Embed Size (px)
Citation preview

Developing a library of authenticated Traditional ChineseMedicinal (TCM) plants for systematic biological evaluation —Rationale, methods and preliminary results from a Sino-American collaboration☆
David M. Eisenberga,c,*, Eric S.J. Harrisa,b, Bruce A. Littlefielda,b, Shugeng Caoa,b, JaneA. Craycrofta, Robert Scholtena, Peter Baylissd,e, Yanling Fuf, Wenquan Wangg, YanjiangQiaod, Zhongzhen Zhaoh, Hubiao Chenh, Yong Liug, Ted Kaptchuka,c, William C. Hahnd,Xiaoxing Wangd, Thomas Robertsd, Caroline E. Shamui, and Jon Clardya,ba Osher Research Center, Division for Research and Education in Complementary andIntegrative Medical Therapies, Harvard Medical School, 77 Louis Pasteur Avenue Suite 1030,Boston, MA 02115, USAb Department of Biological Chemistry and Molecular Pharmacology, Harvard Medical School, 240Longwood Ave., Boston MA 02115, USAc Department of Medicine, Division of General Internal Medicine, Beth Israel Deaconess MedicalCenter, Boston MA 02215, USAd Department of Cancer Biology and Medical Oncology, Dana Farber Cancer Institute, Boston,MA 02115, USAe Department of Pathology, Harvard Medical School, 240 Longwood Avenue, Boston, MA 02115,USAf International Cooperation Center, Beijing University of Chinese Medicine, 11 Bai San HuanDong Lu, Chao Yang District, Beijing 100029, PR Chinag School of Chinese Pharmacy, Beijing University of Chinese Medicine, No. 6 Wangjing ZhongHuan Nan Lu, Chaoyang District Beijing 100102, PR Chinah School of Chinese Medicine, Hong Kong Baptist University, 7 Baptist University Road, KowloonTong, Hong Kong Special Administrative Region, PR Chinai ICCB-Longwood Screening Facility and Department of Systems Biology, Harvard MedicalSchool, 250 Longwood Avenue, Boston, MA 02115, USA
AbstractWhile the popularity of and expenditures for herbal therapies (aka “ethnomedicines”) haveincreased globally in recent years, their efficacy, safety, mechanisms of action, potential as noveltherapeutic agents, cost-effectiveness, or lack thereof, remain poorly defined and controversial.Moreover, published clinical trials evaluating the efficacy of herbal therapies have rightfully beencriticized, post hoc, for their lack of quality assurance and reproducibility of study materials, as
☆Dedicated to Dr. Norman R. Farnsworth of the University of Illinois at Chicago for his pioneering work on botanical naturalproducts, his superb inspiration and leadership as world authority in the field of pharmacognosy.*Corresponding author. Osher Research Center, Division for Research and Education in Complementary and Integrative MedicalTherapies, Harvard Medical School, 77 Louis Pasteur Avenue Suite 1030, Boston, MA 02115, USA. Tel.: +1 617 432 8550; fax: +1617 432 1616. [email protected] (D.M. Eisenberg).
NIH Public AccessAuthor ManuscriptFitoterapia. Author manuscript; available in PMC 2012 January 1.
Published in final edited form as:Fitoterapia. 2011 January ; 82(1): 17–33. doi:10.1016/j.fitote.2010.11.017.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

well as a lack of demonstration of plausible mechanisms and dosing effects. In short, clinicalbotanical investigations have suffered from the lack of a cohesive research strategy which drawson the expertise of all relevant specialties.
With this as background, US and Chinese co-investigators with expertise in Traditional ChineseMedicine (TCM), botany, chemistry and drug discovery, have jointly established a prototypelibrary consisting of 202 authenticated medicinal plant and fungal species that collectivelyrepresent the therapeutic content of the majority of all commonly prescribed TCM herbalprescriptions. Currently housed at Harvard University, the library consists of duplicate or triplicatekilogram quantities of each authenticated and processed species, as well as “detanninized” extractsand sub-fractions of each mother extract. Each species has been collected at 2–3 sites, eachseparated geographically by hundreds of miles, with precise GPS documentation, andauthenticated visually and chemically prior to testing for heavy metals and/or pesticidescontamination. An explicit decision process has been developed whereby samples with the leastcontamination were selected to undergo ethanol extraction and HPLC sub-fractionation inpreparation for high throughput screening across a broad array of biological targets includingcancer biology targets. As envisioned, the subfractions in this artisan collection of authenticatedmedicinal plants will be tested for biological activity individually and in combinations (i.e.,“complex mixtures”) consistent with traditional ethnomedical practice.
This manuscript summarizes the rationale, methods and preliminary “proof of principle” for theestablishment of this prototype, authenticated medicinal plant library. It is hoped that thesemethods will foster scientific discoveries with therapeutic potential and enhance efforts tosystematically evaluate commonly used herbal therapies worldwide.
KeywordsHerbal medicine; Library; Traditional Chinese; Ethnomedicine
1. IntroductionThe topic of whether and how plant based medicines (aka herbal remedies) predictably alterthe natural course of human disease has been an essential and complex aspect of medicinefor thousands of years. By contrast, efforts to systematically apply modern scientificstrategies to prove or disprove the therapeutic value of specific medicinal plants,individually or in complex mixtures, and to optimize their rightful place in modern healthcare, represent a more recent trans-disciplinary challenge.
Focusing on Traditional Chinese Medicine (TCM), there was a singular moment in recenthistory when practitioners of TCM and advocates of modern western medicine wereexplicitly called upon to jointly learn from one another, teach one another and, in theprocess, attempt to generate new knowledge for the common good of the next generation.The time was August 1950. The setting was the first National Health Congress of the newlyestablished People’s Republic of China. Chairman Mao Ze Dong spoke on the occasion ofthe proposed establishment of the first five accredited schools of TCM and the need forcollaboration across disparate expert groups. “We should unite all the young andexperienced medical professionals from both Traditional Chinese Medicine and ModernWestern Medicine to form a firmly united front to jointly strive for a great enhancement ofthe people’s health [1]!” Mao’s intention was clear and practical. He sought to proactivelyengage medical experts from both eastern and western traditions to jointly explore what hecalled “The Treasurehouse of Traditional Chinese Medicine,” including its richpharmacopeia.
Eisenberg et al. Page 2
Fitoterapia. Author manuscript; available in PMC 2012 January 1.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

2. Relevance of herbal and TCM productsRoughly half of all approved prescription drugs are natural products, mostly from plants andmicrobial sources, their semi-synthetic derivatives or fully synthetic analogs [2]. Close to70% of all cancer drugs originated from natural products [3,4]. Therefore, the application ofstate-of-the-art technologies to the systematic evaluation of traditionally used plant basedmedicines (aka ethnobotanicals) remains a highly relevant yet scientifically challenging lineof inquiry.
3. Epidemiology and market relevance of herbal and TCM productsHerbal medicine use by the American public has increased dramatically over the past twodecades. The percentage of US adults reporting the use of herbal (non-vitamin, non-mineral)products to treat or prevent disease increased from 2.5% in 1990 [5] to 12% in 1997 [6] to14% in 2000 [7] to 19% in 2002 [8] and 18% in 2007 [9]. The estimated out-of-pocketexpenditures for herbal therapies by the US adult population in 2007 was $14.8B. This isequivalent to approximately one-third of the total out-of-pocket spending on all prescriptiondrugs ($47.6B) that same year [10].
A marketing analysis suggested that sales of TCM herbal products from China increased atan annual rate of 24% between 2004 and 2008 [11]. In 2008, TCM herbal product salesaccounted for an estimated 22% of China’s overall healthcare product revenue and wereestimated at a value of $26 billion US dollars [11].
4. Rationale to build a prototype library based on challenges and lessonslearned4.1. Lessons learned from selected clinical trials
In 2003, the NIH’s National Center for Complementary and Alternative Medicine(NCCAM) warned that a lack of reproducibility, quality control and dosage schedulesinvolving natural products might lead to methodologically questionable and/or negativeclinical studies, thereby diminishing opportunities for further investigations ofethnobotanicals [12].
By way of example, in 2004 a randomized trial was conducted to test the clinicaleffectiveness of an eight herb Chinese formula, sold under the product name “PC-SPES,” insubjects with advanced prostate cancer [13]. As documented in the medical literature, thiscomplex herbal mixture was found to be clinically superior to the standard, high dose,estrogen salvage protocol in terms of overall reductions in PSA levels and time toprogression of disease for 90 randomized study subjects. However, random testing of theherbal mixture revealed it had been adulterated with small quantities of synthetic estrogenand Coumadin [13]. The authors concluded that the true efficacy of this, and other, herbalmixtures will remain uncertain until the quality, consistency and purity of the naturalproducts under evaluation can be ensured [13]. A review of the medical literature in 2005documented that most publications involving the assessment of herbal therapies in clinicaltrials involved no independent verification of the herbal contents under evaluation [14].
The authors of the PC-SPES study also commented on the fact that the levels of estrogenidentified in the commercial PC-SPES products were far too low to have explained theapparent clinical superiority of the PC-SPES therapy as compared with the estrogen salvageprotocol. As such, their comments could be interpreted to raise the possibility, albeit remote,that specific components (i.e. chemical compounds) within the PC-SPES mixture, when
Eisenberg et al. Page 3
Fitoterapia. Author manuscript; available in PMC 2012 January 1.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

