Embed Size (px)
Citation preview
Effect of Venous Duplex Surveillance on VTE in the
Neurosurgical Population
Donato Pacione MD FAANS
Assistant Professor
Director of Quality Improvement
Department of Neurosurgery NYU School of Medicine
VTE in the Neurosurgical Population
• 1,777,035 Patients form the NSQIP database
• VTE 1.7%
•DVT 1.3%
• PE 0.6%
• Cranial 3.4% vs Spine 1.1%
• Independent Factors
• Ventilator Dependence
• Immobility (quadraparesis, hemiparesis, paraparesis)
•Malignancy
•Chronic Steroid Use
• Sepsis
Rolston JD et. Al. “What Clinical Factors predict deep venous
thrombosis and pulmonary embolism in Neurosurgical patients”.
Journal Neurosurgery Oct 121 (4) ,2014. 2
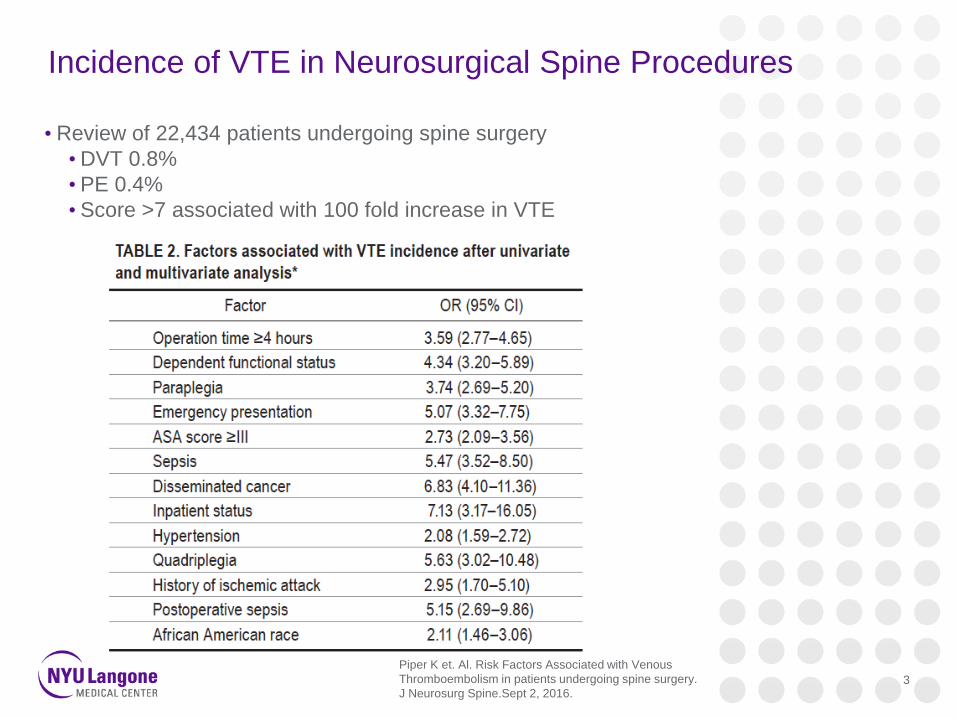
Incidence of VTE in Neurosurgical Spine Procedures
• Review of 22,434 patients undergoing spine surgery
•DVT 0.8%
• PE 0.4%
• Score >7 associated with 100 fold increase in VTE
Piper K et. Al. Risk Factors Associated with Venous
Thromboembolism in patients undergoing spine surgery.
J Neurosurg Spine.Sept 2, 2016.3
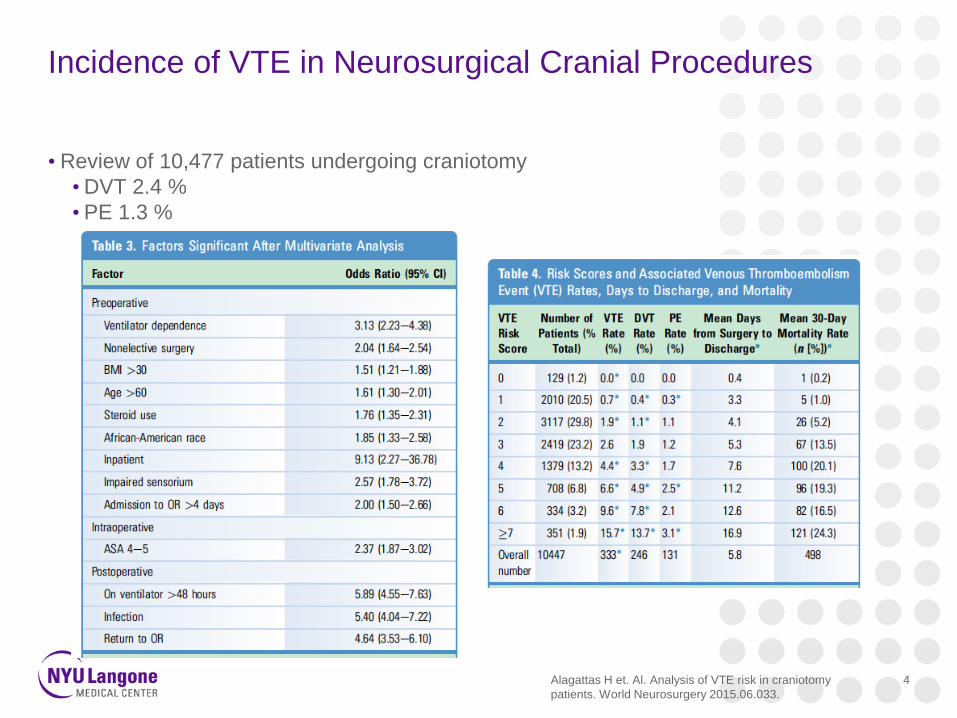
Incidence of VTE in Neurosurgical Cranial Procedures
• Review of 10,477 patients undergoing craniotomy
•DVT 2.4 %
• PE 1.3 %
Alagattas H et. Al. Analysis of VTE risk in craniotomy
patients. World Neurosurgery 2015.06.033.
