Embed Size (px)
Citation preview

Novel Twelve-Generation Kindred of Fatal FamilialInsomnia From Germany Representing the EntireSpectrum of Disease Expression
Anja Harder,1 Klaus Jendroska,2 Friedmar Kreuz,3 Torsten Wirth,4 Constanze Schafranka,1Nadja Karnatz,1 Aguta Theallier-Janko,5 Jens Dreier,2 Karsten Lohan,1 Dirk Emmerich,6Jorge Cervos-Navarro,5 Otto Windl,7 Hans A. Kretzschmar,7 Peter Nurnberg,1 andRegine Witkowski1*1Institut fur Medizinische Genetik, Universitatsklinikum Charite, Humboldt-Universitat zu Berlin, Berlin, Germany2Klinik fur Neurologie, Universitatsklinikum Charité, Humboldt-Universitat zu Berlin, Berlin, Germany3Institut fur Klinische Genetik, Universitatsklinikum Carl-Gustav Carus, Technische Universitat Dresden,Dresden, Germany
4Klinik fur Innere Medizin, Kliniken Erlabrunn GmbH, Erlabrunn, Germany5Institut fur Neuropathologie, Universitatsklinikum Benjamin Franklin, Freie Universitat Berlin, Berlin, Germany6Institut fur Humangenitik und Anthropologie, Albert-Ludwigs-Universitat, Freiburg, Germany7Institut fur Neuropathologie, Universitat Gottingen, Gottingen, Germany
We present a novel large German kindred offatal familial insomnia (FFI) consisting ofthree branches and comprising more than800 individuals of 12 generations, the larg-est pedigree of any familial prion diseaseknown today. There is a wide spectrum ofclinical presentations leading to misdiag-noses of Olivo-Ponto-Cerebellar Atrophy(OPCA), Parkinson’s or Alzheimer’s diseasein addition to Creutzfeldt-Jakob disease(CJD) and Gerstmann-Straussler-Scheinker(GSS) syndrome. Molecular genetic analysisof the prion protein gene (PRNP) confirmedthe mutation D178N segregating with me-thionine at the polymorphic codon 129 ofPRNP in all 7 patients examined. This poly-morphism at codon 129 is supposed to dis-criminate between familial CJD (fCJD) andFFI; the 129M allele determines FFI and129V fCJD. Furthermore, heterozygosity atthis site appears to induce prolonged dis-ease duration as compared to the homozy-gous condition. The variability of the clini-cal and pathological findings documentedfor our patients indicates the difficulty inestablishing the diagnosis of FFI on clinicaland on pathological grounds alone. In threecases (IX-97, XI-21, V-2) followed up by usprospectively insomnia was an early and se-
vere symptom; however, in case notes ana-lyzed retrospectively this symptom was fre-quently missed. In contrast to previous re-ports and in agreement with recent studieswe cannot confirm a clear relationship be-tween the status of the M/V polymorphismat codon 129 and the age-of-onset of this dis-ease. Am. J. Med. Genet. 87:311–316, 1999.© 1999 Wiley-Liss, Inc.
KEY WORDS: prion disease; PRNP muta-tion D178N; fatal familial in-somnia (FFI); Creutzfeldt-Jakob disease; CJD; fCJD
INTRODUCTION
Transmissible spongiform encephalopathies affectboth humans and animals. Current pathogenetic con-cepts are based on a proteinaceous infectious particle,termed Prion [Prusiner, 1982]. Approximately 15% ofcases of human prion disease occur familially, beinglinked to different dominant mutations of the prionprotein gene (PRNP): familial Creutzfeldt-Jakob dis-ease (fCJD) and all cases of both Gerstmann-Straussler-Scheinker syndrome (GSS) and fatal famil-ial insomnia (FFI). About 85 to 90% of Creutzfeldt-Jakob disease (CJD) cases are sporadic, occasionalcases have an iatrogenic or with some probabilityorally infectious background (“new variant”; nvCJD).Kuru, a further distinct type of prion disease is ob-served in a tribe in New Guinea where it is transmittedby ingesting brain tissue of affected relatives duringcannibalistic rites.