added to low dose estrogen, might have resulted in an additive or synergistic effect powerfulenough to alter the course of disease in men with advanced prostate cancer.
A second case of note involved the evaluation of the herb Echinacea (Echinaceaangustifolia DC.) in the prevention of rhinovirus infection (i.e. the common cold). In thisstudy, 437 volunteers were proactively infected with rhinovirus [15]. Subjects were thenrandomized to four groups. Three of the groups received various preparations and doses of acommonly sold Echinacea extract and one group received a placebo. There were nosignificant differences across groups with regard to rates of infection, severity of symptomsor viral titers. As such, the trial was considered to have refuted claims of clinicaleffectiveness of Echinacea. Subsequently, the New England Journal of Medicine publishedcriticisms of the study’s design [16]. These included the suggestion that a differentEchinacea species might have been preferable; that the dose used in the study was far toolow (by a factor of 6) and that a higher dose might have made this trial more clinically andscientifically relevant [16].
A third study involved the evaluation of a popular over-the-counter preparation of the herbsaw palmetto (Serenoa repens (W. Bartram) Small) in the treatment of benign prostatichypertrophy [17]. In this study, 225 subjects were randomized to two groups, one receivinga Saw Palmetto extract in the form of a popular over-the-counter supplement and the othergroup receiving a placebo. There were no significant differences observed between thesetwo groups in terms of symptomatic improvement. An accompanying editorial [18]commented that the study authors had tested a single, commercially available preparation ofsaw palmetto, thereby leaving open the possibility that a different preparation might still beeffective. Furthermore, these authors contended that in the absence of a plausiblemechanism of action, a fair comparison of this herb (or its constituents) to a moreconventional FDA approved therapeutic drug, would be problematic if not impossible.
Lessons learned from these and other ambitious (and expensive) clinical trials suggest thatfuture human clinical trials involving herbal products must ensure the reproducibility andquality of the intervention materials; and, will require an understanding of mechanisms ofaction and dosing prior to the implementation of new, large scale (and expensive) Phase IIor III clinical trials. The current NIH guidelines involving candidate herbal therapies reflectmany of these hard learned lessons [19] as do the Consort Guidelines for publicationsinvolving randomized controlled trials involving herbal interventions [20].
In hindsight, these were methodological inadequacies uncovered by individuals skilled inthe design and conduct of clinical trials. They provided part of the rationale for the studydescribed in this manuscript. What about methodological challenges from the vantage pointof other relevant experts including researchers skilled in botany, chemistry, ethnobotany anddrug discovery?
4.2. Lessons learned from the vantage point of drug discovery and ethnobotanyThe current place of natural products in modern drug discovery is inconsistent with theirpast performance and future potential. Natural products have made, and continue to make,substantial contributions both to understanding basic biological processes and treatinghuman disease. If we focus on cancer, natural products from plants have led to frontlinetherapies such as paclitaxel, vinblastine, camptothecin and etoposide [4]. If we look at theimmediate future, geldanamycin analogs – to pick just one example – are being pursued inclinical trials [21,22]. Thus there is a strong scientific argument for continuing to explorenatural products in drug discovery —an argument that is largely unheeded as pharmaceuticalcompanies cut back on, or eliminate, their natural product programs.
Eisenberg et al. Page 4
Fitoterapia. Author manuscript; available in PMC 2012 January 1.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

Identification of natural product-based leads for Western drug discovery has usually resultedfrom screening of extracts or compounds from diverse biological sources, generally withoutregard to preexisting knowledge of the therapeutic utility of the producing plant. A goodexample is the remarkable portfolio of hundreds of thousands of natural products andextracts amassed by the United States National Cancer Institute (NCI) since the inception ofits natural product-based efforts in 1955 [23]. Between 1960 and 1982, the NCI screenedextracts of 35,000 plant species in collaboration with the U.S. Department of Agriculture(USDA). The strategy adopted was largely one of random selection of a broad range ofnatural product sources as opposed to selection based on medicinal use, i.e. ethnomedicine[4]. To a large extent, the driving force for NCI’s efforts was biological and geographicdiversity rather than pre-existing knowledge of therapeutic utility. Focusing on biologicaland geographic diversity is a typical paradigm of most natural product drug discoverysuccesses, meaning that the use of natural products for Western drug discovery has largelybeen one of trial and error. This approach has been referred to as “bio-prospecting.”Paclitaxel, vinblastine and camptothecin were discovered using this approach. Interestingly,Verpoorte has pointed out that there are an estimated 250,000 flowering plant species onearth while as of 2000, fewer than 15,000 (6%) had been screened for biological activity[24].
In contrast, many cultures around the world have developed ethnomedical traditions basedon therapeutic utility of selected local plants and animals. Such empirical traditions are oftenhundreds if not thousands of years old, as in the case of TCM for which written records existgoing back over 2000 years. Unfortunately, the potential value of ethnomedicines has oftenbeen discounted by Western medicine and science, with several identifiable factorsaccounting for this. First, medical diagnoses in TCM and other ethnomedical systems areoften portrayed in ways that are not readily understood by Western clinicians. Second, TCMand other ethnomedicines are often viewed as fundamentally lacking in the mechanistic,scientific bases that usually underpin claims of Western medical efficacy. Third, there hasbeen a lack of rigorous, well-controlled clinical trials demonstrating clinical efficacy (andmechanisms) of TCM and other ethnomedicines. Fourth, existing scientific and clinicalstudies of TCM have often utilized plants that have been quality compromised, may becontaminated with pesticides or heavy metals, may have been botanically misidentified, orare lacking a consistent and reproducible resupply chain. As such, and as noted earlier, priorstudies have frequently been compromised by quality control and botanical authenticationissues, as well as lot-to-lot variability and lack of knowledge of precise growing locationsand conditions, factors that have too often limited reproducibility. Finally, resupply of herbsfor confirmation and follow-up studies is frequently problematic. The limiting factorsmentioned earlier fall into two main categories: variables related to starting materials, andvariables related to execution or interpretation of scientific and clinical studies. While thetwo are interdependent, without addressing the former, there is little value in pursuing thelatter.
From the vantage point of ethnobotany, researchers have highlighted the difficulties inreplicating the biological activity of a given plant when attempts are made to repeat anexperiment after subsequent recollection [25]. As such, the challenge of reproducibilityremains a formidable one.
There are also challenges in terms of sourcing plant species to be studied. These include:collecting them according to traditional techniques, documenting the precise collection sitesusing GPS technology, authenticating them visually, chemically and, through DNAsequencing, processing and extracting them according to established, traditional andreproducible techniques, storing them properly and so on.
Eisenberg et al. Page 5
Fitoterapia. Author manuscript; available in PMC 2012 January 1.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

Lastly, there is the inherent conundrum which speaks to the heart of the conceptualdifference between traditional (i.e. ethnobotanical) herbal practice and modern (western)drug discovery and therapy. This conundrum can be conveyed through the articulation oftwo testable hypotheses, specifically; do herbal medicines work, when they work,predominantly because of single chemical compounds, albeit in small quantities? Byextension, are herbal medicines and herbal medicine libraries merely repositories forsophisticated “bio-prospecting” in search of novel, and patentable, composition of matterdiscoveries (aka “new chemical entities”) or derivatives of already known chemicalcompounds which can be shown to be of new therapeutic application and benefit? One mustalso consider the fact that herbal therapy as practiced in traditional settings rarely involvesthe prescription of a single herb at a time. Instead, traditional conceptual frameworks, whichpreceded contemporary understanding of chemical compounds and their specific effects onprecise, biological targets, almost always involve multiple herbs and a presumed additivityand/or synergy of effects on the host subject. The shared view among herbalists, in Asia andelsewhere, has been that a mono-therapy approach will be inferior to a multi-therapy,complex herbal mixture approach [26]. By way of example, a typical TCM prescriptionroutinely includes 8–12 herbs, in varying ratios, with one of the herbs serving as the “king”,a second serving in the capacity of “minister”, a third as “adjutant” and a fourth as the“messenger” [27].
Given this disparity of conceptual models, the fundamental (second) testable hypothesis isthat herbal therapies work, when they work, due to complex yet predictable effects ofmultiple compounds within complex mixtures of plant compounds. As evidenced by thenear miraculous success of the three drug “AIDS Cocktail,” we now have unequivocalevidence that multi-drug therapy can sometimes be the best – or only –successful therapeuticoption [28]. The work of Borisy et al. demonstrated the existence of synergistic effectsinvolving multiple (FDA approved) compounds [29] and the work of Wagner hassummarized the existence of synergistic effects involving multiple compounds found in avariety of natural products [30]. Might clinical successes attributed to herbal therapiesinvolve additive and/or synergistic biological effects which can now be more meticulouslydescribed and, ideally, optimized for maximal therapeutic benefit?
Lastly, there is the non-technical challenge that Mao attempted to address a half century ago[1]; specifically, can the two schools of medical thought, Eastern and Western (modernbiomedicine) develop shared research strategies which address the above mentioned knownchallenges without compromising the respective beliefs, practices and fundamental tenantsof each tradition? Can ethnobotanists and modern drug discovery experts established aneffective “united front,” and will this exercise result in novel therapeutic discoveries or not?
To reframe this question, can an artisan collection of authenticated TCM plants beestablished for the purpose of successful systematic biological evaluation and will such alibrary, when screened strategically, lead to the identification of novel compounds, new usesfor known single compounds and/or their derivatives; and/or novel biological mechanisms?With regard to the second hypothesis mentioned earlier, might there also be a newopportunity to employ contemporary high-throughput screening facilities to search foranticipated as well as unanticipated combinations of single compounds which can be shownto be therapeutically effective due to biological additivity and/or synergy of multiple plantderived compounds? Will combinations with evidence of additivity and/or synergy confirmethnobotanical knowledge about specific plant combinations (i.e. formulas) or might entirelyunanticipated active combinations also be identified?
Eisenberg et al. Page 6
Fitoterapia. Author manuscript; available in PMC 2012 January 1.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

