ��� ����������������� �! "� #$����%�� &������ '���� !"� �((" �� !)*!+,� �-� ������ , ���� , �-����-� .&������ , /������0� 1-� �������� 2��� ��������� � �2����-�
��������
3������� 1� �(("� �������� ����-������ ����* ������������ ,�� �-� �2����- ����������� ������ 4���������� �������� /�������� 5��� , 6��7 '�������� �� 8������'��� ����������� ���������� ������� ��� � ���� ����� � � ������� ���� ��������� �� ������� � � ����� )�9� 9) ��� ������� ��:5 � ";�!;++<; !<�;!�
1-� ��� , ����� � ����-����� ������ �������� ������ ������,��� ��-���� �� ����������������� 1-�� �-���� ��������� � ������� � ,���-�� ������� �� ���������� , ������������ ������� , �-�� �-�����������2� 2��- �(� ���������� �������� ����-������ ������� �� �(! ���������
�������� ������� �� ��+ , �-��� ��� , ��� 2��� ���,���� �� ������� ����-�� 2��-���� ,�� ������ �� ���������� ���� �� ��,�������� ���� 2�� �������� ����� �2��,,���� ������ , ���� 2��- � �������� ����-������ ���� ��2 ��,�� � ���2���4�������� , �� ����� � ������� ������� 2�� ��� ��� ����� ������� 2- -��
��� �������� ����� �-� ��� ����� ���������� 8�-��2��� �-��� 2��� ��,,������ ������� ���������� ����� �-� ��,,���� ��2�����=������ �-��;���� ����� 2�� ��������� 2��- -���� � ����� ���� �� �-� 2��� ��
���� ���=�������� ������� 2���� 1-��� 2��� �������-��� ���2�� ���=������ �� ������������� � ���2�� ����� ������� ��������� ����� �� ������� �� ���=������ � ������������������1-� �-���� ��������� -�� ����� �,,��� �-� ��������� , ������� �� ��� , ���
�2���� ������' ��=���� , ������� 2��� ���� � ���������� ��2�� �-� >����� 2-��-�� �-�� -�� ���
��������� �� ���� � � ����� � �����,�� �������� ������� 5����� , !!+ ������� ��������-�� -�� ��� ��������� �� ����� 4���� , �-��� ����� 2��� ���� ������� �� " ����� 2���,���� ��������� ������� �-� ��� ������� 2��� ,���� �-�� 2-� �� ���� � ������ ������� � ����-������
����� �-��� ��� ��������� ���������� ��,,������ ���2�� -2 �-��� ��� ��������� ������������ �� �-� ��,������ �� �� �-� ������� �� ���� �-�� �,,��� ���� � �-��� �-�,��� , ����-������ ����� � �-� ���� , ������� �� 2��� �� �-� ������ ���� , ����������������� -��� -�� ������� �,,�����
� ������ ���������� ������ ������� ��������� �������� , ������� ���� ������������-������ ����� ������� ��������� ��� , ���� �������� ��������� ���,;�����
����� ������ � � ��� �� �������� ! � ���� � ���������� �� � ������� ���� ����� �"#$%&'( )*�� �+� �� � �
? 1���� 3������ �(("
���5 !9+!;9�(9��:5 � ";�!;++<; !<�;!��*�*��*��*����;"9( .-���*@@��������@������A��B��*�*��*��*����;"9( 0

Original papers
This thesis is based on the following papers, referred to by their Roman numerals:
I. Wallsten, T.; Kjellin, L. Involuntarily and voluntarily admitted pa-tients' experiences of psychiatric admission and treatment - a compari-son before and after changed legislation in Sweden. European Psychia-try 2004; 19: 464-468.
II. Wallsten, T.; Kjellin, L. & Lindström, L. Short-term outcome of inpa-tient psychiatric care - impact of coercion and treatment characteris-tics. Social Psychiatry and Psychiatric Epidemiology 2006; 41: 975-980.
III. Wallsten, T.; Östman, M.; Sjöberg, R.L. & Kjellin, L. Patients and next of kins’ attitudes towards compulsory psychiatric care. Nordic Journal of Psychiatry. (In press).
IV. Wallsten, T.; Kjellin, L. & Sjöberg, R.L. The diagnostic accuracy of questions about past experiences of being mechanically restrained in a population of psychiatric patients. Memory. (In press).


Contents
Erik..................................................................................................................7
Introduction.....................................................................................................9 Epidemiology .............................................................................................9 Legal regulations ......................................................................................10
Mental health care legislation in Sweden ............................................10 Coercion ...................................................................................................12 The autonomy-beneficence-conflict.........................................................13 Ethical versus empirical questions ...........................................................15 Research on the reliability of retrospective self-reports...........................16 Perceived coercion ...................................................................................17 False negatives .........................................................................................18 False positives ..........................................................................................19 Attitudes to coercion ................................................................................20
Patient attitudes towards their own commitment.................................20 General attitudes towards coercion......................................................21
How compulsory psychiatric care may influence the mental health of the patient ..................................................................................22 Family burden and participation care.......................................................24
Background to the present thesis ..................................................................25
Aims..............................................................................................................26
Method ..........................................................................................................27 Materials...................................................................................................27 Interviews and data collection..................................................................31 Statistical analyses....................................................................................32 Samples and measures in paper I - IV......................................................32
Paper I..................................................................................................32 Paper II ................................................................................................32 Paper III ...............................................................................................33 Paper IV...............................................................................................33

Results...........................................................................................................34 Paper I ......................................................................................................34 Paper II .....................................................................................................35 Paper III....................................................................................................35
Next of kins .........................................................................................36 Paper IV ...................................................................................................36
Discussion .....................................................................................................38 Limitations and possible biases................................................................41
Deinstitutionalisation and Mental Health Care Reform ......................42 Power ...................................................................................................43
Summary of the results and conclusions.......................................................44
Appendix.......................................................................................................46 Interview questions. .................................................................................46 Paper I ......................................................................................................46 Paper II .....................................................................................................46 Paper III....................................................................................................47 Paper IV ...................................................................................................47
Sammanfattning på svenska..........................................................................48 Bakgrund ..................................................................................................48 Syfte .........................................................................................................50
Delarbete I ...........................................................................................50 Delarbete II ..........................................................................................50 Delarbete III.........................................................................................51 Delarbete IV ........................................................................................51
Konklusion ...............................................................................................52
Acknowledgments.........................................................................................53
References.....................................................................................................56

7
Erik
I met Erik some 15 years ago while working as senior psychiatric con-sultant. Erik was 40 years old and had been given the diagnosis schizophre-nia at about the age of 25. His mother and sister contacted the clinic to in-form us that he had begun to stay up all night, that he was playing music loud in his apartment during odd hours, and that the appearance of his apartment was gradually deteriorating. In addition he was becoming increas-ingly hostile towards some of his relatives.
When I met Erik, he informed me that he for several reasons no longer “believed in” medication. He explained that his reason for taking it for so long was not that he had felt that he needed it, but because he did not want to hurt the feelings of the personnel that had tried to convince him to use them. He furthermore felt that there were increasing problems with side effects, particularly physical unrest. Acknowledging having problems with anxiety he argued that alcohol, particularly beer, was a far better alleviator of these problems than antipsychotic drugs were. I pointed out that regular alcohol consumption may, among other things, impair social judgment, increase the risk for accidents and irresponsible behaviour and that it is associated with a risk for developing a pharmacological dependency on the drug. He agreed that this was usually the case, but stated that he, unlike other persons, was actually invulnerable to the potentially negative side effects of alcohol.
His relatives expressed concerns that his condition was deteriorating and that, if he were not committed to compulsory psychiatric care, he would run the risk of eventually hurting himself, become enable to manage his personal hygiene and to take care of the apartment that he had just moved into. I agreed that a period of psychiatric inpatient care might be good for Erik, but as I suggested this to him he became annoyed and explained that he was in no need of such care since he already had his own apartment and refused to discuss the issue further.
In this situation it was clear that Erik’s relatives and myself as a doctor had a different view than Erik himself when it came to the issue of whether a period of psychiatric inpatient care, would be good for him, for society and for his relatives. But since he, according to my medical opinion, did not pose a threat to his own life, the life of his relatives or anyone else, and since he did not have an absolute need for qualified psychiatric inpatient care, I had to follow the intention of the Swedish law. I had to respect the patient’s view

8
as the most important one, while closely monitoring further changes of his mental health condition.
Some 4-5 weeks later news reached me that Erik had destroyed his toilet, the walls and some furniture in his apartment by kicking it with the solid army boots that he was always wearing. He explained to me that he had been forced by circumstances to do this because destroying things made him feel powerful, and this feeling made him invulnerable to his anxiety. In this situa-tion I once more offered him an opportunity to be voluntarily admitted to psychiatric inpatient care. As he declined I informed him that I did not con-sider him capable of looking out for his own best interest in this situation and that I, in order to prevent him from harming himself, others or from fur-ther deterioration of his mental condition, was going make a referral for compulsory admission. As I told him this he tried to attack me. I quickly rose from my seat and closed the door behind me just in time to hear his solid camp boot hit the other side of the door with full force.

9
Introduction
Epidemiology The case of Eric illustrates one of many situations when a person may be
admitted to hospital for psychiatric care against his or her will. How frequent are such situations? On the 18th of May 2005 The Swedish National Board of Health and Welfare 1 surveyed psychiatric inpatients in Sweden. As part of the investigation, information was given regarding how many patients were admitted voluntarily, sentenced to compulsory care according to the Forensic Psychiatric Care Act (LRV) 2 or subject to civil commitment according to the Compulsory Psychiatric Care Act (LPT) 3.
Even though these numbers as suggested by the authors of the report should be treated with some caution the results suggest that some 855 pa-tients (roughly about 0.01% of the current Swedish population or 9,5 /100 000 individuals) were given compulsory psychiatric inpatient treatment ac-cording to the LPT 3 at this particular given point in time. However, on the same day, an almost equal number of patients were reported to be on leave from compulsory psychiatric care.
Salize and Dressing found in a study of involuntary placement of men-tally ill people across the European Union (EU) during the 1990s, that the total number of compulsory admissions varied, and they also found a re-markable difference in commitment rates (annual number of admissions per 100 000 population) and quotas (percentage of all psychiatric admissions). The compulsory admission rates ranged from 6 annual compulsory admis-sions per 100 000 in Portugal to 218 in Finland. This strongly hints differ-ences in definitions, legal backgrounds and/or procedures 4. If compulsory admissions are considered in isolation, the total number was increasing in Germany, France, England, Austria, Finland and Sweden. The mean length of in-patient stay has been shortened according to the internationally chang-ing patterns of mental health care delivery which may have caused more frequent readmissions 4 5. Priebe et al studied whether reinstitutionalisation is occurring in mental health care and, if so, with what variation in six different European countries. The major characteristics of reinstituionalisation are the rising number of forensic beds, involuntary hospital admissions and places in supported housing. They found that forensic beds and places in supported housing had increased in all countries. They also found that the involuntary admissions had increased in England, the Netherlands, and, especially, in

10
Germany. The reduction in the number of psychiatric beds was greater than the total number of additional forensic beds and places in supported housing established at the same period in time. The increased number of supported housing and forensic beds was much greater than any decrease in conven-tional psychiatric bed numbers in Italy and the Netherlands 5.
In Sweden, the decrease of psychiatric hospital beds was found to be 65% and the decrease of involuntary admissions was 17% between 1990 and 2001. However, an increase was found in forensic beds of 46% between the same years. There was also an increase of supported housing of 15% be-tween 1997 and 2002. The prison population increased 16% between 1992 and 2002 5.
In this thesis some of the experiences of involuntarily and voluntarily ad-mitted patients and their relatives involved in the patients care will be de-scribed. Forensic patients and persons in prison are not studied in this thesis.
Legal regulations Worldwide the use of compulsory psychiatric care is strictly regulated
both according to international conventions such as the Declaration of Ha-waii 6 and the declaration of Madrid 7 and in national legislation. Prior to 1969, most legal frameworks stipulated that a given need for treatment was used as standard for compulsory admission. In some countries harm to the patient him/herself is included as a prerequisite to compulsory admission, while other countries also include harm to the public. Danger to oneself or others is a common criterion across the European Union (EU), but it is not an explicit prerequisite in Italy, Spain or Sweden 4 8.
The definition of mental disorder as a reason for involuntary treatment varies from psychosis, mental illness and psychopathic disorders, the latter being used in United Kingdom 4. Though the details of regulations may vary they all agree that only patients that suffer from serious mental disorders and who may cause harm to themselves or others may be subjected to compul-sory psychiatric care.
Revisions of the mental health legislations in Western countries have re-stricted the criterion for involuntarily admissions and extended the proce-dural safeguards. The purpose of these changes has been to reduce involun-tary care.
Mental health care legislation in Sweden At the end of the 19th century, a discussion started about the legal secu-
rity of the mentally ill patient in Sweden. In 1913 a committee was ap-pointed with the task of examining the current legislation which resulted in

11
the Act on regarding mentally ill persons of 1929 9. The act declared that admission to a mental hospital should be based on whether the individual had a need for care. The patient him/herself could request admission. How-ever, even if admission occurred on a voluntary basis, the patient ran the risk of being detained by force. The right of detention of voluntarily admitted patients was not abolished until 1959a.
The Act on regarding mentally ill persons was replaced in 1967 by Com-pulsory Mental Care [Certain Cases] Act (LSPV) 10. With LSPV the legal security of the patients was improved further. A central criterion for compul-sory care was that the individual should be suffering from a mental illness. In 1982 Sweden passed a general Act on Health and Medical Care (HSL) 11 in which it is emphasised that the basis of all medical care is voluntariness and consent. The autonomy and integrity of the patient has to be respected.
During the 1980s there was intense public controversy in Sweden as to whether Swedish psychiatrists tended to over-use or even abuse the option of involuntary care in clinical decision-making in order to control deviant indi-viduals and enforce conformity, for details see 12. Even though LSPV was considered as a major improvement in terms of legal safeguards for the pa-tients, questions concerning patient rights were highlighted in the following years’ debate about psychiatry. The Social Affairs Commission presented a report, entitled Psychiatry, Compulsion and Legal Security 13, suggesting a new legislation for compulsory psychiatric care. An ideological shift was evident in the report which appeared to be influenced by the debate about psychiatry in the 1960s and 1970s. The role of mental hospitals was ques-tioned. The increased interest in patients’ rights expressed in the report could be seen as one theme in the new way of conceiving of psychiatry.
In its evaluation of LSPV, the Social Affairs Commission concluded that the intentions behind the LSPV had not been realised. In psychiatry, there was a long tradition of coercion and social control. There was a tremendous regional variation in the use of LSPV, which was considered an indication of failure to provide all patients with equal rights 13. The differences could be understood in terms of local traditions and organisational variables. Where large mental hospitals existed, the rate of compulsory treatment tended to be more frequent 14. In the wave of this debate and after years of deliberations, LSPV was in 1992 replaced by new legislation: LPT and LRV 2 3. By LPT a new concept was introduced to identify those liable to compulsory care: instead of mental illness, the patient suffers from a severe mental disorder. The new concept was designed to signal a shift from a biological and medi-cal understanding of the patient’s problems, towards a more ”dynamic” the-ory, which also incorporated psychological and social components. It was
a Since 1983, there are legal rules for “konvertering” (conversion), i.e. detainment of voluntar-ily admitted patients.

