Embed Size (px)
Citation preview
0 | P a g e
Novel Design of Vascular Clamp to Minimize Vessel Injury Senior Design Final Report 4/26/2011 Vanderbilt University School of Engineering Max Hammond, Nadia Hussein, Neha Patel, Francis Simpson, Eric Walk
1 | P a g e
Abstract
The current design of clamps has been fairly unchanged over the past half a century, due
to the lack of acute, macroscopic, visible damage to the vessels. However, studies have
demonstrated significant damage to both the endothelial and smooth muscle layers of vasculature
to which a clamp has been applied, visible on a microscopic level, proportional to the amount of
force applied to the vessel. There are two primary complaints that have prompted the need for a
new vascular clamp design: damage to endothelial layer and length of training time for residents
to use the clamp with their non-dominant hand. The purpose of the Novel Design is to decrease
damage sustained by the endothelium and to reduce training time. Design of the initial prototype
and manufacturing of balloon for occlusion was accomplished using a combination of techniques
including 3D printing, AutoDesk Inventor, and thermal sealing. The results indicate that the
prototype significantly decreased endothelial damage. Percent endothelial relaxation is inversely
proportional to endothelial damage. The percent relaxation for the Debakey clamp was 18.51%
and the percent relaxation for the Hydrogrip clamp was 14.65% compared to the control, which
had a relaxation percentage of 66.55%. The Novel Design had a percent endothelial relaxation of
60.98%. For the comfort category, the Debakey clamp was preferred over the Novel Design with
a p-value of 1.49461E-06. For the ease of use category, the Debakey clamp was preferred over
the Novel Design with a p-value of 3.31852E-05. For the training time category, the Novel
Design was not significantly preferred over the Debakey clamp with a p-value of 0.0814. For the
ingenuity category, the Novel Design was preferred over the Novel Design with a p-value of
2.79256E-05. Our goal that the prototype would reduce the amount of damage to vessels
compared to the current designs was supported by our results. Our goal for the prototype to be
easier to use and more comfortable was not met; however, the goal for decrease in training time
has potential since there was no significant difference between the prototype and the present
clamp and the ingenuity presented by the prototype generates great potential. With some
improvements to the first prototype, Novel Design has the possibility to meet all the goals
presented.
2 | P a g e
Introduction
Full occlusion of blood flow through one or more vessels is essential to the success of a
wide variety of surgical procedures, particularly vascular procedures in which the vessels
themselves are the surgical target. This is mainly necessary to prevent hemorrhage, which will
not only potentially lead to patient death, but also interfere with the surgeon‟s view of the