4.3. Considerations in the development of a prototype authenticated TCM plant libraryBetween 2006 and 2010, investigators from Harvard Medical School (HMS), incollaboration with colleagues from the Beijing University of Chinese Medicine (BUCM)and Hong Kong Baptist University (HKBU), embarked on efforts to build a prototypelibrary of 202 botanically authenticated, quality controlled, collection site-documentedChinese medicinal plants. Each plant was to be tested for pesticide and heavy metalcontamination and qualified using standards defined by the Chinese Pharmacopeia [31], anofficial publication of the State Food and Drug Administration (SFDA) of the People’sRepublic of China. Such an artisan library could serve as a necessary prerequisite toreproducible pre-clinical studies of TCM herbs. These are mandatory prerequisites to thesubsequent design and implementation of the next generation of animal and human studiesof herbal remedies. Moreover, the ethnobotanical knowledge of TCM experts is essential toestablish this library, and to efficiently guide drug development experts in their search fornovel single compounds, novel uses of previously identified compounds and hypothetically,novel demonstrations of additivity and/or synergy involving multiple plant compoundswithin plants and within complex mixtures of medicinal plants.
In planning for, constructing and evaluating this authenticated TCM herbal library, manyfactors had to be considered including: the selection criteria of medicinal plants to beincluded in the research library; quality assurance including harvest sites and GPSdocumentation; botanical species authentication; collection protocols; plant processingdetails; creation of voucher specimens; testing for pesticides and heavy metal contamination;chemical and quality assessment according to existing standards of the ChinesePharmacopeia; Chinese governmental cooperation, authorization and partnership; storageand shipping logistics of all specimens in China and the US; precise and reproducibleextraction and fractionation procedures; selection of appropriate biological screeningstrategies; establishment of a suitable database and database management system; and,continuous efforts to maintain open communications and opportunities for expandedresearch collaboration among all participating co-investigators.
5. Methods(See Fig. 1 for an overview of the methods employed in the creation of this prototype TCMlibrary).
5.1. Criteria for inclusionThe selection of plants for the authenticated TCM herbal library was based on two maincriteria: (1) the plants were listed in the official Pharmacopoeia of the People’s Republic ofChina (CP) [31] and, (2) the species were not endangered. This latter criterion is of concernsince the over-harvesting of plants from wild sources for use in TCM is a growing problem[32]. For example, some plants used in Chinese medicine are on the Convention onInternational Trade in Endangered Species of Wild Flora and Fauna (CITES) list, includingfamous medicines such as Mu Xiang (Saussurea costus (Falc.) Lipsch.) and Rou Cong Rong(Cistanche deserticola Y. C. Ma) [33]. The official CP includes synthetic pharmaceuticalmedicines, but also many traditional medicines derived from natural sources. At the timethis study was launched, the most recent edition was the 2005 Chinese Pharmacopeia.
The first volume of the 2005 CP includes monographs on Traditional Materia Medica and iscomprised of substances derived from animals, minerals, plants, and fungi. A total of 471monographs based on plant products are included in this volume, comprising 550 differentspecies. The prototype library included a total of 200 species of plants and 2 species offungi, representing more than one-third of all plant species listed in the CP. The 202 selected
Eisenberg et al. Page 7
Fitoterapia. Author manuscript; available in PMC 2012 January 1.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

plants (see Appendix A) are some of the most commonly used in the CP and hence areestimated to represent approximately 75% of all plants used in routine TCM practice.
5.1.1. Monograph summarizing relevant information of each plant—Monographswere written for each species included in the project. The goals of the monographs includedproviding a comprehensive literature review of the traditional uses, as well as a summary ofrecent information about experimental studies of each plant. In particular, it was envisionedthat the monographs would be a useful source of information for screeners of the library.Each monograph included the following sections: names and synonyms of the plant,collection and processing methods, therapeutic indications in TCM and western medicine,types of extracts, major chemical constituents, description of medicinal part of the plant,contraindications, common preparations and inclusion in common TCM formulae, andselected references in the TCM and western literature. The monographs are included in theproject database (see section 5.7).
5.2. Collection protocolWhenever possible, collection locations were selected from the region that is traditionallyknown for production of the plant species being collected. Additionally, each plant specieswas collected from three distinct locations in China separated by hundreds or thousands ofmiles and usually in different provinces, to ensure that at least one of these plants could meetthe appropriate requirements of species identity, quality, and purity, including the absence ofcontamination by pesticides and/or excessive heavy metals. Plant collection consisted ofthree separate activities: environmental investigation, bulk harvest, and voucher collection.The environmental investigation included a survey to ensure that the collection area wassuitable and capable of yielding enough plant material for the project. The bulk harvestconsisted of the harvest of the medicinal part of the plant at the time that the herb istraditionally collected. During the bulk harvest, each sample was collected to give a total of10 kg dry weight. Following the bulk harvest, all herbs were processed according to thetraditional method as specified by the CP. This typically involved the removal of impuritiessuch as other plant species or soil, followed by drying in the sun for a period of days orweeks. Lastly, vouchers of each sample, consisting of flowering or fruiting material of theplant, were collected according to standard protocols [34]. Vouchers have been stored alongwith a voucher of the bulk harvest medicinal part for future reference. The plant acquisitionteam, organized and overseen by BUCM co-investigators and consultants from HKBU,consisted of at least one Chinese herbal medicine resource expert from each of the 30provinces and autonomous zones where plant acquisition took place. In addition, a 34 personBeijing-based acquisition team consisting of faculty and graduate students of BUCM as wellas 8 additional TCM botanical experts oversaw the quality control and processing of allplant samples collected. Authentication of plant species was overseen by a separate group offaculty with TCM ethnobotanical expertise at HKBU. All steps of plant collection weredocumented using a combination of standardized collection forms, GPS data collection,photographs, and video. (See Appendices B–E for examples of photos imported into study’sdatabase). After harvest and processing, plants were authenticated and tested for quality (seesections 5.3 and 5.4).
5.3. Authentication and quality assessmentThe taxonomic identification of each plant was confirmed by multiple experts in China.Plants were authenticated according to morphological and anatomical characteristics [35] bya team at HKBU and examined according to criteria listed in the CP for quality assessmentat BUCM. The quality assessment tests were conducted according to the guidelines andstandards provided in the CP 2005 edition [31]. The CP specifies the method for conductingrelevant tests and provides standard reference values for results. In general, the quality
Eisenberg et al. Page 8
Fitoterapia. Author manuscript; available in PMC 2012 January 1.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

assessment tests include methods for determining the identity and purity of the plant. For thepurposes of the quality assessment tests, the identity of the plant is determined usingmethods such as qualitative thin-layer chromatography (TLC) and reactivity tests. There arealso quantitative tests to determine the concentration of certain chemical ingredients. Forexample, the CP stipulates that licorice root (Glycyrrhiza glabra L.) must have at least 2.0%glycyrrhizic acid by dry weight [31]. Lastly, some of the quality assessment tests relate todetermination of impurities in the plants. For example, many species require a test of waterand ash content. The test of water content is to determine how well the sample may bepreserved, and the test of ash content provides information about the amount of solidimpurities, such as soil, that are included with the plant sample. Samples which did not meetquality assessment tests were considered to be unsuitable for subsequent study as they didnot meet established and reproducible standards of quality assurance. The list of qualityassessment tests stipulated by the CP is provided in Table 1. The methods used for decidingon the results of quality assessment tests and whether the results would necessitate plantrecollection are summarized in Fig. 2.
5.4. Testing for heavy metals and pesticidesFollowing standards established by NSF International and American Standards Institute(ANSI) Standard 173 for acceptable metal levels in dietary supplements [36], all plants weretested for heavy metal and pesticide content, including five heavy metals (As, Cd, Cr, Pband Hg) and pesticide residues.
There is currently considerable variation between different countries for testing pesticides indietary supplements [37], and typically only a few pesticides are routinely examined. Acomprehensive approach to pesticides testing was used in this project, and a broad screenincluding 162 pesticide residues was employed. More details pertaining to these researchmethods are reported separately [38].
5.5. Shipping, import, export and maintenance of plant materialsThe logistics involved in the dried plant material supply chain, from when the material wastransferred from BUCM to HMS possession, included abiding by the export/importregulations for all countries involved, freight forwarders, and insurance to protect theresources. Prior to shipment, it was necessary to apply for and obtain the appropriate importpermits from the United States Department of Agriculture Animal and Plant InspectionServices (USDA APIS). With the USDA APIS permit in hand, service agreements wereexecuted. At certain steps of the project, it was necessary that the dried plant material bulkshipments be maintained in a pest-free, climate-controlled storage facility. For example, thesamples were held in China prior to shipment to the United States. After the samples arrivedin the United States they were placed in storage. In both instances, bulk samples weremaintained in a special storage facility with controlled temperature and humidity. Thesamples currently maintained in the United States are kept at 20 °C and 50% relativehumidity in a state-of-the-art facility.
5.6. Selecting one of three samples for initial extraction and fractionationEach species in the library was collected from three separate locations, but only one sampleper species was to be initially extracted and fractionated for high throughput screening.Samples were selected for extraction and fractionation using two main criteria: (1) absenceor lowest values of heavy metal and pesticide contamination among samples collected foreach species; and (2) ease of collection. Heavy metal and pesticide amounts weredetermined as described elsewhere [38]. Ease of collection was judged by collection expertsat BUCM. The explicit decision tree used to make determinations is summarized in Fig. 3.
Eisenberg et al. Page 9
Fitoterapia. Author manuscript; available in PMC 2012 January 1.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

