Embed Size (px)
Citation preview

NON-MALIGNANT AFFECTIONS OF THE UPPER STOMACHLecture delivered at the Royal College of Surgeons of England
on26th September, 1951
byNorman C. Tanner, F.R.C.S.
Surgeon, St. James' Hospital, London, S.W.12.
THERE ARE NO very strong anatomical or physiological reasons for makinga distinction between lesions of the upper and lower stomach. The treat-ment of diseases of the upper stomach does not vary in its basic principlesfrom that of the middle and lower stomach. Nevertheless, at this stageof the history of the surgery of the stomach there are some reasons whyit is profitable to consider the upper stomach separately. The first reasonis that lesions of the upper stomach have not been very accessible to easysurgical manipulation until the last ten years, and so it is now the time toconsider whether to continue with our previous rather conservative mea-sures or to change to more radical measures carried out through a thoracicapproach. The second reason is that improved radiology, improvedendoscopy, the introduction of the flexible oesophagoscope and gastro-scope, have given us more knowledge of some pathological conditionswhich affect the cardiac end of the stomach.
The Exposure of the Upper StomachLet me begin by saying that simply because by means of a trans-
pleural approach we can now extirpate the upper stomach with com-parative ease and with a good prospect of survival, it does not necessarilyfollow that every patient with a lesion near the cardia requires such anapproach. Despite the safety and ease with which the pleural cavitycan be opened, I still consider a transpleural, or abdomino-thoracicapproach to the cardiac end of the stomach, both in the young and aged,to be a more formidable procedure than a laparotomy.The risks of the transpleural approach to the upper stomach lie more in
the post-operative complications than in the operation itself. Therefore,whenever the transpleural exposure is used every effort must be made toprevent such complications, and to deal with them rapidly should theyoccur. If it is considered that an operation on the upper stomach can beequally well carried out by the abdominal or by the transthoracic route,then the abdominal route should be chosen even if it means that the surgeonis working with somewhat less ease. If, however, an operation can becarried out more efficiently by a transthoracic route, for example, a growthcan be removed more radically, or an oesophageal anastomosis mademore secure, then this consideration greatly outweighs all others and thethoracic approach should be used. For example, an abdominal surgeonshould not find it necessary to open the thorax in order to perform a
45
4-2

NORMAN C. TANNER
Heller operation or expose a gastric diverticulum in a thin patient. Onthe other hand every gastric malignancy involving the upper half of thestomach, and every operation requiring an oesophageal anastomosis isbest carried out through some form of transpleural incision.
Upper Partial GastrectomySome clarification in our terminology for operations for resection of
the upper stomach is needed. Many terms are used to describe removalof the upper stomach, with transection below through the stomach, andtransection above through the oesophagus, for example, cardiectomy,oesophago-gastrectomy, &c. I would like to recommend that a simplerterm would be Upper Partial Gastrectomy, and, to differentiate it fromthe resection of the stomach for ulcer in which the upper section is throughstomach and the lower through duodenum, the latter should be calledLower Partial Gastrectomy (even though it may be an extensiveresection).
I believe, too, that the word " radical'" should be used more exactly.By radical resection some surgeons mean extensive. I think it should beused much as we use it in describing mastectomy. By mastectomy wemean total mastectomy and the addition of the word radical implies aresection as for carcinoma, with resection of adjacent muscles, lymphglands and lymphatic fields. Therefore, in qualifying any form of gas-trectomy by the word " radical," we should infer not merely that gastrictissue was removed well wide of the growth, but also that the lymphaticfields and glands, and probably the greater and lesser omenta were alsoresected.
Peptic Ulceration of the Upper StomachGastric ulceration at the cardiac end of the stomach may be due to
ulceration originating in the upper stomach, or it may follow invasion ofthe upper stomachlby a mid or lower gastric ulcer which gradually ulceratesmore and more gastric tissue until the upper edge may be within a centi-metre or two of the cardiac orifice, even though the lower edge of theulcer is in the antrum, or even at the pylorus. In many cases the granulationtissue in the ulcer base may be actively contracting almost as fast as theedge ulcerates, so that such an ulcer may not necessarily be of widediameter. The result is that the pylorus and cardia become drawn togetheruntil there are only a few centimetres between them.
Ulcers arising primarily in the upper stomach may appear at any levelfrom the cardia downwards, and more commonly affect the posteriorsurface near the lesser curvature. A very common site is on the posteriorpart of the lesser curvature about a quarter of the way from the cardiato the pylorus, a site which I find particularly common in women.Occasionally there may be hourglass scarring with-two or more ulcers onthe cicatricial ring, and very rarely an ulcer may be found nearer thegreater than the lesser curvature. As such ulcers are near the point where
46