surgical field during a procedure. The primary method used to block these vessels involves the
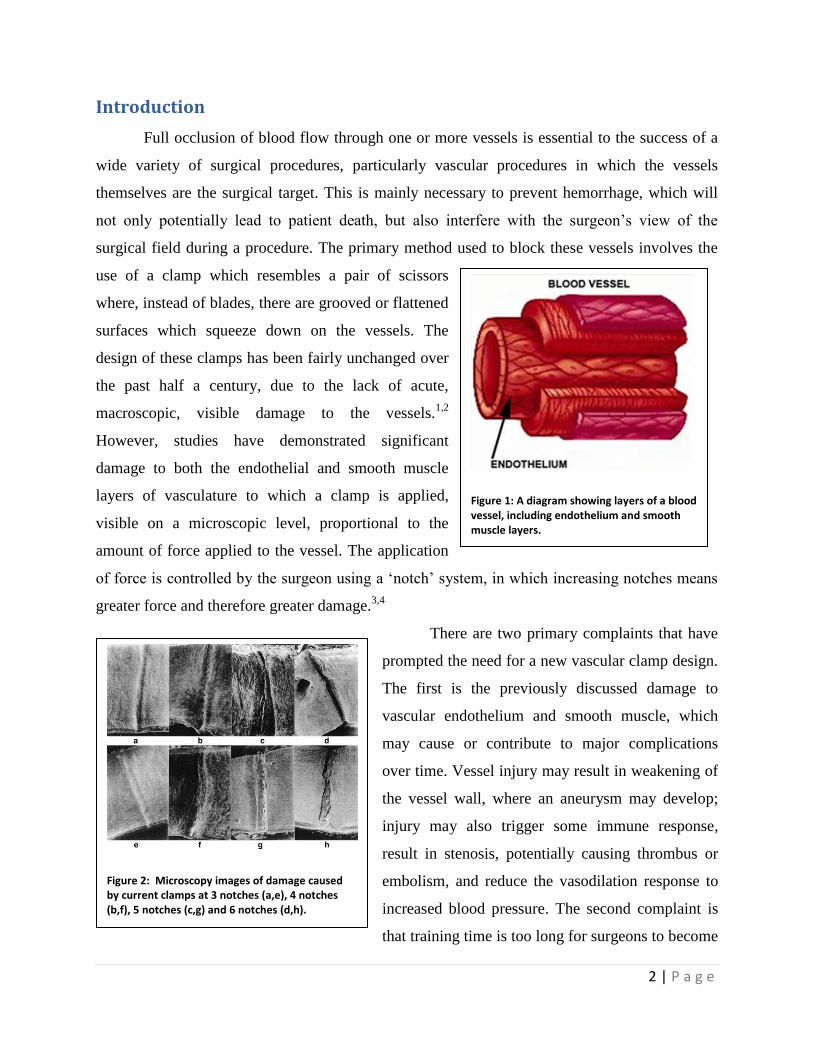
use of a clamp which resembles a pair of scissors
where, instead of blades, there are grooved or flattened
surfaces which squeeze down on the vessels. The
design of these clamps has been fairly unchanged over
the past half a century, due to the lack of acute,
macroscopic, visible damage to the vessels.1,2
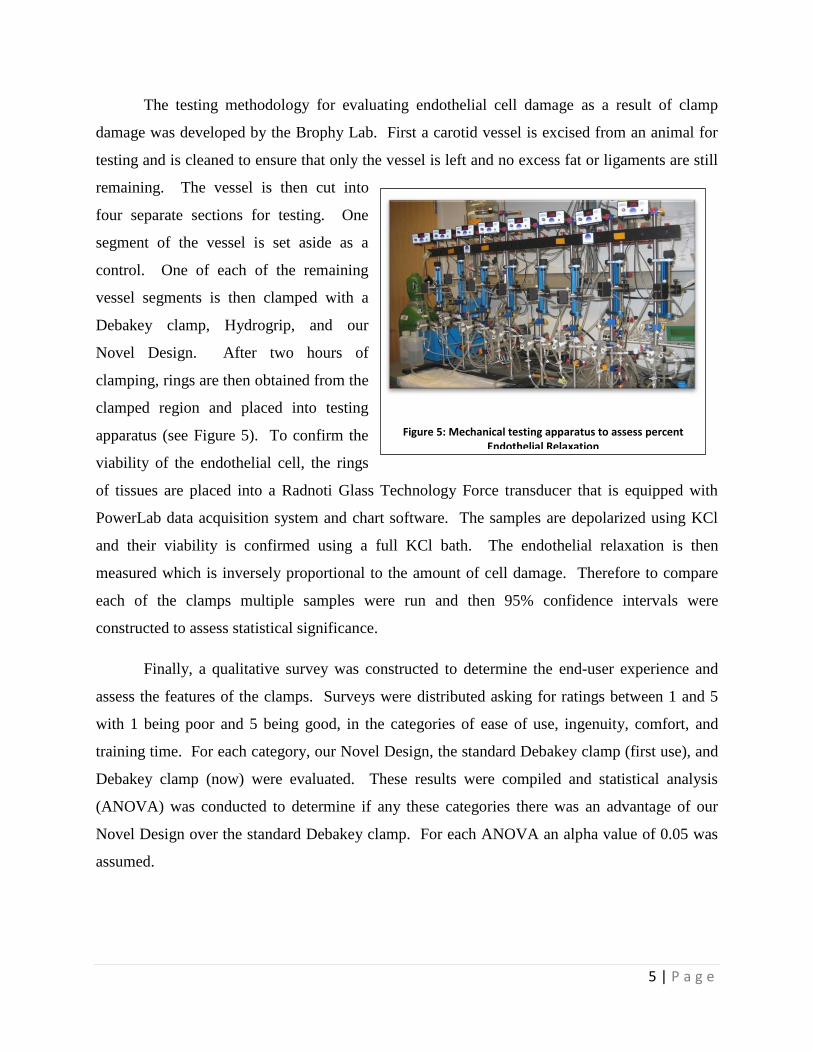
However, studies have demonstrated significant
damage to both the endothelial and smooth muscle
layers of vasculature to which a clamp is applied,
visible on a microscopic level, proportional to the
amount of force applied to the vessel. The application
of force is controlled by the surgeon using a „notch‟ system, in which increasing notches means
greater force and therefore greater damage.3,4
There are two primary complaints that have
prompted the need for a new vascular clamp design.
The first is the previously discussed damage to
vascular endothelium and smooth muscle, which
may cause or contribute to major complications
over time. Vessel injury may result in weakening of
the vessel wall, where an aneurysm may develop;
injury may also trigger some immune response,
result in stenosis, potentially causing thrombus or
embolism, and reduce the vasodilation response to
increased blood pressure. The second complaint is
that training time is too long for surgeons to become
Figure 1: A diagram showing layers of a blood vessel, including endothelium and smooth muscle layers.
Figure 2: Microscopy images of damage caused by current clamps at 3 notches (a,e), 4 notches (b,f), 5 notches (c,g) and 6 notches (d,h).

3 | P a g e
comfortable with non-dominant hand control (as the dominant hand is usually otherwise
occupied with other aspects of the procedure). A successful new clamp design would reduce
training time as well as reduce damage to vessels.
When approaching the design of the new clamp, many factors were considered when
evaluating potential success. In addition to the primary goals of reducing training time by 50%
and vessel damage by a minimum of 20%, it was necessary to meet several criteria for the
viability of the design. First, the design must be capable of fully occluding flow through a vessel
for the entire duration of a surgery, and over the full range of blood pressures that are
physiologically possible. The clamp must also be either sterilizable or disposable, to avoid any
opportunity for contamination and infection in the operating room (OR). The size of the clamp is
also an important factor, as space in the surgical field is limited and a device larger than current
designs would likely be received unfavorably. In order to ensure sustainable production of the
device, the final design should be able to be sold for under $2000 per clamp, and must be
profitable to allow for adequate manufacturing.