12
also emphasised that the patients should have as much say as possible in treatment issues, even under compulsory care 3 15.
In the LSPV, the medical indication could be used when a patient dis-played an obvious lack of insight into his/her illness at the same time as there was a risk that his/her condition would deteriorate unless he/she was hospitalised or alternatively an improvement could be expected if he /she was given treatment.
According to LPT, compulsory psychiatric care is only permissible if the patient suffers from a severe mental disorder, there is an absolute need for full-time psychiatric care, and the patient refuses voluntary psychiatric care, whereas the needs to protect the public is given less weight. Furthermore, even though decisions about compulsory care according to the new legisla-tion are made by physicians they have to be tried by courts of law if they are to be extended for a period longer than 4 weeks 3 15.
Compulsory care according to LPT shall have the purpose of making a person, who has an indispensable need of the psychiatric care that is pro-vided after admission to a psychiatric clinic, capable of voluntarily taking part in the required treatment and receiving the necessary support 3 15.
The procedure for deciding about compulsory psychiatric care is sur-rounded by strict regulations, as well as a continuing debate and controversy. The reason is that it more or less invariably involves a conflict between the perspectives of the patient and of representatives of the psychiatric and/or legal systems. This conflict which sometimes, as in the case of Erik, may even bring the parties to resort to physical confrontations, mirrors an ethical conflict that lies at the heart of the issue of compulsory psychiatric care.
Coercion Coercion will in this thesis be defined as a situation in which the patient is
deprived of his or her influence over clinical decisions pertaining to his or her psychiatric care. Furthermore, in this thesis legal coercion refers to coer-cion defined by legal parameters, whereas perceived coercion refers to coer-cion as subjectively experienced by the patient 8 16-23.
In the psychiatric context, a distinction is made between coercion at ad-mission to psychiatric inpatient care and coercion during the subsequent inpatient care episode. Coercion during inpatient care can furthermore be divided into coercive measures and coercive treatments. Coercive treatments are intended to treat, help or cure the patient regardless of the patient’s resis-tance, while coercive measures like restraint and seclusion are primarily used to control agitated and violent behaviour. Not only coercion at admission, but also the use of coercive treatment and coercive measures during care are strictly regulated in the LPT. Most inpatient care episodes go on, however, without the use of any coercive treatment and measures.

13
In modern societies, the use of psychiatric coercion implies a fundamental ethical conflict between the right of the individual to decide over his own fate and the obligation of the psychiatrist to do what is best for the patient and to avoid harming him or her, his or her next of kins and/or society. In textbooks of medical ethics (e.g. 24) this is described as a conflict between the principles of Autonomy and Beneficence.
The autonomy-beneficence-conflict The principle of autonomy is often referred to the 18th century German
philosopher Immanuel Kant (1724-1804). According to Kant a person is choosing autonomously when he or she chooses something as a pure act of will, on the basis of impersonal general laws, not on the basis of his or her desires and wishes 25. When this is the case, autonomy is an inherently good thing. However, it should be noted that Kant argues that human choices are worthy of respect, and genuinely autonomous, only if they are not con-strained by the agent’s own desires or conceptions of the good: if they are based on recognition of what is objectively good as such, as determined by universal moral principles.
In an elaboration of these ideas, more in line with our contemporary use of the concept, John Stuart Mill (1806-1873) argued that “the only purpose for which power can be rightfully exercised over any member of a civilized community, against his will, is to prevent harm to others” 26. According to Mill a psychiatric patient like Erik has a right to have even decisions that may seem crazy (like destroying the walls and toilet in order to reduce anxi-ety) respected as long as he does not hurt others. That is, maintaining and defending such rights, even when the bearers of these rights chose to execute them in apparently bizarre ways is an inherently good thingb 24 27.
However, the health care sector does not have as its sole purpose to de-fend the autonomy of the patients. Beauchamp and Childress has proposed a pragmatic analytical approach that examines the roles of four main ethical principles that they mean are part of a ”common morality” shared by ”all morally serious persons”, whatever the underlying philosophical or religious commitments of those persons 24.
Among these is the principle of autonomy which requires the health care professional always to acknowledge and carry out the value-based prefer-ences of others regardless of what one thinks the consequences of doing so might be. However, also the principles of nonmaleficence and beneficence
b Mill adds, however, that those who are too young, retarded or disturbed, or temporarily lack the capacity for autonomous decisions, should not be allowed to refuse beneficial treatment . Much has been written about competence for making decisions, but a further discussion of this concept is beyond the scope of this thesis.

14
according to which the health care professional is required to avoid harm and to act in a way that is expected reliably to produce the greatest balance of goods over harms in the lives of othersc. In practice moral decision-making involves a process of specification of the principles’ implications in the par-ticular situation and balancing the relative importance of the principles if they conflict. Though ethics is a complicated and ultimately subjectively based branch of philosophy, the pragmatic approach of basing ethical deci-sion-making on the foundation provided by this (or some kind of similar) set of principles has become a widely accepted and useful way of dealing with ethical issues in the health care sector 28-30 and it is the foundation on which further reasoning will rely in this thesis.
As discussed above, compulsory psychiatric care occurs, when the psy-chiatric and legal system decide to provide care to a patient, regardless of the known preferences of the patient with the goal of benefiting the patient or avoiding harm to the patient, others and/or societies.
Figure 1. Decisions about compulsory psychiatric care involve a difficult balance between different ethical principles. c A fourth principle is justice, which is also relevant when discussing coercive care but not a topic for the present thesis.

15
This implies a conflict between the principle of autonomy and the princi-ples of beneficence (Figure 1). The idea that there are situations in which certain individuals, such as physicians, may have to override the preferences and wishes of patients in order to do good to him or her may be referred to as “medical paternalism” 31. The idea that this may be justified in order to do good to others and society may be referred to as “social paternalism” 32.
Ethical versus empirical questions In cases involving decisions about compulsory medical care, such as that
of Erik presented at the beginning of this text, we may assume that an ethical conflict exists between the principles of autonomy and beneficence. It may further be argued that the responsibility of the psychiatrist in this situation is to balance these principles against one another, and then make a decision based on sound ethical reasoning and the legal framework provided by soci-ety. However, it should be noted that such reasoning is also highly depend-ent on the state of empirical knowledge in the field. In fact, even the mere idea that a conflict exists in such a case, relies on assumptions regarding empirical questions. So for instance, in the case of Erik, it may be argued that there is a conflict between the respects for Erik’s right to manage his anxiety in any way he may please and the need to offer him a secure envi-ronment and an efficient psychiatric treatment for his condition. How can we even know that the kind of care we would have been able to offer him actu-ally would have been successful? What constitutes success in this context anyway? Should it be measured in terms of how patients experience the psy-chiatric care, or in patient attitudes to it afterwards? Would the attitudes of next of kins be a more interesting measure? Should patients’ or psychiatrists’ assessments of global functioning be used?
The way ethical reasoning and ethical decision-making applies to real life situations in general, and real life situations involving decisions on compul-sory care in particular, are highly dependent on the answers researchers are able to give to these kinds of questions. However, such research requires the use of decisions on compulsory care and/or aspects of such care (such as legislation on compulsory care, or variations in how compulsory care is ad-ministered) as an independent variable. Obviously performing such research raises a number of both ethical and practical questions. So for instance in most other fields of clinical medicine, the study of a common but highly controversial treatment, would normally lead to the design and execution of a number of randomized clinical trials to study outcomes. But since it is re-garded as unethical to expose a person to coercion if it is not absolutely nec-essary, randomization is very difficult to perform for ethical reasons. Conse-quently researchers have for a long time seemed to almost have given up on doing something useful in this field of study. However, during the last 20

16
years or so, a number of efforts have been made to correct this state of af-fairs.
In addition to shedding some light on the relation between aspects of compulsory care and outcome, this research has also led to the discovery of another important feature or general principle that applies to the compulsory care situation, and echoes findings made for instance within the field of memory research during the last 20 years, namely that the views of the psy-chiatrist and the psychiatric system and of the patient are often diverging, even when it comes to describing the very same situation.
This is the reason for the need to distinguish between perceived coercion and other forms of coercion, and an understanding of this problem is neces-sary for the understanding of this field of research in general. Before dis-cussing the relation between compulsory care and outcome it is thus relevant to discuss this finding.
Research on the reliability of retrospective self-reports During the last decades, the reliability of accounts of past, unpleasant ex-
periences have been the subject of considerable debate not only in the con-text of research on compulsory psychiatric care 33-46. One important reason for this has been an increased demand for empirical understanding of memo-ries for emotionally traumatic events. In the 1950s some researchers believed that a memory was like “a strip of cinematographic film with sound-track” that is set in motion at the time of memory retrieval 47. However, current knowledge suggests that memory more resembles a synthesis of experiences than a replay of a videotape, which implies that memory can also be drasti-cally changed or even created 48. As a consequence people tend to differ in their memory of past experiences, even when it comes to memories of the same event.
So for instance, even though memory for past experiences most often tends to work without problems, we all tend to lose important aspects of memories retrospectively (false negatives), but may also under some circum-stances remember events that never occurred (false positives). Individuals may furthermore differ in their perception and understanding of events due to differences in perspectives, personality or the influence of factors such as drugs or level of consciousness (i.e. head trauma). Finally people may some-times consciously withhold or distort information about past experiences when giving them to interviewers or interrogators.

17
Perceived coercion For researchers on compulsory psychiatric care the fact that descriptions
of the past vary widely depending on the source of information (e.g. patient or psychiatrist) is a very salient feature, providing the rationale for the com-mon practice amongst researchers to differentiate between “perceived coer-cion” and coercion as defined by care-givers or the legal system.
In one study of the consistency between measures of perceived and legal coercion Poulsen and Engberg asked 143 Danish psychiatric inpatients ques-tions such as: Right now, are you in the ward out of your own free will?; Was this admission voluntary/involuntary?; Have you experienced restric-tions in leaving the ward?; Do you take medication against your own will?. When comparing the answers with information in medical files agreement rates between 67% and 87% were found with some aspects of strikingly low agreement. For instance, the positive predictive value (the likelihood that a statement of being coerced was consistent with medical files) of statements of forced medication was 38%. Inconsistencies between self-reports and medical files were more common amongst psychotic patients and it seems reasonable to assume that some of these inconsistencies were caused by mis-understandings between the personnel and the patients 49. Similar findings of low consistency between self reported coercion and formal coercion has been described in other studies 8 18 19 21-23 50-53.
None of these studies suggests that the accounts provided in medical files should be considered as the gold standard, since many coercion related in-terventions may not be documented or documented in a way that may make important contextual aspects of them hard to interpret retrospectively. Lidz et al, when trying to circumvent the problem of a lack of a gold standard for what actually happened, decided to relate the information given by patients and other informants by creating a “Most Plausible Factual Account” (MPFA) of what happened during a treatment episode. When doing so they found that patients self reports corresponded fairly well to this measure as compared to those of other informants. However, a limitation of this ap-proach is obviously that the decisions made about how such an account should be constructed are to a considerable extent subjective in themselves 54.
Put simply, it can be argued that there are three potential sources of dis-crepancies between patient and psychiatrist descriptions of incidents of coer-cion that may emanate from the patient. First, there is the possibility that the patient interprets and understands the situation differently than the psychia-trist. Second, there is the possibility that the patient does not remember or report a past experience that actually did occur (false negative) and third, there is the corresponding possibility that the patient remembers or reports an event that did not occur (false positive).