4
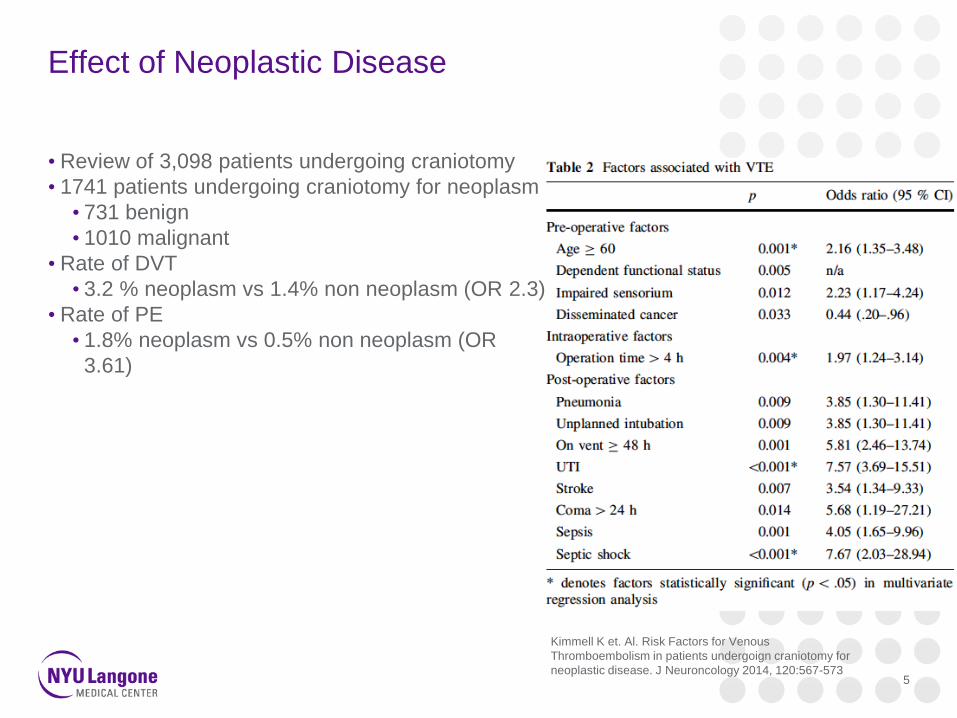
Effect of Neoplastic Disease
• Review of 3,098 patients undergoing craniotomy
• 1741 patients undergoing craniotomy for neoplasm
• 731 benign
• 1010 malignant
• Rate of DVT
• 3.2 % neoplasm vs 1.4% non neoplasm (OR 2.3)
• Rate of PE
• 1.8% neoplasm vs 0.5% non neoplasm (OR
3.61)
Kimmell K et. Al. Risk Factors for Venous
Thromboembolism in patients undergoign craniotomy for
neoplastic disease. J Neuroncology 2014, 120:567-5735
VTE in Malignant Glioma
• Examined 317 high grade glioma patients
• IDH 1 wild type
• VTE 26-30%
• IDH 1 mutant
• VTE 0%
• No significant difference in length of surgery or neurologic deficit
• IDH 1 wild type tumors found to have microthrombi
• IDH 1 mutant no evidence of microthrombi
• Confirmed IDH 1 mutant cells create antithrombotic activity
• Wild type GBM significantly more likely to develop VTE
PresenUnruh D, Schwarze SR, Khoury L, Thomas C, Wu
M, Chen L, Chen R, Liu Y, Schwartz MA, Amidei C,
Kumthekar P, Benjamin CG, Song K, Dawson C, Rispoli
JM, Fatterpekar G, Golfinos JG, Kondziolka D,
Karajannis M, Pacione D, Zagzag D, McIntyre T,
Snuderl M, Horbinski C. Mutant IDH1 and thrombosis
in Gliomas, Acta Neuropathol. 2016 Dec;132(6):917-
930. Epub 2016 Sep 23. 6
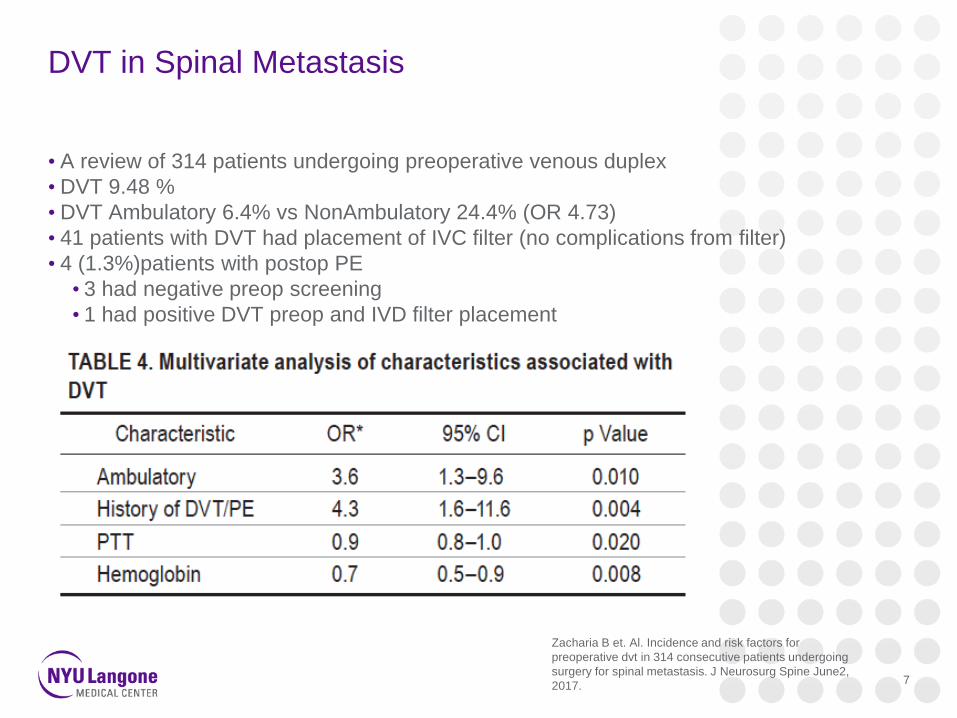
DVT in Spinal Metastasis
• A review of 314 patients undergoing preoperative venous duplex