4 | P a g e
Methodology
Design of the initial prototype and manufacturing of balloon for occlusion was
accomplished using a combination of techniques including 3D printing, AutoDesk Inventor, and
thermal sealing. The main body of the
prototype was designed using AutoDesk
Inventor 2011 and was fabricated by
FineLine Prototyping using 3D printing
with WaterShed XC 11122 Normal-
Resolution Stereolithography build in
0.004" layers and post-processed for
biocompatibility per DSM' process for
passing USP Class VI testing. The
balloon for occlusion was fashioned using 1/8” inner diameter tubing and IV bag plastic which
was thermally sealed to create a balloon to be placed around the vessel. A one-way valve
assembly with quick release was fabricated using spare IV tubing parts and connected between
the device and the syringe used for
inflation.
To test the ability of the new clamp
design to hold pressure, an ex vivo test was
performed using a synthetic carotid made
from graft material. The setup for the y-
tubing is shown in Figure 3. The system
was completely filled with water and the
vessel was them placed inside of the clamp.
The balloon was inflated using 10 mL of air
and the vessel was pressurized to 300 mmHg equivalent. The vessel ending was then checked to
make sure that no water was coming out after the clamped region and was used to evaluate the
pressure at which leakage (if any) would occur.
Figure 4: Pressuring testing device to determine how much pressure the clamp will be able to take and still occlude the
vessel.
Figure 3: The prototype. Left most end is the balloon inside the main body of the device. Center is the valve assembly (from left: quick release, one way valve, Y-joint between
syringe and one way valve).
5 | P a g e
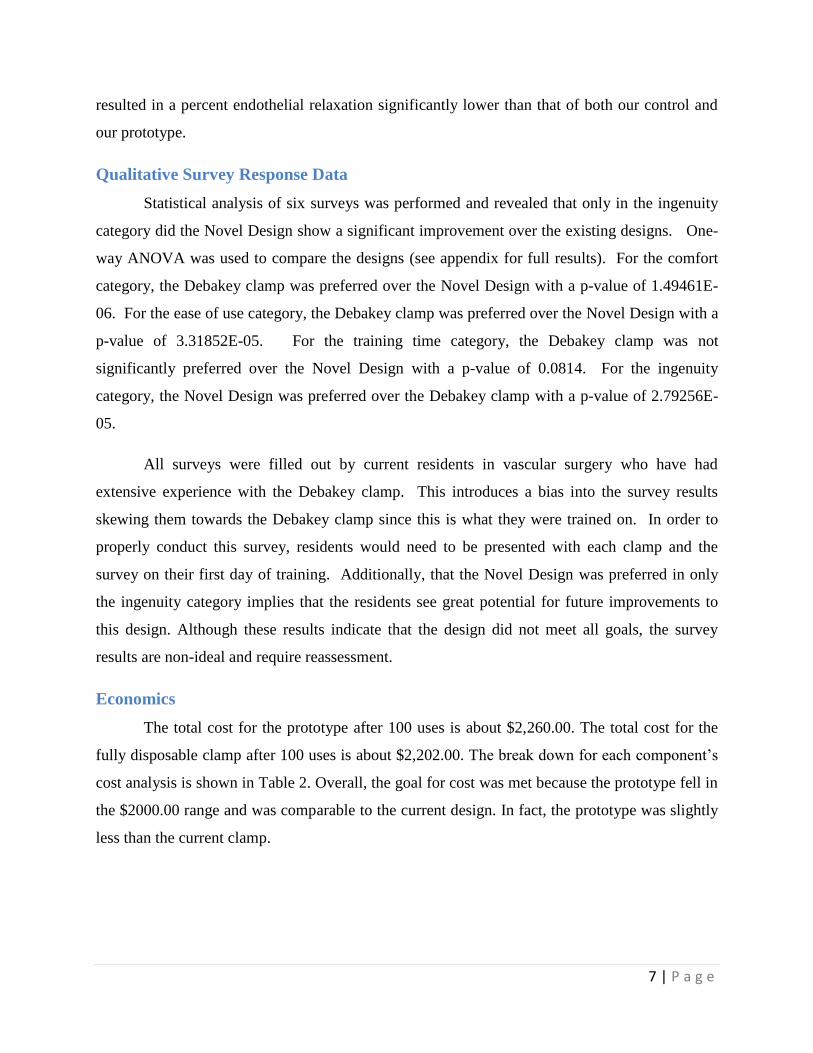
The testing methodology for evaluating endothelial cell damage as a result of clamp
damage was developed by the Brophy Lab. First a carotid vessel is excised from an animal for
testing and is cleaned to ensure that only the vessel is left and no excess fat or ligaments are still
remaining. The vessel is then cut into
four separate sections for testing. One
segment of the vessel is set aside as a
control. One of each of the remaining
vessel segments is then clamped with a
Debakey clamp, Hydrogrip, and our
Novel Design. After two hours of
clamping, rings are then obtained from the
clamped region and placed into testing
apparatus (see Figure 5). To confirm the
viability of the endothelial cell, the rings
of tissues are placed into a Radnoti Glass Technology Force transducer that is equipped with
PowerLab data acquisition system and chart software. The samples are depolarized using KCl
and their viability is confirmed using a full KCl bath. The endothelial relaxation is then
measured which is inversely proportional to the amount of cell damage. Therefore to compare
each of the clamps multiple samples were run and then 95% confidence intervals were
constructed to assess statistical significance.