18
The idea that some of the discrepancies may be caused by different under-standings of the situation has suggested the approach of studying aspects of the care giving situation that may influence perceived coercion.
So for instance empirical research during the 1990s has found that pa-tient’s experiences of not having ones will respected, not being listened to or more seriously being subject to shows of force (an act that demonstrates the availability of force, if it is needed, such as calling the police or hospital security) during a treatment episode, may increase the extent to which the patient perceives himself or herself as having been coerced 20 54-56.
Another factor that may influence perceived coercion is the extent to which the patient perceives the system and principles according to which they are treated as just and legitimate. So for instance results from one ex-perimental study in which psychiatric patients were exposed to videos de-scribing mock hearings concerning compulsory commitment suggested that patients are indeed sensitive to procedural justice issues and that these issues are also important to their attitudes towards psychiatric care 57. Perceptions of procedural justice has also been found to be important for how patient’s perceive their own admissions and this concept has thus become important in discussions on how to improve compulsory psychiatric inpatient care20.
Bonsack and Borgeat showed that clinicians could decrease feelings of coercion of their patients while discussing need for hospitalization, legal status and subjective feeling of coercion as different dimensions50.
The fact that such aspects of the care giving situation influence perceived coercion supports the notion that differences in the understanding and inter-pretation of a situation may explain some discrepancies between clinicians and patients. Also, importantly, it suggests ways to possibly reduce levels of perceived coercion that should be used for ethical reasons or because coer-cion may reduce adherence to treatment 55.
False negatives Sometimes people who have experienced highly unpleasant things in the
past (such as for instance sexual assaults) fail to report these events when later asked for them by researchers, law enforcement officers, social work-ers, friends or relatives 58-61. There are several possible reasons for this, such as normal forgetting, embarrassment or influence by drugs or by head trauma 58 59 62-64. Finally there is also the highly controversial 65 and empiri-cally relatively unsupported idea of “repression”, “psychogenic” or “disso-ciative” amnesia as a source of forgetting of “traumatic memories” 66 67. The extent to which people falsely deny salient and highly unpleasant past ex-periences varies between studies and most likely also for the kind of events concerned. As noted above, memories for past experiences of child sexual abuse has been one of the most studied past events in this respect, with dis-

19
closure rates varying between 16% and 50% in different studies and samples 59-61. It may be reasonable to assume that non-disclosures because of shame and embarrassment may be particularly high in this group. However, non disclosures for other reasons such as distorted sense of reality due to drug effects, psychosis etc may be more prevalent when it comes to memories of past experiences of compulsory psychiatric care.
False positives In the beginning of the 1990s researchers using a number of different
paradigms were able to demonstrate that false memories for highly salient and unpleasant events could not only be created in a laboratory setting 35 43 45
68, but had also in some particular historical contexts most likely occurred in a number of large scale events outside the laboratories of experimental psy-chologists 38 40 58 69-71. The extent to which such false positives are common in everyday situation is still subject to debate and controversy 72.
From a memory research point of view, the source monitoring theory 73 74 probably provides the most influential account for how false memories emerge. According to this theory we identify sources for our memories in the course of retrieving themd. At this instance memories from internal sources (e.g. thoughts, feelings) are distinguished from memories from external ones (e.g. seeing, reading) on the basis of characteristics of the memory trace, such as for instance the amount and nature of intellectual cognitive opera-tions vs. the amount of perceptual detail. Many source monitoring decisions are made rapidly and unconsciously, without any awareness of a decision making process, while others involve a more conscious strategic decision making process. When either the decision-making process or characteristics of the memory are influenced confusions of sources may occur which may create illusory memories. One possible source of such influence that was much discussed during the earlier part of the 1990s, were certain forms of psychotherapeutic treatment. In clinical settings with patients that may be psychotic with delusions or with severe depressive symptoms, other poten-tial of source monitoring influence may be the psychiatric disease itself, particularly psychotic disorders, which are known to cause a number of cog-nitive deficits in many patients. Another source of such influence may be psychopharmacological treatment and also possibly the ward milieu with its different impressions on the patient. Patients with delusions and hallucina-tions may for example have a disruptive failure in source remembering as delusions and hallucinations involve loss of control of thoughts. In these
d Memory is amongst researchers typically defined as the process of encoding storage and retrieval of information. Memory is furthermore commonly divided into several subsystems. The discussion above refers to ”episodic” or ”declarative” memories.

20
situations thoughts come up automatically, or unbidden. The delusive thoughts may produce little reflective cognitive-operations information and may be easy to confuse with external stimuli.
Attitudes to coercion In order for psychiatric coercion to occur according to current Swedish
legislation there is assumed to be a negative attitude towards a patient’s own involuntary admission. Research on attitudes has a long and complicated history in psychological science. Of particular importance has been the rela-tion between attitudes and behaviour for instance in health research 75. Sum-marizing this research one textbook in social psychology describes an atti-tude as:
“…a hypothetical mediating variable assumed to intervene between stimu-lus and response. Attitudes involve at least an evaluation of the attitude ob-ject, and many definitions also include cognitions and behavioural tenden-cies” 76.
However, researchers dealing with attitudes towards compulsory psychi-atric care have not so much focused on attitudes as a predictor of behaviour but more on the evaluative opinions of patients, professionals and next of kins concerning both their experiences of specific incidents of compulsory psychiatric care 21 77-79 and the phenomenon of psychiatric care in a more general and abstract perspective 80.
Patient attitudes towards their own commitment Patients’ attitudes towards involuntary commitment are an area of interest
because patients are consumers to health service, and consumer satisfaction is of importance of health care in general. The positive attitude of patients towards commitment correlates with better response to treatment 81.
In an early study of patient attitudes towards their own admissions, Toews et al found that patients tended to be more appreciative of the need to admit them some time after the incident than during it 82. Patient perceptions of having been kept properly informed and treated in a respectful manner was furthermore associated with a more positive attitude towards psychiatric coercion in general. In another study Edelsohn and Hiday found that a ma-jority of patients interviewed six months after discharge found their com-mitment as helpful and necessary and even wanted to be committed again if they would become sick and dangerous in the future 83. However 46% de-scribed the treatment episode as definitely depressing and 41% as unpleas-ant. In a Swedish study of patient satisfaction it was found that half of the involuntarily admitted patients regarded their own experience of compulsory

21
treatment as wrong and unnecessary while 28% rated it as good and neces-sary 84.
In a study of retrospective attitudes to injections and restraint, including schizophrenic patients, interviewed after 60-80 days from discharge, almost half of the patients had retrospectively positive attitudes to the coercive measures and only 23% rejected them 85.
However, not all studies support the view of the grateful psychiatric pa-tient. Gardner et al concluded that perception of coercion were stable from admission to follow up four to eight weeks after discharge. In this study some patients changed their minds about the need for involuntary hospitali-sation but this did not result in forgetting or forgiving the use of coercion 86. They also found that patients who believed that they did not need hospitali-sation tended to perceive that they were 1) more coercively treated 2) subject to forceful and threatening pressure to be admitted, and 3) treated with less procedural justice.
Anxiety, anger and helplessness are reported by patients who have been committed even though coercive interventions were viewed favourably af-terwards 85. Events that have been perceived as severely stressful are being forced to remain at a close ward, side effects of medication and feelings of helplessness. Other adverse consequences were negative psychological se-quels such as loss of confidence or fear of relapse, loss of independence, loss of custody of children or fewer social contacts 87. Patients wanted to be re-spected in their beliefs about how commitment could be avoided, e.g., more understanding, supportive and corrective behaviour (opposed to confronta-tive, non-individualized approaches) on the part of hospital staff and after admission, and more understanding and supportive behaviour on the part of relatives, neighbours or police before admission 87.
General attitudes towards coercion Previous research on general attitudes to compulsory psychiatric care has
studied public attitudes 88, but also attitudes among mental health profes-sionals and patients 89-91. In a Swiss study by Lauber et al, assessing the public attitude to compulsory admission, more than 70% of the respondents had a positive attitude to compulsory admission 88. Patients with and without treatment experience showed about the same percentage of agreement with compulsory admission as did the general population 92. However, there are also a number of studies to suggest that the role an individual plays in rela-tion to the phenomenon of compulsory care (i.e. patient, next of kin, profes-sional or general public with or without experience of compulsory care) may be important for general attitudes towards the phenomenon 90 93.
The legal framework, the clinical practice, public opinion, and attitudes of patients, professionals and relatives are likely to interact. One of the main changes in 1992 when the former LSPV (Compulsory Mental Care [Certain

22
Cases] Act) of 1967 was replaced by the LPT (Compulsory Psychiatric Care Act) was the introduction of legal proceedings for matters, which previously could be decided exclusively by a doctor. In the LPT, need of treatment cri-teria are emphasised, and the aim of involuntarily admitting a patient should be to make the patient comply with voluntary treatment. Treatment should be given, as far as possible, in co-operation with the patient and with rela-tives 15. Kjellin and Nilstun found discrepancies between the law reform in Sweden and the attitudes of different groups of people involved in or af-fected by civil commitment. A large majority of all groups stated that doc-tors and not the judicial process should decide about involuntary admissions, and there was strong support for coercion in the interest of others. However, the study was conducted before the LPT came into force 32.
How compulsory psychiatric care may influence the mental health of the patient
The question of whether coercion may positively or negatively influence the mental heath of the patient has been the subject of discussion and debate at least since the late 18th century. At this time the French psychiatrist Phil-ippe Pinel (1745-1826) argued that even though coercion may be necessary and justified in some cases, cruel treatment may also do psychological harm to patients 94. A related question, also raised by Pinel and also addressed by much late 20th century research, as discussed above, was whether measures taken to give coercion a more human face (maintaining a respectful attitude, informing patients etc) may alleviate perceived coercion and thus also possi-ble harmful effects of it.
From a scientific point of view a study of the effects of coercion should ideally be randomized so that some patients that may need compulsory psy-chiatric care were given it and others not. However, because of the ethical difficulties of conducting research in this way on compulsory treatment most studies have had to rely on other methods, consequently with a greater level of insecurity regarding the results.
In a rare example of a randomized study of the outcome of coercion, Swartz et al compared the effects of outpatient commitment (OPC) to ad-herence to community based mental health treatment (taking medication and scheduled appointment) 95. Patients with severe mental disorders have diffi-culties in adherence to prescribed outpatient treatment in the community. It is known that schizophrenic patients often have low adherence to antipsy-chotic medication 96 which is associated with poor outcome like readmission to hospital, drug abuse and violence 97 98. In the Swartz et al study patients volunteered to be randomized either to outpatient commitment or to be re-leased without outpatient commitment. A non-randomized group with a his-

23
tory of serious violence was also studied under outpatient commitment. However, despite the impressive study design, the results remained incon-clusive as to what treatment modality should be recommended 95. The impact of outpatient commitment on for example involuntarily readmission rates are unclear 99. Outpatient commitment is not yet a legal option in Sweden, but a proposal introducing this possibility as law has recently been presented by the governmente.
In a study of outcome in relation to coercion as perceived by patients, Svensson and Hansson found the perceived coercion group less satisfied with care including staff-patient relationship, information and influence. They also scored a lower global improvement during care 84. Nicholson et al found that patients that reported higher levels of coercion during admission had higher levels of functioning at discharge 56. In a study on ethical benefits and costs of coercion Kjellin et al found an association between being re-spected and positive outcome 100. Self-reported outcome of psychiatric inpa-tient care has been shown to differ from outcome systematically assessed by professionals 56 100. Similarly, Steinert and Schmid, found that short-term outcome of inpatient treatment, was independent of whether treatment was legally involuntary or voluntary 101.
Katsakou and Priebe assessed 18 papers on the outcome of involuntary hospital admissions in general adult psychiatry and found that most patients showed significant clinical improvement (observer rated clinical change) after involuntary treatment. In the review, data on predictors was limited and inconsistent. Different evaluation instruments have been used regarding sub-jective and objective improvement and the times of assessment across the different studies varied and it is difficult to compare studies where different inclusion criteria (regarding diagnosis, age, etc.) are used. There is still little research on the impact of coercion on treatment outcome, and there are many confounding factors when outcome of coercion is studied.102.
Furthermore, little is known about the outcome of brief inpatient treat-ment interventions in general in routine psychiatric practice and associated patient and treatment characteristics 103. For example, it is common practice in Swedish psychiatry to appoint a contact person for each patient during inpatient care, and according to the LPT a treatment plan should be estab-lished in co-operation with the patient and his next of kins. Patient experi-ences and the effects of such efforts are not known.
e Lagrådsremiss Ny vårdform inom den psykiatriska tvångsvården Stockholm den 17 januari 2008.

24
Family burden and participation care Mental illness obviously primarily affects the life of the individual suffer-
ing from the mental disorder, but it also has consequences for next of kin. Family burden is a concept that can be defined as the negative impact that living with a relative suffering from a mental disorder has on caregivers. This phenomenon, which has been studied since the 1950s, includes objec-tive aspects (i.e. observable effects such as income) and subjective aspects (i.e. negative psychological impact) 104 105. Caregiving is burdensome and Perlick et al found that 54% of family members of people with bipolar ill-ness reported severe levels of burden 106. The psychological burden on rela-tives is often considerable. So, for instance, partners of individuals with a psychiatric diagnosis are at increased risk of developing a depressive disor-der 107 108. In a study by Östman and Hanson, relatives of both voluntarily and involuntarily admitted patients were found to have a considerable amount of burden and different subgroups (parents, spouses and grown-up children) of relatives experienced the burden in different ways. Grown-up children experienced more internal burden and more mental disturbance of their own while the parents were more concerned about the patient attempt-ing suicide. More often spouses showed a greater external burden. No sig-nificant differences in family burden were found between relatives of the voluntarily and involuntarily admitted patients. Only a minor proportion of the relatives were exposed to physical violence. Regarding the psychological internal burden, almost half of the relatives were concerned that the patient should harm himself through suicide or suicide attempts. About half of the relatives experienced mental health problems of their own. Relatives of vol-untarily admitted patients more often experienced sufficient participation in the patient’s treatment, which may be of some clinical use as treatment of compulsorily admitted patients in psychiatric services ought to render more and not less participation for the family 107.
Nordström, studying violent male offenders with schizophrenia and their relatives found that although parents were not living with their adult sons they were much emotionally involved with them. Since next of kins are often involved in the every day life of the person, their attitudes towards compul-sory psychiatric care are potentially important 109.

25
Background to the present thesis
In the first half of the 1980s the Swedish County Council of Söder-manland started to close down the Sundby mental hospital. As the County Council of Västmanland never had a mental hospital of its own and the pa-tients in need of compulsory mental health care were sent to mental hospitals such as Sundby and Säter ( in another neighbouring county) an intensive planning for “taking home” the patients from Säter and Sundby started in Västmanland. One of the most important aspects of the planned change was the development of evidence based routines for the handling of compulsory psychiatric care. However, at that time not much systematic research was found in this field, either in Sweden or internationally. Most importantly there was a lack of research on patients’, relatives and staff experiences of compulsory care.
In order to make amends for this an interview- and survey study was per-formed as a collaboration between researchers from the County Councils of Västmanland and Uppsala during the mid 1980s (Lars Kjellin, personal communication). In this study patients subjected to either compulsory care or voluntary care were included. Also included were relatives to these patients. During the 1990s two similar waves of data collection were performed be-fore and after the change of legislation on compulsory psychiatric care in 1992. The first time as a collaboration between Västmanland and Uppsala and the second time as a larger multicenter study involving three additional Swedish counties, Älvsborg, Västerbotten and Kristianstad. Data from these two later investigations of the Swedish coercion study provide the empirical basis for the present thesis.

26
Aims
The main objectives of the present thesis were -to compare patients’ experiences of care during two different laws of
compulsory care, LSPV and LPT, focusing on the aims of the law reform and some of the main legal changes,
-to investigate whether legal and perceived coercion, and other features of short-term psychiatric in-patient care, were associated to treatment outcome,
-to investigate whether a change in legislation was reflected in patients’ and next of kins’ attitudes towards coercive treatment,
-to describe and further explore differences between coercion as well as treatment related parameters as perceived by patients and the same parame-ters as reported by other sources.