NON-MALIGNANT AFFECTIONS OF THE UPPER STOMACH
the left gastric artery with its sometimes bulky adjacent lymph glandsapproaches the stomach and are near the upper part of the lesser peri-toneal sac, they may be missed by anything but the most painstakingexamination, and this examination should be both digital and, afterdivision of the hepato-gastric ligament and rotation of the stomach,visual.
There are many special problems concerning the surgical treatment ofhigh gastric ulcer which are of great practical importance. Their solutionmust to some extent vary with the surgeon's experience. Generallyspeaking we must regard it as desirable to perform a partial gastrectomy,if possible including the ulcer or ulcer scar in the excision, because a nowvery long experience has persuaded surgeons everywhere that this is acertain method of cure of chronic gastric ulcer. Some surgeons declare thathigh gastric ulcer requires a total or quasi-total gastrectomy. With thisI would not agree. I believe that total gastric resection is never justifiedfor an obviously innocent chronic gastric ulcer. I think it unnecessaryand undesirable even to perform an excessively high resection for gastriculceration. In a personal series of over 700 resections for gastric ulcerI have never seen recurrent ulceration occur, so that stomal ulcerationfollowing gastrectomy for gastric ulceration can almost be eliminated as apossibility. The means of avoiding over-high resection in most caseslie in forming the so-called Pauchet modification to the gastrectomy,that is making a line of transection across the greater curve of the bodyof the stomach at a suitable level, and then taking a tongue-shaped pieceof the lesser curvature up high enough to encircle the ulcer. The lessercurve is then resutured and the cut end of the stomach anastomosed tothe duodenum or jejunum as desired. If the ulcer is much on the posteriorsurface of the stomach, then a tongue-shaped piece of the posterior wallis removed and the anterior mainly used for the anastomosis. This maybe made technically easier, if after mobilisation of the ulcer and of thecurvatures of the stomach, the ulcer is grasped and drawn to the rightand the anterior surface of the body drawn to the left. The clamps arenow placed on the stomach in that position (see Fig. 1). If the ulcer isvery near the cardiac orifice clamps cannot be used to encircle the ulcer,but the incision round the ulcer must be carved out little by little, usingscissors. The stomach then has to be kept empty with a sucker and theposition of the cardiac orifice confirmed by introducing a finger into thestomach, or by inspection. In such cases a stomach tube should be leftin the oesophagus until suturing is finished in order to prevent narrowingof the cardiac orifice by sutures.An ulcer almost reaching the cardiac orifice may be dealt with in this
way, and if a Polya form of operation is done the afferent loop of jejunummay be used to reinforce the lesser curvature suture line near theoesophagus.What of the ulcer which has reached the level of the cardiac orifice,
or which the surgeon feels that he could not safely include in the resection ?
47

NORMAN C. TANNER
Fig. 1. Pauchet manoeuvre adapted for ulcer high on the posterior wall of the stomach.The stomach is rotated to bring the posterior ulcer to what was the position of the lesser
curvature (inset) and the clamps are placed on as shown by the dotted line.
Sometimes the patient is obese and deep chested, or has an associatedhiatus hernia, making work in the subphrenic region very difficult. Insuch types of case I believe in pursuing medical treatment enthusiastically,including bed rest for a minimum of three weeks, (1) to ensure, byobserving the healing process, that the ulcer is innocent, (2) to get theulcer as nearly healed as possible. After this then the best course is to doas high a gastrectomy as possible, but just below the ulcer level. If thereis doubt concerning the benignity of the ulcer then a biopsy and examina-tion of a frozen section may be undertaken before proceeding to resect
48