5.6.1. Extraction and fractionation procedures—Between 1 and 4 kg of the herbsamples selected for extraction and fractionation were subjected to industrial-scale grinding,followed by extraction in 95% (v/v) ethanol for 30 min with sonication, using a solvent-to-herb volume ratio of 7:1. Using this method, compounds with a broad range of polarity canbe extracted. Tannins were removed from the resulting ethanol extracts via polyamidecolumn chromatography (polyamide: extract=10:1), followed by desalting and defatting onHP-20 resin (HP-20: extract=50:1). The HP-20 column was washed with water to removesalts, then with ethanol, and finally with 50% ethanol/dichloromethane to remove fattyacids. The resulting ethanol eluate was subjected to large-scale reverse-phase C-18 HPLCchromatography, with step-wise elution using 2% ethanol increments from 0 to 100% in 70min and then 100% ethanol for 26 min, resulting in approximately 48 fractions per extract.Target quantities were 15 mg eluted material per fraction: 15 mg or less of each fraction wasthen dried in 4 ml glass vials for future formatting for screening. For each fraction for whichmore than 15 mg of material was obtained, the extra material was dried in appropriatelysized glass vials. All dried fractions were stored at −20 °C until prepared for screening orused for further purification steps.
5.6.2. Preparing extract fractions for screening—To re-suspend fractions, 100%DMSO was added to each dried fraction in 4 ml vials for a final concentration of 15 mg/ml.DMSO was added using the Biomek FX (Beckman Coulter, Inc.) automated pipetting workstation, allowing 352 fractions to be processed in each plating session. Small (10 mm)Teflon-coat stir bars (V&P Scientific) were added to each 4 ml glass vial and vials werestirred overnight at room temperature. Fractions that did not go into solution by stirring werehand-pipetted briefly the next morning to fully re-suspend them. Fractions were aliquoted byhand into 96-deep well plates (VWR 4002-011). To make plates for screening, extracts werere-formatted from the 96-well master plates into 384-well plates (ABgene AB-1056) using aVelocity-11 V-Prep (Agilent) automated pipetting work station. All plated extracts werestored at −20 °C.
5.7. Construction of electronic databaseIn order to meet the data requirements of this initiative, a novel database was designed toorganize and store data related to all aspects of plant collections, authentication, shipping,processing and biological screening. The database, called the “Traditional MedicineCollection Tracking System (TM-CTS),” was designed to support the daily needs of theproject in the context of the international collaboration between investigators in the UnitedStates and China, and to include information related to all aspects of the project from plantcollection through extraction and fractionation. In addition, the database was constructed towork in concert with the screening database used in the project. The TM-CTS is described ina separate paper [39].
5.8. Initial screening strategiesStrategies used for screening the initial collection of several thousand pre-fractionatedextracts were based on five major themes. First, assays needed to represent therapeutic areasof high unmet medical need. Second, assays were to represent the most “cutting-edge”biological advances in their respective therapeutic areas, in recognition of the fact that thegoal was to identify and develop high-impact new drugs with therapeutic efficacies orscopes going beyond existing medicines. Third, assays needed to be carried out on smallenough scales to support high throughput screening (HTS) in 96- or 384-well plate formats,and to not require unreasonably large amounts of material. More specifically, targeted assayvolumes ranged from 0.1 to 1.0 μL per assay point, with occasional exceptions made for 8–10 μL per assay point for certain cell-based assays considered to be of uniquely high value.Fourth, sufficient down-stream assay capabilities, particularly the existence of appropriate in
Eisenberg et al. Page 10
Fitoterapia. Author manuscript; available in PMC 2012 January 1.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

vivo animal models for the particular disease being targeted, needed to exist, in order toensure that any lead compounds identified in initial screening campaigns could be furtherdeveloped pharmacologically to a point where drug development value could be firmlyestablished. Fifth, assays needed to offer the possibility of eventual patent-protectedlicensable opportunities (compound, target, or both), since it was recognized that eventualdevelopment of lead compounds would depend on interest by the pharmaceutical industry,which would likely require appropriate intellectual property protections allowing for a returnon investment.
Guided by the above five principles, the first several thousand fractions were screenedacross a range of assays representing a variety of therapeutic areas. Although beyond thescope of this manuscript, active screens included targets in the following areas: oncology(angiogenesis, tumor-specific differential cytotoxicity, and cell survival pathways), anti-infectives (bacterial, anthrax), anti-virals (HIV-1), diabetes and neurodegeneration(Alzheimer’s disease, Parkinson’s disease). Other therapeutic areas under considerationincluded assays for novel targets in arthritis, cancer (and non-cancer) stem cells,cardiovascular disease, anti-infectives (Methicillin-resistant Staphylococcus aureus,tuberculosis, influenza A/H1N1), hepatitis C, immuno-oncology approaches, inflammation,multiple sclerosis, and pain.
5.9. Description of selected (initial) screens involving cell based and whole organism (e.g.Zebra fish) assays
Human fibroblasts and cancer cell lines [LNCaP, PC3 (Prostate), MCF7, MDA-231(Breast), A549 (Lung), BJ Fibroblasts] were propagated using standard conditions assuggested by ATCC. Cell proliferation and/or survival were determined by using Cell TiterGlo (Promega) in a 384-well format assay as previously described [40].
For zebra fish screening, fractions were delivered robotically to 96 well plates. Fourembryos were added per well by pipette at roughly 6 h post fertilization to allow earlydevelopment to occur before treatment. More than 1000 extract fractions were initiallyscreened at nominal concentrations (based on the assumption of a pure compound of MW500) on embryos in 10% Hank’s Saline with 0.003% phenyl thiourea in water, observingfrom 6 h post fertilization to 72 h post fertilization. All wells were examined by lightmicroscope to look for signs of altered development and impaired angiogenesis. Fractionsthat showed grossly defective development were not further analyzed.
5.9.1. LC/MS and NMR techniques for compound characterization—LC/MS wasperformed on an Agilent 6130 Single Quadrupole system. NMR spectra of activecompounds were obtained on a Varian 600 MHz spectrometer. Compounds were identifiedeither using authentic samples or comparing their chemical shifts with those reported in theliterature.
5.9.2. International collaboration agreements—Agreements covering the scope ofwork, ownership of materials and intellectual property, sharing of potential financialrevenues and co-authorship of academic publications were negotiated by representatives ofthe participating US and Chinese Academic Institutions. These were also reviewed byrepresentatives of the Chinese Ministry of Health, Chinese Ministry of Education, StateAdministration of TCM, Chinese FDA and the Chinese Ministry of Science andTechnology.
Eisenberg et al. Page 11
Fitoterapia. Author manuscript; available in PMC 2012 January 1.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
6. Results6.1. Current status of the authenticated TCM library
The initial plans of the participating co-investigators involved the collection of 202individual TCM species in triplicate and the completion of all aspects of the methodsdescribed earlier as applied to all collected specimens. As envisioned, this would haveresulted in an estimated 10,000 fractions. A total of 3709 fractions from 80 TCMauthenticated species have been created and screened to date. Consequently, the resultsreported here are those that have been obtained based on work completed thus far.
At least one bulk sample has been collected from each of 202 species of TCM plants andfungi. Of these, 186 species have been authenticated according to macroscopic andmicroscopic characteristics, 158 species have been tested for quality according to standardsin the CP [31] and 129 species have been tested for heavy metals and pesticides. The bulksamples of 136 species and voucher samples of 79 species have been delivered to HMS,with the remaining samples in China. All of the data and images related to collections,authentication, extraction, and fractionation, are currently stored in the project’s TM-CTSdatabase for future reference [39].
The mean number of fractions per sample is 45 (median 47; range 19–52). In addition to thefractions that were eluted from the HPLC column, the total number of fractions per plantalways included four additional fractions that represent the crude extract, the desalting anddefatting washes of the crude extract, and the cleaned extract prior to fractionation. Forexample, the maximum number of fractions for one plant, 52, is equal to these four fractionsplus a maximum of 48 possible fractions that are eluted from the HPLC fractionationcolumn. These four additional fractions were included in the screening library. See Table 2for a summary of the status of the library to date.
6.2. Summary of plant species includedAlmost all (~99%) of the plants included in the prototype TCM library are flowering plants.The library includes 2 species of gymnosperm and 2 species of fungi. Of the floweringplants, the most commonly represented families are: Asteraceae, (10.7%), Rosaceae, (5.9%),Lamiaceae, (5.4%), Fabaceae, (4.9%), and Liliaceae, (4.9%). Of the bulk samples in thelibrary, the majority come from underground parts of plants (42.4%), including bulbs,rhizomes, roots, and tubers. Other medicinal plant parts in the collection, consistent withTCM practice, include fruit and/or seed (29.8%), leaf and/or stem (17.1%), flower (5.4%),and whole plant (4.4%). The names of all species included in the library appear in AppendixA.
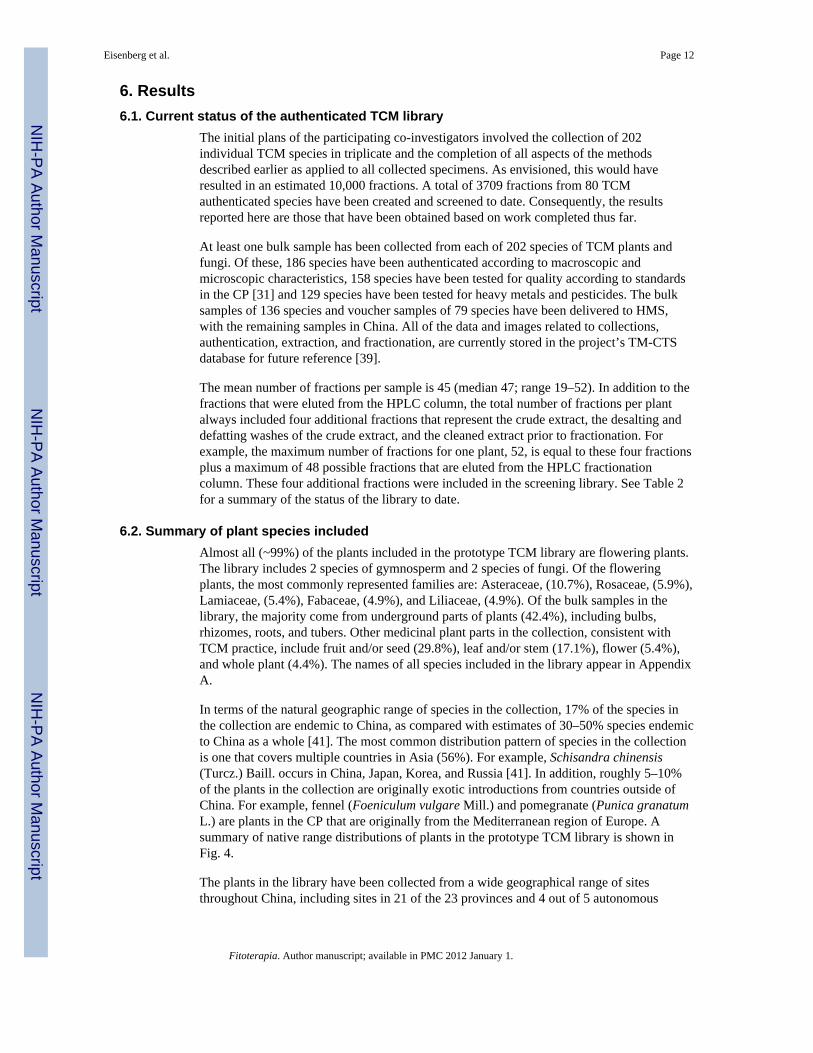
In terms of the natural geographic range of species in the collection, 17% of the species inthe collection are endemic to China, as compared with estimates of 30–50% species endemicto China as a whole [41]. The most common distribution pattern of species in the collectionis one that covers multiple countries in Asia (56%). For example, Schisandra chinensis(Turcz.) Baill. occurs in China, Japan, Korea, and Russia [41]. In addition, roughly 5–10%of the plants in the collection are originally exotic introductions from countries outside ofChina. For example, fennel (Foeniculum vulgare Mill.) and pomegranate (Punica granatumL.) are plants in the CP that are originally from the Mediterranean region of Europe. Asummary of native range distributions of plants in the prototype TCM library is shown inFig. 4.
The plants in the library have been collected from a wide geographical range of sitesthroughout China, including sites in 21 of the 23 provinces and 4 out of 5 autonomous
Eisenberg et al. Page 12
Fitoterapia. Author manuscript; available in PMC 2012 January 1.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