Finally, a qualitative survey was constructed to determine the end-user experience and
assess the features of the clamps. Surveys were distributed asking for ratings between 1 and 5
with 1 being poor and 5 being good, in the categories of ease of use, ingenuity, comfort, and
training time. For each category, our Novel Design, the standard Debakey clamp (first use), and
Debakey clamp (now) were evaluated. These results were compiled and statistical analysis
(ANOVA) was conducted to determine if any these categories there was an advantage of our
Novel Design over the standard Debakey clamp. For each ANOVA an alpha value of 0.05 was
assumed.
Figure 5: Mechanical testing apparatus to assess percent Endothelial Relaxation

6 | P a g e
Results
Percent Endothelial Relaxation
Endothelial relaxation is an essential
component of the control of
vasodilation/constriction. The current clamps,
Debakey and Hydrogrip clamps cause a disruption of
the endothelial physiology of the vessels which
reduce the percent relaxation in response to physical
and chemical triggers. This endothelial damage has
the potential to create complications resulting from a
localized increase in blood pressure at the site of
former clamping due to limited dilation response of
the vessel. By performing a percent endothelial
relaxation test with the current clamps, our prototype, and an unclamped control vessel, we were
able to compare the endothelial damage caused by each clamping procedure. As that the
endothelium is the most sensitive aspect of the vessel it was chosen for damage assessment. Two
hours of clamping was chosen as a protocol because that represents the upper limit of the
majority of vascular surgeries.
Figure 6 verifies that both the Debakey and Hydrogrip clamps cause significant decreases
in the percent endothelial
relaxation. The percent
relaxation for the Debakey
clamp was 18.51% and the
percent relaxation for the
Hydrogrip clamp was
14.65% compared to the
control, which had a relaxation percentage of 66.55%. Our prototype had a percent endothelial
relaxation of 60.98%. Table 1 shows the 95% confidence intervals for each design. The
confidence intervals of the prototype and the control overlapped indicating there was not a
significant difference between these values in our test. The Debakey and Hydrogrip designs
Figure 6: Percent Endothelial Relaxation for current designs after two hours of clamping.
Table 1: 95% Confidence intervals (CI) for each design.
Control New Clamp Debakey Hydrogrip
Upper limit
of 95% CI 52.73 63.64 21.43 18.18
Lower limit
of 95% CI 80.37 58.33 15.60 11.11
Mean 66.55 60.98 18.51 14.65
7 | P a g e
resulted in a percent endothelial relaxation significantly lower than that of both our control and
our prototype.
Qualitative Survey Response Data
Statistical analysis of six surveys was performed and revealed that only in the ingenuity