• DVT 9.48 %
• DVT Ambulatory 6.4% vs NonAmbulatory 24.4% (OR 4.73)
• 41 patients with DVT had placement of IVC filter (no complications from filter)
• 4 (1.3%)patients with postop PE
• 3 had negative preop screening
• 1 had positive DVT preop and IVD filter placement
Zacharia B et. Al. Incidence and risk factors for
preoperative dvt in 314 consecutive patients undergoing
surgery for spinal metastasis. J Neurosurg Spine June2,
2017.7
• 219 patients with prophylactic IVC filter due to risk factors
•History of DVT/PE, Current Malignancy, Hypercoagulable State, Prolonged Immobility,
Staged Procedure >5 levels, Anterior/Posterior, Iliocaval Manipulation, Anesthesia >8h,
Smoker, Estrogen/Progesterone
• 41 (18.7%) patients with DVT
• 8 (3.6%) patients with PE
• 2 (0.9%) developed IVC thrombus
• 1 (0.5%) paradoxical embolism
Presentation Title Goes Here 8
Surveillance for DVT
• 174 neurosurgical patients
• Screening protocol of venous duplex
• Patients non ambulatory for 7 days
•Weekly screening until ambulatory
• 312 venous duplex performed
• 21.8% DVT rate
• 0% PE
• Mechanical prophylaxis in all patients and variable chemoprophylaxis
•DVT rate of 19% vs 41%
• Isolated Calf DVT 37.7%
• 0% developed PE
Dermody M et. La. “The Utility of Screening for Deep
Venous Thrombosis in Asymptomatic, Non-ambulatory
Neurosurgical Patients”. Journal of Vascular Surgery
May 2011.