The PRNP gene is located on chromosome 20 (pter-
*Correspondence to: Regine Witkowski, Institute of MedicalGenetics, Humboldt University Medical School, Charite, Luis-enstr 13a, 10098 Berlin, Germany.E-mail: [email protected]
Received 30 March, 1999; Accepted 10 July 1999
American Journal of Medical Genetics 87:311–316 (1999)
© 1999 Wiley-Liss, Inc.

p12) and consists of two exons. Recently published datasuggest an additional 58-noncoding exon [Lee et al.1998]. Exon 2 is comprising the whole open readingframe of 759 bp encoding for 2.4 kb mRNA [Oesch et al.,1985; Robakis et al., 1986; Kretzschmar et al., 1986;Puckett et al., 1991]. To date 14 different point muta-tions are known as well as 8 octarepeat sequence ex-pansions leading to fCJD, GSS, or FFI. A correlationbetween the location of the mutation within the exonand the clinical type of disease has not yet been estab-lished. Clinical phenotypic differences between thethree familial diseases are apparently related to thedistribution of brain pathology. FFI is characterized byuntreatable insomnia in addition to autonomic, endo-crine, and motor dysfunctions. The leading manifesta-tions are attributed to lesions originally thought to berestricted to the anterior and dorsomedial thalamic nu-clei [Lugaresi et al., 1986; Lugaresi, 1992]. However,familial CJD and FFI, show considerable phenotypicvariation even within a family or a sibship.
The D178N mutation of PRNP has been described in9 families of CJD [Goldfarb et al., 1992a, 1992b;Bosque et al., 1992; Kretzschmar et al., 1995] and inabout 20 families and one further possibly sporadiccase with FFI phenotype [Lugaresi et al., 1986; Medoriet al., 1992; Petersen et al., 1992; Medori andTritschler, 1993; Reder et al., 1995; Silburn et al., 1996;Nagayama et al., 1996; Colombier et al., 1997; McLeanet al., 1997; Rossi et al., 1998] in worldwide distribu-tion. The clinical and neuropathological differences be-tween fCJD and FFI both caused by the same D178Nmutation have been attributed to the 129M/V polymor-phism [Goldfarb et al., 1992a] which was found to beassociated with different isoforms of proteinase resis-tant prion protein (PrPres) in fCJD and FFI patients[Monari et al., 1994]. In all cases reported so far, asso-ciation of the 129Met allele with the D178N mutationpredisposed to FFI while the 129Val allele was associ-ated with fCJD. Furthermore, homo- or heterozygosityof codon 129 is supposed to influence the age of diseaseonset, its duration, and phenotypic expression [Gam-betti et al., 1995; Goldfarb et al., 1992a; Reder et al.,1995]. We report on an extensive German kindred of 12generations comprising more than 800 individuals andapproximately 200 living potential carriers with af-fected patients exhibiting the mutation D178N segre-gating with 129M at the polymorphic site.
PATIENTS AND METHODSStudy Design
From an initial group of 4 sisters and 5 further pa-tients from the same region all suffering from priondisease, we obtained pedigrees that were traced usinginformation from registry offices, parish registers, andpersonal communications. To look for a common ances-tor parish registers were searched for names, dates ofbirth, baptisms, and marriages, as well as dates andcauses of death in more than 25 towns and villages inthe Erzgebirge mountains of Saxony, South East Ger-many.
To prove the diagnosis, a blood sample or autopsymaterial was obtained from 7 cases for genomic muta-
tion analysis of PRNP. In two cases (IX-90 and IX-95)no suitable material was available, however, kinship tothe other affected individuals with proven mutationwas confirmed. Nine patients had clinical documenta-tion and autopsy and neuropathological investigationswere performed in 6 cases. Three cases (IX-97, XI-21,V-2) were followed up by us after mutation analysisbecame available.
Genomic Mutation Analysis
Genomic DNA was prepared by standard proceduresand 100 ng were used for polymerase chain reaction(PCR): 750 nM of each primer, 200 mM of each dNTP,10 mM Tris-HCl (pH 4 8.4), 50 mM KCl, 1.5 mMMgCl2, 0.001% w/v gelatine, 2.5 U Taq-Polymerase(Perkin Elmer). Primer pairs for the first nested PCRwere applied according to Hsiao et al. [1992], leading toa product of 864 bp (primers K and H). The secondsemi-nested PCR leading to a 833 bp PCR product wascarried out using primer H (58-AAGGATCCCTCAAGC-TGGAAAAAGA-38) and primer A (58-ATGCTG-GTTCTCTTTGTGGC-38). For both reactions the sametemperature profile was used: pre-denaturation at96°C for 7 min; 30 cycles of denaturation at 96°C for 1min, annealing at 58°C for 1 min, elongation at 72°Cfor 2 min, and final elongation at 72°C for 10 min.