regions. The provinces of Shaanxi and Hebei had the most collection sites (see Fig. 5 forsummary of site collections).
6.3. Heavy metal and pesticides screeningA total of 334 samples representing 126 species were tested for five heavy metals. Of those,294 samples representing 112 species were also tested for 162 pesticide residues.
A full discussion of the patterns of heavy metal and pesticide content and the differentmethods for interpreting the clinical significance of these observations is beyond the scopeof this manuscript and will be reported separately [38].
6.4. Quality assurance resultsA total of 382 samples representing 142 species were tested for quality according tostandards in the CP [31]. Of those, a total of 54 samples, or 14%, failed one or more of thequality assessment tests (see Tables 1 and 2). The most common reason for samples failingwas due to the quantitative tests of chemical content. A total of 29 samples, representing 8%of the total, did not meet CP standards for chemical content. In those cases, a new samplewas collected or the standard in the CP was re-assessed. Under certain circumstances, if ourTCM experts reached a consensus that the existing CP standard was unrealistic and in needof revision, the sample was provisionally accepted. For example, in some cases, it wasknown that the CP was being changed for the 2010 edition. In these instances, a writtenjustification was provided and assessed by experts at multiple universities of TCM in China.The next most common reason that samples failed was a result of tests of water or ashcontent, with roughly 5% of samples failing each. Samples that failed water or ash contentwere re-processed by drying the sample or re-cleaning it and tested again until they met theCP standard.
6.5. Shipment experienceIn general, all shipments for the project went smoothly, possibly due to the fact thatendangered or otherwise questionable species were not included in the project. For example,costus root (Saussurea costus (Falc.) Lipsch.) is listed in the CP but was excluded from theproject because it is also a species with trade restrictions. However, shipments wereregularly held in customs upon their entry in the United States and some were inspected. Inparticular, species of Chinese medicine that are related to either important agriculturalspecies or potential weeds were inspected. For example, plants in the Citrus family(Rutaceae) like Chen Pi (Citrus reticulata Blanco) and Zhi Qiao (Citrus aurantium L.) wereexamined before they entered the United States presumably to protect the U.S. citrusindustry.
6.6. Reproducibility of extraction processSee Fig. 6 for evidence of reproducibility of the extraction protocol as applied to a single 2kg shipment of authenticated TCM plant materials. Extracts made on two separate dates arecharacterized by comparable HPLC tracings.
6.7. Initial high-throughput screening targetsSee Appendix F for a listing of initial screening targets applied to preliminary evaluation ofthe 3709 TCM fractions from 82 authenticated TCM species.
Eisenberg et al. Page 13
Fitoterapia. Author manuscript; available in PMC 2012 January 1.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

6.8. Examples of selected initial screens as “proof of principle:” cytotoxicity screens andzebra fish assays
Six human cell lines were initially screened against 1686 library fractions to identify thosefractions that induced cell death and/or inhibited cell proliferation. We identified 6 fractions(out of 1686) that preferentially affected the human fibroblast cell line BJ and a number offractions that showed specificity for each of the other cell lines. Of note, we found severalfractions that affected both prostate cancer and breast cancer cell lines. All fractions wereretested, and identification of the active compounds is on-going.
Fractions were also screened for their efficacy in blocking angiogenesis using a wholeorganism, zebra fish embryo assay. Of fractions screened thus far only a small numbershowed impaired angiogenesis with few other defects. Of these, one specific fraction fromthe plant Stellaria dichotoma var. lanceolata Bge. showed the most striking anti-angiogeniceffects (see Fig. 7).
A more detailed evaluation of the qualitative changes that this fraction had on blood vesseldevelopment in the zebra fish involved a transgenic line which expresses green fluorescentprotein specifically in the endothelial cells of blood vessels. We observed that the dorsalartery and posterior cardinal vein develop normally when exposed to the extract, indicatingthat vasculogenesis was not adversely affected. However, the angiogenic process wherebyintersegmental vessels grow dorsally from these two major vessels was inhibited. As shownin Fig. 7, at 72 h post-fertilization, many intersegmental vessels were either absent, stuntedin growth, thin or occasionally misguided compared to untreated controls. The only otherobvious gross phenotypic abnormality which was observed following treatment with thisfraction was pericardial edema, which is visible by 48 h post fertilization. Pericardial edemais commonly seen in a wide range of cardiovascular developmental abnormalities, includingangiogenesis defects.
LC/MS and NMR analyses showed that the fraction contained a relatively pure majorchemical entity, which was identified as Dihydroferulic acid. Reference material (Sigma)when tested in the zebra fish assay showed the previously observed vascular phenotype atconcentrations above 50 μM. A series of chemically related compounds was tested in anattempt to obtain a structure activity relationship (see Fig. 8). Of all structurally relatedcompounds tested, the most active was cinnamaldehyde, which impaired angiogenesis atconcentrations above 0.1 μM. Notably, the most active compounds were known to beagonists of TRP channels. To explore the relationship further, Dihydroferulic acid wastested in a TRP channel assay and found to be active at concentrations above 50 μM. Wealso tested other known agonists of TRP channels and found them to be active in the zebrafish assay. Unfortunately, further experiments to confirm the identity of the target of thezebra fish fraction have not given definitive results to date.
Interestingly the TCM literature suggests that the plant containing this fraction, S.dichotoma, is effective in treating disorders of the blood. Western scientific literature furthersuggests that the active component from S. dichotoma, Dihydroferulic acid, is effective inblocking endothelial cell growth while cinnamaldehyde has been shown to be active inblocking angiogenesis.
7. DiscussionThis manuscript summarizes our rationale for the development of a library of authenticatedmedicinal plants, methods used, the status of this library and preliminary research conductedto date. The discussion will be limited to lessons learned based on the work completed thusfar, followed by a preliminary list of researchable hypotheses and proposed next steps.
Eisenberg et al. Page 14
Fitoterapia. Author manuscript; available in PMC 2012 January 1.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

Importantly, through the present collaborative study, US and Chinese co-investigators havejointly proposed and implemented a potentially reproducible strategy to identify, collect,authenticate, quality control, extract and pre-fractionate medicinal (TCM) plant species forthe purpose of systematic biological, i.e. pre-clinical, evaluation using state of the sciencedrug discovery technologies. While expensive and complex, this methodological approachhas the potential to address many of the criticisms aimed at previous investigationsinvolving herbal (natural) products and sets the stage for future pre-clinical researchinvestigations involving medicinal plants.
US and Chinese co-investigators with expertise in (TCM), botany, chemistry and drugdiscovery, have jointly established a prototype library consisting of 202 authenticatedmedicinal herbal and fungal species that collectively represent the therapeutic content of themajority of all commonly prescribed TCM herbal prescriptions. Currently housed at HMS,the library consists of duplicate or triplicate kilogram quantities of each authenticated andprocessed species, as well as “detanninized” extracts and sub-fractions of each motherextract. Importantly, each species has been collected at two or three unique sites, eachseparated geographically by hundreds of miles, with precise GPS documentation of eachcollection location as well as information about the seed origins of plant. Each of the plantsamples has been authenticated visually and chemically prior to testing for contamination byheavy metals and/or pesticides. An explicit decision process has been developed wherebysamples of each species with the least contamination were selected to undergo ethanolextraction and reproducible HPLC sub-fractionation procedures in preparation for highthroughput screening across a broad array of biological targets including, but not limited to,targets relating to cancer biology. (See Appendix G for a graphic summary of methods usedto develop this prototype library).
In the process of developing this prototype TCM library, we tested all collected specimensfor their heavy metal and/or pesticide content. A detailed summary of these findings andtheir clinical significance is beyond the scope of this article and is being reported in aseparate manuscript [38].
Preliminary biological screening of this library has led to the following observations. Wehave been able to document evidence of biological activity in a variety of screens rangingfrom standard cell based growth assays to screens involving whole animals (i.e. zebra fish).As anticipated, the fractionation process has resulted in many fractions that are dominatedby single compounds and this has greatly facilitated the process of identifying activecomponents in a given screen. The finding that TRP channel agonists may alter angiogenesisis provocative but has yet to be reduced to a molecular mechanism. Indeed, the cellulartargets are still unknown as we might have obtained the observed effects by stimulatingchannels on the endothelial cells or some other cell type that plays a role in angiogenesis.
Given that the work presented here only includes preliminary screens and compoundcharacterization, a number of testable hypotheses remain unanswered. First, is the questionof how this library, developed according to a systematic protocol differs from comparablelibraries consisting of TCM plant species, extracts and fractions elsewhere. As examples, atleast five such collections of research TCM extracts are known to exist throughout East Asiaand these include the: (1) TCM natural product library at the Dalian Institute of Chemical,Physics, Chinese Academy of Sciences; (2) Kunming Institute of Botany, the ChineseAcademy of Sciences; (3) Beijing Tong Ren Tang Chinese Medicine Co. Ltd.; (4) ShanghaiInstitute of Materia Medica; and (5) Sun Ten Pharmaceuticals Co. Ltd. and Sun TenPhytotech in Taiwan. While several of these collections include a minority of samples whichwere individually grown and/or collected by the named entity mentioned earlier, themajority of plant samples in these extract collections were purchased on the open market
Eisenberg et al. Page 15
Fitoterapia. Author manuscript; available in PMC 2012 January 1.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