NON-MALIGNANT AFFECTIONS OF THE UPPER STOMACH
below the ulcer. The progress of the ulcer must thereafter be followedgastroscopically. There is not a great deal of good literature on this sub-ject but several good reports have been given,1 and the only two caseswhich I have dealt with in this manner, three years ago, have been entirelysatisfactory.
Hourglass StomachI have mentioned that in the treatment of high gastric ulcer, it is possible
by fashioning the line of gastric transection 'a Pauchet, that a reasonableamount of stomach can be conserved and a very high resection is unneces-sary. There is a rare exception to this rule, namely the high hourglassdeformity. Here, if gastrectomy is to be carried out, the stomachshould be transected just above the hourglass scar, but this may involvealmost a complete resection. In an elderly or feeble person I do not thinkit would be incorrect to carry out the now almost obsolete operation ofsleeve resection for the condition.
Is the Ulcer Benign or Malignant?Every effort should be made to determine before operation whether the
ulcer is benign or malignant. If the X-ray examination leaves any doubton the matter gastroscopy or oesophagoscopy should be undertaken,and this will leave very few cases in which there is any doubt. However,some ulcer-cancers have both surface and X-ray appearances identicalwith benign ulcer. In such cases ten to fourteen days' bed rest should begiven and then X-ray and gastroscopy repeated. If there is no evidenceof healing then it is well to regard and treat the ulcer as malignant. Undersome circumstances even after opening the abdomen it remains uncertainwhether the ulcer of the cardiac end of the stomach is benign or malignant.I need not enter into all the points in differential diagnosis concerned withinspection, palpation and perhaps examination of a frozen section ofpart of the ulcer edge. In the upper stomach exact diagnosis is of evengreater importance than in the lower stomach. Radical resection of thelower stomach-and by radical I mean resection of the stomach well wideof the tumour together with omenta and glands-does not carry a muchhigher risk to life than partial resection as for ulcer. In the upper stomach,however, simple resection for ulcer carries a mortality of only betweenone and four per cent., whereas radical resection as for carcinoma willnormally demand thoracotomy, resection of a length of oesophagus,together with the posterior mediastinal and the left gastric lymph glands,splenectomy, &c., and will carry a mortality of between 15 per cent. and30 per cent. Now if a mistake is likely to be made, then to increase therisk to life in the simple ulcer case-the person with very nearly a 100 percent. good life-is to my mind a much worse mistake than to remove acancer incompletely, for the cancer sufferer is a " poor" life, using theinsurance man's terminology. Furthermore, if the error is discovered,the cancer sufferer can be operated on again and the radical procedure
49

NORMAN C. TANNER
carried out in a second stage. If the simple ulcer sufferer has lost his life,or unnecessarily lost his whole stomach, nothing more can be done.Therefore, if in doubt despite careful consideration and examination Iwould say treat the case of high gastric ulcer as a simple ulcer.
The Surgical Approach to Simple Ulcer at the Cardiac End of the StomachIn nearly every case of simple peptic ulceration, provided that good
anaesthesia and adequate muscular relaxation is obtained, the lesion canbe quite adequately dealt with by an abdominal incision, preferablyright or left paramedian. I have no doubt that a laparotomy is less riskythan a thoracotomy, particularly in the hands of the abdominal surgeon,and is productive of fewer after-effects. One must not of course be abso-lutely rigid on this point, and there might be occasions when a very highgastric ulcer in a patient who is obese and deep chested, or has an associatedhiatus hernia, would be better dealt with by thoracotomy. I can onlysay that I have never found it necessary to approach a simple gastriculcer transpleurally, though two cases were dealt with by this route undera pre-operative mis-diagnosis of carcinoma.
Herniation of the Upper StomachThe stomach may be partially extruded through hernial orifices in the
diaphragm, through the oesophageal hiatus, pleuro-peritoneal canal,the foramen of Morgagni, or through openings resulting from congenitalabsence of or trauma to the diaphragm. Less important is herniationthrough congenital, acquired or post-operative umbilical or epigastrichernia. Of them all the most important is herniation through the oeso-phageal hiatus, and it is also the most frequent, accounting for over fourout of five of the cases coming to operation 2.Now it is not proposed to go into great detail concerning the various
types of hernia or to discuss the oesophagus in detail, but rather to con-sider how the upper stomach is affected. Part or the whole stomach maybe herniated, and the colon, spleen and other organs may follow thestomach.
Three forms of oesophageal hiatus hernia are usually described. Thefirst is the congenital short oesophagus type which of course is notcorrectly speaking a hernia at all. Both the septum transversum, fromwhich the anterolateral part of the diaphragm is formed, and the stomachanlage which appears as a thickening of the foregut, are present at thelevel of the fourth cervical segment in the 3mm. embryo. Normally theyboth descend to the adult position, but occasionally the descent of thestomach is arrested, resulting in a shortened oesophagus and the presenceof the upper stomach in the thoracic cavity, above the diaphragm.The second form or " para-oesophageal hiatus hernia " is one in which,
although the cardia remains in its normal position, as a result no doubt ofthe persistence of part of the fibro-elastic diaphragmatico-oesophageal
50