After checking PCR products on an agarose gel theywere directly sequenced applying the Cycle SequencingKit (Amersham) and radioactive labelled oligonucleo-tides using T4 Polynucleotide Kinase (Promega) andg33ATP (NEN-DuPont). Labelling was carried out at37°C for 45 min and denaturation at 95°C for 5 min(modified according to Promega product information).Radioactive products were analyzed on a 6% denatur-ating polyacrylamide gel in TBE buffer. After drying,the gel was exposed to an X-ray film for 2 days. Thefollowing sequencing primers were used: KH02, KH03,KH06 (antisense) [Hsiao et al., 1992], K5, K7 [Kita-moto et al., 1993], and PRBK (58-TAACGTCGGTCTC-GGTGAAG-38, antisense).
Restriction Enzyme Analysis
Endonuclease cleavage was carried out to distin-guish alleles for the 129M/V polymorphism in cases ofheterozygosity detected by sequencing. A 393 bp frag-ment between nucleotides 320 and 713 was amplifiedand digested with restriction enzymes MaeII and AspIaccording to Goldfarb et al. [1992a].
RESULTSClinical Data
Patients with this familial prion disease were clini-cally documented, PRNP mutations were analyzed andpost mortem examinations carried out. They belongedto three different pedigrees (A, B, C) and presentedwith different leading clinical symptoms, courses, agesof onset, and durations of illness. The main data arepresented in Table I.
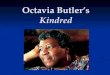
Five cases belonged to kindred A. Four sisters as wellas one distant relative were affected and are shown inFigure 1 with display of relevant relationships.
312 Harder et al.

Patient IX-77 (A). Initial symptoms of disease atthe age of 53 years were attacks of cardiasthenia anddepression which was progressive despite therapy.Five months later a diagnosis of a dementia was madeand two months later the patient was admitted forpneumonia. At this time he was completely disorientedand somnolent. A diagnosis of Gerstmann Straussler-Scheinker syndrome was considered when the familyhistory was recognized. No prominent neurological ab-normalities were noted. Death occurred 6 months afterdisease onset of pneumonia. At autopsy the brain ap-peared normal, however, on histopathological exami-nation discrete spongiform change associated with glio-sis was observed in the cerebral cortex and basal gan-glia. Amyloid plaques were not found.
Patient IX-90 (A). The patient’s history was char-acterized by prominent psychiatric abnormalities.Vivid nightmares and insomnia were the first symp-toms recognized at age 54 years. Increasing restless-ness, severe weight loss, auditory and later visual hal-lucinations, paranoia, as well as depression followedover the next two years. Cranial CT and EEG werenormal at that time. Dementia and drug-resistant psy-chosis developed. Then progressive ataxia, dysarthria,dysphagia, hyperactive reflexes with Babinskis signwere noted. EEG showed generalized slowing but noperiodic activity typical of CJD. Finally, dementia pro-gressed rapidly, extrapyramidal signs developed, andmyoclonic jerks appeared frequently. Usually she waseither somnolent or confused and hallucinating. Death
was due to pneumonia after a disease duration of al-most 3 years. Brain autopsy showed mild frontal andparietal cortical as well as brainstem and thalamic at-rophy. There was partial demyelination and spongiosisof the corpus callosum, of the central parietal and oc-cipital white matter and of the internal capsule. Medialanterior thalamic nuclei showed severe astrocytosisand loss of neurons. Moderate gliosis was found in thehypothalamus and olives. Thalamo-nigro-bulbospinalatrophy was diagnosed with atrophy of the inferior ol-ives.
Patient IX-93 (A). Progressive ataxia, parkinso-nian features, dysarthria and insomnia were symp-toms of the patient from age 70. The relatives recog-nized them as symptoms of the disease running in theirfamily. Death occurred six months after disease onset.An autopsy was not carried out.