27
Method
Materials As described above the empirical basis for the present thesis was two
studies within the Swedish coercion study on compulsorily and voluntarily admitted psychiatric patients. The first was performed in the counties of Västmanland and Uppsala in 1991 and the second one in the counties of Älvsborg, Västerbotten, Kristianstad and Västmanland in 1997-1999.
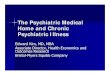
In both studies exclusion criteria were: age less than 18 and more than 70 years; a main diagnosis of substance abuse; severe mental retardation; sen-tenced to care; severe dementia and not able to communicate in Swedish. Also excluded were those patients not living in the catchments areas. Exclu-sions and dropouts of different stages of the process are described in Figures 2-3 and the samples used in the four different studies presented below are specified in Table 1. Committed patients were included in the study consecu-tively, and a corresponding number of voluntarily admitted patients were consecutively randomised either to take part of the study or not to.
Of excluded patients in 1997-1999, more than 60% were excluded due to a primary diagnosis of substance abuse and 25% because they were younger than 18 or older than 69 years. Some of the eligible patients were not con-tacted because the interviewers did not manage to get in touch with them within five days from admission. Of patients asked to participate, 13% of both patient groups in 1991, and 30% of committed and 20% of voluntarily admitted patients in 1997-1999, declined. The dropouts (patients not con-tacted and refusing patients) and the participating patients did not differ in age and sex, except for committed patients in 1991 where there were more female patients among the dropouts than among the interviewees. Another 11-19% of the patients were lost at the follow-up since they could not be reached or did not want to participate in another interview (Figure 2-3). Among remaining patients, included in the studies of the present thesis, there were less psychoses and more other diagnoses, and higher Brief Psychiatric Rating Scales (BPRS) 110 total score at admission, in 1997-1999 than in 1991 (Table 1).

28
1991 1997-1999
Involuntarily admitted patients during study period
229
Eligible for inclusion 116
Excluded 113
Interviewed at admission 95
Dropouts at follow up
11
Not contacted 7 Refused to participate 14
21
Interviewed at discharge/3 weeks
84
No relatives or No consent from patient
or relatives 31
Interviewed 64
Next of kins 95
Involuntarily admitted patients during study period
568
Eligible for inclusion 251
Excluded 317
Interviewed at admission 138
Dropouts at follow up
20
Not contacted 55 Refused toparticipate58
113
Interviewed at discharge/3 weeks
118
No relatives or No consent from patient
or relatives 65
Interviewed 73
Next of kins 118
Figure 2 Flowchart. Involuntarily admitted patients in 1991 and 1997-1999. Drop-outs and patients included in the first interview within five days and the follow-up interview at discharge or after three weeks. Next of kins, dropouts and those inter-viewed.

29
1991 1997-1999Voluntarily admitted patients
during study period 2282
Eligible for inclusion 841
Random sample 120
Excluded 1441
Interviewed at admission 94
Dropouts at follow up
10
Not contacted 12 Refused to participate 14
26
Interviewed at discharge/3 weeks
84
No relatives or No consent from patient
or relatives 25
Interviewed 69
Next of kins 94
Voluntarily admitted patients during study period
4636
Eligible for inclusion 2215
Random sample 274
Excluded 2421
Interviewed at admission 144
Dropouts at follow up
27
Not contacted 95 Refused to participate 35
130
Interviewed at discharge/3 weeks
117
No relatives or No consent from patient
or relatives 55
Interviewed 89
Next of kins 144
Figure 3 Flowchart. Voluntarily admitted patients in 1991 and 1997-1999. Dropouts and patients included in the first interview within five days and the follow-up inter-view at discharge or after three weeks. Next of kins, dropouts and those interviewed.

30
Table 1. Patient characteristics. Gender, age, diagnosis, global functioning and symptoms among participating patients. GAF=Global Assessment of Functioning Scale, BPRS= Brief Psychiatric Rating Scale.
Patients interviewed at discharge/three weeks
Involuntarily admitted patients
Voluntarily admitted patients
1991 1997-99 1991 1997-99 n=84 n=118 n=84 n=117
Sex (%) Female 48 57 63 73
Male 52 43 37 27
Age 1) Mean (SD) 40 (13) 41 (13) 40 (13) 42 (12)
Diagnostic category (%) 1)
Psychoses 64 50 35 20 Mood disorders 31 32 * 44 44 * Other diagnoses 5 18 21 36
GAF at admission 2) Mean (SD) 32 (12) 34 (11) 42 (14) 41 (12)
BPRS at admission 3) 2) 4) 5) Mean (SD) 24 (12) 29 (14) * 20 (8) 25 (10) **
1) 1 missing, 2) 2 missing, 3) 19 missing, 4) 3 missing, 5) 11 missing. * p<0.05 , ** p<0.01
In the 1991 study, 18% of the included patients refused to allow the re-searchers to contact next of kins or said they had no close person. For the remaining subjects, 14% of the relatives refused participation or could not be reached. In 1997-1999, 27% of the patients did not allow contact with rela-tives and seven percent stated they had no next of kins. Of relatives asked, twelve percent did not want to participate (Figure 2-3).

31
Interviews and data collection On both study occasions, a first interview was conducted within 5 days of
admission. The interview items were based on previous Swedish and Nordic studies 30 111. The patients were assessed by the Global Assessment of Func-tioning Scale (GAF) 112 and the BPRS, (16 items) 110. Participating patients were also asked for permission to contact a relative or another person close to the patient (next of kin). Two scales of perceived coercion were used in the initial interview in 1997-1999. One was the MacArthur Perceived Coer-cion Scale (MPCS) 17which is a 5-item scale with focus on freedom, choice, idea, control and influence to give a measure for perceived coercion ranging from 0 to 5, where a score of 5 reflects the maximum degree of subjective coercion. The other was the Coercion Ladder (CL), a visual analogue scale, providing a single global score as a direct expression of perceived coercion 111 113. The CL was shown to the patients who were asked to mark their de-gree of perceived coercion on the ladder whilst instructions were read. Scores ranges from l to 10, where 10 represent the highest possible degree of perceived coercion.
A follow-up patient interview concerning experiences of care was under-taken at discharge or at 3 weeks from admission if the care episode was not finished by then. Furthermore, an interview with the next of kin took place, focusing on their attitudes towards psychiatry. Interview items were struc-tured and the interviewer classified the answers of the interviewee according to fixed categories, in many cases added by open-ended questions. The ques-tions used for the present thesis are given in Appendix. The interviewers were psychiatrists and psychiatric psychologists or social workers, exten-sively trained in conducting the interviews for the study. They were not per-sonally involved in the treatment of the patients interviewed and did not know the next of kins they interviewed. When the patient seemed not to un-derstand the question asked the interviewer further made clear the interview question. Additional data was collected from the medical records.
The interrater reliability of the patient interviews had a Cohen’s kappa
value of 0.96 114. In a test-retest reliability study the majority of the items measuring next of kins attitudes towards compulsory care showed a percent-age of concordance greater than 70% 115.
The patients were diagnosed according to the DSM-III-R 116 during the 1991 study and the DSM-IV 112 during the 1997-99 study. The diagnoses were classified into psychoses (schizophrenia, delusional disorders, schizoaf-fective and schizophreniform disorders and atypical psychosis), affective mood disorders (including bipolar affective disorders) and other diagnosis.
The studies were approved by the ethical committee of the Medical fac-ulty at Uppsala University.

32
Statistical analyses In all studies basic statistical methods as Chi-2 (Paper I, II and III), Fish-
ers’ exact test (Paper IV), student-t- test (Paper I, II, III and IV) and Mann Whitney U-test (Wilcoxon rank-sum test) (Paper I, II, III and IV) were used. In addition Cohen’s kappa (Paper II), Kruskal-Wallis, ANOVA (Paper IV) and Logistic regression analyses were performed (Paper II). P-values of <0.05 were considered significant.
Samples and measures in paper I - IV
Paper I Forty-four committed patients and 40 voluntarily admitted patients from
the Västmanland part of the 1991 study were included. In the second inter-view 37 committed and 33 voluntarily admitted patients were interviewed. From the 1997-1999 study 49 committed and 49 voluntarily admitted pa-tients were included. The follow-up interview was performed with 43 and 40 patients, respectively.
A number of questions concerning patient experiences of admission and treatment were used as dependent variables and current legislation was used as the independent variable. The exact list of questions is presented in Ap-pendix.
Paper II The sample consisted of 235 patients participating in the second interview
at the four settings of the 1997-1999 study. Due to missing data in two cases in the key variable concerning subjective outcome of care, the study in-cluded a total of 233 patients.
A number of questions concerning patient experiences of admission and treatment, presented in Appendix, were used. In addition, the MPCS 17 the CL 111 113, GAF 112 and BPRS 110were used as independent variables.
For subjective outcome the following question was used: Considering your mental problems, how do you feel now compared with at the time of admission? Answers were categorized as improved or not improved.
For assessed outcome we used GAF. An increase in GAF-score >10 was considered as an improvement. These questions and ratings were used as dependent variables.

33
Paper III The samples included in paper III were - 84 committed and 84 voluntarily admitted patients interviewed at fol-
low-up in the 1991 study - 118 committed and 117 voluntarily admitted patients interviewed at fol-
low-up in the 1997-1999 study - 64 next of kins of the committed and 69 relatives of the voluntarily ad-
mitted patients 1991 - 73 next of kins of the committed and 89 of the voluntarily admitted pa-
tients in 1997-1999. Current legislation was used as the main independent variable. Questions concerning general attitudes towards compulsory care as a pub-
lic policy issue collected during the second patient interview and the next of kin interview were used as a dependent variable. These questions are given in Appendix.
Paper IV The sample for this study was 118 patients participating in the follow-up
interview in 1997-1999. Due to missing data in three cases in the key vari-able concerning restraint, the study included a total of 115 patients.
Answers to the question: ”During this treatment episode, were you at any time restrained by belt?” (Appendix) at the second interview were used to categorize self-reports. Data regarding mechanical restraint, medication and diagnosis, collected from medical records were used to measure the accuracy of such reports. In addition GAF 112, the BPRS 110, DSM-IV diagnosis 112, and information regarding current medication was used as predictors of false negative ad false positive responses.

34
Results
Paper I This study, which compare patients’ experiences of care during the previ-
ous law of compulsory care, the LSPV, and the current LPT, is focusing on some of the main legal changes. There were no significant differences in gender, age, diagnosis, social functioning or symptoms among the patients between 1991 and 1997-1999.
Of the committed patients 19% in 1991 and 12% in 1997-1999 said they were not, or did not know if they were, formally committed. Of the voluntar-ily admitted patients, 16-21% believed or did not know if they were formally committed. There were no significant differences between the two study occasions in these aspects.
About two thirds of the committed patients and half of the voluntarily admitted patients reported that they were denied to leave the ward. Around half of the committed patients and 15-21% of the voluntarily admitted pa-tients reported that they had been subjected to coercive measures during the care episode. Thirty percent of the committed patients 1991 and 54% of the committed patients in 1997-1999 reported at least one coercive measure as forced medication, restraint or seclusion. This was a significant increase. None of the voluntarily admitted patients reported any of these measures.
Of the committed patients who knew they were committed 40% in 1991 and 29% in 1997-1999 considered it was right that they were admitted against their own will (n.s).
In the follow up interview about 90% of the voluntarily admitted patients reported that they were admitted at the right time or that they should have been admitted earlier. Around one third of the committed patients were of the opinion that they should not have been admitted at all, with no differ-ences between the study occasions.
Having a contact person at the ward was reported by 61-68% of the pa-tients. The existence of a treatment plan was reported by 19-28% of the committed patients and by 33-36% of the voluntarily admitted patients. Not all of them thought they had been participating in planning of the treatment plan. The relatives participating in the treatment of the patients during care was reported in 26-39% of the cases. There were no differences between the 1991 and 1997-1999 study.

35
Paper II Little is known about the outcome of brief inpatient treatment interven-
tions in psychiatric practice. We studied whether subjective (patient reports) and assessed outcome (according to GAF) of brief psychiatric inpatient care are related to patient characteristics, coercion at admission and during care, and other treatment characteristics.
Sixty-four per cent of the patients were female, and the mean age was 42 (SD=12). Thirty-five per cent of the total sample were classified as having a psychosis, 38% as having mood disorders and 27% had other diagnoses. Mean GAF at admission was 38 (SD=12) and mean BPRS score 27 (SD=12).
Of all 233 participating patients, 50% were legally involuntarily admitted. Sixty-seven per cent were classified as subjectively improved and 33% as not improved. GAF assessments at baseline and follow-up were obtained for 222 of the patients, of whom 58% were assessed as improved and 42% not improved. There was no association between subjective and assessed im-provement (Kappa=0.027 p=0.68).
Coercion at admission was not related to the outcome of treatment during the hospitalisation period. Legal status at admission and subjective experi-ences of coercion measured by MPCS and CL were not associated with sub-jective or assessed outcome. In the logistic regression analyses, different predictors for subjective and assessed outcome, respectively, were found. Predictors for subjective improvement were being well treated by the staff (OR=4.1, 95% C.I.=2.1 -7.9, p<0.001), having one or more contact persons at the ward (OR=4.2, 95% C.I.=2.1-8.6, p<0.001), and not having a diagno-sis of the category “other diagnoses” (OR=0.4, 95% C.I.=0.2-0.9, p=0.015). Predictors for a GAF change of +10 or more were a low GAF score at ad-mission (OR=0.9, 95% C.I.=0.9-0.9, p<0.001), and having a mood disorder diagnosis (OR=2.1, 95% C.I.=1.1-4.0, p=0.026).
Interestingly perceived or formal coercion was not a predictor of subjec-tive or assessed improvement.
Paper III Differences in attitudes of patients and next of kins towards involuntary
admission, before and after the change in the psychiatric compulsory care legislation was studied.
About 70% of the committed patients in the 1991 study and in the 1997-1999 study stated that it should be possible to compulsory admit patients. Among the voluntarily admitted patients, 74% in the 1991 study and 86% 1997-1999 stated that it should be possible to compulsory admit patients (Chi2 = 4.995, df = 1, p = 0.025). Of those involuntarily and voluntarily