NON-MALIGNANT AFFECTIONS OF THE UPPER STOMACH
ligament, there is a defect in the oesophageal hiatus through whichpart of the gastric fundus herniates into the thoracic cavity, to lie at theside of the oesophagus.The third and commonest form is the sliding type in which the oeso-
phageal hiatus is enlarged or defective, the diaphragmatico-oesophagealligaments which normally tether the cardia region are stretched, atrophiedor torn, and so, either permanently or on straining, the lowest oesophagus.and upper stomach slide up into the posterior mediastinum.
SymptomatologySymptoms resulting from herniation of the stomach may be entirely
absent. There may be symptoms of oesophagitis, caused by the reflux ofgastric juice into the oesophagus, or there may be reflux of gastric juiceinto the mouth without oesophagitis (these latter, relatively more fortunatepeople usually seem to be those with a lower gastric acidity). Our know-ledge of the mechanism which normally prevents the reflux of gastricjuice and chyme into the oesophagus is incomplete. The intricate arrange-ment of the muscle layers at the cardia, the control of the circular muscleof the lower oesophagus, the rather oblique entry of the cardia into thestomach, the apposition of the folds at the gastro-oesophageal junctionand the so-called pinchcock action of the diaphragm, have all beenimplicated, but their comparative importance is uncertain. There is nodoubt, however, that in the presence of gastro-oesophageal sliding hernia,and in congenital short oesophagus, the mechanism fails and gastricjuice comes into prolonged contact with the oesophageal mucosa. How-ever, reflux is by no means the only cause of symptoms. There may besymptoms of gastric obstruction resulting from gastric volvulus orgastric incarceration. Associated disease of the upper stomach may bepresent. Obstruction or torsion of other viscera entering the sac maybe the complication bringing the hernia to light. Rarely there may berespiratory or cardiac embarrassment if the hernia is very large.
Causes of Symptoms which may follow entry of Stomach into OesophagealHiatus Hernia
(1) Sometimes absent.
(2) Reflux of gastric juice(a) Oral regurgitation without oesophagitis (usually low acidity).(b) With oesophagitis-dysphagia
painhaemorrhage (massive or chronic anaemia)acute perforation of ulcercicatricial stricture 4- shortening of oeso-
phagus.
51

NORMAN C. TANNER
(3) Gastric obstruction(a) Due to incarceration in sac(b) Due to volvulus of stomach, "upside down " stomach(c) Delayed emptying following heavy eating or drinking.
(4) Disease in the herniatcd stomach, erosion, ulceration, atrophy,carcinoma.
(5) Intestinal obstruction of small bowel or colon entering the sac withthe stomach.
(6) Respiratory or cardiac embarrassment in large hernias.
The symptoms due to these various factors are not always clearly cut,but among the more common are complaints of dysphagia, epigastric orthoracic pain after meals, fluid regurgitations, eructations or vomiting,pallor, haemorrhage, dyspnoea and palpitations.The painful sensations may radiate through to the back and be brought
on by recumbency, or by eating, and they may be relieved by sitting up.Sometimes the patient has a feeling of distension as a result of temporarygastric obstruction. Some are relieved by regurgitation or vomitingwhich in some occurs readily as a result of incompetence of the cardia.On the other hand in rare cases the dilated stomach may press on anddeform the lower oesophagus and prevent the regurgitation of fluid orair, thus adding to the distress. The attacks may be episodic-that is amatter of a few hours from time to time suggesting that the incarcerationof the stomach is intermittent, or there may be the periodic remissionsand relapses typical of peptic ulceration. Haemorrhage may be obviousand even massive, or it may be occult. The most frequent cause of theanaemia is bleeding from the eroded oesophagus, but it may be due tocongestion or erosion of the incarcerated stomach, or peptic ulcer in theupper stomach. In some it is an iron deficiency anaemia due to an asso-ciated atrophic gastritis or to dietary restrictions.The symptoms may appear at any time from infancy onwards, and
because of their great variety they are notorious for mimicking otherlesions, particularly cholecystitis, peptic ulcer, cardiospasm, oesophagealcarcinoma and cardiac disease.
DiagnosisClinical examination usually gives little help although bizarre findings
may be discovered on auscultation of the chest.Radiological examination gives the greater help. X-ray of the chest
may show a shadow, possibly containing a gas bubble, above the dia-phragm. Barium meal X-ray will show the degree to which the stomachhas entered the chest, whether other parts of the alimentary canal arepresent, and, in the smaller herniae, the extent to which the stomach slidesthrough the hiatus may be shown. In very small herniae the conditionmay be overlooked unless care is taken to examine the patient in a position
52