Patient IX-95 (A). Disease began at age 62 withfatigue, daytime sleepiness, depression, decreasing ef-ficiency, and severe weight loss. Disorientation, confu-sion, and blurring of speech followed. Seven monthslater the patient was admitted suffering from severeataxia, dysarthria, and hallucinations. However, cra-nial CT and CSF were normal, multiple hyperintenselesions of the white matter were seen in brain MRIscans which were neither typical of vascular nor of in-flammatory change. The mental syndrome was pro-gressive. She was somnolent, completely disoriented,and occasionally agitated. Choreatic movements andrigidity were noted but no myoclonus occurred. She
Fig. 1. Extract from pedigree A including clinically described patients with relevant relationships. Numbering is equivalent to the full pedigree whichcan be provided by authors on request. Symbol descriptions: h, male; s, female; filled, affected individuals; ?, possibly affected; (, carrier; N, not affected;+, dead before manifestation age; /, dead; h
–, no children in descendence; s
–, DNA examined for mutation.
TABLE I. Age at Onset, Duration of Illness, and Previous Diagnoses of the Individuals of Kindreds A, B, C in Comparison toPolymorphism V129M
Individual(pedigree) Sex
Onset(years)
Duration(months) Clinical diagnosis
Neuropathologicaldiagnosis
Geneticdiagnosis
D178N(yes 4 +) Codon 129
IX-77 (A) Male 53 6 Alzheimer’s disease, GSS GSS, but atypical FFI + 129MIX-90 (A) Female 54 32 CJD Atypical CJD None No DNA No DNAIX-93 (A) Female 70.5 6 Prion disease None FFI + 129MIX-95 (A) Female 62 10 Dementing disorder Morbus Fahr None No DNA No DNAIX-97 (A) Female 44 44 CJD CJD FFI + 129M/VX-7 (B) Female 70.5 6 OPCA FFIb FFI + 129MX-9 (B) Male 58.5 6 Mult. syst. atrophya None FFI + 129MXI-21 (B) Male 47 8 CJD/FFIb FFIb FFI + 129MV-2 (C) Female 47.5 41 FFIb Noneb FFI + 129M/V
aMultiple system atrophy.bDiagnosis after known results of mutation analysis.
Novel German Kindred of FFI 313

died after 10 months of pneumonia. At autopsy thebrain was slightly atrophic, spongy edema was de-scribed in the cerebral and spinal white matter as wellas basal ganglia. Calcification of small arteries mainlyof the basal ganglia suggested early Fahrs disease. Thediagnosis of CJD was rejected when 36 specimens ofcerebrum and cerebellum failed to demonstrate dis-ease-specific pathology.
Patient IX-97 (A). First signs and symptoms atage 43 years were ataxia, double vision and headache.After a period of complete remission depression, dysar-thria, dysmetria, tremor, brisk reflexes, and increasedmuscle tone of the right side developed. Progressivecortical and subcortical brain atrophy was seen in suc-cessive CT scans. About one year after disease onsetmemory disturbances, anxiety, paranoia, and halluci-nations became evident. After 15 months she had de-veloped dementia accompanied by cerebellar and ex-trapyramidal signs and somnolence. Three years afterdisease onset she was completely dependent. Therewas myoclonus, primitive reflexes, and increasedmuscle tone with Babinskis sign. She died 4 years afterdisease onset of pneumonia. The neuropathologist re-ported spongiform degeneration of the cerebral cortex,moderate astrocytosis, and loss of neurons predomi-nantly in the temporal lobe and in the cerebellar ver-mis. Severe neuronal loss associated with astrocytosiswas further seen in the inferior olives.
Three cases belonged to pedigree B (two sibs and ason of their grand-cousin).
Patient X-7 (B). At age 70 years this patient notedprogressive insomnia, general weakness, fatigue, andweight loss. Confusion and reduced attention were fol-lowed by dysarthria. Two months before death she wasadmitted because of dysphagia. At that time she suf-fered from kachexia, somnolence, dysarthria, contrac-tion of both hips and feet, and muscle hypotonia. Shedied 6 months after disease onset of cardiac failure. Onautopsy there was brain edema and ventricular en-largement. Focal spongiform degeneration was foundaffecting the laminae II-IV of the frontal and parietalcortex as well as basal ganglia, pons, medulla oblon-gata, and the cerebellum. On histopathological exami-nation loss of neurons was prominent in the basal gan-glia, olives, cerebellum, and in the cervical spinal cord.Furthermore, the pons was atrophic and glial nodesand nerve cell vacuolization were reported in the pon-tine peduncles. Astrocytosis and vacuolization of re-maining occasional neurons was also described in theinferior olives.