and almost certainly came from multiple collection sites (i.e. numerous farms and/or wildsites) with uncertain (and heterogeneous) collection and processing procedures. As such,these other established TCM library collections are less stringent with regard to qualityassurance and the potential for reproducibility as compared with the present library.
As noted in the Introduction, any study of botanical medicines must adhere to strict andrepeatable methods for ensuring the quality of the botanical product. It has been welldocumented that the bioactive ingredients of plant-based medicines vary in ways that havepharmacological consequences [42–44]. This variation can exist within a single populationof one named species [45]. Furthermore, plant chemistry is known to vary according tomany factors, including ontogeny [46], geography [47,48], and season [49,50], even withinthe same genetic individual. Consequently, one plant-based medicine may consist ofmultiple genotypes, even within one species. Each genotype may consist of multiplechemotypes, depending on the place where they live and the time of collection. Efforts torigorously test the biological activity of plant-based medicines and reliably producestandardized plant extracts for clinical use must account for the combined possibility ofgenetic and chemical variability within a single botanical medicine [51]. Therefore, it is ofthe utmost importance to ensure that the botanical provenance and details of the collectionand processing are recorded in detail and to the maximal extent possible. Every step in thecreation of this prototype library, from collection to extraction and fractionation has beenstored in a database created specifically for this project (i.e. the TM-CTS) [39]. While thesesteps maximize the prospect of demonstrating reproducibility of biological effects fromcompounds derived from specific plant collections, explicit proof of reproducibility remainsanother critically important next step.
The larger question, of course, is whether the effort and expense required to create such alibrary of authenticated medicinal plants will result in scientific discoveries that justify theinvestment. Some would argue that this investment, while risky, is justifiable and essentialto the comprehensive and authoritative assessment of commonly used medicinal plantsworldwide. In their important review of this subject, Schmidt and colleagues [52] remind usthat most medical systems developed prior to the 20th Century relied almost exclusively onmulticomponent medicines obtained from natural sources. Today, however, the modernpharmaceutical industry relies almost exclusively on single-ingredient drugs, typicallyreferred to as new chemical entities (NCE’s). However, the rate of NCE discovery hasslowed in recent decades [53,54]. In addition more diseases are being treated withcombinations of single-component drugs. These combination therapies are designed to lowerthe incidence of resistance or target several pathological processes simultaneously. They areparticularly important in treating infectious diseases such as HIV [28], tuberculosis [55],malaria [56] and complex chronic diseases like cancer [57] and metabolic syndrome [58].
By contrast, traditional herbal medicinal systems, including those of China, India, Africa,the Asian Pacific and Hawaii classically relied on complex mixtures of plants to treatcommon symptoms and diseases. Schmidt et al. contend that traditional medicinal use ofmulticomponent botanicals may be better suited to prevent or control complex multi-factorial diseases as compared with the efficacy of single active ingredient pharmaceuticals[52]. This conceptual model inextricably leads to a testable hypothesis, namely, thatmulticomponent botanical therapies (MCBTs), if standardized using unequivocal botanicalidentification techniques and quality assurance methods, can be shown to contain individualchemical compounds which, when combined in specific ratios, result in predictable additiveand/or synergistic biological effects capable of altering the natural course of establisheddisease. How then might we get from our current state of knowledge to a confirmation orrejection of this testable hypothesis?
Eisenberg et al. Page 16
Fitoterapia. Author manuscript; available in PMC 2012 January 1.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

The specific methods detailed in this manuscript, which can be used to expand the entirelibrary of TCM medicinal plants or, alternatively, to build new parallel libraries of medicinalplants from other cultures and continents (e.g., those of India, Africa, the Mideast, Hawaii,etc.) begin to address issues pertaining to standardization and quality control of MCBTs.The next logical challenge is to use such potentially reproducible libraries to produceevidence of: (1) novel single compounds (i.e. NCE’s) with demonstrable provocativebiological effects; or, (2) single compounds which are already known but which can beshown through HTS screening to possess here-to-fore unknown biological properties; or (3)evidence of entirely novel biological mechanisms; and (4) evidence that single compoundsof interest, from this library (aka, “singletons”), when paired with one or more additionalcompounds from the same plant, a different plant in a MCBT (as is the case in mosttraditionally used herbal formulas and “patent medicines”) or hypothetically, in combinationwith a small molecule which has already been recognized as an FDA approved drug, willresult in additive or synergistic effects. Such combination studies could readily be performedunder automated HTS conditions using well-established techniques for combination-basedscreening based on the combination index methodology originally established by Chou andTalalay [59].
The present library sets the stage for these subsequent investigations. Initial screening of the3709 fractions from 80 authenticated TCM plant species has resulted in a spectrum of leads,the majority of which remain in early stages of investigation for their reproducibility,relative potency, pharmacokinetics, safety and therapeutic potential as prospective singlecompound drug candidates. While we remain intrigued by the potential of combinatorialstudies, due to funding challenges, we have yet to initiate combinatorial studies to explorethe existence of additivity or synergy of biological effects involving lead candidatecompounds within the TCM library and/or with FDA approved small drug molecules.
Several implications of this ongoing work are noteworthy. First, the successful academicpartnerships between US and Chinese institutions and co-investigators have resulted in aseries of agreements which are consistent with the Convention on Biological Diversity [60]and demonstrate the willingness of multiple international stakeholder groups to collaborateacross professional disciplines and international boundaries. These agreements and workingrelationships properly acknowledge the indigenous and traditional medical knowledge of ourTCM co-investigators and their home country, China. Indeed, the ethnobotanical expertiseof our Chinese colleagues has been a prerequisite to the implementation of this prototypelibrary, and will be essential for the continued, targeted scientific evaluation of this libraryover the coming years. Future investigations of medicinal plants in other countries maychoose to refine this collaborative strategy for use in their respective international settings.
Second, in spite of the fact that there has been a relative decline in natural product-baseddrug discovery by most major pharmaceutical companies, the history of modern drugdiscovery and the relatively high proportion of FDA approved prescription drugs derivedfrom plants. “....begs the question of whether plant (based compounds), secondarymetabolites and related synthetic compounds perform better as drugs than randomlysynthesized compounds [52].” For this reason, we plan to continue investigations of thisprototype library in search of compounds and/or combinations of compounds withtherapeutic potential.
Third, while the therapeutic value of MCBT’s has not, as of yet, been firmly established, animportant hypothetical adjunct favoring them is that they have the potential “…to providecombination therapies which can simultaneously target various elements of human diseases,providing efficacy and safety unmatched by NCE’s.” This multi-targeted “birdshot”
Eisenberg et al. Page 17
Fitoterapia. Author manuscript; available in PMC 2012 January 1.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

approach may provide a viable alternative to the “silver bullet” NCE approach betterdesigned to work with one symptom or pathogen at a time [52].
There is also the undeniable realization that generations of traditional herbal practitionerswho serve as repositories of millennia of empirical ethnobotanical knowledge are thinning innumbers. Unless reproducible research strategies are soon established to promote thoughtful,culturally sensitive and scientifically authoritative evaluation of herbal medicine systems,and evidence of their value, we may witness a decline in the number of well-educatedtrainees interested in maintaining these ethnomedical traditions worldwide. As a result, wemay diminish opportunities for scientific discovery and the perpetuation of ethnobotanicalstudy as a direct result of our failed collective stewardship of this shared global heritage.
The challenge to “form a firmly united front” [1] by engaging experts in both traditional andmodern medicine is still timely today. The difference is that we now have far more powerfultechnologies to illuminate our shared path towards this goal.
Only time will tell if the methods proposed here to establish a testable library ofauthenticated, commonly used medicinal plants will result in the discovery of newknowledge and the advent of novel therapeutic options. We will continue screening theexisting library as resources allow. It is encouraging that the NIH and NCCAM have listed“Research on Complementary and Alternative Medicine pharmacologic interventions,”which presumably includes TCM and other herbal therapies, as a prioritized strategicobjective for the next five years of NIH funding [61]. It is hoped that this prototype TCMlibrary as well as other natural product repositories with similar features, will enhanceongoing efforts to systematically evaluate commonly used herbal therapies worldwide.
An anonymous Chinese proverb says: “The methods used by one may be faulty. Themethods used by many will be better.”
Supplementary materials related to this article can be found online at doi:10.1016/j.fitote.2010.11.017.
Supplementary MaterialRefer to Web version on PubMed Central for supplementary material.
AcknowledgmentsThis work was supported in part by grants from the National Institutes of Health National Cancer Institute (U19CA128534), the National Center for Complementary and Alternative Medicine (AT03002 PIRC), the BernardOsher Foundation, and Hope Funds for Cancer Research.
INBio (Instituto Nacional de Biodiversidad) performed the chemical extraction and fractionation of all of thesamples for the project.
NSF International Center for Applied Research, Ann Arbor, Michigan performed the heavy metal and pesticideanalyses.
The sponsors were not involved in the collection, management, analysis or interpretation of the data.
References1. Zedong, M. Mao Zedong’s Manuscripts since the Funding of People’s Republic of China. Beijing,
China: The Central Literature Publishing House; 1991.2. Harvey AL. Natural products in drug discovery. Drug Discov Today 2008;13:894–901. [PubMed:
18691670]
Eisenberg et al. Page 18
Fitoterapia. Author manuscript; available in PMC 2012 January 1.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