9
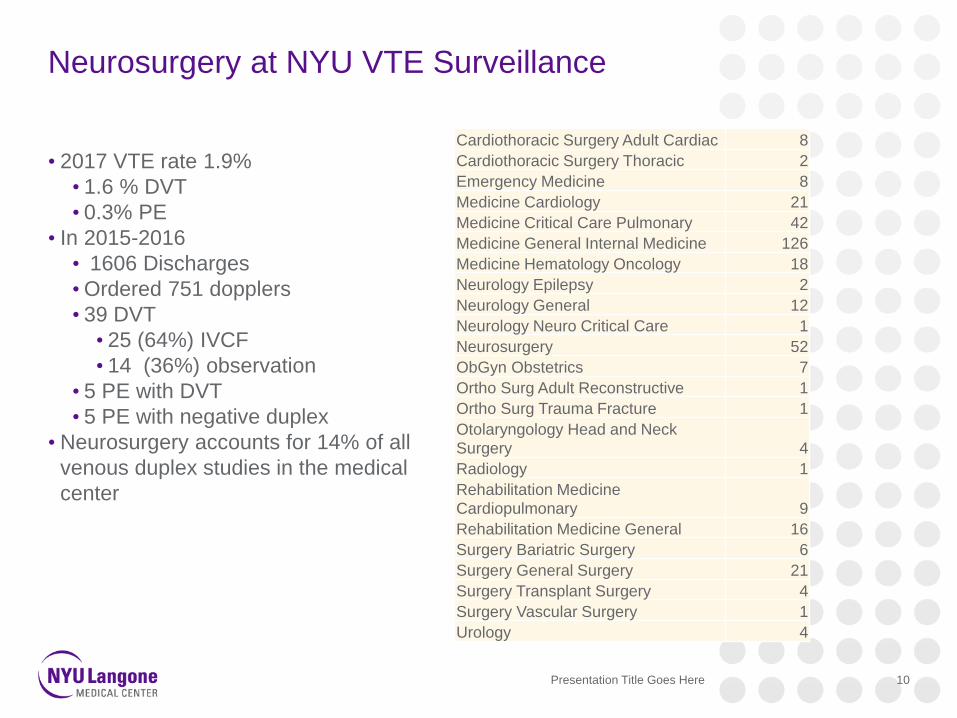
Neurosurgery at NYU VTE Surveillance
Presentation Title Goes Here 10
• 2017 VTE rate 1.9%
• 1.6 % DVT
• 0.3% PE
• In 2015-2016
• 1606 Discharges
•Ordered 751 dopplers
• 39 DVT
• 25 (64%) IVCF
• 14 (36%) observation
• 5 PE with DVT
• 5 PE with negative duplex
• Neurosurgery accounts for 14% of all
venous duplex studies in the medical
center
Cardiothoracic Surgery Adult Cardiac 8
Cardiothoracic Surgery Thoracic 2
Emergency Medicine 8
Medicine Cardiology 21
Medicine Critical Care Pulmonary 42
Medicine General Internal Medicine 126
Medicine Hematology Oncology 18
Neurology Epilepsy 2
Neurology General 12
Neurology Neuro Critical Care 1
Neurosurgery 52
ObGyn Obstetrics 7
Ortho Surg Adult Reconstructive 1
Ortho Surg Trauma Fracture 1
Otolaryngology Head and Neck
Surgery 4
Radiology 1
Rehabilitation Medicine
Cardiopulmonary 9
Rehabilitation Medicine General 16
Surgery Bariatric Surgery 6
Surgery General Surgery 21
Surgery Transplant Surgery 4
Surgery Vascular Surgery 1
Urology 4
VTE Surveillance Protocol
• Prospective surveillance of neurosurgical inpatients with preoperative venous duplex as
part of the standard preoperative workup:
• Any inpatient that is scheduled for a non emergent neurosurgical procedure will have a
venous duplex ordered on admission/transfer.
• Patients with a DVT will undergo placement of retrievable IVC filter prior to
neurosurgical procedure
• Plan for filter removal once anticoagulation is deemed safe from neurosurgical
prospective.
• Post operative Surveillance:
• A venous duplex should be performed in any patient with signs or symptoms of DVT
• A CT PE chest should be performed in any patient with signs or clinical symptoms of
PE.