36
admitted patients who stated that it should be possible to compulsory admit patients, about 90% were of the opinion that doctors should decide upon compulsory admissions.
Among those 55 patients in the 1997-1999 study who stated that it should not be possible to compulsory admit patients, 42% thought that the doctor should be involved in the decision regarding compulsory admission, to com-pare with 86% of those 180 patients who thought that it should be possible to compulsory admit patients (Chi2 = 44.986, df = 1, p < 0.001). No other dif-ference between attitudes to decision regarding compulsory admission was found between the 55 and 180 patients.
Next of kins About 90% of next of kins of the voluntarily and the involuntarily admit-
ted patients stated that compulsory admission should be used to protect the patients or in circumstances where the patient is not aware of that he/she is in need of care. A great majority stated that compulsory admission could be used to protect others, while a lower proportion, especially among next of kins of voluntarily admitted patients, stated that compulsory care is needed to ease the burden of the patient’s network. There was no difference between the two studies.
All next of kins of the committed patients, stated that doctors should de-cide about compulsory admission in the 1991 study and 88% in the 1997-1999 study. A similar result was found among next of kins of the voluntarily admitted patients. A small proportion (11-16%) of next of kins stated that decision regarding compulsory admission should be made by legal authori-ties. Between the two studies the proportions, among both involuntarily and voluntarily patients, who stated that relatives should decide about compul-sory admission decreased significantly, while the proportions of next of kin’s of voluntarily admitted patients who stated that relatives, only, should decide increased.
Paper IV The mechanical restraint, which was considered to be reliably docu-
mented in the medical records, was used to estimate the diagnostic accuracy of questions about past emotional trauma in involuntarily admitted patients, both with regard to rates of false negative (patient denied experiences of mechanical restraint, inconsistent with medical record) but also false positive (patient report of mechanical restraint inconsistent with the documentation in medical records) results.
The study included a total of 115 committed patients. Nineteen patients reported they had been mechanically restrained. Eleven of these cases were

37
true positive (patient report of mechanical restraint consistent with the documentation in medical records) and 8 (42%) were false. Ninety-six pa-tients reported that they had not been mechanically restrained. Four of these (4%) were false negative.
The sensitivity of patient self-reports was 73% (11/15) and the specificity was 92% (92/100). The positive predictive value of patients self reports was 58% (11/19) and the negative predictive value was 96% (92/96) (Table 2).
There was no significant relations between the validity of self reports and type of medication at admission or discharge. The only significant relation between psychiatric symptoms and the validity of self reports were found on GAF scores at discharge which were higher amongst individuals giving re-ports that were inconsistent with medical records and BPRS item self esteem which was lowest amongst those falsely denying experiences of being re-strained, M = 0.3 (SD 0.5) and highest amongst those accurately reporting such experiences M = 2.4 (SD 1.4). However, none of these results survived correction for multiple testing.
Table 2. Distribution of patients’ answers to the question “During this treatment episode were you at any time restrained by belt?” related to documentation in medi-cal records.
Medical record
YES
Medical record NO
Self report YES
True positive n=11
False positive n=8 19
Self report NO
False negative n=4
True negative n=92 96
15
100

38
Discussion
In this thesis, aspects of coercion in psychiatric care were studied in groups of Swedish psychiatric inpatients, some of which had been subject to formal legal compulsory care and some who had not. There were two main findings that resurfaced in different forms throughout the studies.
First, mental health professionals and patients perceive and understand
the same situations and phenomena in very different ways. This finding first occurred in Paper I in which, consistent with previous findings discussed in the introduction 8 18 19 21 22 50 52 53, a considerable confusion among patients as to their status as compulsorily or voluntarily treated became apparent. In this study about one fifth of voluntarily admitted patients believed that they were subject to compulsory care and a similar number of compulsorily admitted patients believed that they were admitted voluntarily.
The results of Paper II suggest that this discrepancy between patient and staff perceptions does not only apply to coercion but also to perceptions of treatment outcome. That is, no statistical relation what so ever (Kappa=0.027) was found between changes in professional assessments of global functioning of life as measured before and after treatment and the patients answers to the question whether they felt that they had improved during treatment.
Finally the results of Paper IV suggest that some discrepancies between perceived and formal coercion may actually be caused, not only by misun-derstandings and differences in opinions between patients and staff mem-bers, but also by relatively unambiguous errors in patient self reports. In this study patient self reports of being mechanically restrained were related to documentation of such measures which, unlike some other aspects of coer-cion, are subject to strict regulation and demands for documentation accord-ing to Swedish law, which implies that the objective documentation can be regarded as relatively reliable. The positive predictive value (i.e. the likeli-hood that a patient who claimed to have been mechanically restrained actu-ally had been so) was only some 58% which is just a little bit above chance level though the sensitivity, specificity and negative predictive values were somewhat higher.
As noted above, the fact that such a discrepancy exists for perceptions of compulsory care has previously been demonstrated and it has been suggested that many of these discrepancies may be explained by errors and misreport-

39
ing on behalf of mental health professionals and next of kins 54. The results of the studies presented in the present thesis does not contradict this notion but suggest, first that these discrepancies may apply to a broader range of psychiatric phenomena than degrees of coercion, and second, that a consid-erable amount of misreporting may occur not only among mental health professionals, but also among psychiatric patients. Of course there are a number of possible sources of discrepancies between the world view of the psychiatric patient and the staff of a psychiatric hospital. One obviously con-cerns the different perspectives on the situation the patient finds himself in. Another concerns factors related to the psychiatric disease, such as disturbed cognitive functions, influence of drugs and the impairments in the ability to separate internal and external stimuli that constitute the hallmark of psy-chotic diseases. There is also the possibility that patients may not always have been truthful in their communications with the research interviewers and finally there are common forms of memory errors that may be made by psychiatric and non psychiatric patients alike. One such error that may pos-sibly have influenced the results of study four may be confusion regarding the timing of an event. For example a patient that actually had experienced mechanical restraint earlier, but not during the last treatment episode, may if reporting mechanical restraint, be coded as a false positive. However, in the present study none of these mechanisms could be demonstrated as more important than another. In fact a number of them even turned out as non significant in the analyses made in Paper IV.
The second main finding of the present thesis is a consistent lack of asso-
ciations between aspects of the compulsory psychiatric care and patients perceptions of it. In Paper II it was found that whether a patient was volun-tarily admitted or not did not significantly influence his or her level of re-covery either as assessed by professionals or by patients. Predictors for a positive subjective outcome were perceptions of having been well treated (e.g. to be respected and heard; to be met with a positive and upbeat attitude and to be actively and positively involved in treatment and treatment plan-ning), during the treatment episode, having a contact person at the ward and not having a diagnosis of “other” diagnosis. Patients with diagnosis of eating disorders and personality disorders are included in the group ”other” diagno-sis. Their subjective symptoms can not be expected to be reduced by inpa-tient short time care. However it should be noted that one possible explana-tion for these associations is a general positive bias amongst subjectively improved patients. Predictors of improvement as assessed by professionals were a low level of functioning at admission and a diagnosis of a mood dis-order. It may be easier to obtain improvement from a short inpatient episode for patients with mood-disorders. A deeply depressive patient can be ex-pected to get an increase in GAF from very low to high during inpatient care due to medical treatment, sleep and other ward aspects as to break social

40
isolation and to get support and encourage from staff and other patients. Another possible explanation for these findings may be the phenomenon of regression towards the mean 117.
Paper I and III failed to detect clear differences before and after the new legislation 1992 on compulsory psychiatric care on attitudes and aspects of treatment such as involvement of relatives, having a contact person at the ward, having a treatment plan or inconsistencies in patient and professional classification of patients as voluntarily or compulsory admitted. However, there was a finding of an increased number of patients who reported having been subject to coercive measures such as mechanical restraint, forced medi-cation and seclusion under the new legislation.
One possible interpretation of this apparent lack of findings may be that compulsory care is a phenomenon that is an integrated and even necessary part of a modern society as to prove fairly resistant to temporary, ideologi-cally based changes over time. Indeed the idea of mental illness in general and compulsory aspects of psychiatry in particular, as an important part of the foundation of contemporary culture and contemporary psychiatry in gen-eral, has been proposed by a number of scholars and historians most notably Michele Foucault 118. From this point of view, compulsory psychiatric care is regarded as a way to enforce abstract and superficial perceptions about nor-mality, by defining behaviours that may be hard to perceive as rational by men in authority as “madness”.
However, this problem can also be understood from the very down to earth level of the clinical psychiatrist. Suppose, that you are confronted with a case like that of Erik, presented in the introduction of this thesis, or even that you are confronted with an individual who, because he or she is under the influence of a psychiatric disease has immediate plans to commit suicide. I would propose that regardless of current legislation most sensible individu-als (psychiatrists or not) would agree that some kind of intervention in order to protect the patient is needed. Such interventions may involve some kind of force, and in western modern societies since the age of reason it is widely held that use of force should be monopolized by representatives of public society (i.e. the state) and subject to legal regulations. Most of the next of kins during the both study occasions stated that compulsory care should be used to protect the patient or in circumstances where the patient is not aware of that he/ she is in need of care. Also a great majority stated that involuntary admission could be used to protect the general public (social paternalism). However, a lower proportion of next of kins, stated that compulsory care is needed to ease the burden of the network. The findings of our study were not able to explain why there are few differences in attitudes before and after the new legislation in 1992, neither were our findings able to ascertain the im-pact of the LPT.
As suggested by the results of the present thesis there seems to be a fairly wide agreement at least amongst psychiatric patients and their next of kins

41
that psychiatrists rather than other possible groups (i.e. judges, social work-ers) should play an important role in dealing with such problems. These re-sults seem to reflect strong support for the medical profession’s involvement in the commitment process. This seems to support medical paternalism. Pa-tients and next of kins even stated that different categories of professionals and relatives should be involved in the decision. It should be noted that the fact that there are considerable international and regional differences in the ways compulsory psychiatric care is studied, evaluated and executed 4 30 119 highlights the importance of further debate and studies on how compulsory care is best performed.
Limitations and possible biases The easiest and most elegant way to control for bias when scientifically
studying the effect of one phenomenon (independent variable) on another (dependent variable) is to randomize subjects to treatment conditions. This way all other variables than the one studied (such as age, previous alcohol problems, gender, number of children, interest in the classical arts, hair col-our, shoe size etc.) will, regardless of whether they are relevant to the study question or not, be randomly rather than systematically distributed in all study groups (most often an experimental group and a control group).
However, randomized studies of compulsory care are almost non existent, because randomizing an individual to compulsory care, when it is not abso-lutely certain that the patient is in an indispensable need for such care, is considered unethical. As well, randomizing a patient, who is in an indispen-sable need for such care to a control group, is also unethical. Consequently, all studies in this thesis, as well as almost all studies performed so far within this field of research, are non-randomized, which means that there is poten-tial for a vast number of biases between groups.
In Papers I and III the effect of the change from the 1967 (LSPV) to the 1992 (LPT) legislation was studied. Few changes in attitudes among invol-untarily and voluntarily admitted patients and their next of kins towards in-voluntary psychiatric admission were found between the two study occa-sions, 1991 and 1997-1999. One reason may be that the samples were un-derpowered to detect true differences. Another reason may be that the atti-tudes among committed patients are actually more favourable after the change in legislation, but the fact that only patients, who according to LPT refuse care, can be committed, may have biased the 1997-1999 sample in a way that cancelled out this difference. However, it may also be speculated that a reason for the lack of difference between 1991 and 1997-1999 may be that clinical practice with regard to involuntary psychiatric care may have been stable despite the legislation and organization reforms and that attitude

42
shaping experiences are also similar before and after the introduction of new legislation.
Deinstitutionalisation and Mental Health Care Reform During the 1960s, the anti-psychiatric movements in the USA and Europe
influenced those who criticized the treatment of psychiatric patients in Swe-den. There was a strong emphasis on closing the larger mental hospitals, as in other western countries 120 121. A so called sectorized psychiatry, where the psychiatric organization was responsible for all mental health services in a geographically defined catchment area, was introduced in Sweden between 1975 and 1985. Large institutions were closed and the number of psychiatric beds reduced. An evaluation of this reform showed that long-term mentally ill patients, e.g. those with schizophrenia, did not receive satisfactory treat-ment 122 123. Needs for medical treatment were mainly fulfilled, but other needs, e.g. social support, were not satisfied. As in other European countries, the number of psychiatric beds has continued to decrease in Sweden in the 1990s 5.
A parliamentary commission of 1992, the Committee on Psychiatric Care, concluded that the efforts of social services for people with long-term mental illness were still largely inadequate and were not being provided in a satis-factory manner 124. Therefore, the mandate upon municipal social services was clarified through the Mental Health Care reform 1995 125. The reform was directed towards individuals suffering from severe and long-standing mental illness. The objective was social integration and the best life possible for people with mental illness, on equal terms with the rest of the population. The social services and psychiatry must support one another in their work with the target group, and the involvement of the individual and families in the rehabilitation process is given particular emphasis. A new governmental report recently concluded that these aims have not been fulfilled 126.
The Mental Health Care reform may have influenced the studies pre-sented in this thesis on the effects of the changes in legislation because it occurred between the study periods. In Paper I we could see no difference according to diagnosis between the 1991 and 1997-1999 study. However, this paper only included patients from the County Council of Västmanland.
Both the Mental Health Care reform in itself as well as the changed legis-lation in 1992 may have created a group with a more severe psychopa-thology in the 1997-1999 sample than in the 1991 one and true differences between the study periods may in fact have been masked by this effect (i.e. a lack of difference in perceived coercion may actually be a decrease in per-ceived coercion masked by the fact that much more disturbed patients that by necessity should have to endure more severe coercion were sampled the second time). As shown in table 1, there were less patients having psychosis,

43
and a higher BPRS among both involuntarily and voluntarily admitted pa-tients in the 1997-1999 study.
Power Finally it should be noted that in order to statistically detect differences
between different groups a certain number of observations have to be in-cluded in the calculations. Typically large effect sizes may be detected with smaller samples whereas small effect sizes requires larger samples. When, as is to some extent the case in this thesis, negative findings are discussed the possibility that true differences would have been detected if samples have been larger should be kept in mind.

