Embed Size (px)
Citation preview

MOROGORO
NEWSLETTER
OOVVEERRVVIIEEWW OOFF JJOOIINNTT FFIINNAALL EEVVAALLUUAATTIIOONN
OOFF MMOORROOGGOORROO HHEEAALLTTHH PPRROOJJEECCTT
ear Readers,
Congratulations!!
After the report on the Joint Final Project
Evaluation in October 2005 the Morogoro Health
Project (MHP) has succeeded to get Japan
International Cooperation Agency (JICA) approval
for extension for one year; until March 2007.
MHP, supported by JICA, welcomed Tanzania -
Japan Joint Final Evaluation Team (headed by Ms.
Harumi Kitabayashi, JICA Headquarters, Tokyo,
Japan) to review the project progress and
achievements since the project commencement in
April 2001. Because the Project was originally
designed to end after five-year implementation in
March 2006, this is a prime time to consider the
Project future orientation.
The Evaluation Team, consisting of JICA
Headquarter independent External Consultant, Ms.
Minako Nakatani and two representatives from the
Ministry of Health, Tanzania, reviewed the project
achievements through in-depth interview and
questionnaire to the counterparts, conducting
independent on-site visits to all the districts and
through attending several important meetings, such
as “Project Final Internal Evaluation Workshop”,
“Morogoro Health Stakeholders Conference” and
“Tanzania – JICA Project Review Workshop”,
during the evaluation period from 1st to 23rd October
2005.
Finally, the Evaluation Team discussed the
Evaluation Report with high authorities from the
President’s Office Regional Administration and
Local Government, Ministry of Health, Morogoro
Regional Secretariat and District Councils in
Morogoro Region. They agreed upon optimal project
outcomes in health management development,
certain impacts on health service delivery and
utilization in Morogoro Region.
D
ISSN 0856-9525 ISSUE No.5 December 2005
Group picture of Joint Final Project Evaluation
for Morogoro Health Project

Morogoro Health Newsletter - No.5
2
The Evaluation Report concluded, “During the
Evaluation Mission, various behavioral changes
towards evidence-based management among
Regional Health Management Team (RHMT) and
Council Health Management Team (CHMT)
members were recognized. Such changes are
valuable in supporting the decentralization process
under Local Government Reform and Health Sector
Reform, and essential for ensuring the improvement
of district health services. Future efforts are
necessary by all stakeholders to consolidate such
changes in the managerial capacities of RHMT and
CHMT members, for the benefit of the Frontline
Health Workers and ultimately the health service
users of the Morogoro Region”.
In order to consolidate project outcomes in
RHMT and CHMTs and disseminate project lessons
and experiences to other regions, the Evaluation
Team recommended the Project to be extended one
more year from April 2006 to March 2007 under full
scale assistance by JICA. The project can be a model
of future managerial capacity development in health
systems in Tanzania. Tanzania and Japan should
work together harder for quality and equitable health
services in Tanzania.
MHP would like to appreciate the enduring efforts
from all our stakeholders and to admit more and
more commitment to the Project.
If you need more information on the Final
Evaluation Report, it is available in the MHP office
and Regional Medical Officer (RMO) / District
Medical Officer (DMO) s’ offices.
Thank you very much for your kind cooperation
and consideration for the Project. We have to serve
for the better future of the people in Tanzania.