• Surveillance Duplex once weekly should be performed in patients who are ventilator
dependent (>48 hours), Unable to ambulate independently, active cancer diagnosis,
history of VTE, BMI>40, were on therapeutic anticoagulation preoperatively
Presentation Title Goes Here 11
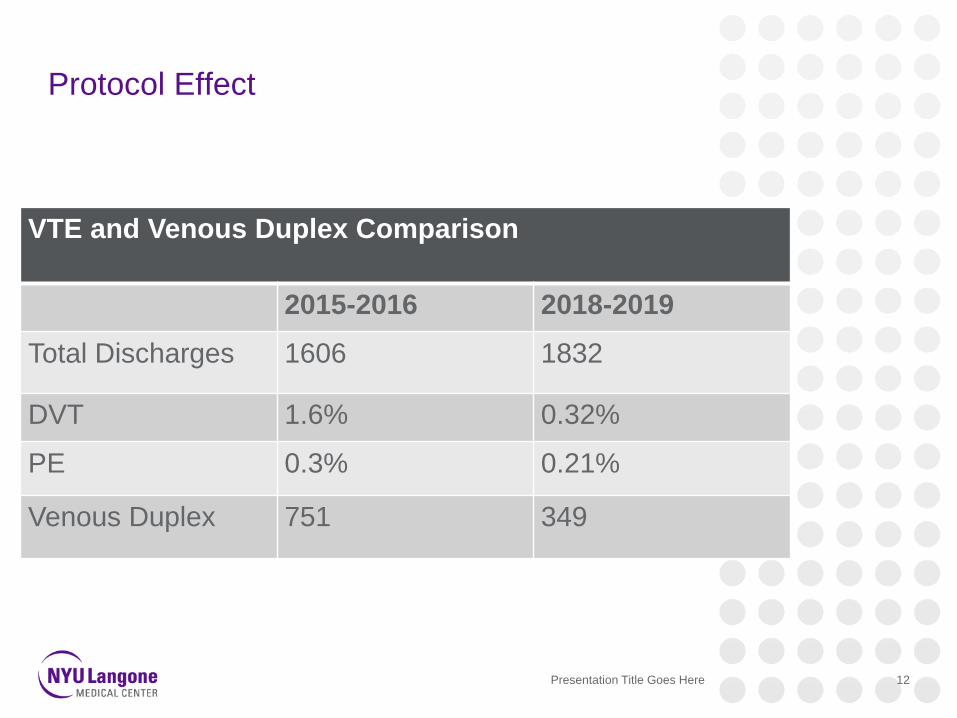
Protocol Effect
Presentation Title Goes Here 12
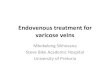
VTE and Venous Duplex Comparison
2015-2016 2018-2019
Total Discharges 1606 1832
DVT 1.6% 0.32%
PE 0.3% 0.21%
Venous Duplex 751 349
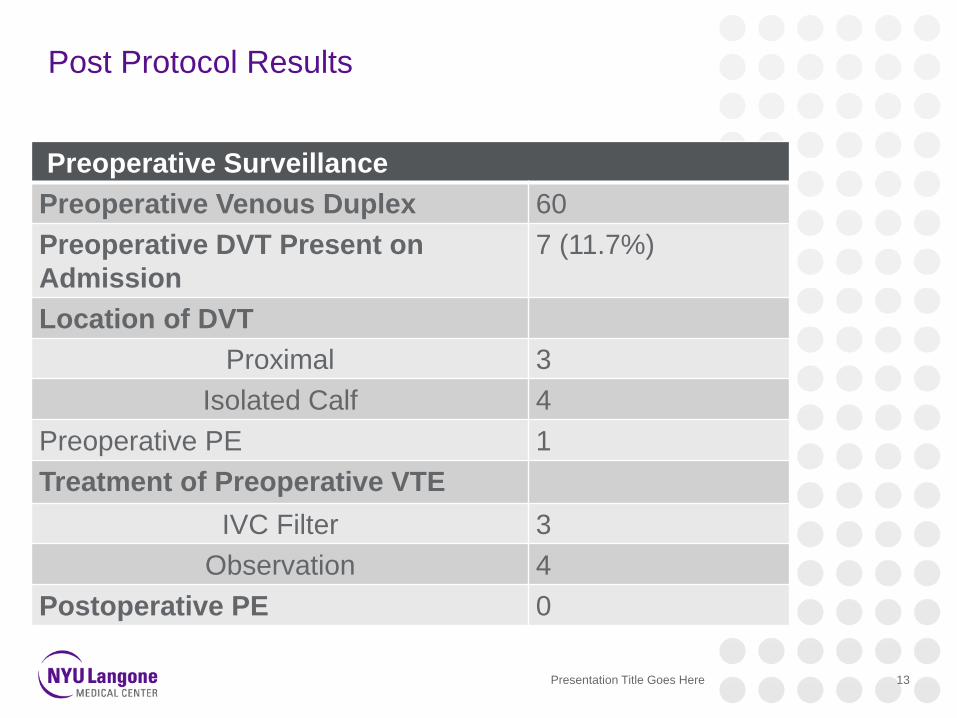
Post Protocol Results
Presentation Title Goes Here 13
Preoperative Surveillance
Preoperative Venous Duplex 60
Preoperative DVT Present on
Admission
7 (11.7%)
Location of DVT
Proximal 3
Isolated Calf 4
Preoperative PE 1
Treatment of Preoperative VTE
IVC Filter 3
Observation 4
Postoperative PE 0
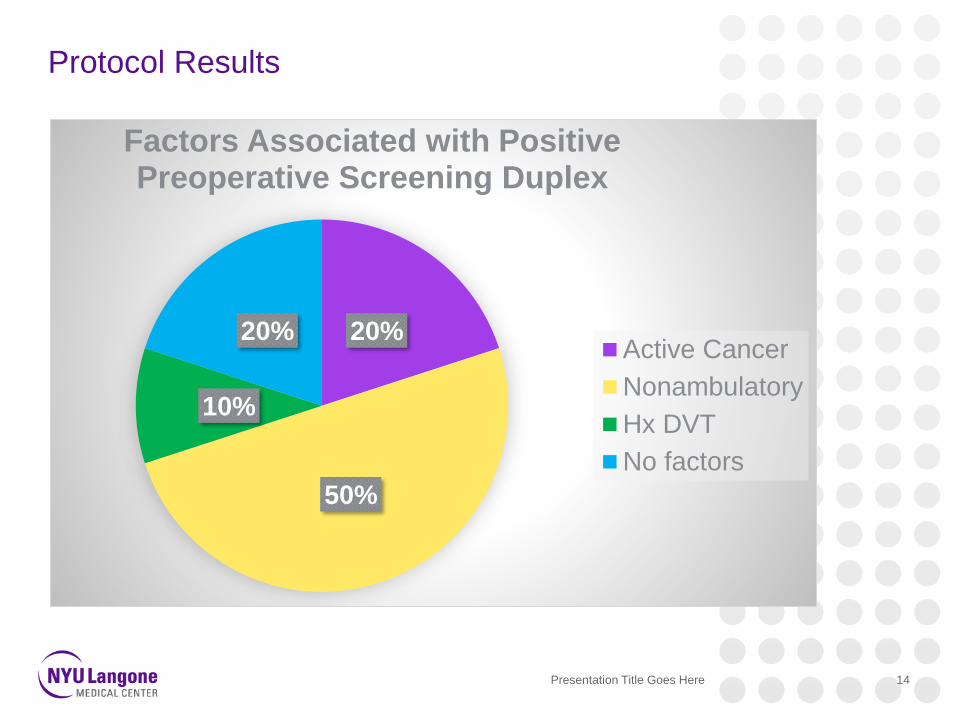
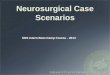
Protocol Results
Presentation Title Goes Here 14
20%
50%
10%
20%
Factors Associated with Positive Preoperative Screening Duplex