44
Summary of the results and conclusions
The use of coercion is probably the most difficult question facing the clinically active psychiatrist both from a legal, a scientific, an ethical and an emotional point of view. This thesis represents an attempt to further increase our understanding of some empirical questions regarding this issue. In sum-mary, the findings were:
- No differences were found in patients’ experiences of care during LSPV and LPT regarding most items related to the aims of the law reform and the main legal changes. Sixteen to 21% of the voluntarily admitted patients be-lieved, or did not know whether they were committed or not. Of the involun-tarily admitted patients, 12-19% said they were not, or did not know if they were formally involuntarily admitted according to the commitment act. An individual treatment plan was reported by 19-28% of the committed patients and by 33-36% of the voluntarily admitted patients. The only difference found was that more committed patients in 1997-1999 reported at least one coercive measure: i.e. forcibly medicated, secluded and/or restrained by belt.
- A majority of the patients in the 1997-1999 study were improved at dis-charge or after three weeks of admission. No relationship between subjective and assessed outcome was found. Subjective outcome was associated with whether patients stated having a contact person at the ward and whether pa-tients experienced being treated well or not. Patients improved according to GAF, more often had mood-disorders and low GAF score at admission. Le-gal status and perceived coercion had no bearing on either subjective or as-sessed improvement.
- A majority of all patients in 1991 and 1997-1999 stated that it should be possible to compulsorily admit patients. A great majority of the patients and the next of kins stated that decisions regarding compulsory admission should be taken by doctors. Strong support for coercion in order to protect the pa-tient and others was found among next of kins. The law reform was not re-flected in attitudinal differences.
- A majority of patients answered accurately to the question whether they had been restrained by belt or not. Nineteen of 115 patients reported they had been restrained by belt. Eleven of these cases were true positive and 8 cases were false positive. The positive predictive value of patient self reports was 58% (11/19) and specificity was 92% (92/100). The diagnostic accuracy of patients’ responses to questions during structured interviews may confer a significant risk of not only false negative but also false positive reports. The

45
way patients experience and relate to the past, may best be understood as a dynamic part of a contextual social relation.
In conclusion, the main results were first that when it comes to issues re-
lated to psychiatric coercion there is typically considerable difference be-tween how this is perceived and interpreted by the professional and by the patient, and second that efforts made to change the face of psychiatric coer-cion in the minds of patients as well as the public on part of public policy-makers have had limited effects. Within the legal context, our current profes-sional understanding of psychiatric coercion relies on three pillars. First there is the practical experience of the individual clinicians, second there is science, and third there is the ethical foundation for decisions made. Though the clinical experience is important, science and ethics are of vital impor-tance to keep this difficult process balanced, legitimate and working in the best interest of patients and society. Science and ethics furthermore are in-terdependent so that both draw heavily on each other in order to maximise their impact.
Hopefully one important contribution of the present thesis may be both to inspire further research but also to contribute to the formation of amore solid empirical foundation for further ethical discussions on this issue.

46
Appendix
Interview questions.
Paper I Are you admitted according to the commitment act (LSPV/LPT, respec-
tively)? Do you think you were admitted at the right time? Do you have a contact person at the ward? Has a treatment plan been made up for you? If so, have you been participating in the treatment plan? Is there someone close to you participating in the treatment? Have you been denied to leave the ward? During this treatment episode, were you at any time subjected to meas-
ures against your own will? During this treatment episode, were you at any time exposed to forced
medication? During this treatment episode, were you at any time restrained by belt? During this treatment episode, were you at any time secluded?
Paper II Considering your mental problems, how do you feel now compared with
at the time of admission? Do you have a contact person at the ward? Has a treatment plan been made up for you? Is there someone close to you participating in the treatment? In psychiatric care there are a number of different categories of person-
nel. Often you need contact with several people, either in psychiatric care oroutside (for example doctor, psychologist, psychiatric social worker, nurses,

47
and social service staff). Have you had such contacts? Within and outsidepsychiatry?
Have you received any information about the effects and side effects ofmedication?
Have you been treated well by the staff? Have you been subjected to measures against your own will during this
treatment period
Paper III Patients: Do you think it should be possible to compulsorily admit patients? Who should decide whether a patient should be compulsorily admitted:
doctors, legal authorities, social workers, relatives? Answers were given to a four-degree scale: yes/uncertain/ no/don’t
know. Next of kins: Compulsory care is needed to protect the patient. Compulsory care is needed because the patient himself/herself does not
realise the need of treatment. Compulsory care is needed to ease the burden of the patient’s network. Compulsory care is needed to protect the relatives. Compulsory care is needed to protect the general public. Decisions about compulsory psychiatric care should be made by: doc-
tors, legal authorities, social workers, relatives (four different statements). The interviewer marked on a three-degree scale if the subjects agreed or
not (agree entirely/partly, uncertain, disagree entirely/partly
Paper IV During this treatment episode, were you at any time restrained by belt?

48
Sammanfattning på svenska
Bakgrund Den psykiatriska vården är en av de få medicinska specialiteter som har
både skyldigheter och rättigheter att vårda människor mot deras vilja. Tvångsvården inom psykiatrin, har varit och är föremål för debatt både inom och utom Sverige. Om patienten tvångsvårdas kan det vara svårt att samti-digt tillgodose principen att ”göra gott” och att respektera patientens behov av och rätt till självbestämmande. Inom tvångsvården finns det alltså in-byggda etiska konflikter.
Ett argument för tvångsvård i ett enskilt fall kan vara att patientens psy-kiska status eller hälsotillstånd kan förväntas bli bättre, som ett resultat av tvånget i sig och/eller genom att en fast ram erbjuds en person som befinner sig i svår kris. Själva tvångsintagningen kan även ge vården möjligheter att vidtaga andra tvångsåtgärder såsom t ex injektioner av neuroleptika, fast-spänning eller möjligheter att skydda patienten själv, medpatienter, familj och samhället.
År 1992 ersattes den tidigare psykiatriska tvångsvårdslagstiftningen La-gen om sluten psykiatrisk vård i vissa fall (LSPV) av Lagen om psykiatrisk tvångsvård (LPT) och Lagen om rättpsykiatrisk vård (LRV). Syftet med den ändrade lagstiftningen var att minska användandet av tvång i den psykiatris-ka vården samt att stärka patienternas autonomi och rättsäkerhet. Tanken med den nya lagstiftningen (LPT) var att psykiatrisk vård skall ges under frivilliga former i så stor utsträckning som möjligt. Vårdbehovet skall vara avgörande för bedömningen av om tvångsvård får tillgripas och ändamålet skall vara att patienten blir i stånd till att medverka frivilligt i vården. Skyd-det för omgivningen skall beaktas men inte tillmätas samma betydelse som i LSPV. Kriterierna ändrades och för att någon skall få tvångsvårdas krävs att patienten lider av allvarlig psykisk störning, att patienten har ett oundgäng-ligt behov av psykiatrisk sluten vård och att patienten motsätter sig vården, eller att det finns grundad anledning att anta att vården inte kan ges med hans samtycke. Med den tidigare lagstiftningen kunde patienter tvångsvårdas om en specialist i psykiatri ansåg det vara viktigt utifrån patientens tillstånd och prognos och till skillnad från LPT kunde vården bedrivas oberoende av patientens samtycke. Det juridiska inflytandet stärktes och läkarnas möjlig-heter att besluta om tvångsvård begränsades med LPT. Senast efter fyra

49
veckors vårdtid sker idag en juridisk prövning huruvida tvångsvården skall fortsätta.
Under de senaste decennierna har antalet slutenvårdsplatser och därmed slutenvårdspatienter i psykiatrin drastiskt minskat. Stora skillnader gällande den psykiatriska tvångsvårdens omfattning har konstaterats både mellan och inom olika länder. Beträffande olikheter i lagstiftning är det svårt att göra jämförelser mellan olika länder. Forskning och diskussioner kring tvångs-vård kan inte begränsas till det formella tvånget.
Även frivilligt vårdade patienter kan uppleva sig utsatta för tvång av olika slag. Patienter har inte alltid kännedom om sin legala status. Patienter som vårdas frivilligt uppger sig vara tvångsvårdade och vice versa. Inom senare forskning har det formella tvånget och det upplevda tvånget alltmera stude-rats, liksom vad som sker under själva inläggningen vid psykiatrisk tvångs-vård. Även tvångsåtgärder har studerats och det är inte alltid som patienters rapportering av tvångsåtgärder, såsom t.ex tvångsinjektioner, stämmer med vad som finns dokumenterat i journalhandlingar.
Minnen rörande en händelse kan ha flera ursprung: det man själv upplev-de vid händelsen, det man kan ha hört om den i efterhand och det som har skrivits om händelsen. Enligt ursprungsbedömningsteorin (Source-monitoring theory) gör människor ständigt bedömningar av sina minnens ursprung. Både faktiska, perceptuella händelser och händelser genererade inifrån lämnar enligt teorin bestående minnesspår. Misstag som vi gör när vi försöker minnas kan vara att vi inte gör skillnad på ursprunget till ett min-nesspår. Det kan också vara svårt att skilja på minnen från yttre verkliga händelser och på minnen från inre upplevelser som fantasier, drömmar och tankar om händelser.
Vårdresultat av tvångsvård har studerats på olika sätt, såsom om patienten har upplevt sig förbättrad, liksom patientens attityder till själva vårdepiso-den. Även olika skattningsinstrument har använts t.ex. GAF( Global As-sessment of Functioning Scale) som mäter medicinsk, psykologisk och soci-al funktion.
Anhörigas delaktighet i vården har ökat och betonas särskilt i den nya tvångsvårdslagstiftningen. Utifrån sektoriseringen, avinstitutionaliseringen och Psykiatrireformen 1995 har stora delar av den psykiatriska vården förts över till kommunerna, som därmed fått ett ökat ansvar för psykiatriska pati-enter. Det har påverkat anhörigas livssituation och bördan på anhöriga har ökat.

50
Syfte -att studera patienters erfarenheter av vård under två olika lagstiftningar,
LSPV och LPT, utifrån syftet med den förändrade lagstiftningen, -att studera huruvida legalt och upplevt tvång, samt andra vårdfaktorer i
den slutna vården, relaterar till vårdresultatet, -att studera om den förändrade lagstiftningen återspeglas i patienters och
anhörigas attityder till psykiatrisk tvångsvård, samt -att beskriva och närmare undersöka skillnader mellan tvångsåtgärder och
andra behandlingsaspekter, rapporterade av patienten, i förhållande till upp-gifter i andra källor.
Delarbete I Fyrtiofyra tvångsvårdade och 40 frivilligt vårdade patienter intervjuades
vid den första intervjun 1991 i Västmanland och vid uppföljningsintervjun 37 tvångsvårdade och 33 frivilligt vårdade patienter. I studien 1997-1999 intervjuades i Västmanland vid den första intervjun 49 tvångsvårdade och 49 frivilligt vårdade patienter och vid uppföljningsintervjun 43 tvångsvårdade och 40 frivilligt vårdade patienter.
Av de tvångsvårdade patienterna uppgav sig 19% 1991 och 12% 1997-1999 inte vårdas på tvång eller känna till huruvida de vårdades på tvång. Av de frivilligt vårdade patienterna var det 16-21% som trodde eller inte visste om de vårdades på tvång.
Huvudresultatet blev att utifrån patienternas upplevelser av vården tycktes väldigt lite ha förändrats mellan de två studietillfällena. Den enda signifikan-ta skillnaden var att fler tvångsvårdade patienter 1997-1999 uppgav sig ut-satta för åtminstone en tvångsåtgärd såsom tvångsmedicinering, fastspänning eller avskiljning. Ingen av de frivilligt vårdade patienterna uppgav sig vara utsatta för formella tvångsåtgärder. Vare sig de tvångsvårdade eller de frivil-ligt vårdade patienternas självrapporterade upplevelser av delaktighet i vård-planeringen skilde sig åt mellan mättillfällena.
Delarbete II Sammanlagt 233 tvångsvårdade och frivilligt vårdade patienter intervjua-
des 1997-1999 inom fem dagar efter intagningen samt vid utskrivning eller efter tre veckors vårdtid. Det förelåg inte något samband mellan patienternas subjektivt upplevda förbättring och förbättring mätt med Global Assessment of Functioning Scale(GAF), som mäter medicinsk, psykologisk och social

51
funktionsförmåga (kappa= 0.027, p=0.681). Vare sig formellt eller subjektivt tvång var relaterat till vårdresultatet. Att känna sig väl bemött av personalen och att ha en kontaktperson hade samband med subjektiv förbättring, samt vissa diagnoser. Patienter förbättrade enligt GAF hade lägre GAF vid intag-ningen, mera symtom och oftare affektiva tillstånd.
Delarbete III Åttiofyra tvångsvårdade och 84 frivilligt vårdade patienter intervjuades
1991 och 118 tvångsvårdade och 117 frivilligt vårdade patienter intervjuades 1997-1999 vid utskrivning eller efter tre veckor vårdtid. 1991 intervjuades 64 närstående till tvångsvårdade och 69 närstående till frivilligt vårdade pa-tienter och 1997-1999 intervjuades 73 närstående till tvångsvårdade och 89 närstående till frivilligt vårdade patienter ca en månad efter intagningen. En majoritet av såväl tvångsvårdade som frivilligt vårdade patienter ansåg att tvångsvård behövs. Av de frivilligt vårdade är det fler 1997-1999 som tyckte att tvångsvård behövs jämfört med 1991. De flesta närstående var positiva till tvångsvård samt ansåg att tvångsvård behövs när patienten inte inser sitt vårdbehov samt för att skydda patienten, den närmaste omgivningen och allmänheten. Beslut om tvångsvård ansågs som en medicinsk fråga, där läka-ren är den viktigaste beslutsfattande aktören.
Delarbete IV Etthundrafemton tvångsvårdade patienter tillfrågades 1997-1999 vid ut-
skrivning eller efter tre veckors vårdtid om de utsatts för fastspänning under vårdtiden. Patienternas svar jämfördes med journaluppgifter gällande tvångsåtgärden fastspänning. Nitton patienter rapporterade att de hade utsatts för fastspänning. I 11 av dessa fall stämde patients uppgift överens med journaluppgiften om fastspänning (sant positiva) och i 8 fall uppgav patien-ten sig varit utsatt för fastspänning vilket inte överensstämde med journal-uppgifterna (falskt positiva). Nittiosex patienter rapporterade att de inte varit utsatta för fastspänning denna vårdepisod varvid uppgift om fastspänning inte fanns i journalen för 92 (sant negativa) medan uppgift om fastspänning fanns för fyra av dessa patienter (falskt negativa).
Inget klart samband mellan psykiatriska symtom, medicinering eller ej och reliabilitet vad gäller patienters självrapportering kunde påvisas i studi-en.