category did the Novel Design show a significant improvement over the existing designs. One-
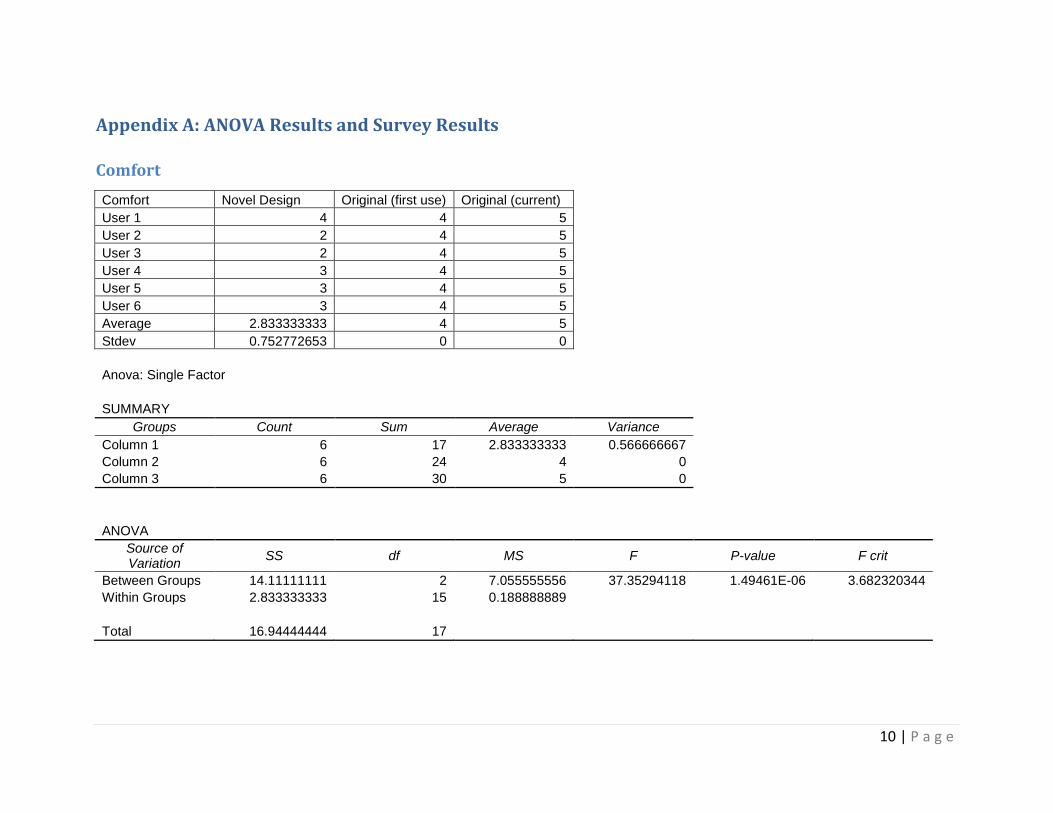
way ANOVA was used to compare the designs (see appendix for full results). For the comfort
category, the Debakey clamp was preferred over the Novel Design with a p-value of 1.49461E-
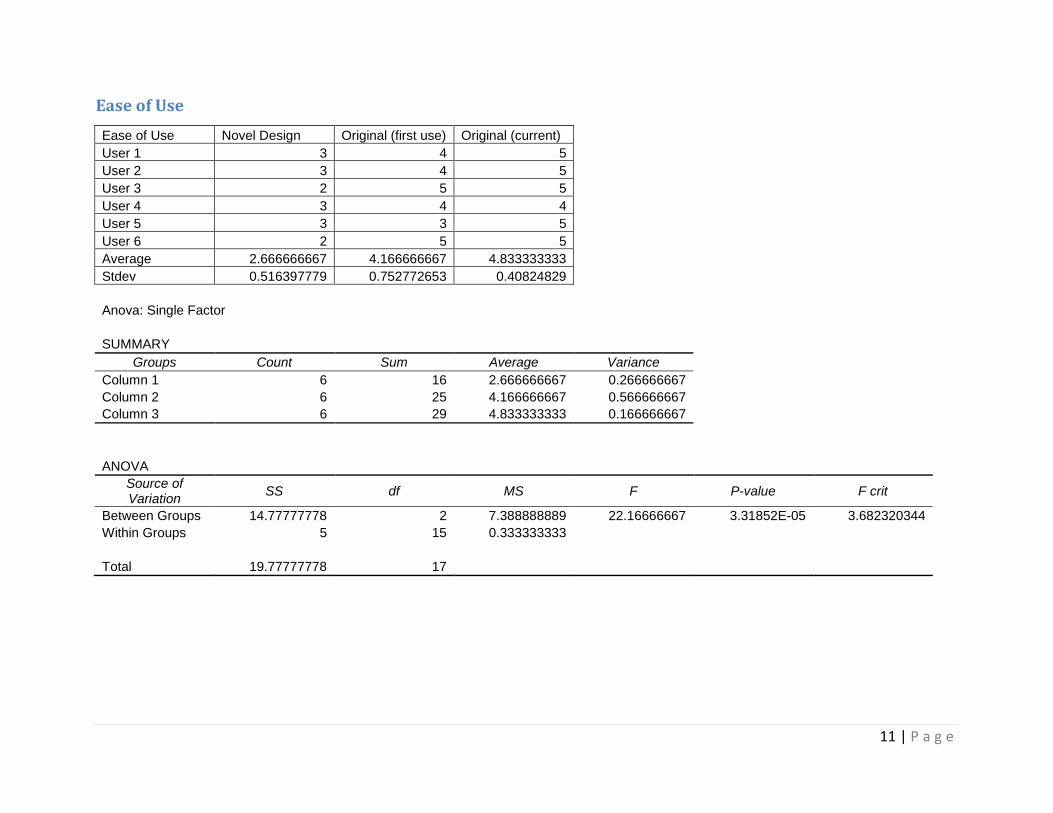
06. For the ease of use category, the Debakey clamp was preferred over the Novel Design with a
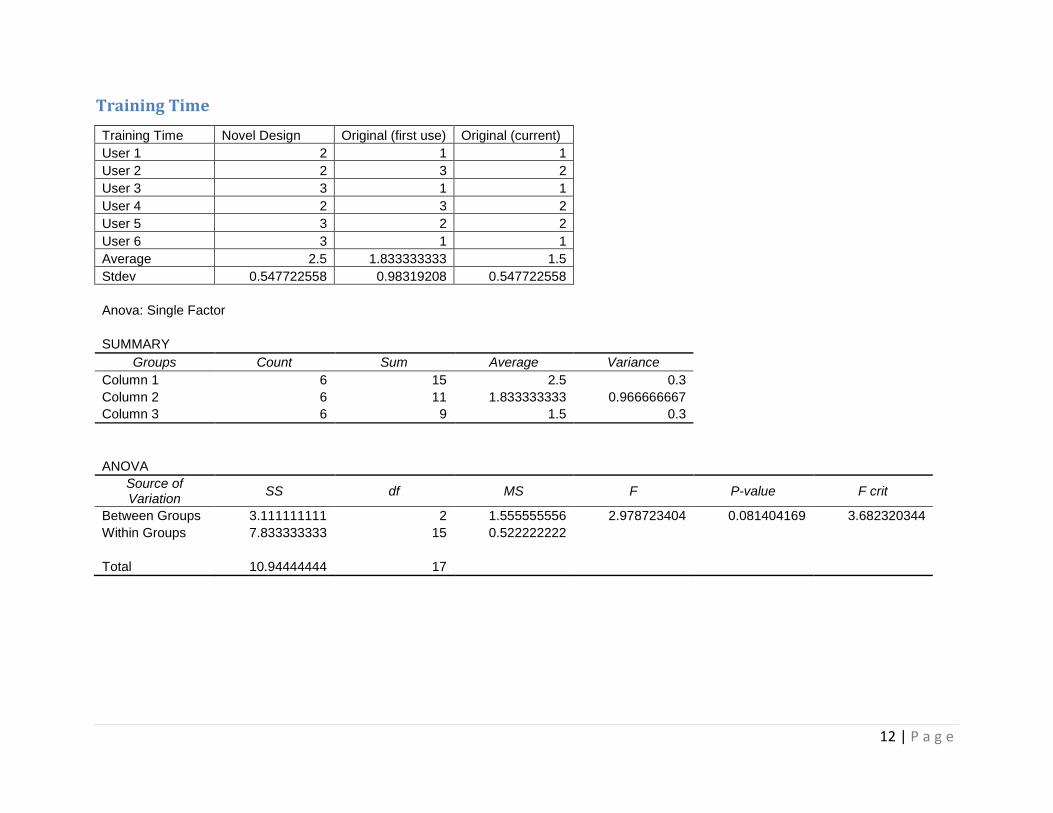
p-value of 3.31852E-05. For the training time category, the Debakey clamp was not
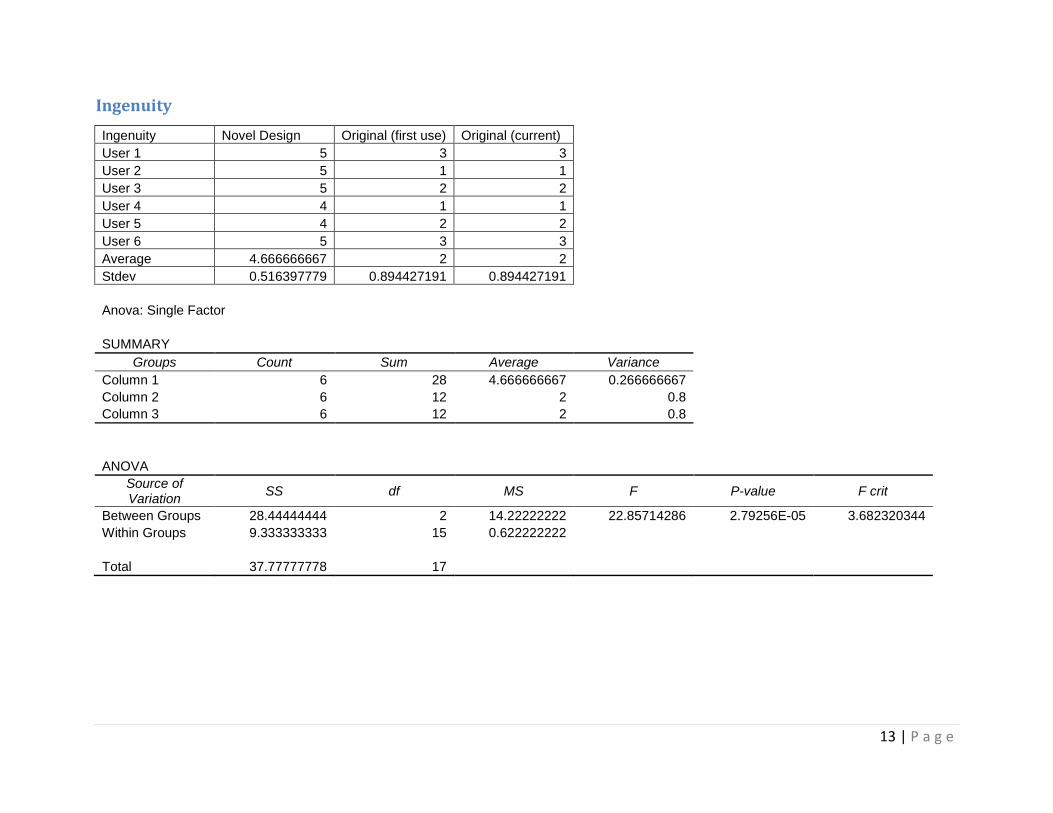
significantly preferred over the Novel Design with a p-value of 0.0814. For the ingenuity
category, the Novel Design was preferred over the Debakey clamp with a p-value of 2.79256E-
05.
All surveys were filled out by current residents in vascular surgery who have had
extensive experience with the Debakey clamp. This introduces a bias into the survey results
skewing them towards the Debakey clamp since this is what they were trained on. In order to
properly conduct this survey, residents would need to be presented with each clamp and the
survey on their first day of training. Additionally, that the Novel Design was preferred in only
the ingenuity category implies that the residents see great potential for future improvements to
this design. Although these results indicate that the design did not meet all goals, the survey
results are non-ideal and require reassessment.