NON-MALIGNANT AFFECTIONS OF THE UPPER STOMACH
which will reproduce gastric herniation, e.g., in the Trendelenbergposition, or while the patient is straining. Suitable methods of strainingare by flexing both legs at the hips with knees kept straight or by puffingout the cheeks (Valsalva). In some cases the stomach is indented by theoesophageal opening making it difficult to exclude a " filling defect " ofthe stomach. On lying down in some cases barium may be seen to leavethe stomach and re-enter the oesophagus, demonstrating the incom-petence of the cardia and the reason for the reflux of gastric juices intothe oesophagus in such cases. The cardia may be quite changed from itsusual appearance and appear to come from the highest part of the stomach.In others, oesophageal deformity resulting from displacement, inflamma-tion and cicatrization will be present. It must not be forgotten thatcarcinoma of the cardia region may co-exist with gastric herniation.
In all cases with severe symptoms endoscopic examination should bemade, provided there is no contra-indication.By oesophagoscopy the presence of oesophagitis, stricture or oeso-
phageal ulceration will be made evident. In the absence of oesophagitisit may be discovered that gastric contents enter the gullet with abnormalfreedom and the oesophagus may appear patulous and rather short, or itmay be of normal length. The latter information is valuable as it indicatesthat at operation the oesophagus will be sufficiently long to draw thecardiac end of the stomach back into the abdominal cavity.
Gastroscopy may give considerable information if carried out by onewell practised in this method of endoscopy. If there is no oesophagealstenosis the instrument can usually be passed with ease, though skill isnecessary in order to pass through the part of the stomach narrowed bythe diaphragmatic opening.
If the cardia and part of the cardiac end of the stomach are intra-thoracic as in the congenital short oesophagus and sliding types of hernia,the condition can usually be recognised. The lower stomach and pyloricantrum may appear normal. On withdrawing the gastroscope the mucuslake is seen and then the stomach narrows as if the cardia had beenreached. On passing through the narrowed area, however, it will be foundthat the cavity reopens and stomach folds are seen again. On inspectingthe narrowed area through which the instrument passed it will be seento be a rounded opening lined with closely opposed gastric folds. Theopening will be seen to widen with expiration and narrow with inspirationbut remain the same diameter if the patient holds his breath-demon-strating that it is a narrowing of the body of the stomach caused bypressure of the oesophageal hiatus in the diaphragm. The upper compart-ment is the intrathoracic part of the stomach. It may also be noticed thatthe stomach slides up and down inside the constricted area. On lookingat the lower-most part of the intrathoracic compartment a second mucuslake, similar to the one seen below the diaphragm, will be found-showingthat there is a small gastric residue both above and below the diaphragmlevel. On turning the instrument anteriorly one sometimes finds the
53

NORMAN C. TANNER
gastric wall bounding wildly-this of course being the cardiac movementstransmitted through the stomach wall. On withdrawing the instrumentfurther the true cardia with its change from gastric to the paler and flatteroesophageal mucosa will be found.
In addition to finding or confirming the presence of a hiatus hernia,gastroscopy is useful on occasions when in addition it leads to the demon-stration of mucosal atrophy, mucosal erosions, sometimes a high gastriculcer, or a carcinoma. In some cases of herniation of the upper stomachit will be impossible to introduce the gastroscope.
Treatment of Herniation of the Upper StomachMinor degrees of symptomless herniation through the oesophageal
hiatus are so common, particularly in the elderly, as to be of no moresignificance than a mild degree of direct inguinal " bulging " in the aged,and are no more in need of repair. Even the large herniae in the feebleand elderly require no treatment unless they are producing symptoms.
In the minor degrees of the condition and in feeble subjects medicaltreatment may be tried. This involves sleeping with the head of the bedraised and with many pillows in order to diminish the gravitational entryof gastric juice into the gullet and to return regurgitated juice into thestomach. It also makes use of gravity as an aid to reduce the stomachinto the abdomen. A regime of frequent small feeds with milk betweenmeals to buffer the regurgitated gastric juice is ordered. Frequent dosesof non-absorbable alkali should be taken between meals and at night.The ideal surgical treatment is of course to repair the hernia and return
the stomach to its normal position, but each case requires carefulconsideration on its own merits.
If there is a reflux oesophagitis with or without ulceration or scarring,then the alternative aims are (1) to prevent or diminish the reflux,(2) to diminish the peptic digestive activity of the refluxed fluid. Thefirst aim may be best obtained by operative repair of the hernia, afterreducing the stomach into the abdomen. The second, that of diminishingthe acid-peptic activity can be obtained in one of several ways, (a) by anextensive lower partial gastrectomy, (b) by vagotomy combined withpyloroplasty, or (c) by oesophago-jejunostomy after transecting thelowest oesophagus, either with or without total gastrectomy. Obviouslythe first method, hernia repair, should be used whenever possible. Thegastrectomy or vagotomy, which are still under trial, are alternatives ifreduction of the stomach is impossible, and if there is a severe oesophagitis.Oesophageal transection followed by aRouxtype ofoesophago-jejunostomyis a method of treatment for reflux oesophagitis which is complicated bybleeding, stenosis or intractable pain. It should only be used when herniarepair is impossible or has failed to produce relief. The stomach need notbe removed. It is a drastic treatment but provides a certain cure of theoesophagitis.
54