3. Newman DJ, Cragg GM, Snader KM. The influence of natural products upon drug discovery. NatProd Rep 2000;17:215–34. [PubMed: 10888010]
4. Cragg GM, Boyd MR, Cardellina JH, Newman DJ, Snader KM, McCloud TG, et al. Ethnobotanyand drug discovery: the experience of the US National Cancer Institute. Ciba Found Symp1994;185:178–90. [PubMed: 7736854]
5. Eisenberg DM, Kessler RC, Foster C, Norlock FE, Calkins DR, Delbanco TL. Unconventionalmedicine in the United States. Prevalence, costs, and patterns of use. N Engl J Med 1993;328:246–52. [PubMed: 8418405]
6. Eisenberg DM, Davis RB, Ettner SL, et al. Trends in alternative medicine use in the United States,1990–1997: results of a follow-up national survey. JAMA 1998;280:1569–75. [PubMed: 9820257]
7. Kaufman DW, Kelly JP, Rosenberg L, Anderson TE, Mitchell AA. Recent patterns of medicationuse in the ambulatory adult population of the United States: the Slone survey. JAMA2002;287:337–44. [PubMed: 11790213]
8. Barnes PM, Adams PF, Schiller JS. Summary health statistics for the U.S. population: NationalHealth Interview Survey, 2001. Vital Health Stat 2003;10:1–82.
9. Barnes PM, Bloom B, Nahin RL. Complementary and alternative medicine use among adults andchildren: United States. Natl Health Stat Report 2007;2008:1–23.
10. Nahin RL, Barnes PM, Stussman BJ, Bloom B. Costs of complementary and alternative medicine(CAM) and frequency of visits to CAM practitioners: United States. Natl Health Stat Report2007;2009:1–14.
11. Li, B.; Wu, S.; Lui, C. China pharmaceuticals: investing in Traditional Chinese Medicine (TCM).Hong Kong: 2009.
12. National Center for Complementary and Alternative Medicine (NCCAM) Centers for Research onComplementary and Alternative Medicine (CRC) Program. CY 2003 Research Priorities. Apriority to elucidate mechanisms of action and conduct small, well-developed phase I and II trials.Dec 22002 [Accessed September 19, Accessed 2010]. athttp://web.archive.org/web/20021225053952/http://nccam.nih.gov/research/priorities/indexhtm#2
13. Oh WK, Kantoff PW, Weinberg V, et al. Prospective, multicenter, randomized phase II trial of theherbal supplement, PC-SPES, and diethylstilbestrol in patients with androgen-independent prostatecancer. J Clin Oncol 2004;22:3705–12. [PubMed: 15289492]
14. Wolsko PM, Solondz DK, Phillips RS, Schachter SC, Eisenberg DM. Lack of herbal supplementcharacterization in published randomized controlled trials. Am J Med 2005;118:1087–93.[PubMed: 16194636]
15. Turner RB, Bauer R, Woelkart K, Hulsey TC, Gangemi JD. An evaluation of Echinaceaangustifolia in experimental rhinovirus infections. N Engl J Med 2005;353:341–8. [PubMed:16049208]
16. Blumenthal M, Farnsworth NR. Echinacea angustifolia in rhinovirus infections. N Engl J Med2005;353:1971–2. author reply -2. [PubMed: 16267331]
17. Bent S, Kane C, Shinohara K, et al. Saw palmetto for benign prostatic hyperplasia. N Engl J Med2006;354:557–66. [PubMed: 16467543]
18. DiPaola RS, Morton RA. Proven and unproven therapy for benign prostatic hyperplasia. N Engl JMed 2006;354:632–4. [PubMed: 16467551]
19. NCCAM Policy: Natural Product Integrity. [Accessed 10/6/10]. athttp://nccam.nih.gov/research/policies/naturalproduct.htm
20. Schulz KF, Altman DG, Moher D. CONSORT 2010 statement: updated guidelines for reportingparallel group randomized trials. Ann Intern Med 2010;152:726–32. [PubMed: 20335313]
21. Holzbeieriein J. Hsp90: a drug target? Curr Oncol Rep 2010;12:95–101. [PubMed: 20425593]22. Richardson P. Tanespimycin monotherapy in relapsed multiple myeloma: results of a phase 1
dose–escalation study. Br J Haematol 2010;150:438–45. [PubMed: 20618337]23. Suffness M, Douros J. Current status of the NCI plant and animal product program. J Nat Prod
1982;45:1–14. [PubMed: 7069421]24. Verpoorte R. Pharmacognosy in the new millennium: leadfinding and biotechnology. J Pharm
Pharmacol 2000;52:253–62. [PubMed: 10757412]
Eisenberg et al. Page 19
Fitoterapia. Author manuscript; available in PMC 2012 January 1.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

25. Fabricant DS, Farnsworth NR. The value of plants used in traditional medicine for drug discovery.Environ Health Perspect 2001;109(Suppl 1):69–75. [PubMed: 11250806]
26. Bensky, D.; Clavey, S.; Stoger, E.; Gamble, A. Chinese Herbal Medicine: Materia Medica. Seattle:Eastland Press; 2004.
27. Scheid, V.; Bensky, D.; Ellis, A.; Barolet, R. Chinese herbal medicine: Formulas and strategies. 2.Seattle: Eastland Press; 2009.
28. Agrawal L, Lu X, Jin Q, Alkhatib G. Anti-HIV therapy: current and future directions. Curr PharmDes 2006;12:2031–55. [PubMed: 16787246]
29. Borisy AA, Elliott PJ, Hurst NW, Lee MS, Lehar J, Price ER, Serbedzija G, Zimmermann GR,Foley MA, Stockwell BR, Keith CT. Systematic discovery of multicomponent therapeutics. PNAS2003;100:7977–82. [PubMed: 12799470]
30. Wagner H, Ulrich-Merzenich G. Synergy research: approaching a new generation ofphytopharmaceuticals. Phytomedicine 2009;16:97–110. [PubMed: 19211237]
31. Chinese Pharmacopoeia Commission. Pharmacopoeia of the People’s Republic of China. Beijing:People’s Medical Publishing House; 2005.
32. Larsen HO, Olsen CS. Unsustainable Collection and Unfair Trade? Uncovering and AssessingAssumptions Regarding Central Himalayan Medicinal Plant Conservation. Biodiversity andConservation 2007;16(6):1679–1697.
33. Convention on International Trade in Endangered Species of Wild Flora and Fauna and Flora(CITES) Appendices I, II and III. [Accessed September 19, 2010]. athttp://www.cites.org/eng/app/appendices.shtml
34. Hildreth J, Hrabeta-Robinson E, Applequist W, Betz J, Miller J. Standard operating procedure forthe collection and preparation of voucher plant specimens for use in the nutraceutical industry.Anal Bioanal Chem 2007;389:13–7. [PubMed: 17572883]
35. Zhao ZZ, Xiao PG, Xiao Y, Yuen JPS. Quality assurance of Chinese Herbal Medicines (CHMs). JFood Drug Anal 2007;15:337–46.
36. NSF International Standard/American National Standard. #173 for Dietary Supplements. AnnArbor: NSF International; 2008.
37. World Health Organization. Operational Guidance: Information needed to support clinical trials ofherbal products UNICEF/UNDP/World Bank/WHO Special Programme for Research andTraining in Tropical Diseases (TDR). 2005.
38. Harris, ESJ.; Woolf, AD.; Eisenberg, DM., et al. Heavy Metal and Pesticide Content in CommonlyPrescribed Individual Raw Chinese Herbal Medicines. In Preparation
39. Harris, ESJ.; Erickson, SD.; Tolopko, AN.; Cao, SG.; Craycroft, JA.; Scholten, R.; Fu, YL.; Wang,WQ.; Liu, Y.; Zhao, ZZ.; Clardy, J.; Shamu, C.; Eisenberg, DM. Traditional Medicine CollectionTracking System (TM-CTS): A Database for Ethnobotanically-Driven Drug-Discovery Programs.In Review
40. Firestein R, Bass AJ, Kim SY, Dunn IF, Silver SJ, Guney I, et al. CDK8 is a colorectal canceroncogene that regulates B-catenin activity. Nature 2008;455:547–51. [PubMed: 18794900]
41. Wu, ZY.; Raven, PH. Flora of China, Multiple Volumes. St. Louis: Missouri Botanical GardenPress; 1994.
42. Delabays N, Simonnet X, Gaudin M. The genetics of artemisinin content in Artemisia annua L andthe breeding of high yielding cultivars. Curr Med Chem 2001;8:1795–801. [PubMed: 11772351]
43. Goodger JQD, Whincup AL, Field AR, Holtum JAM, Woodrow IE. Variation in huperzine A andB in Australasian Huperzia species. Biochem Syst Ecol 2008;36:612–8.
44. Viljoen AM, Subramoney S, van Vuuren SF, Baser KH, Demirci B. The composition,geographical variation and antimicrobial activity of Lippia javanica (Verbenaceae) leaf essentialoils. J Ethnopharmacol 2005;96:271–7. [PubMed: 15588679]
45. Hong DY, Lau AJ, Yeo CL, et al. Genetic diversity and variation of saponin contents in Panaxnotoginseng roots from a single farm. J Agric Food Chem 2005;53:8460–7. [PubMed: 16248538]
46. Rehill BJ, Whitham TG, Martinsen GD, Schweitzer JA, Baily JK, Lindroth RL. Developmentaltrajectories in cottonwood phytochemistry. J Chem Ecol 2006;32:2269–85. [PubMed: 17001533]
Eisenberg et al. Page 20
Fitoterapia. Author manuscript; available in PMC 2012 January 1.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