Economics
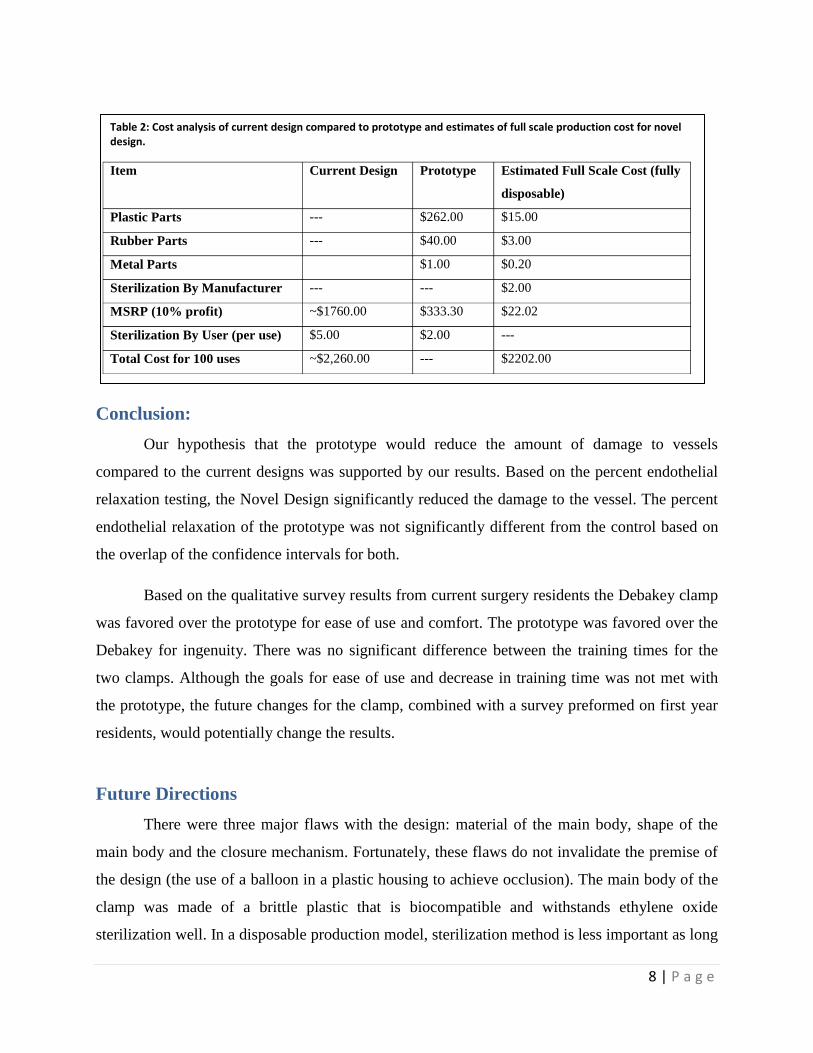
The total cost for the prototype after 100 uses is about $2,260.00. The total cost for the
fully disposable clamp after 100 uses is about $2,202.00. The break down for each component‟s
cost analysis is shown in Table 2. Overall, the goal for cost was met because the prototype fell in
the $2000.00 range and was comparable to the current design. In fact, the prototype was slightly
less than the current clamp.
8 | P a g e
Conclusion:
Our hypothesis that the prototype would reduce the amount of damage to vessels
compared to the current designs was supported by our results. Based on the percent endothelial
relaxation testing, the Novel Design significantly reduced the damage to the vessel. The percent
endothelial relaxation of the prototype was not significantly different from the control based on
the overlap of the confidence intervals for both.
Based on the qualitative survey results from current surgery residents the Debakey clamp
was favored over the prototype for ease of use and comfort. The prototype was favored over the
Debakey for ingenuity. There was no significant difference between the training times for the
two clamps. Although the goals for ease of use and decrease in training time was not met with
the prototype, the future changes for the clamp, combined with a survey preformed on first year
residents, would potentially change the results.
Future Directions
There were three major flaws with the design: material of the main body, shape of the
main body and the closure mechanism. Fortunately, these flaws do not invalidate the premise of
the design (the use of a balloon in a plastic housing to achieve occlusion). The main body of the
clamp was made of a brittle plastic that is biocompatible and withstands ethylene oxide
sterilization well. In a disposable production model, sterilization method is less important as long
Table 2: Cost analysis of current design compared to prototype and estimates of full scale production cost for novel design.