Dr. T. Sugishita
Chief Advisor
Morogoro Health Project
-- IInn TThhiiss IIssssuuee --
JJooiinntt FFiinnaall EEvvaalluuaattiioonn ooff MMoorrooggoorroo HHeeaalltthh PPrroojjeecctt 11 EEddiittoorriiaall 33 CCuussttoommss aanndd TTaabbooooss HHaarrmmffuull ttoo TTeeeetthh 44 NNeeww AAnnttii--MMaallaarriiaa DDrruuggss 44 FFoooodd VVeennddoorrss KKAAPP –– RReesseeaarrcchh PPaappeerr 55 MMaannaaggiinngg tthhee EEnnvviirroonnmmeenntt TThhrroouugghh tthhee CCoommmmuunniittyy 77 HHoommee BBaasseedd CCaarree 88 OOppeerraattiioonnaall RReesseeaarrcchh MMaannaaggeemmeenntt 1100 IImmppoorrttaanntt EEvveennttss:: AAuugguusstt –– DDeecceemmbbeerr 22000055 1111 CCaarrttoooonn 1122
EDITORIAL BOARD
Chairperson:
Mr. N. Masaoe Regional Health Officer
Secretary:
Ms. C. Maro District Reproductive and Child
Health Coordinator, Morogoro
Deputy Secretary:
Ms. N. Ahmed Nursing Officer, Morogoro Municipality
Members:
Mr. J. Mankambila Regional Health Secretary
Dr. G. Mtey Municipal Medical Officer of Health, Moro.
Dr. O. Mbena District Dental Officer, Mvomero
Mr. J. Bundu District Health Officer, Kilosa
Mr. D. Dia District Health Secretary, Kilombero
Mr. W. Mkessey Ag. District Health Officer, Ulanga
Ms. M. Tsuda Advisor, MHP*
Chief Advisor:
Dr. M. Massi Regional Medical Officer
Associate Member:
Dr. F. Fupi Advisor, MHP*
Advisory Committee:
Mr. H. Mohamed Lecturer, Sokoine University of
Agriculture, Morogoro
*MHP: Morogoro Health Project, JICA

Morogoro Health Newsletter - No.5
3
MOROGORO HEALTH NEWSLETTER Dear esteemed readers,
On behalf of the Editorial Board of this
Newsletter, I welcome you to the 5th issue of this
Newsletter.
Today I would like to high-light various issues.
The general public should be aware that Malaria, the
leading public health problem, no longer responds
adequately to Sulfadoxine - Pyrimethamine (SP). A
new combination therapy is expected to be initiated
from 2006. The public is advised to wage collective
combined strategy to fight the mosquitoes which
transmit Malaria by for example: extensive use of
ITNs, destroying all mosquito breeding sites,
screening houses, seeking early treatment.
The Board commends the leadership of Central
Government and Councils in Morogoro Region for
their recognition of the Newsletter and hence putting
up budget line in their annual plans for its
publication. This spirit has impressed JICA, the
donor of the Morogoro Health Project (MHP). This
has assured firm sustainability of the Newsletter
when the donor support ends.
Nine members of the Editorial Board attended a
four-day-training on Newsletter type setting and
related computer skills, which was conducted at
Mzumbe University. The training was important in
enhancing the skills of the Board members. The
Board thanks MHP for financing the training.
A team of four external final evaluators of MHP,
Ms. Harumi Kitabayashi, Prof. Ichiro Okubo, Mr.
Ikuo Takizawa and Ms. Minako Nakatani conducted
the MHP Final Evaluation from 1st to 23rd October
2005. The Team visited all six Councils of
Morogoro Region. In the 14 health facilities visited
the team observed some health workers using the
Newsletter to disseminate health education issues to
their clients. Most of health workers interviewed
were aware of the existence of the Newsletter. This
highly impressed the Evaluation Team. The Board
commends those who read the Newsletter and share
the text with community. Others are advised to
emulate. The Evaluation Team was satisfied with
implementation of MHP. The Team’s opinion was
that the MHP objective of managerial capacity
building of the Health Management Teams in
Morogoro region has been optimally realized. The
MHP project which was to end in March 2006 has
been extended to March 2007.
The Board is further requesting all readers of this
Newsletter to send articles and suggestions for
publication. This will facilitate achieving the
objective of the Newsletter, i.e. to exchange
experience and skills among health service providers
and the community.
I take this opportunity to inform our readers that,
mid-January 2006, I shall retire from Public Service;
hence my position as Chairperson of the Editorial
Board seizes mid-December 2005. My best wishes
to the incoming Chairperson Dr. G. Mtey and assure
him of my un-swayed support and commitment to
the development of the Newsletter.