Active Cancer
Nonambulatory
Hx DVT
No factors
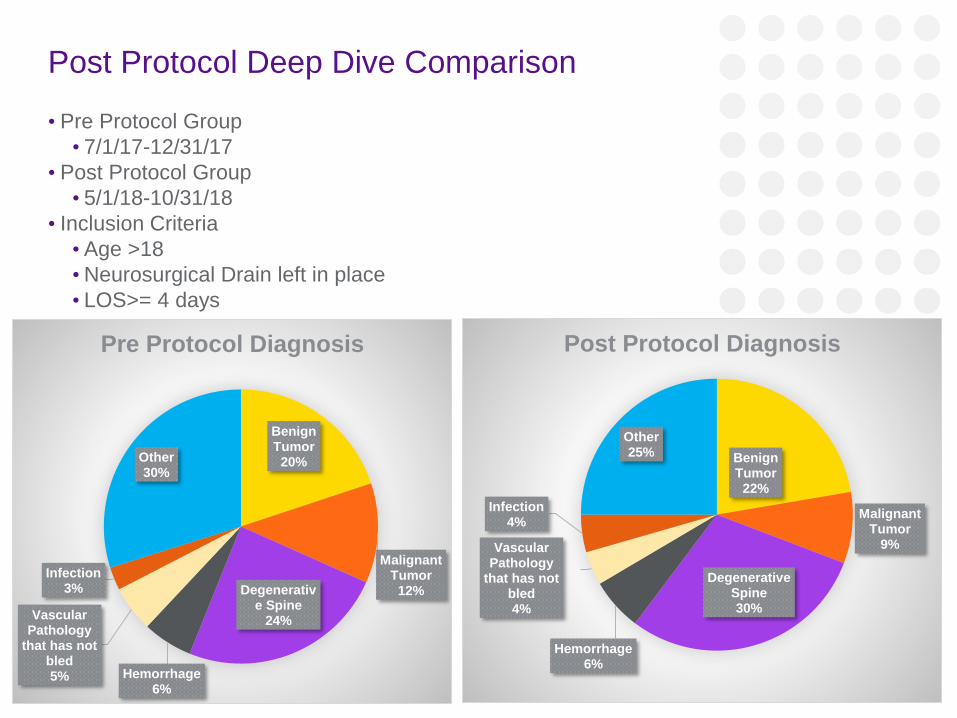
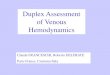
Post Protocol Deep Dive Comparison
• Pre Protocol Group
• 7/1/17-12/31/17
• Post Protocol Group
• 5/1/18-10/31/18
• Inclusion Criteria
• Age >18
•Neurosurgical Drain left in place
• LOS>= 4 days
Presentation Title Goes Here 15
Benign Tumor
20%
Malignant Tumor
12%Degenerative Spine
24%
Hemorrhage6%
Vascular Pathology
that has not bled5%
Infection3%
Other30%
Pre Protocol Diagnosis
Benign Tumor
22%
Malignant Tumor
9%
Degenerative Spine30%
Hemorrhage6%
Vascular Pathology
that has not bled4%
Infection4%
Other25%
Post Protocol Diagnosis
Presentation Title Goes Here 16
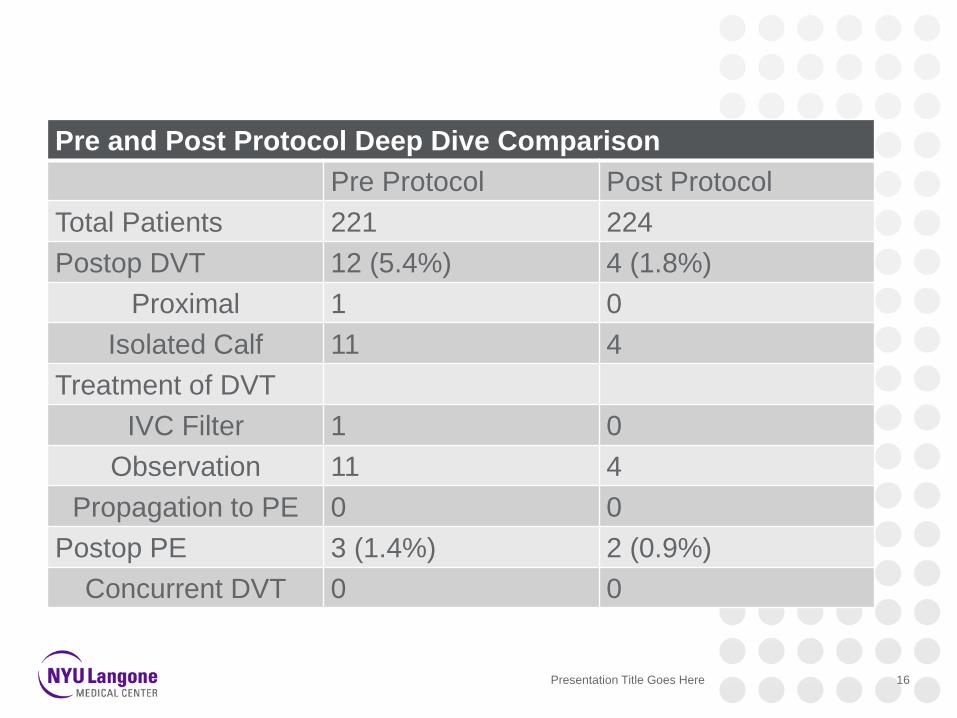
Pre and Post Protocol Deep Dive Comparison
Pre Protocol Post Protocol
Total Patients 221 224
Postop DVT 12 (5.4%) 4 (1.8%)
Proximal 1 0
Isolated Calf 11 4
Treatment of DVT
IVC Filter 1 0
Observation 11 4
Propagation to PE 0 0
Postop PE 3 (1.4%) 2 (0.9%)
Concurrent DVT 0 0
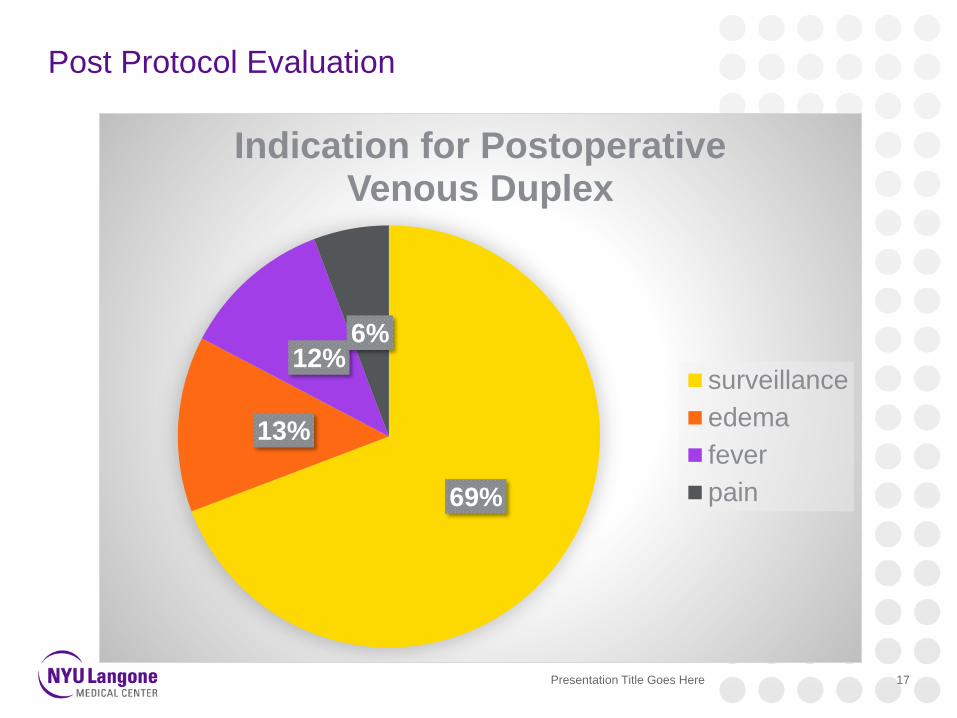