52
Konklusion Avhandlingens resultat leder till två huvudsakliga slutsatser. Den ena är att psykiatrisk personal och patienter kan uppleva och förstå
samma situationer och fenomen på mycket skilda sätt. Vare sig formellt eller subjektivt upplevt tvång var relaterat till vårdresultatet. Inte heller tycktes det finnas något samband mellan subjektiv upplevd förbättring och förbättring mätt med GAF. Att känna sig väl bemött av personalen och att ha en kon-taktperson hade samband med subjektivt upplevd förbättring. Det var låg överensstämmelse mellan patienternas uppgifter om tvångsåtgärden fast-spänning och journaldokumentationen. Patienternas minnesbild av själva vården kan grumlas av deras psykiska symtombild och medicinering liksom av generella svårigheter att minnas tidigare händelser.
Den andra är att patienters upplevelser av vården liksom patienters och närståendes attityder till tvångsvård föreföll relativt opåverkade av den psy-kiatriska tvångsvårdslagstiftningen. Få patienter upplevde delaktighet i vår-den, men flertalet patienter och närstående var generellt positiva till psykiat-risk tvångsvård, vid bägge studietillfällena. Patienters upplevelser av tvång liksom hur patienter upplever och beskriver tidigare händelser kan bäst för-stås såsom en dynamisk process i en social kontext.

53
Acknowledgments
I would like to express my sincere gratitude to all colleagues and friends who encouraged me to undertake, continue and finish this project. A project like this is nothing you can manage by yourself. Especially, I want to thank the following:
Rickard L. Sjöberg, my supervisor and co-author, for encouragement and a never ceasing flow of constructive criticism. You have been a tough and forceful supervisor and you gave the project a dosage of vital injection. You have widened my intellectual horizon and you have always been available for consultations.
Leif Lindström, my former supervisor and co-author. You guided me with patience and wisdom through phases of the research project. Thank you for sharing your wide international scientific as well as your clinical interest and experience.
Jerzy Leppert, co-supervisor and Head of the Centre for Clinical Research in Västerås, for your ability to make impossible things possible and always having your door open and listening patiently. Thanks for providing the time and resources that made my research possible and for taking us all the way to Camargue!
Lars Kjellin, my co-supervisor, co-author and friend, for your interest and constant enthusiastic guidance and patience throughout the study. You have always been helpful and giving me personal support. You convinced me that I could do this.
Christina Jogér, Head of the Department of Psychiatry, for providing the time and resources that made my research possible and for your kind interest in this thesis.
Lars von Knorring, for making it possible to start my doctoral studies
Margareta Östman, my co-author in paper III, for inspiration and friendly support.

54
Gerdt Wretmark, my late professor, for introducing me to medical ethics in psychiatry and to the “interpersonal process recall method” (Terapeutisk hållning - Relationer - Samtalskonst). At the age of 23, working in the excel-lent Psychiatric Clinic in Linköping, I decided to become a psychiatrist.
Kerstin Eriksson, my colleague, for introducing me to this project at a con-ference in Visby, Gotland, years ago.
Claes-Göran Westrin and Olle Östman, the scientific founders of the “tvångsvårdprojektet”, for your enthusiasm and personal support.
Inga-Lill Candefjord, Marianne Erkki, Kerstin Rännar and Kristina Anders-son, for sharing experiences and hard work for so many years.
All the co-operators who performed the interviews in the participating cen-tres, Borås, Umeå, Uppsala, Västerås and Ängelholm.
Eva Thors-Adolphsson, my dear friend and roommate at Centre for Clinical Research, Västerås, and in Camargue, for kindness, support, fruitful discus-sions, constructive advice and joy.
Tony Wiklund, for kindness, support with my crashed and non-crashed com-puters and for stimulating discussions.
Kent Nilsson, statistical advisor, giving me guidance and friendly support.
Katarina Ringström, Maria Dell’Uva Karlsson, Gun Nyberg and Marja-Lena Ojutkangas, at Centre for Clinical Research, for kind and respectful support.
Leif Bergkvist, Jana de Boniface, Mats Enlund, Arne Eklund, Håkan Flink, Helena Granstam-Björneklett, Ann Christin Johansson, Eva Nohlert, Marie-Louise Södersved-Källestedt, Anders Westman, Bertil Vinnars and Cecilia Åslund. Thank you for the time we have shared with research work, semi-nars, discussions, manuscript writing, as well as joy and laughter!
Åke Tegelberg and Göran Nilsson, for support, fruitful discussions and in-terest in this work.
Robert Cookson, my son-in-law, for your support and linguistic revision of my manuscripts.
The staff at the Central Hospital Library, especially Gunnel Hellman and Fredrik Thorén, who always have been helpful in the search for references and literature without hesitation.

55
Bo Simonsson, for supporting me when I really needed it.
Aina Brandell and Gunnel Ersson, my dear colleagues and friends, for sup-porting and giving me invaluable comments on drafts of my thesis.
Birgitta Laghé, my dear friend, for all your support and encouragement. You have been an inspiring example in my research work for the last years.
Johanna, Elin, Jakob and Daniel, our children for giving me so much love and constant support.
Anna, Emma and William, my lovely grandchildren, for reminding me what is important in life. Now I will have more time to be your ”mormor”, listen-ing to the song ”Let´s go to San Fransisco”.
Gunnar, my beloved husband, you are the most important to me. Since we met 18 April 11 years ago, you have been by my side. Without your love, words of wisdom, support and mindfulness, I would not have been able to complete this project. And, believe me or not, from you I learned patience with computers!
Last but not least, I would like to express my very special thanks to all pa-tients and their next of kins participating in this study. Without your and the staff members contribution, there had not been any thesis.
The studies have been supported by County Councils of Västmanland, Kris-tianstad, Uppsala, Västerbotten, Älvsborg and Örebro and the National Board of Health and Welfare.

56
References
1. Socialstyrelsen. Den rättspsykiatriska vården 2005 : en sammanställning
från inventeringen 18 maj 2005. [Elektronisk resurs]. Stockholm: Socialstyrelsen, 2005.
2. SFS nr: 1991:1129. Lag (1991:1129) om rättspsykiatrik vård, 1991. 3. SFS nr: 1991:1128. Lag (1991:1128) om psykiatrisk tvångsvård, 1991. 4. Salize HJ, Dressing H. Epidemiology of involuntary placement of men-
tally ill people across the European Union. Br J Psychiatry 2004;184:163-8.
5. Priebe S, Badesconyi A, Fioritti A, Hansson L, Kilian R, Torres-Gonzales F, et al. Reinstitutionalisation in mental health care: comparison of data on service provision from six European countries. Bmj 2005;330(7483):123-6.
6. WPA. Declaration of Hawaii. J Med Ethics 1978;4(2):71-3. 7. Okasha A. The Declaration of Madrid and its implementation. An update.
World Psychiatry 2003;2(2):65-7. 8. Kjellin L, Hoyer G, Engberg M, Kaltiala-Heino R, Sigurjonsdottir M.
Differences in perceived coercion at admission to psychiatric hospi-tals in the Nordic countries. Soc Psychiatry Psychiatr Epidemiol 2006;41(3):241-7.
9. Svensson G, Kjellin L. Legal report: Sweden. In: Kallert TW, Torres-Gonzales F, editors. Legislation and coercive mental health care in Europe. Frankfurt am Main: Peter Lang, 2006.
10. SFS nr: 1966:293. Lag (1966:293) om beredande av sluten psykiatrisk vård i vissa fall, 1966.
11. SFS nr: 1982:763. Hälso- och sjukvårdslag (1982:763). Omtryck: SFS 1992:567 ed: SFS, 1982.
12. Gronwall L, Holgersson L. Psykiatrin, tvånget och lagen : en lagkom-mentar i historisk belysning till den psykiatriska tvångsvårdslagstift-ningen år 2001. Stockholm: Norstedts juridik, 2001.
13. SOU 1984:64. Psykiatrin, tvånget och rättssäkerheten : slutbetänkande. Stockholm: Liber/Allmänna förl., 1984.
14. Ostman O. Descriptors of the function of mental health service - exam-ples from Sweden. In: Cronholm B, von Knorring L, editors. Evaluation of mental health services programs. Hässelby: Medi-cinska forskningsrådet, 1983:81-95.
15. Socialstyrelsen. LPT: tillämpning av lagen om psykiatrisk tvångsvård. Allmänna råd från Socialstyrelsen ; 1991:9 Stockholm: Allmänna förl. [distributör], 1991.

57
16. Bindman J, Reid Y, Szmukler G, Tiller J, Thornicroft G, Leese M. Per-ceived coercion at admission to psychiatric hospital and engagement with follow-up--a cohort study. Soc Psychiatry Psychiatr Epidemiol 2005;40(2):160-6.
17. Gardner W, Hoge SK, Bennett N, Roth LH, Lidz CW, Monahan J, et al. Two scales for measuring patients' perceptions for coercion during mental hospital admission. Behav Sci Law 1993;11(3):307-21.
18. Hoge SK, Lidz C, Mulvey E, Roth L, Bennett N, Siminoff L, et al. Pa-tient, family, and staff perceptions of coercion in mental hospital admission: an exploratory study. Behav Sci Law 1993;11(3):281-93.
19. Kjellin L, Westrin CG. Involuntary admissions and coercive measures in psychiatric care. Registered and reported. Int J Law Psychiatry 1998;21(1):31-42.
20. Lidz CW, Hoge SK, Gardner W, Bennett NS, Monahan J, Mulvey EP, et al. Perceived coercion in mental hospital admission. Pressures and process. Arch Gen Psychiatry 1995;52(12):1034-9.
21. McKenna BG, Simpson AI, Laidlaw TM. Patient perception of coercion on admission to acute psychiatric services. The New Zealand ex-perience. Int J Law Psychiatry 1999;22(2):143-53.
22. Rogers A. Coercion and "Volontary" Admission: An Examination of Psychiatric Patient Views. Behav Sci Law 1993;11:259-67.
23. Bennett NS, Lidz CW, Monahan J, Mulvey EP, Hoge SK, Roth LH, et al. Inclusion, motivation, and good faith: the morality of coercion in mental hospital admission. Behav Sci Law 1993;11(3):295-306.
24. Beauchamp TL, Childress JF. Principles of biomedical ethics. New York: Oxford University Press, 2001.
25. Kant I, Retzlaff J. Grundläggning av sedernas metafysik. Göteborg: Dai-dalos, 1997.
26. Mill JS, Ahlberg A. Om friheten. Stockholm: Natur och kultur, 1984. 27. Gillon R. Autonomy and the principle of respect for autonomy. Br Med J
(Clin Res Ed) 1985;290(6484):1806-8. 28. Engstrom I. Tvingad till hjälp : om tvång, etik och tillit i barn- och ung-
domspsykiatrisk vård. Lund: Studentlitteratur, 2006. 29. Jonsen AR, Siegler M, Winslade WJ. Clinical ethics : a practical ap-
proach to ethical decisions in clinical medicine. New York: McGraw Hill, Medical Pub. Division, 2006.
30. Kjellin L. Coercion in psychiatric care : formal and informal-justification and ethical conflicts. Uppsala: Acta Universitatis Upsa-liensis, 1996.
31. Hanson R. Making sense of medical paternalism. Med Hypotheses 2007. 32. Kjellin L, Nilstun T. Medical and social paternalism. Regulation of and
attitudes towards compulsory psychiatric care. Acta Psychiatr Scand 1993;88(6):415-9.
33. Ceci SJ, Bruck M. Jeopardy in the courtroom : a scientific analysis of children's testimony. Washington, D.C.: American Psychological Association, 1995.

58
34. Ceci SJ, Friedman RD. The suggestibility of children: Scientific research and legal implications. Cornell Law Review 2000;86:33-108.
35. Hyman IE, Jr., Loftus EF. Errors in autobiographical memory. Clin Psy-chol Rev 1998;18(8):933-47.
36. Lindsay DS, Read JD. "Memory work" and recovered memories of childhood sexual abuse: Scientific evidence and public, professional and personal issues. Psychology, Public Policy and Law 1995;1:846-909.
37. Redelmeier DA, Tu JV, Schull MJ, Ferris LE, Hux JE. Problems for clinical judgement: 2. Obtaining a reliable past medical history. Cmaj 2001;164(6):809-13.
38. Sjoberg RL. Child testimonies during an outbreak of witch hysteria: Sweden 1670-1671. J Child Psychol Psychiatry 1995;36(6):1039-51.
39. Sjoberg RL. False allegations of satanic abuse: case studies from the witch panic in Rattvik 1670-71. Eur Child Adolesc Psychiatry 1997;6(4):219-26.
40. Sjoberg RL. The outbreak of mass allegations of Satanist child abuse in the parish of Rattvik, Sweden, 1670-71: two texts by Gustav J. El-vius. Hist Psychiatry 2004;15(60 Pt 4):477-87.
41. Sjoberg RL. [Satanic ritualistic murders and child abuse--evidence-basing versus ideology]. Lakartidningen 2005;102(40):2824-5.
42. Sjoberg RL, Lindholm T. A systematic review of age-related errors in children's memories for voiding cystourethrograms (VCUG). Eur Child Adolesc Psychiatry 2005;14(2):104-5.
43. Sjoberg RL. Pre-school children remembering unpleasant events: com-plying with the unwritten rules of an invisible game. Applied Cogni-tive Psychology 2001;15:687-91.
44. Spanos NP. Multiple identity enactments and multiple personality disor-der: a sociocognitive perspective. Psychol Bull 1994;116(1):143-65.
45. Spanos NP, Nicholas P, Menary E, Gabora NJ, DuBreuil SC, Dewhirst B. Secondary identity enactments during hypnotic past-life regres-sion: A sociocognitive perspective. Journal of Personality and So-cial Psychology 1991;61(2):308-20.
46. Wells GR, Small M, Penrod S, Malpass SM, Fulero SM, Brimacombe CAE. Eyewitness Identification Procedures: Recommendations for Lineups and Photospreads. Law and Human Behaviour 1998;22(6):1-39.
47. Penfield W. The interpretive cortex; the stream of consciousness in the human brain can be electrically reactivated. Science 1959;129(3365):1719-25.
48. Loftus E. Our changeable memories: legal and practical implications. Nat Rev Neurosci 2003;4(3):231-4.
49. Poulsen HD, Engberg M. Validation of psychiatric patients' statements on coercive measures. Acta Psychiatr Scand 2001;103(1):60-5.