Item Current Design Prototype Estimated Full Scale Cost (fully
disposable)
Plastic Parts --- $262.00 $15.00
Rubber Parts --- $40.00 $3.00
Metal Parts $1.00 $0.20
Sterilization By Manufacturer --- --- $2.00
MSRP (10% profit) ~$1760.00 $333.30 $22.02
Sterilization By User (per use) $5.00 $2.00 ---
Total Cost for 100 uses ~$2,260.00 --- $2202.00

9 | P a g e
as it is compatible with one of them. Ideally a less brittle plastic would be used so as to avoid
breakage in manufacturing. The shape of the handle could also be improved to be slightly thicker
so as to avoid breaks during manufacture. Additionally, the diameter of the opening for the
vessel was designed to the maximal size of the carotid in a human; however the thickness of the
balloon was underestimated. Thus a larger diameter is required. Finally the closure mechanism
needs to be adjusted in two ways. First, the hinge mechanism needs to be changed such that the
parts do not separate when the balloon is inflated. Second, the lever arm needs to be compounded
so as to provide greater mechanical advantage (i.e. a small movement at the distal end creates a
big movement at the proximal end). The first problem is solved simply, creating a series of
interlocking fingers along the joint and running the hinge pin through them to create a “piano”
style hinge. The second problem is more complex requiring the careful design of a series of pivot
points along the arm to act as a mechanical amplifier (much as the bones in the inner ear). These
adjustments should help to alleviate the concerns expressed in the surveys by the residents;
consideration should be given to methods for automatic inflation upon closure to further address
these concerns. With these adjustments to the design it should be more adept in in-vivo
scenarios; the current prototype was sufficient, however, for proving that it is possible and
practical to occlude a vessel with an inflatable cuff.
References:
1. Darçin OT, Cengiz M, Özardali I, et al. Pressure-controlled vascular clamp: a novel device for
atraumatic vessel occlusion. Ann Vasc Surg 2004;18:254-256.
2. Gersak B, Trobec R, Krisch I, et al. Loss of endotheliummediated vascular relaxation as a
response to various clamping pressures. Eur J Cardiothorac Surg 1996;10: 684-689.
3. Margovsky AI, Lord RS, Meek AC, et al. Artery wall damage and platelet uptake from so-
called atraumatic arterial clamps: an experimental study. Cardiovasc Surg 1997;5:42-47.
4. Margovsky AI, Chambers AJ, Lord RS. The effect of increasing clamping forces on
endothelial and arterial wall damage: an experimental study in the sheep. Cardiovasc
Surg 1999;7: 457-463.
5. Zhang Y, Luo Y, Kodaira S, et al. Application of Shape Memory Alloy Pressure-Controlled
Vascular Clamp for Atraumatic Vessel Occlusion. Ann Vasc Surg 2009; 23: 813-820
10 | P a g e
Appendix A: ANOVA Results and Survey Results
Comfort
Comfort Novel Design Original (first use) Original (current)
User 1 4 4 5
User 2 2 4 5
User 3 2 4 5
User 4 3 4 5
User 5 3 4 5
User 6 3 4 5
Average 2.833333333 4 5
Stdev 0.752772653 0 0
Anova: Single Factor
SUMMARY
Groups Count Sum Average Variance
Column 1 6 17 2.833333333 0.566666667
Column 2 6 24 4 0
Column 3 6 30 5 0
ANOVA
Source of Variation
SS df MS F P-value F crit
Between Groups 14.11111111 2 7.055555556 37.35294118 1.49461E-06 3.682320344
Within Groups 2.833333333 15 0.188888889
Total 16.94444444 17
11 | P a g e
Ease of Use
Ease of Use Novel Design Original (first use) Original (current)
User 1 3 4 5
User 2 3 4 5
User 3 2 5 5
User 4 3 4 4
User 5 3 3 5
User 6 2 5 5
Average 2.666666667 4.166666667 4.833333333
Stdev 0.516397779 0.752772653 0.40824829
Anova: Single Factor
SUMMARY
Groups Count Sum Average Variance
Column 1 6 16 2.666666667 0.266666667
Column 2 6 25 4.166666667 0.566666667
Column 3 6 29 4.833333333 0.166666667
ANOVA
Source of Variation
SS df MS F P-value F crit
Between Groups 14.77777778 2 7.388888889 22.16666667 3.31852E-05 3.682320344
Within Groups 5 15 0.333333333
Total 19.77777778 17
12 | P a g e
Training Time
Training Time Novel Design Original (first use) Original (current)
User 1 2 1 1
User 2 2 3 2
User 3 3 1 1
User 4 2 3 2
User 5 3 2 2
User 6 3 1 1
Average 2.5 1.833333333 1.5
Stdev 0.547722558 0.98319208 0.547722558
Anova: Single Factor
SUMMARY
Groups Count Sum Average Variance
Column 1 6 15 2.5 0.3
Column 2 6 11 1.833333333 0.966666667
Column 3 6 9 1.5 0.3
ANOVA
Source of Variation
SS df MS F P-value F crit
Between Groups 3.111111111 2 1.555555556 2.978723404 0.081404169 3.682320344
Within Groups 7.833333333 15 0.522222222
Total 10.94444444 17
13 | P a g e
Ingenuity
Ingenuity Novel Design Original (first use) Original (current)
User 1 5 3 3
User 2 5 1 1
User 3 5 2 2
User 4 4 1 1
User 5 4 2 2
User 6 5 3 3
Average 4.666666667 2 2
Stdev 0.516397779 0.894427191 0.894427191
Anova: Single Factor
SUMMARY
Groups Count Sum Average Variance
Column 1 6 28 4.666666667 0.266666667
Column 2 6 12 2 0.8
Column 3 6 12 2 0.8
ANOVA
Source of Variation
SS df MS F P-value F crit
Between Groups 28.44444444 2 14.22222222 22.85714286 2.79256E-05 3.682320344
Within Groups 9.333333333 15 0.622222222
Total 37.77777778 17