Embed Size (px)
Citation preview

November 6, 2014
Presenter:
Robert P. Heaney, MDJohn A. Creighton University Professor/Professor of Medicine
Creighton UniversityModerator:
James M. Rippe, MD – Leading cardiologist, Founder and Director, Rippe Lifestyle Institute
Approved for 1 CPE (Level 2) by the Commission on Dietetic Registration, credentialing
agency for the Academy of Nutrition and Dietetics.
NUTRI-BITES®
Webinar Series
Sodium: Too much, too little or just
right?
Original recording of the November 6, 2014 webinar and PDF download of presentation available at:www.ConAgraFoodsScienceInstitute.com

Based on this webinar the participant will be able to:Review the evolution of sodium intake recommendationsUnderstand the physiology related to regulating sodium metabolismDiscuss latest findings of the association of sodium intake to health outcomesOutline practical dietary strategies dietitians can offer clients as the science on sodium evolves
NUTRI-BITES®
Webinar Series
Sodium: Too much, too little or just right?

CU ORC
SOME SODIUM INTAKE FACTS 2004 IOM recommendations for adults:
< 1,500 mg/day up to age 50< 1,300 mg/day from 50 to 70< 1,200 mg/day after age 70
mean Na intake in U.S. & Europe:3,450 mg/day (95% probability range: 2,600–5,000 mg/day)
this intake has been stable for at least 50 years in forty five 1st world nations

CU ORC
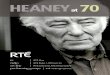
NUTRIENT RESPONSE CURVE*
Intake of Nutrient
Risk
of D
eficien
cy
Risk
of T
oxicity
UL
RDA
EAR
*DRI book; IOM (2006)

CU ORC
RISK AT BOTH EXTREMES
5
Intake
Risk
of H
arm
deficiencytoxicity

CU ORC
THE DRI PROCESS
first, the consequences of inadequate and excessive intakes are defined
data describing intakes needed to avoid those consequences is gathered
an intake just sufficient to avoid inadequacy is defined as the requirement
recognizing that individuals will have differing requirements, an average requirement is estimated (the EAR)
6

CU ORC
THE SODIUM DRIs
the IOM noted that Na effects arose not from Na, per se, but from NaCl, the form in which ~90% of ingested Na enters the body
the IOM stated that there was not enough evidence regarding NaCl effects to establish the usual DRIs, and so proposed, instead, an AI
7

CU ORC
THE SODIUM DRIs
the adverse effect with increasing salt intake, which the AI seeks to minimize, is elevated blood pressure
the IOM, in effect, ignored adverse effects at low intakes, i.e., the panel used a linear model rather than a U-shaped model
this explains why the BP data and the health outcomes data disagree
8

CU ORC
STARTING INTAKE MATTERS
9
Intake
Risk
of H
arm
H
ealt
h o
utc
om
es
are
the
pro
xy

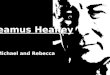
CVD RISK vs. Na INTAKE
17 country study
N = 101,945 mean follow-
up: 3.7 years O’Donnell et
al. NEJM 371:612 (2014)
10
Sodium Excretion (g/day)
0 2 4 6 8 10 12
Odds R
atio
1.0
1.5
2.0
2.5
3.0

CU ORC
11
DASH–I*
three-way trial of dietary intervention standard American diet diet high in fruits and vegetables diet high in fruits & vegetables plus
low-fat milk (~730 mg extra Ca)
Na intake held constant at ~3000 mg across all three diets
*Appel et al., NEJM 1997; 336:1117-24

CU ORC
12
DASH-I: Conclusions
BP reduction was as large as produced by standard anti-hypertensive mono-therapy regimens
if applied at a population level, the full DASH diet would reduce incidence of stroke by 27 % MIs by 15 %

CU ORC
13
DASH – ANOTHER CONCLUSION the possibly harmful effects of high
Na intake are magnified when the diet is inadequate in Ca and K
high Ca & K intakes mitigate the possible harm of high Na intakes

CU ORC
THE NUTRIENT PROBLEM
the field lacks a consensus on how to define “normal” or “adequate”
that leaves the field virtually without a target to aim at
and forces reliance upon empirical evidence that, e.g., intake A is “better” by some measurable endpoint than intake B
the evidence must be in the form of RCTs
14

RAAS – A RESCUE MECHANISM
sympathetic activity
NaCl reabsorption & water retention
aldosterone secretion
arteriolar constriction & rise in BP
ADH secretion from pituitary
15
angiotensinogen
renin
angiotensin I angiotensin II
ACE
renal
blood flow
. . . but notice: when you
reduce Na intake below a
critical level, you activate
mechanisms that try to raise
BP

CU ORC
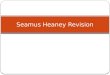
RISK CURVE FOR BP LOWERING 5-yr non-
concurrent cohort study
398,419 hypertensive pts. at Kaiser SoCal
risk of death &/or ESRD
Sim et al., J Am Coll Cardiol 2014; 64:588–97
Systolic Blood Pressure
<110110–120
120–130
130–140
140–150
150–160
160–170
>170A
dju
sted H
azard
Ratio
0
1
2
3
4
5
6
7

CU ORC
CONCLUSIONS the risk curve for Na is the same as for
other nutrients: U-shaped risk of harm rises at both extremes of
intake the lowest risk range seems to be at about
the current U.S. average Na intake there is no evidence to justify efforts to
decrease average salt intake we should be emphasizing increasing Ca
and K intakes, rather than decreasing Na intake