I thank the Editorial Board members and readers
for their cooperation, support and commitment
which lead to the success of the Newsletter. I wish
you all Merry X-mass and Prosperous New Year. We
shall meet if God wishes.
Mr. N. Masaoe
Chairperson
Editorial Board
Mr. N. MasaoeChairperson
Editorial Board

Morogoro Health Newsletter - No.5
4
CCUUSSTTOOMMSS AANNDD TTAABBOOOOSS HHAARRMMFFUULL TTOO TTEEEETTHH
A human tooth is among the organs of the body
that plays a role of beautify the face, protection
essentially as a weapon and also chewing food and
fruits.
Therefore maximum care has to be taken to
safeguard them from harm or damage, by seeking
treatment whenever necessary and frequent
check-up.
However in some countries, people are used to do
some traditional sculpture works on their teeth,
based on some cultural beliefs. Teeth sculpturing
became famous in most countries. Some decades
ago it conveyed various messages and meanings; e.g.
during wartimes and as a gesture of prestige,
especially among women.
Tooth extraction was also considered as a
“Medical’’ intervention to relieve outstanding pain
of some teeth. This move was however, more
psychological, and rarely as an appropriate. Teeth
decoration, in any form is doing harm to the mouth
and the teeth itself.
In the modern times, teeth decoration is no longer
useful to the Tanzanian. We have to discourage
decoration practice and even its extraction without
reasonable cause.
Some of the traditional belief and practices which
need to be discouraged are:
Tooth sculpturing and polishing. This
practice destroys the upper layer that
protects the teeth.
Extraction of front lower teeth.
Extraction of front upper teeth and piercing
of the upper lip to insert cylindrical object
(“Ndonya”), a decorative gesture by woman,
mostly older women.
Extraction of infancy teeth. This hurts the
child, and delays the growth of permanent
teeth. The rumors of ‘plastic teeth’ is mere
myths, all teeth are genuine ones.
Use of teeth to uncap bottles mostly of
beverages and soft drinks, cutting ropes,
crushing bones and lifting heavy objects.
To polish brown teeth due to e.g. fluorine.
Disadvantages of the practices are:
Difficulty and pain when the tooth gets into
contact with cold or even hot food or drinks.
Tooth decay can be easily accelerated.
A tooth becomes loose easily and can
ultimately be exfoliated.
Hence let us take all necessary measures to
observe the guidance to safeguard our teeth for
better health.
Dr. O. Mbena
DDO Mvomero
NNEEWW AANNTTII--MMAALLAARRIIAA DDRRUUGGSS
Malaria is still the most common dangerous disease
in the third world and it ranks number one in terms of
high morbidity and mortality, especially in under five
children and pregnant mothers. The Government
produced new National Guidelines for Diagnosis and
Treatment of Malaria for the aim of attaining uniform
malaria cases management in the country .The guiding
principle of Malarial drug policy is to promote safe,
effective, good quality, affordable, accessible and
acceptable Malaria treatment also encourage rational
Morogoro Health Newsletter – No.5
5
drug use in order to minimize development of drugs
resistance.
Our country changed its Malaria Treatment Policy
Guideline from Chloroquine to Sulfadoxine -
Pyrimethamine (SP) combination therapy as the first
line for drug for the treatment of acute Malaria
episodes in August 2001. However over the last 4
years resistance to SP has already been reported to be
on the increase. Recent studies (2004) in Tanzania
indicate that the mean SP treatment failure is now
25.5% and molecular markers of SP resistance have
recorded high levels of mutation. The mean treatment
failure of Amodiaquine, the 2nd line anti-Malaria is
12%. The findings indicate that a change in the
treatment guideline is necessary.
According to the risk of increasing parasites
resistance to existing mono-therapies, there is now a
global move towards use of combination therapy.