Patient X-9 (B). Fatigue, weakness, and restless-ness were the first symptoms of the patient at age 58years. Kachexia and disturbances of the circadianrhythm were reported. The patient died 12 months af-ter disease onset. A neuropathological examinationwas not carried out.
Patient XI-21 (B). Disease began with insomniaand pruritus of the head and chest at the age of 47.Over the next two months weakness and anxiousnessdeveloped followed by poor attention, amnesia, and ir-ritability. Restlessness at night, confusion, disorienta-tion, progressive dementia, and disturbed perceptionled to admission. At that time insomnia and daytime
sleepiness as well as occasional myoclonic jerks werenoted. Repeated EEGs showed slowing but no periodicactivity. Results of neuroimaging studies and evokedpotentials were normal. The patient died 8 monthsafter disease onset of pneumonia. Neuropathologicalexamination showed severe nerve cell loss and astro-cytosis of the medial and anterior thalamic nuclei,moderate gliosis and neuronal depletion of the hypo-thalamus, tegmentum, cerebellar dentate nucleus andvermis, and inferior olives. There was no spongiosis ofthe cerebral cortex. Microglial activation was promi-nent in the olives, cerebellum, and tegmentum.
One patient (V-2) of pedigree C was clinically inves-tigated at age 47: Initial symptoms were insomnia, diz-ziness, ataxia, and night sweats. At that time cranialCT and evoked potentials were normal. EEG showedalpha rhythm with generalized theta-alpha-groups.The progress of the disease was characterized by inter-mittent ptosis, dysconjugate eye movements with ver-tical nystagmus, dysphagia, dysphonia, and fatigue.Twenty-one months after disease onset she sufferedfrom increasing ataxia, double vision, nocturnal confu-sion, hallucinations, and urinary incontinence. EEGshowed absence of normal sleep activity. The patientdied 41 months after disease onset of pneumonia. Noneuropathological examination was carried out.
Mutation Analysis
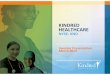
Results of mutation analysis of PRNP are shown inTable I. In all cases investigated the mutation D178Nwas detected by sequencing and co-segregation withthe 129M allele was confirmed. Association of D178Nwith the 129M allele was demonstrated in two (IX-97(A) and V-2 (C)) heterozygous cases by restriction en-donuclease cleavage and in the homozygous cases byradioactive sequencing (Fig. 2).
Summarizing the data of Table I it appears that het-erozygosity leads to considerably longer disease dura-tion, however, neither association between homozygos-ity (129M) and early age of onset nor between hetero-
Fig. 2. Mutation and polymorphism analyses by radioactive sequenc-ing. A: Mutation D178N (GAC → AAC) leading to exchange of aspartic acid(Asp) by asparagine (Asn). B: Homozygosity for methionine (ATG) at poly-morphic codon 129. In case of heterozygosity (V129M or ATG → GTG)restriction endonuclease cleavage was performed to determine the segre-gation of mutation and polymorphic codon.
314 Harder et al.

zygosity (V129M) and late onset of disease was found.Instead, the patient with the earliest manifestation(XI-97) was a heterozygote, whereas two homozygouspatients experienced first symptoms beyond the age of70 years.
Genealogical Studies
We compiled three pedigrees (A, B, and C) all origi-nating from the same region, the Erzgebirge in SouthEast Germany (Saxony). They comprise more than 800individuals in 12 generations. The D178N mutation ofthe prion gene was confirmed in all cases examined.
In pedigrees A and B we were able to trace ancestorsto the seventeenth century. This is before, according toMcGowan [1914], the first record of a prion disease insheep appeared in 1713. The ancestors of these twokindreds shared an identical surname and lived inclose proximity of about seven miles between their vil-lages. Kindred A contains 493 individuals from 11 gen-erations whereas B comprises 332 individuals of 12generations. Pedigree C which includes 47 individualsof 7 generations was traced to the eighteenth century.Their ancestors come from a region which is little morethan 25 miles from the one mentioned above but islocated within the same rural area.