Post Protocol Evaluation
Presentation Title Goes Here 17
69%
13%
12%6%
Indication for Postoperative Venous Duplex
surveillance
edema
fever
pain
Venous Duplex Protocol Change
Presentation Title Goes Here 18
• Preoperative Screening Criteria
• History VTE
• Nonambulatory
• Active cancer
• Symptomatic
• Postoperative
• Venous Duplex only if symptomatic
• CT PE is symptomatic
• No “Surveillance”
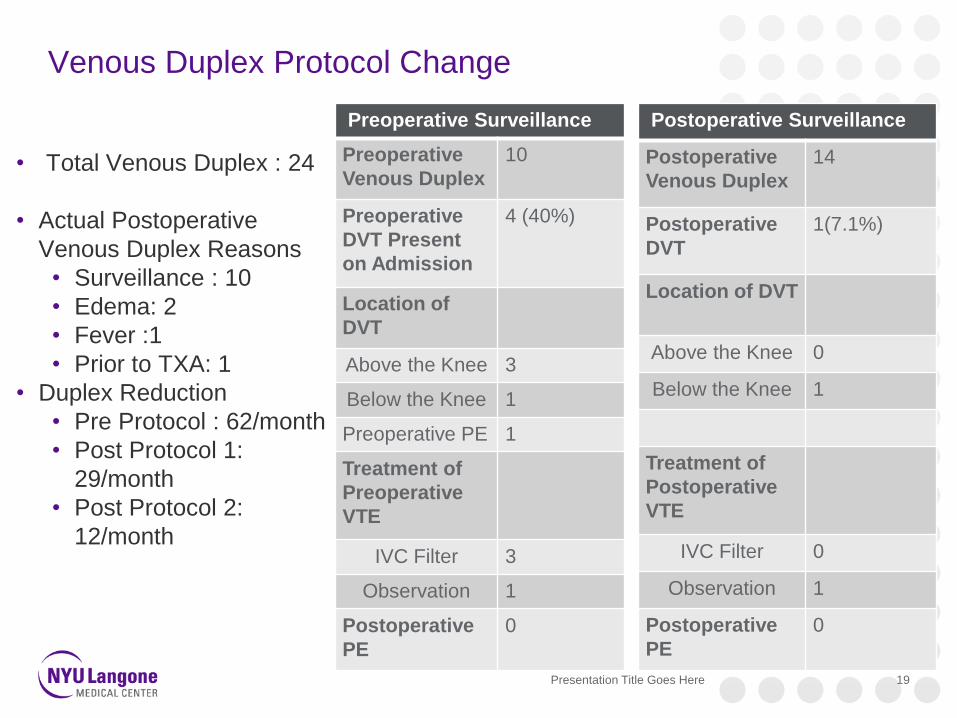
Venous Duplex Protocol Change
Presentation Title Goes Here 19
• Total Venous Duplex : 24
• Actual Postoperative
Venous Duplex Reasons
• Surveillance : 10
• Edema: 2
• Fever :1
• Prior to TXA: 1
• Duplex Reduction
• Pre Protocol : 62/month
• Post Protocol 1:
29/month
• Post Protocol 2:
12/month
Preoperative Surveillance
Preoperative
Venous Duplex
10
Preoperative
DVT Present
on Admission
4 (40%)
Location of
DVT
Above the Knee 3
Below the Knee 1
Preoperative PE 1
Treatment of
Preoperative
VTE
IVC Filter 3
Observation 1
Postoperative
PE
0
Postoperative Surveillance
Postoperative
Venous Duplex
14
Postoperative
DVT
1(7.1%)
Location of DVT