Another reason is that these drugs are more
efficacious and they may delay the spread of drug
resistance.
Recommended therapy:
• Combination therapy recommended is
ARTEMETHER / LUMEFANTRINE (ALU), it
is recommended as first line therapy.
(See Table-1)
• The second line drug where ALU has failed or is
contraindicated is Quinine.
• The drug of choice for treatment of severe
Malaria is Quinine.
• The first line drug for pregnant women and
children less than 5 kg (under two months) is
Quinine.
• SP will continue only for pregnant women as
Intermittent Presumptive Treatment (IPT). The
dose is administered between 20-24 weeks of
gestational age and second dose of IPT will be
administered at 28-32 weeks.
Administration of SP to all pregnant women will
prevent them from high risk of peripheral parasitaemia
and placental Malaria because during pregnancy
Malaria is often asymptomatic.
IPT should be administered as Direct Observed (DOT)
during an ant-natal visit.
Drug compliance is very important to prevent
incorrect administration of ALU, since ALU is not a
single dose therapy. Early diagnosis and effective case
management of Malaria is very important. Clear
instruction to the patient is necessary. All pregnant
mothers should be encouraged to use Insecticide
Treated Nets (ITNs) besides using IPT.
Reference: Malaria Control Series 10
Ms. C. Maro
DRCHCo Morogoro
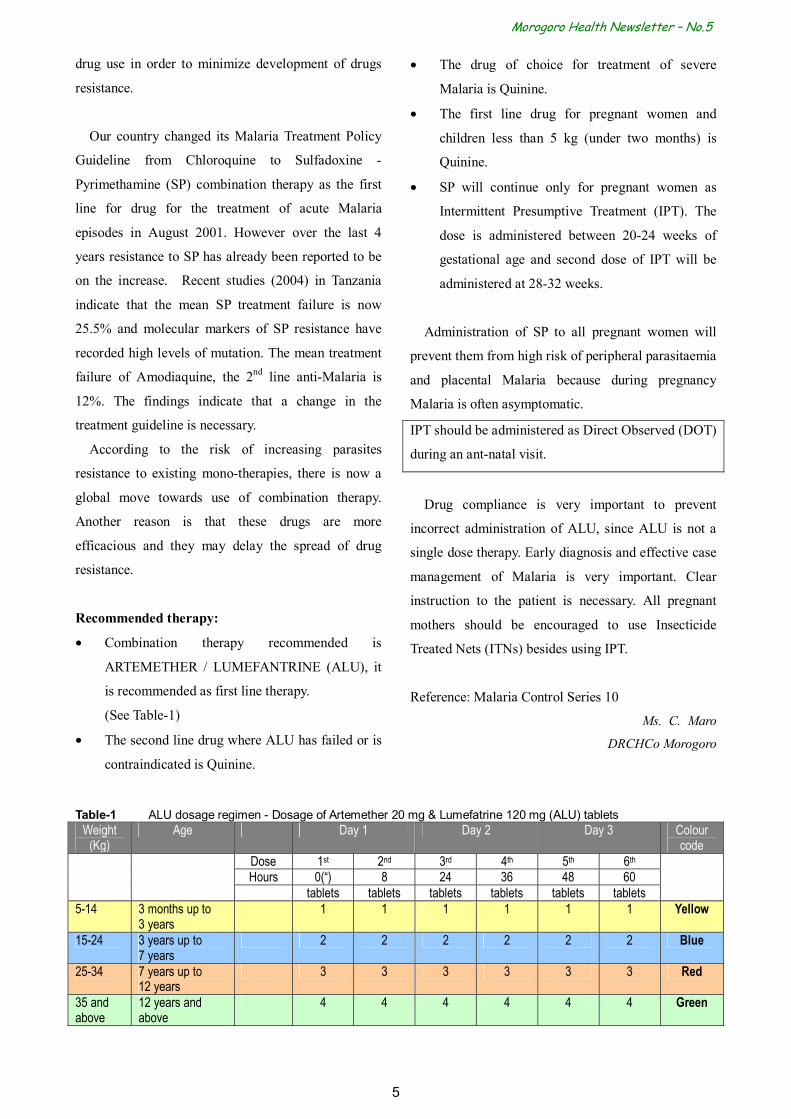
Table-1 ALU dosage regimen - Dosage of Artemether 20 mg & Lumefatrine 120 mg (ALU) tablets
Weight (Kg)
Age Day 1 Day 2 Day 3 Colour code
Dose 1st 2nd 3rd 4th 5th 6th Hours 0(“) 8 24 36 48 60 tablets tablets tablets tablets tablets tablets 5-14 3 months up to
3 years 1 1 1 1 1 1 Yellow
15-24 3 years up to 7 years
2 2 2 2 2 2 Blue
25-34 7 years up to 12 years
3 3 3 3 3 3 Red
35 and above
12 years and above
4 4 4 4 4 4 Green
Morogoro Health Newsletter - No.5
6
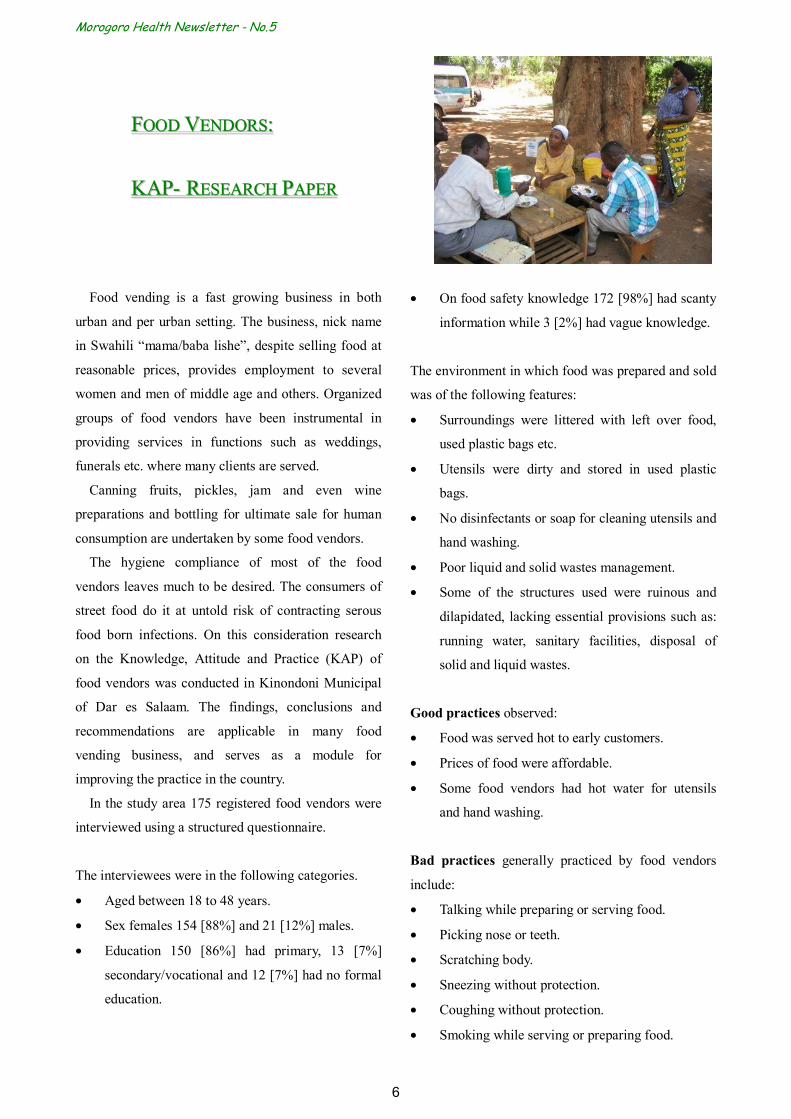
FFOOOODD VVEENNDDOORRSS:: KKAAPP-- RREESSEEAARRCCHH PPAAPPEERR
Food vending is a fast growing business in both
urban and per urban setting. The business, nick name
in Swahili “mama/baba lishe”, despite selling food at
reasonable prices, provides employment to several
women and men of middle age and others. Organized
groups of food vendors have been instrumental in
providing services in functions such as weddings,
funerals etc. where many clients are served.