Two further FFI kindreds with the D187N mutationand association to the 129M allele were found recentlyin two other German cities close to Saxony (H. Thiele,personal communication; R. Hauschild, personal com-munication). Some families of the presented kindredsmoved to other distant regions within Germany includ-ing Dresden, Heidelberg, Nurnberg, Heilbronn,Freiburg i.Br., Schweinfurt, Berlin, and Stuttgart. Fewrelatives moved abroad to Switzerland, Ecuador, andthe U.S. Therefore, the disease must be assumed tohave become quite widespread over the last decades.
DISCUSSIONPhenotypic Variability
A considerable variety of clinical and pathologicalphenotypic expression was observed in these patientsleading to a variety of diagnoses ranging from CJD,atypical CJD, GSS, Alzheimer’s disease, Morbus Fahr,multiple system atrophy, OPCA to FFI. Interestingly,the diagnosis of FFI was made only after PRNP se-quence analysis was available and the pedigrees be-came familiar to us. On clinical grounds alone and evenby histopathology we consider the diagnosis of this raredisease difficult to establish. In most case notes exam-ined by us retrospectively, insomnia was either ignoredor it was not considered an important specific diagnos-tic symptom. Furthermore, in an Australian kindredwith D178N genotype in conjunction with 129M fea-tures of CJD, FFI, and autosomal dominant cerebellarataxia (ADCA) were described [McLean et al., 1997].Thus, there is difficulty in distinguishing fCJD fromFFI phenotypes in some cases as supported by otheraccounts [Colombier et al., 1997; Chapman et al., 1996;Prusiner and Hsiaou, 1994; Kretzschmar and Windl,1998].
In accordance with previous reports [Gambetti et al.,1995] we found that patients manifested a long dura-
tion of disease (mean: 42.5 months) in cases of hetero-zygosity for the M/V at codon 129 whereas patientshomozygous for Met displayed a rapid course of illness(mean: 6.4 months). However, the disease durationmay also be substantially influenced by the age-of-onset rather than the polymorphism at codon 129 sinceall late-onset cases had a short survival. In contrast toother reports, our patients homozygous for the 129Mpolymorphism did not experience a particularly earlyonset of disease. This is in accordance to one recentreport by Montagna et al. [1998]; on the contrary twohomozygous patient fell ill after the age of 70, whereasone heterozygote was the youngest known patient af-fected in this kindred. The same observation was madeby Gambetti et al. [1995] and Goldfarb et al. [1992b].
With longer disease duration we find increasingsimilarity between CJD and FFI of both clinical andhistopathological expressions. Important distinguish-ing characteristics to consider are prominent insomniaand at least for some time a mild and fluctuating de-mentia in FFI with limited cerebral cortical pathologybut severe neuronal depletion, gliosis and some spon-giosis of thalamic, cerebellar and brain stem nuclei. Intypical cases of CJD, organic dementia is an earlysymptom and severe spongiform degeneration of cere-bral cortex accompanied by neuronal loss and astroglio-sis is the rule. The detailed case reports will be re-ported elsewhere (Jendroska et al., in preparation).
Consideration of a Founder Effect
Three probably related pedigrees originating fromthe same county were compiled comprising more than800 individuals. Pedigree A and B have been reduced tothe main individuals and relationships of interest forthis publication, however, they include over 1,100 in-dividuals. A kindred of this size has never been re-ported for any prion disease. Ancestors of pedigree Aand B were traced to the seventeenth century and areassumed to share the same ancestor because in addi-tion of having the same allele (which cannot be provedfor ancestors decades ago) their surnames were identi-cal and they lived in close proximity.
Considering that all three families come from thesame rural area which was relatively isolated up untiltwo centuries ago and that rapidly expanded in popu-lation a founder effect of the mutation D178N can beassumed. This may explain the high regional frequencyof the mutant allele in contrast to the low frequency ofone per million for prion disease in general. Althoughthe mutation D178N cannot be proven in cases whodied decades ago we have reason to suspect that thosein the early generations who died from pneumonia,nerve disease, brain tumor, or consumption at a rela-tively young age suffered from prion disease. The ge-nealogical tables presented support the view that theyall suffered from FFI which is traced back to one singlemutation originating from a de novo mutation of afounder or may have been introduced by a founder fromanother population.