Above the Knee 0
Below the Knee 1
Treatment of
Postoperative
VTE
IVC Filter 0
Observation 1
Postoperative
PE
0
VTE Lessons Learned
1. Everhardt D, Vaccaro J, et. Al. Retrospective
Analysis of Outcomes following IVC Filter Placement
in a Managed Care Population. J Thromb
Thrombolysis. 2017, Aug 44 (2), 179-189.
2. Charalel RA, et. Al . Statewide Inferior Vena Cave
Placement, Complications, and Retrievals:
Epidemiology and Recent Trends. Med Care 2018,
Mar; 56(3) , 260-265
20
• Venous Duplex surveillance does not prevent PE
• Venous duplex is not a substitute for CT PE
study
• Venous Duplex in asymptomatic patient does not
prevent PE
• Venous Duplex surveillance in asymptomatic
patients increases rate of diagnosis of below
knee DVT
• Below knee DVT does not become PE
• Risk of PE from IVC filter > risk from below knee
DVT1,2
Acknowledgements
• John G. Golfinos MD
• Ariane Lewis MD
•Myra Trang NP
• Julia Bevilacqua NP
• Janine Healey NP
•Danielle Golub
• Aaron Rothstein MD
• Peter Rozman MD
•David Kurland MD
Presentation Title Goes Here 21
Thank You