NON-MALIGNANT AFFECTIONS OF THE UPPER STOMACH
In cases where there is no severe oesophagitis and the main complaintis of post-prandial pain, apparently due to incarceration or rotation of thestomach in the hernia, then again reduction of the stomach and repairof the hernia is the most satisfactory procedure. However, many of thesufferers from the condition are feeble, and in such cases it is well worthwhile to try crushing the left phrenic nerve first. It often gives considerablerelief even in some cases with oesophagitis. It is not quite clear whyphrenicotomy should have such an effect. No doubt it relaxes the tensionin the oesophageal hiatus and enables the stomach to pass through moreeasily. The raised diaphragm too probably slightly increases the intra-thoracic and lowers the intra-abdominal pressure and so there is lesstendency for the stomach to be drawn up into the chest. Permanentinterruption of the phrenic nerve has the disadvantage of causing atrophyof the diaphragm and should not be done in patients in whom it is likelythat the hernia will be later repaired. On the other hand temporaryinterruption relaxes the diaphragm and undoubtedly facilitates subsequentattempts to repair the hernia.
In some cases it is not possible to reconstruct the hiatus round theoesophagus, for example in congenital short oesophagus, or in cases ofcicatricial shortening or fixation of the oesophagus. In such cases thefirst move is to perform a phrenic nerve crush. It may then be possible,using a transthoracic approach, to draw the oesophageal hiatus highenough to surround the oesophagus. If this is not possible partial resectionof the stomach to lower its acidity, or oesophageal transection followedby oesophago-jejunostomy may be required, provided that the symptomswarrant it.
Resection of the lower oesophagus and upper stomach-upper partialgastrectomy-was for a time considered a suitable operation for pepticoesophageal ulceration, and good results are sometimes obtained by it.However, it is a severe operation and unless the greater part of the stomachis removed there is a possibility that the regurgitating gastric fluid-forreflux into the oesophagus still continues after upper gastric resection-may lead to further oesophageal erosion. A very extensive lower partialgastrectomy is probably more satisfactory, though as I have inferred, itis an operation which is still under trial.
Benign Tumours of the Upper StomachThese are similar in their pathology and course to those of the lower
stomach. They may be conveniently divided into the epithelial tumours,and the connective tissue, or mesoblastic tumours. The epithelial tumours,usually adenomata of the upper stomach, are nearly always symptomless,and come to the attention of the surgeon as a result of associated disease,for example, atrophic gastritis, carcinoma or ulcer. Sometimes thetumours are multiple and a polypoid tumour of the pyloric end maycause symptoms by prolapsing into the pylorus and causing gastric
55