Novel German Kindred of FFI 315

ACKNOWLEDGMENTS
We thank Mr. J. Schreiber for helping with the ge-nealogical studies.
REFERENCESBosque PJ, Vnencak-Jones CL, Johnson MD, Whitlock JA, McLean MJ.
1992. A PrP gene codon 178 base substitution and a 24-bp interstitialdeletion in familial Creutzfeldt-Jakob disease. Neurology 42:1864–1870.
Chapman J, Arlazaroff A, Goldfarb LG, Cervenakova L, Neufeld MY, Wer-ber E, Herbert M, Brown P, Gajdusek DC, Korczyn AD. 1996. Fatalfamilial insomnia in a case of familial Creutzfeldt-Jakob disease withthe codon 200Lys mutation. Neurology 46:758–761.
Colombier C, Geraud G, Delisle MB, Laplanche JL, Pavy-le-Traon A, AlizeP, Delpla PA. 1997. Insomnie fatale familiale: variation phenotypiquedeterminee par le polymorphisme du codon 129. Rev Neurol Paris 153:239–243.
Gambetti P, Parchi P, Petersen RB, Chen SG, Lugaresi E. 1995. Fatalfamilial insomnia and Creutzfeldt-Jakob diseases: clinical, pathologicaland molecular features. Brain Pathol 5:43–51.
Goldfarb LG, Petersen RB, Tabaton M, Brown P, LeBlanc AC, Montagna P,Cortelli P, Julien J, Vital C, Pendelbury WW, Haltia M, Wills PR,Hauw JJ, McKeever PE, Monari L, Schrank B, Swergold GD, Autilio-Gambetti L, Gajdusek DC, Lugaresi E, Gambetti P. 1992a. Fatal fa-milial insomnia and familial Creutzfeldt-Jakob disease: disease phe-notype determined by a DNA polymorphism. Science 258:806–808.
Goldfarb LG, Brown PB, Haltia M, Cathala F, McCombie WR, Kovanen J,Cervenakova L, Goldin L, Nieto A, Godec MS, Asher DM, Gajdusek DC.1992b. Creutzfeldt-Jakob disease cosegregates with the codon 178Asn
PRNP mutation in families of European origin. Ann Neurol 31:274–281.
Hsiao K, Dlouhy SR, Farlow MR, Cass C, Costa MD, Conneally PM, HodesME, Ghetti B, Prusiner S. 1992. Mutant prion proteins in Gerstmann-Straussler-Scheinker disease with neurofibrillary tangles. Nat Genet1:68–71.
Kitamoto T, Ohta M, Doh-ura K, Hitoshi S, Terao Y, Tateishi J. 1993.Novel missense variants of prion protein in Creutzfeldt-Jakob diseaseor Gerstmann-Straussler syndrome. BBRC 191:709–714.
Kretzschmar HA, Stowring LE, Westaway D, Stubblebine WH, PrusinerSB, Dearmond S. 1986. Molecular cloning of a human prion proteincDNA. DNA 5:315–324.
Kretzschmar HA, Neumann M, Stavrou D. 1995. Codon 178 mutation ofthe human prion protein gene in a German family (Backer family):sequencing data from 72-year old celloidin-embedded brain tissue. ActaNeuropathol 89:96–98.
Kretzschmar HA, Windl O. 1998. Spongiforme Enzephalopathien. In RießO, Schols L, editors. Neurogenetik, molekulargenetische Diagnostikneurologischer Erkrankungen. Heidelberg: Springer-Verlag Heidel-berg. p 95–107.
Lee IY, Westaway D, Smit AFA, Wang K, Seto J, Chen L, Acharya C,Ankener M, Baskin D, Cooper C, Yao H, Prusiner SB, Hood LE. 1998.Complete genomic sequence and analysis of the prion protein generegion from three mammalian species. Genome Research 8:1022–1037.
Lugaresi E, Medori R, Montagna P, Baruzzi A, Cortelli P, Lugaresi A,Tinuper P, Zucconi M, Gambetti P. 1986. Fatal familial insomnia anddysautonomia with selective degeneration of thalamic nuclei. N Engl JMed 315:997–1003.
Lugaresi L. 1992. The thalamus and insomnia. Neurology 42:28–33.