59
50. Bonsack C, Borgeat F. Perceived coercion and need for hospitalization related to psychiatric admission. Int J Law Psychiatry 2005;28(4):342-7.
51. Hiday VA, Swartz MS, Swanson J, Wagner HR. Patient perceptions of coercion in mental hospital admission. Int J Law Psychiatry 1997;20(2):227-41.
52. Hoge SK, Lidz CW, Eisenberg M, Monahan J, Bennett N, Gardner W, et al. Family, clinician, and patient perceptions of coercion in mental hospital admission. A comparative study. Int J Law Psychiatry 1998;21(2):131-46.
53. Monahan J, Hoge SK, Lidz C, Roth LH, Bennett N, Gardner W, et al. Coercion and commitment: understanding involuntary mental hospi-tal admission. Int J Law Psychiatry 1995;18(3):249-63.
54. Lidz CW, Mulvey EP, Hoge SK, Kirsch BL, Monahan J, Bennett NS, et al. The validity of mental patients' accounts of coercion-related be-haviors in the hospital admission process. Law Hum Behav 1997;21(4):361-76.
55. Lidz CW, Mulvey EP, Hoge SK, Kirsch BL, Monahan J, Eisenberg M, et al. Factual sources of psychiatric patients' perceptions of coercion in the hospital admission process. Am J Psychiatry 1998;155(9):1254-60.
56. Nicholson RA, Ekenstam C, Norwood S. Coercion and the outcome of psychiatric hospitalization. Int J Law Psychiatry 1996;19(2):201-17.
57. Cascardi M, Poythress NG, Hall A. Procedural justice in the context of civil commitment: an analogue study. Behav Sci Law 2000;18(6):731-40.
58. Sjoberg RL, Lindblad F. Delayed disclosure and disrupted communica-tion during forensic investigation of child sexual abuse: a study of 47 corroborated cases. Acta Paediatr 2002;91(12):1391-6.
59. Sjoberg RL. False claims of victimization: a historical illustration of a contemporary problem. Nord J Psychiatry 2002;56(2):132-6.
60. Widom CS, Weiler BL, Cottler LB. Childhood victimization and drug abuse: a comparison of prospective and retrospective findings. J Consult Clin Psychol 1999;67(6):867-80.
61. Williams LM. Recall of childhood trauma: a prospective study of women's memories of child sexual abuse. J Consult Clin Psychol 1994;62(6):1167-76.
62. Loftus EF, Garry M, Feldman J. Forgetting sexual trauma: what does it mean when 38% forget? J Consult Clin Psychol 1994;62(6):1177-81; discussion 1182-6.
63. Pope HG, Jr., Hudson JI. Can memories of childhood sexual abuse be repressed? Psychol Med 1995;25(1):121-6.
64. Pope HG, Jr., Hudson JI, Bodkin JA, Oliva P. Questionable validity of 'dissociative amnesia' in trauma victims. Evidence from prospective studies. Br J Psychiatry 1998;172:210-5; discussion 216-7.

60
65. Pope HG, Jr., Oliva PS, Hudson JI, Bodkin JA, Gruber AJ. Attitudes toward DSM-IV dissociative disorders diagnoses among board-certified American psychiatrists. Am J Psychiatry 1999;156(2):321-3.
66. Brandon S, Boakes J, Glaser D, Green R. Recovered memories of child-hood sexual abuse. Implications for clinical practice. Br J Psychiatry 1998;172:296-307.
67. Brewin CR, Andrews B. Recovered memories of trauma: phenomenol-ogy and cognitive mechanisms. Clin Psychol Rev 1998;18(8):949-70.
68. Ceci SJ, Huffman ML. How suggestible are preschool children? Cogni-tive and social factors. J Am Acad Child Adolesc Psychiatry 1997;36(7):948-58.
69. Bottoms BL, Shaver PR, Goodman GS. An analysis of ritualistic and religion-related child abuse allegations. Law and Human Behaviour 1996;20:1-34.
70. Lanning KV. Ritual abuse: a law enforcement view or perspective. Child Abuse Negl 1991;15(3):171-3.
71. Sjoberg RL, Lindblad F. Limited disclosure of sexual abuse in children whose experiences were documented by videotape. Am J Psychiatry 2002;159(2):312-4.
72. Lyon TD. The new wave in children's suggestibility research: A critique. Cornell Law Review 1999;1999(84):1004-87.
73. Johnson MK, Hashtroudi S, Lindsay DS. Source monitoring. Psychol Bull 1993;114(1):3-28.
74. Johnson MK, Raye CL. Reality Monitoring. Psychological Review 1981;88:67-85.
75. Andersson P. Predicting health behaviour : population-based studies of knowledge and behaviour related to cardiovascular diseases. Upp-sala: Acta Universitatis Upsaliensis, 2006.
76. Fiske ST, Taylor SE. Social cognition. New York: McGraw-Hill, 1991. p. 507.
77. Haglund K, Von Knorring L, Von Essen L. Forced medication in psychi-atric care: patient experiences and nurse perceptions. J Psychiatr Ment Health Nurs 2003;10(1):65-72.
78. Lidz CW, Mulvey EP, Hoge SK, Kirsch BL, Monahan J, Bennett NS, et al. Sources of coercive behaviours in psychiatric admissions. Acta Psychiatr Scand 2000;101(1):73-9.
79. Olofsson B, Jacobsson L. A plea for respect: involuntarily hospitalized psychiatric patients' narratives about being subjected to coercion. J Psychiatr Ment Health Nurs 2001;8(4):357-66.
80. Conlon P, Merskey H, Zilli C, Frommhold K. The attitudes toward committal of patients hospitalized in a psychiatric facility for the first time. Can J Psychiatry 1990;35(4):324-7.
81. Kane JM, Quitkin F, Rifkin A, Wegner J, Rosenberg G, Borenstein M. Attitudinal changes of involuntarily committed patients following treatment. Arch Gen Psychiatry 1983;40(4):374-7.

61
82. Toews J, el-Guebaly N, Leckie A, Harper D. Patients' attitudes at the time of their commitment. Can J Psychiatry 1984;29(7):590-5.
83. Edelsohn GA, Hiday VA. Civil commitment: a range of patient attitudes. Bull Am Acad Psychiatry Law 1990;18(1):65-77.
84. Svensson B, Hansson L. Patient satisfaction with inpatient psychiatric care. The influence of personality traits, diagnosis and perceived co-ercion. Acta Psychiatr Scand 1994;90(5):379-84.
85. Naber D, Kircher T, Hessel K. Schizophrenic patients' retrospective atti-tudes regarding involuntary psychopharmacological treatment and restraint. Eur Psychiatry 1996;11(1):7-11.
86. Gardner W, Lidz CW, Hoge SK, Monahan J, Eisenberg MM, Bennett NS, et al. Patients' revisions of their beliefs about the need for hospi-talization. Am J Psychiatry 1999;156(9):1385-91.
87. Langle G, Renner G, Gunthner A, Stuhlinger M, Eschweiler G, U'Ren R, et al. Psychiatric commitment: patients' perspectives. Med Law 2003;22(1):39-53.
88. Lauber C, Nordt C, Falcato L, Rossler W. Public attitude to compulsory admission of mentally ill people. Acta Psychiatr Scand 2002;105(5):385-9.
89. Kullgren G, Jacobsson L, Lynoe N, Kohn R, Levav I. Practices and atti-tudes among Swedish psychiatrists regarding the ethics of compul-sory treatment. Acta Psychiatr Scand 1996;93(5):389-96.
90. Lepping P, Steinert T, Gebhardt RP, Rottgers HR. Attitudes of mental health professionals and lay-people towards involuntary admission and treatment in England and Germany--a questionnaire analysis. Eur Psychiatry 2004;19(2):91-5.
91. Olofsson B. Use of coercion in psychiatric care as narrated by patients, nurses and physicians. Umeå: Univ., 2000.
92. Lauber C, Falcato L, Rossler W. Attitudes to compulsory admission in psychiatry. Lancet 2000;355(9220):2080.
93. Reed F, Fitzgerald L. The mixed attitudes of nurse's to caring for people with mental illness in a rural general hospital. Int J Ment Health Nurs 2005;14(4):249-57.
94. Weiner DB. Philippe Pinel's "Memoir on Madness" of December 11, 1794: a fundamental text of modern psychiatry. Am J Psychiatry 1992;149(6):725-32.
95. Swartz MS, Swanson JW, Hiday VA, Wagner HR, Burns BJ, Borum R. A randomized controlled trial of outpatient commitment in North Carolina. Psychiatr Serv 2001;52(3):325-9.
96. Weiden PJ, Olfson M. Cost of relapse in schizophrenia. Schizophr Bull 1995;21(3):419-29.
97. Swartz MS, Swanson JW, Hiday VA, Borum R, Wagner HR, Burns BJ. Violence and severe mental illness: the effects of substance abuse and nonadherence to medication. Am J Psychiatry 1998;155(2):226-31.

62
98. Swartz MS, Swanson JW, Hiday VA, Borum R, Wagner R, Burns BJ. Taking the wrong drugs: the role of substance abuse and medication noncompliance in violence among severely mentally ill individuals. Soc Psychiatry Psychiatr Epidemiol 1998;33 Suppl 1:S75-80.
99. Kisely S, Campbell LA, Preston N. Compulsory community and invol-untary outpatient treatment for people with severe mental disorders. Cochrane Database Syst Rev 2005(3):CD004408.
100. Kjellin L, Andersson K, Candefjord IL, Palmstierna T, Wallsten T. Ethical benefits and costs of coercion in short-term inpatient psychi-atric care. Psychiatr Serv 1997;48(12):1567-70.
101. Steinert T, Schmid P. Effect of voluntariness of participation in treat-ment on short-term outcome of inpatients with schizophrenia. Psy-chiatr Serv 2004;55(7):786-91.
102. Katsakou C, Priebe S. Outcomes of involuntary hospital admission--a review. Acta Psychiatr Scand 2006;114(4):232-41.
103. Clarke P, Hafner RJ, Holme G. The brief admission unit in emergency psychiatry. J Clin Psychol 1997;53(8):817-23.
104. Hoenig J, Hamilton MW. Elderly psychiatric patients and the burden on the household. Psychiatr Neurol (Basel) 1966;152(5):281-93.
105. Hoenig J, Hamilton MW. The schizophrenic patient in the community and his effect on the household. Int J Soc Psychiatry 1966;12(3):165-76.
106. Perlick D, Clarkin JF, Sirey J, Raue P, Greenfield S, Struening E, et al. Burden experienced by care-givers of persons with bipolar affective disorder. Br J Psychiatry 1999;175:56-62.
107. Ostman M, Hansson L, Andersson K. Family burden, participation in care and mental health--an 11-year comparison of the situation of relatives to compulsorily and voluntarily admitted patients. Int J Soc Psychiatry 2000;46(3):191-200.
108. Wittmund B, Wilms HU, Mory C, Angermeyer MC. Depressive disor-ders in spouses of mentally ill patients. Soc Psychiatry Psychiatr Epidemiol 2002;37(4):177-82.
109. Nordstrom A. Violent offenders with schizophrenia. Umeå: Univ., 2004. 110. Overall J, Gorham D. The Brief Psychiatric Rating Scales. Psychologi-
cal Reports 1962;10:799-812. 111. Hoyer G, Kjellin L, Engberg M, Kaltiala-Heino R, Nilstun T, Sigur-
jonsdottir M, et al. Paternalism and autonomy: a presentation of a Nordic study on the use of coercion in the mental health care system. Int J Law Psychiatry 2002;25(2):93-108.
112. APA. Diagnostic and Statistical Manual of Mental Disorders. 4th ed. Washington, DC: American Psychiatric Association, 1994.
113. Cantrill H. The pattern of human concern. New Brunswick, Nj: Rutgers University Press, 1965.
114. Candefjord IL, Lampinen K, Ängfors G. Patienters upplevelse av akut psykiatrisk vård. (Patients´experiences of short-term inpatient psy-chiatric care. In Swedish). Social-Medicinsk Tidskrift 1994;71:447-53.

63
115. Ostman M, Hansson L. Family burden and care participation. A test-retest reliability study of an interview instrument concerning fami-lies with a severely mentally ill family member. Nordic Journal of Psychiatry 2000;54:327-32.
116. APA. Diagnostic and Statistical Manual of Psychiatric Disorders. 3rd revised ed. Washington DC: American Psychiatric Association, 1987.
117. Sjoberg RL. [A critical question: Therapeutic effect or regression to-wards the mean?]. Lakartidningen 2006;103(26-27):2057-8.
118. Foucault M. Vansinnets historia under den klassiska epoken. Stock-holm: Aldus/Bonnier, 1973.
119. Gilbody SM, House AO, Sheldon TA. Outcomes research in mental health. Systematic review. Br J Psychiatry 2002;181:8-16.
120. Becker I, Vazquez-Barquero JL. The European perspective of psychiat-ric reform. Acta Psychiatr Scand Suppl 2001(410):8-14.
121. Fakhoury W, Priebe S. The process of de-institutionalisation: an inter-national overview. Current Opinion of Psychiatry 2002;15:187-192.
122. Stefansson CG, Cullberg J. Introducing community mental health ser-vices. The effects on a suburban patient population. Acta Psychiatr Scand 1986;74(4):368-78.
123. Stefansson CG, Cullberg J, Steinholtz Ekecrantz L. From community mental health services to specialized psychiatry: the effects of a change in policy on patient accessibility and care utilization. Acta Psychiatr Scand 1990;82(2):157-64.
124. SOU 1992:73. Välfärd och valfrihet : service, stöd och vård för psykiskt störda : slutbetänkande. Stockholm: Allmänna förl., 1992.
125. Stefansson CG, Hansson L. Mental health care reform in Sweden, 1995. Acta Psychiatr Scand Suppl 2001;(410):82-8.
126. SOU 2006:100. Ambition och ansvar : nationell strategi för utveckling av samhällets insatser till personer med psykiska sjukdomar och funktionshinder : slutbetänkande. Stockholm: Fritze, 2006.

Acta Universitatis UpsaliensisDigital Comprehensive Summaries of Uppsala Dissertationsfrom the Faculty of Medicine 326
Editor: The Dean of the Faculty of Medicine
A doctoral dissertation from the Faculty of Medicine, UppsalaUniversity, is usually a summary of a number of papers. A fewcopies of the complete dissertation are kept at major Swedishresearch libraries, while the summary alone is distributedinternationally through the series Digital ComprehensiveSummaries of Uppsala Dissertations from the Faculty ofMedicine. (Prior to January, 2005, the series was publishedunder the title “Comprehensive Summaries of UppsalaDissertations from the Faculty of Medicine”.)
Distribution: publications.uu.seurn:nbn:se:uu:diva-8607
ACTA
UNIVERSITATIS
UPSALIENSIS
UPPSALA
2008