NORMAN C. TANNER
obstruction. Single non-ulcerated tumours of the stomach should bekept under gastroscopic observation in view of their probable tendencyto malignant transformation. If there are multiple epithelial tumoursone may reasonably consider that the likelihood of malignant diseasesoccurring is high and so partial gastrectomy should be performed. Idoubt if it is justifiable to perform total gastrectomy in such cases, a highpartial resection should suffice, but any isolated tumours in the fundusshould be separately excised or fulgurated at the time of gastrectomy.In patients who have isolated fundic adenomata, and even after gastrec-tomy, it is wise to maintain careful observation for the remainder of theirlives. Such observation must include radiological examination if thereis any change in the symptoms, or periodic gastroscopy in those patientswho find gastroscopy no ordeal.The mesoblastic tumours are usually single, though occasionally multiple.
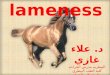
Small insignificant lipomata, fibromata, myomata or islets of ectopicpancreas may be found. The large tumour is usually either a leiomyoma,neurilemmoma, or fibromyoma. These may attain a great size and areprone to ulcerate, bleed, or intussuscept into the pylorus. Even fundictumours may enter the duodenum, leading to bouts of epigastric colicand vomiting (Fig. 2). It is not always easy to differentiate thesetumours from the sarcomata, either macroscopically or microscopicallyand they should be excised, together with a generous circumference ofmucosal and muscular tissue at the base. This may be most convenientlycarried out as a partial gastrectomy or wedge resection, though if thetumour base is near the cardia a somewhat more limited excision isjustifiable, unless malignancy is suspected, in which case a formal upperpartial gastrectomy (oesophago-gastrectomy) is advisable.
Diverticulum affecting the Upper Stomach
In a series of 1,750 gastroscopic examinations the writer found fivegastric diverticulae, four being in the upper stomach.
Diverticulum of the stomach may be congenital or acquired and theacquired type may result from pulsion or traction. The condition is mostcommonly seen in middle life but has been reported in infancy and youngadults. In my experience the commonest site for diverticulum is high onthe posterior part of the lesser curve of the stomach. The diverticulumis formed of gastric mucosa covered with thinned-out muscle and peri-toneum and it may extend between the layers of the gastro-hepaticomentum. There appears to be a congenital or acquired weakness in themusculature at this point. Traction plays no part and none that I have seenin this region was due to the stretching of a healed ulcer scar.
It is not uncommon to find other lesions associated with diverticulum.Diverticula may be found in other parts of the alimentary tract, but moreoften it is associated with an entirely different type of lesion, for example,peptic ulcer, gastritis, abdominal carcinoma or gallstones.
56

NON-MALIGNANT AFFECTIONS OF THE UPPER STOMACH
Fig. 2. X-ray showing a leiomyoma of the fundus which has entered the duodenum.The stalk of the tumour is seen as a tubular filling defect to the left of the oesophagealopening. The tumour, filled with a thin layer of barium, expands the duodenum.
SymptomsMost gastric diverticula, like duodenal and colonic diverticula, are
symptomless, and that is why they appear to have a high incidence ofassociated lesions. It is not the diverticulum but the symptoms of theassociated lesion which first direct attention to the stomach in the majorityof cases.
In one case associated with a gastric ulcer, the high diverticulum andthe ulcer were both clearly seen on gastroscopy. The patient was givencomplete bed rest, diet and alkalisation. Three weeks later all symptomswere gone, and on repeating the gastroscopic examination the ulcer wasseen to be soundly healed but the diverticulum was quite unchanged. Inanother case associated with atrophic gastritis medical treatment gave no
57

NORMAN C. TANNER
Telief to the symptoms and eventually I removed the diverticulum. Thepatient was pleased to lose his diverticulum and to have the reassuranceof a laparotomy, but his symptoms were not really greatly improved,possibly because the symptoms were due more to the gastritis than to theKdiverticulum.
However doubtful and indefinite the symptoms of a gastric diverticulumusually are, there is no doubt that a large diverticulum immediately belowthe cardiac orifice may give rise to epigastric discomfort, particularly afterswallowing or after meals, and the pain may radiate into the back. Loss ofweight may occur. Haematemesis or melaena is sometimes associated withdiverticulum, but whether the bleeding results from the diverticulum is notwell established.The diagnosis of high gastric diverticulum usually depends on finding a
smooth narrow-necked outpouching from the stomach on X-rayexamination. There may be a fluid level with air in the upper part of thepouch and barium may remain in the diverticulum for up to 24 hours afterit has been taken.By gastroscopic examination one can usually differentiate it from pene-
trating ulcer. The mouth of the diverticulum is seen to be lined withgastric mucosa, and gastric folds may be seen to enter the diverticulum.The inner side may be seen to be spherical in shape and a small pool ofmucus is sometimes seen inside the diverticulum.TreatmentNo treatment beyond that of associated more severe disease is
required in the majority of cases, but in some cases of very high sub-cardiac lesions the symptoms may be definite and severe enough towarrant surgical intervention. The discovery of the diverticulum at lapa-rotomy is not always easy. Visualisation may be improved by dividingthe left triangular ligament of the liver and flexing the left lobe over to theright. It may be necessary to divide the left gastric pedicle in order ade-quately to explore the posterior part of the upper lesser curvature of thestomach. When the diverticulum is found the possible alternativeprocedures are to excise the diverticulum or to invaginate the diverticulumand to repair the muscular defect. The latter is very easy, and is satisfactoryif the diverticulum is not near the cardiac orifice. If the diverticulum isnear the cardiac orifice it must be excised, for after invagination such adiverticulum may become oedematous and swell, leading to ball-valveobstruction of the cardia. This occurred in a case of mine and afteroperation the patient could swallow air and fluid and solids, but wasunable to eructate or vomit. This led to intense post-operative gastro-intestinal distension, which required gastric decompression and laterexcision of the diverticulum.Gastric Varices
In cases of portal hypertension secondary to obstruction of the portalvein flow, as for example in hepatic cirrhosis, upper gastric varices may
58