McGowan JP. 1914. Investigation into the disease of sheep called “Scra-pie”. Blackwood: Edinburgh.
McLean CA, Storey E, Gardner RJM, Tannenberg AEG, Cerevnakova L,Brown P. 1997. The D178N (cis-129M) “fatal familial insomnia” muta-tion associated with diverse clinicopathological phenotypes in an Aus-tralian kindred. Neurology 49:552–558.
Medori R, Montagna P, Tritschler HJ, LeBlanc A, Cortelli P, Tinuper P,Lugaresi E, Gambetti P. 1992. Fatal familial insomnia: a second kin-dred with mutation of prion protein gene at codon 178. Neurology 42:669–670.
Medori R, Tritschler H. 1993. Prion protein gene analysis in three kindredswith Fatal Familial Insomnia (FFI): codon 178 mutation and codon 129polymorphism. Am J Hum Genet 53:822–827.
Monari L, Chen SG, Brown P, Parci P, Petersen RB, Mikol J, Gray F,Cortelli P, Montagna P, Ghetti B, Goldfarb LG, Gajdusek DC, LugaresiE, Gambetti P, Autilio-Gambetti L. 1994. Fatal familial insomnia andfamilial Creutzfeld-Jacob disease: different prion proteins determinedby a DNA polymorphism. Pro Natl Acad Sci USA 91:2839–2842.
Montagna P, Cortelli P, Avoni P, Tinuper P, Plazzi G, Gallassi R, Porta-luppi F, Julien J, Vital C, Delisle MB, Gambetti P, Lugaresi E. 1998.Clinical features of fatal familial insomnia: phenotypic variability inrelation to a polymorphism at codon 129 of the prion protein gene.Brain Pathol 8:553–620.
Nagayama M, Shinohara Y, Furukawa H, Kitamoto T. 1996. Fatal familialinsomnia with a mutation at codon 178 of the prion protein gene: firstreport from Japan. Neurology 47:1313–1316.
Oesch B, Westaway D, Walchli M, McKinley MP, Kent SBH, Aebersold R,Barry RA, Tempst P, Teplow DB, Hood LE, Prusiner SB, Weissmann C.1985. A cellular gene encodes scrapie PrP 27-30 protein. Cell 40:735–746.
Petersen RB, Tabaton M, Berg L, Schrank B, Torack RM, Leal S, Julien J,Vital C, Deleplanque B, Pendlebury WW, Drachman D, Smith TW,Martin JJ, Oda M, Montagna P, Ott J, Autilio-Gambetti L, Lugaresi E,Gambetti P. 1992. Analysis of the prion protein gene in thalamic de-mentia. Neurology 42:1859–1863.
Prusiner SB. 1982. Novel proteinaceous infectious particles cause scrapie.Science 216:136–144.
Prusiner SB, Hsiao KK. 1994. Human prion disease. Ann Neurol 35:385–395.
Puckett C, Concannon P, Casey C, Hood L. 1991. Genomic structure of thehuman prion protein gene. Am J Hum Genet 49:320–329.
Reder AT, Mednick AS, Brown P, Spire JP, Van Cauter E, Wollmann RL,Cervenakova L, Goldfarb LG, Garay A, Ovsiew F, Gajdusek DC, RoosRP. 1995. Clinical and genetic studies of fatal familial insomnia. Neu-rology 45:1068–1075.
Robakis NK, Devine-Gage EA, Jenkins EC, Kascsak RJ, Brown WT, Kraw-czun MS, Silverman WP. 1986. Localization of a human gene homolo-gous to the PrP gene on the arm of chromosome 20 and detection ofPrP-related antigens in normal human brain. Biochem Biophys ResCommun 140:758–765.
Rossi G, Macci G, Porro M, Giaccone G, Bugiani M, Scarpini E, Scarlato G,Molini GE, Sasanelli F, Bugiani O, Tagliavini F. 1998. Fatal familialinsomnia: genetic, neuropathologic and biochemical study of a patientfrom a new Italian kindred. Neurology 50:688–692.
Silburn P, Cerevnakova L, Varghese P, Tannenberg A, Brown P, Boyle R.1996. Fatal familial insomnia: a seventh family. Neurology 47:1326–1328.
316 Harder et al.