47. Han T, Hu Y, Zhou SY, Li HL, Zhang QY, Zhang H, Huang BK, Rahman K, Zheng HC, Qin LP.Correlation between the genetic diversity and variation of total phenolic acids contents in FructusXanthii from different populations in China. Biomed Chromatogr 2008;22:478–86. [PubMed:18205144]
48. Su S, He CM, Li LC, Chen JK, Zhou TS. Genetic characterization and phytochemical analysis ofwild and cultivated populations of Scutellaria baicalensis. Chem Biodivers 2008;5:1353–63.[PubMed: 18651621]
49. Dong TT, Cui XM, Song ZH, et al. Chemical assessment of roots of Panax notoginseng in China:regional and seasonal variations in its active constituents. J Agric Food Chem 2003;51:4617–23.[PubMed: 14705886]
50. Ma XQ, Shi Q, Duan JA, Dong TT, Tsim KW. Chemical analysis of Radix Astragali (Huangqi) inChina: a comparison with its adulterants and seasonal variations. J Agric Food Chem2002;50:4861–6. [PubMed: 12166972]
51. Ribnicky DM, Poulev A, Schmidt B, Cefalu WT, Raskin I. Evaluation of botanicals for improvinghuman health. Am J Clin Nutr 2008;87:472S–5S. [PubMed: 18258641]
52. Schmidt BM, Ribnicky DM, Lipsky PE, Raskin I. Revisiting the ancient concept of botanicaltherapeutics. Nat Chem Biol 2007;3:360–6. [PubMed: 17576417]
53. Butler MS. The role of natural product chemistry in drug discovery. J Nat Prod 2004;67:2141–53.[PubMed: 15620274]
54. Sams-Dodd F. Drug discovery: selecting the optimal approach. Drug Discov Today 2006;11:465–72. [PubMed: 16635811]
55. Blomberg B, Fourie B. Fixed-dose combination drugs for tuberculosis: application in standardisedtreatment regimens. Drugs 2003;63:535–53. [PubMed: 12656652]
56. Schellenberg D, Abdulla S, Roper C. Current issues for anti-malarial drugs to control P.falciparum malaria. Curr Mol Med 2006;6:253–60. [PubMed: 16515515]
57. Waterhouse DN, Gelmon KA, Klasa R, et al. Development and assessment of conventional andtargeted drug combinations for use in the treatment of aggressive breast cancers. Curr Cancer DrugTargets 2006;6:455–89. [PubMed: 17017873]
58. Deedwania PC, Volkova N. Current treatment options for the metabolic syndrome. Curr TreatOptions Cardiovasc Med 2005;7:61–74. [PubMed: 15913505]
59. Chou T, Talalay P. Quantitative analysis of dose–effect relationships: the combined effects ofmultiple drugs or enzyme inhibitors. Adv Enzyme Regul 1984;22:27–55. [PubMed: 6382953]
60. UNEP. Convention on Biological Diversity. United Nations Environment Programme. [AccessedSeptember 19, 2010]. at http://www.cbd.int
61. National Center for Complementary and Alternative Medicine. Accessed at http://nccam.nih.gov/
Eisenberg et al. Page 21
Fitoterapia. Author manuscript; available in PMC 2012 January 1.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

Fig. 1.Flow chart describing methods to develop a prototype authenticated Chinese medicinal plantlibrary for systematic biological evaluation.
Eisenberg et al. Page 22
Fitoterapia. Author manuscript; available in PMC 2012 January 1.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

Fig. 2.Decision Tree For Acceptance or Rejection of Plant Samples Based On ChinesePharmacopoeia Quality Assessment (QA) Tests. See also Table 1 for details of qualityassessment tests in the Chinese Pharmacopoeia.
Eisenberg et al. Page 23
Fitoterapia. Author manuscript; available in PMC 2012 January 1.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

Fig. 3.Decision Tree for Choosing One of Several Plant Samples per Species for Extraction andFractionation. Asterisk (*) indicates instances where clinical toxicological judgment may berequired. For example, if all samples are contaminated, the preference is for the least toxicsample whether that is the lowest concentration of contaminant or contaminants with lowestclinical toxicity.
Eisenberg et al. Page 24
Fitoterapia. Author manuscript; available in PMC 2012 January 1.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
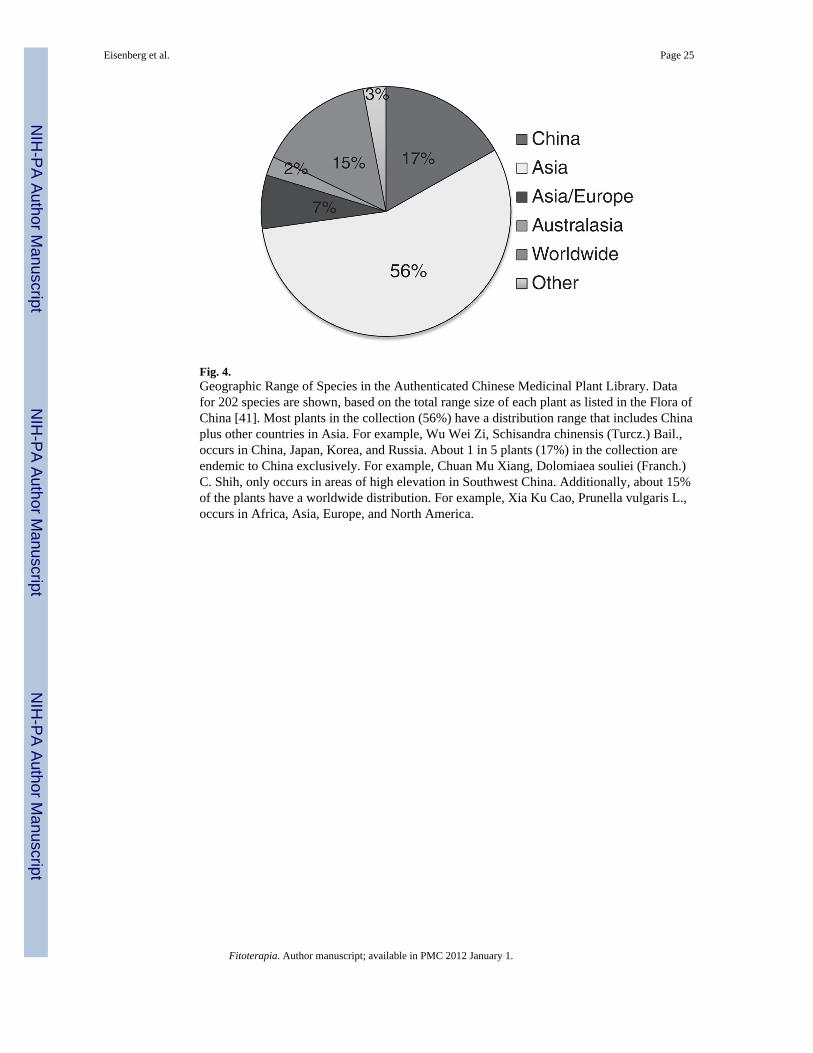
Fig. 4.Geographic Range of Species in the Authenticated Chinese Medicinal Plant Library. Datafor 202 species are shown, based on the total range size of each plant as listed in the Flora ofChina [41]. Most plants in the collection (56%) have a distribution range that includes Chinaplus other countries in Asia. For example, Wu Wei Zi, Schisandra chinensis (Turcz.) Bail.,occurs in China, Japan, Korea, and Russia. About 1 in 5 plants (17%) in the collection areendemic to China exclusively. For example, Chuan Mu Xiang, Dolomiaea souliei (Franch.)C. Shih, only occurs in areas of high elevation in Southwest China. Additionally, about 15%of the plants have a worldwide distribution. For example, Xia Ku Cao, Prunella vulgaris L.,occurs in Africa, Asia, Europe, and North America.
Eisenberg et al. Page 25
Fitoterapia. Author manuscript; available in PMC 2012 January 1.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

Fig. 5.Map of Collection Locations in the People’s Republic of China. A total of 558 samplelocations, representing 202 species, are shown. No collections were made in the provinces ofQinghai, Xizang (Tibet), or Taiwan. The highest number of collections were in Shaanxi(N=61) and Hebei provinces (N=47).
Eisenberg et al. Page 26
Fitoterapia. Author manuscript; available in PMC 2012 January 1.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

Fig. 6.Evidence of Reproducibility of Extraction Methods (BioXPlore HPLC) Involving A SingleSpecies Dried Material Extracted on Different Dates.
Eisenberg et al. Page 27
Fitoterapia. Author manuscript; available in PMC 2012 January 1.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

Fig. 7.Zebra Fish Aniti-Angiogenesis Assay - Example of Proof of Principle. (A) Zebrafishembryo at 27 hrs; (B) Normal blood vessels; (C) Higher magnification of normal vessels;(D) (E) (F) Developmental abnormalities in intersegmetal vessels due to a style plant extractfraction. DA = dorsal artery, PCV = posterior cardinal vein, ISV’s = intersegmental vessels.
Eisenberg et al. Page 28
Fitoterapia. Author manuscript; available in PMC 2012 January 1.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

Fig. 8.Testing related compounds for relative anti-angiogenesis potency.
Eisenberg et al. Page 29
Fitoterapia. Author manuscript; available in PMC 2012 January 1.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
Eisenberg et al. Page 30
Table 1
Quality assessment tests based on the Chinese Pharmacopoeia.
Test Type of test*
Character Test related to plant origin (A-2)
TLC identification Test related to plant origin (A-2)
Foam reaction identification Test related to plant origin (A-2)
Color reaction identification Test related to plant origin (A-2)
Sublimation reaction identification Test related to plant origin (A-2)
Impurity examination Test related to plant processing (A-1)
Leaf examination Test related to plant processing (A-1)
Water content examination Test related to plant processing (A-1)
Total ash content examination Test related to plant processing (A-1)
Acid-insoluble ash content examination Test related to plant processing (A-1)
Peroxide value examination Test related to plant origin (A-2)
Loss on drying examination Test related to plant processing (A-1)
Volatiles Test related to chemical content (B)
Extract Test related to chemical content (B)
Content determination Test related to chemical content (B)
*For relevance to decision tree with regard to accepting or rejecting plant samples see Fig. 2.
Fitoterapia. Author manuscript; available in PMC 2012 January 1.

NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
Eisenberg et al. Page 31
Table 2
Status of prototype library of authenticated traditional Chinese medicinal plants to date. The number ofsamples collected, authenticated, processed, and quality tested to date is shown. In addition to total number ofsamples that were processed at each stage, comments regarding authentication, quality assessment, andcontaminants are provided.
Number of samplesComments regarding quality assurancetesting
Total number TCM species planned for collection 202
Total number samples (two or three) planned for collection 582
Actual number that were collected 562
Total samples authenticated 451 7 (1.6%) failed authentication
Total samples which completed Chinese Pharmacopeia quality assessment 382 54 (14.1%) failed quality assessment
Total number samples tested for heavy metals 334*
Total number samples tested for pesticides 294*
Total number of species extracted and fractionated 80
Total number of fractions currently available for biological screening 3709
*Details about heavy metal and pesticide levels as well as their clinical implications are reported in a separate paper [38].
Fitoterapia. Author manuscript; available in PMC 2012 January 1.