NON-MALIGNANT AFFECTIONS OF THE UPPER STOMACH
develop as an extension of the oesophageal varices which carry the col-lateral venous circulation between the hypertensive gastric veins of theportal circulation and the normotensive azygos veins of the systemicvenous circulation.2 What is less well known is that in the cardia regiongastric varices may develop as an extension of the oesophageal varices.In certain unusual cases of extrahepatic portal block there may be gastricvarices and little or no oesophageal varices. For example, if there is alocalised obstruction in the middle of the splenic vein, the tension rises onthe splenic side of the obstruction but is normal in the portal and leftgastric veins. As a result a collateral circulation develops between thehypertensive vasa brevia and the normotensive left and right gastricand right gastro-epiploic veins and this circulation is more prominentin the body of the stomach than it is in the slighter collateral circulationbetween the vasa brevia and the azygos veins in the oesophagus (Fig. 3).
It is thus important to remember that gastric rather than oesophagealvarices may be the cause of bleeding in some cases of portal hypertension.A practical application of this finding is that in resection of the oesophagus
Fig. 3. An obstruction in the splenic vein. A collateral circulation between the hyper-tensive and normotensive parts of the portal circulation develops across the stomach
and gastro-epiploic arch.
595

NORMAN C. TANNER
for varicosities it is always wise to include the upper stomach in theresection. The presence and extent of gastric varices can usually bedetermined by gastroscopic examination.
Post-Operative Conditions of the Upper Stomach
After lower partial gastrectomy for ulcer the stomach may remainnormal in appearance, but not infrequently it undergoes gastritic changes.Gastroscopic examination may reveal an abnormal degree of stippledcongestion and later atrophic changes may occur. Not a few stomachswhich are the seat of gastric ulcer are gastritic at the time of operation,but there is some evidence that the development of atrophic gastritis issomewhat more rapid after gastrectomy than is found normally.
Oesophago-gastric anastomosis, an operation which was once morepopular than it is now in the treatment of cardiospasm, may also lead togastric changes. It is nowadays well-known that in some of these casesthe wide anastomosis made between the gastric fundus and the oesophagusallows the regurgitation of gastric juice into the oesophagus, resulting inpeptic oesophagitis with all its attendant risks of haemorrhage, cicatriza-tion and pain. Not so well known is the fact that gastric changes mayalso occur.Not every case of haemorrhage is due to erosive oesophagitis or oesopha-
geal ulcer. Peptic ulceration of the upper stomach just below the oeso-phagogastric suture line may occur.3 In a case which I treated oeso-phagogastric anastomosis was followed by violent persistent haematemesis,which was thought to be due to an acute oesophagitis, but at autopsyit was found to be the result of acute erosive gastritis.
REFERENCES1 COLP, R. and DUCKERMAN, L. J. (1946) Ann. Surg. 124, 675.2 HARRINGTON, S. W (1948) Abdominal Operations [2nd Edition] p. 1197. New
York, Appleton Century.3 ScoTr, W. J. M. and EMERSON, G. L. (1951) Rev. Gastroent. 18, 257.
RESTORATION AND DEVELOPMENT FUND
Viscount Nuffield's magnificent gift of £250,000 for the building of theNuffield College of Surgical Sciences has now been completed by thefinal instalment of £25,000.The Wellcome Trustees have generously increased their grant for the
building of the Wellcome Museums from £80,000 to £100,000.Other recent donations include £100 Os. Od. from Mr. R. S. Corbett
and £50 Os. Od. from Professor Francis Stock.
60