Canning fruits, pickles, jam and even wine
preparations and bottling for ultimate sale for human
consumption are undertaken by some food vendors.
The hygiene compliance of most of the food
vendors leaves much to be desired. The consumers of
street food do it at untold risk of contracting serous
food born infections. On this consideration research
on the Knowledge, Attitude and Practice (KAP) of
food vendors was conducted in Kinondoni Municipal
of Dar es Salaam. The findings, conclusions and
recommendations are applicable in many food
vending business, and serves as a module for
improving the practice in the country.
In the study area 175 registered food vendors were
interviewed using a structured questionnaire.
The interviewees were in the following categories.
• Aged between 18 to 48 years.
• Sex females 154 [88%] and 21 [12%] males.
• Education 150 [86%] had primary, 13 [7%]
secondary/vocational and 12 [7%] had no formal
education.
• On food safety knowledge 172 [98%] had scanty
information while 3 [2%] had vague knowledge.
The environment in which food was prepared and sold
was of the following features:
• Surroundings were littered with left over food,
used plastic bags etc.
• Utensils were dirty and stored in used plastic
bags.
• No disinfectants or soap for cleaning utensils and
hand washing.
• Poor liquid and solid wastes management.
• Some of the structures used were ruinous and
dilapidated, lacking essential provisions such as:
running water, sanitary facilities, disposal of
solid and liquid wastes.
Good practices observed:
• Food was served hot to early customers.
• Prices of food were affordable.
• Some food vendors had hot water for utensils
and hand washing.
Bad practices generally practiced by food vendors
include:
• Talking while preparing or serving food.
• Picking nose or teeth.
• Scratching body.
• Sneezing without protection.
• Coughing without protection.
• Smoking while serving or preparing food.
Morogoro Health Newsletter – No.5
7
• Irregular or no medical examinations etc.
• Absence of uniforms and or protective gear.
Conclusion and Recommendations:
Food vending is a fast growing industry. The
conducts of operations require regular monitoring and
continuous orientations on good preparation practices.
The following is recommended to the responsible
authorities.
• Identification, registration and certification of all
food vendors.
• Prepare and institute, in consultation with food
vendors, minimum standards and regulations.
• Ensure and institute regular medical examination
of every food vendor.
• Organize regular and frequent health education
sessions on food safety. Such trainings can be
financed trough the Comprehensive Council
Health Plans.
• Assist them to acquire loans to facilitate
improving their business.
• Recognize their leadership and plan with them
regular meetings and dialogue.
• Ensure that all food vendors have clean uniforms
and protective gear all the time.
• Keep young children/infants away from business
premises.
Ms. L. F. Temu
HO [Internship]
Morogoro Regional Hospital
MMAANNAAGGIINNGG TTHHEE EENNVVIIRROONNMMEENNTT TTHHRROOUUGGHH TTHHEE CCOOMMMMUUNNIITTYY
IINN MMOORROOGGOORROO MMUUNNIICCIIPPAALLIITTYY
Morogoro Municipal is one of the Municipalities
with an attractive environment and scenery of the
Uluguru Mountains, many rivers and numerous
streams. However, this is systematically deteriorating
due to reasons hereunder.
• The majority of residents do not value
cleanliness. They rarely participate in activities
geared to keep the Municipal clean.
• Liquid and solid wastes flow and accumulate in
the residential areas unabated.
• Some residential buildings do not have;
o Acceptable sanitary facilities (latrines)
o Proper soakage pits for waste water disposal
o Proper washing slabs
o Receptacles for storage of domestic wastes
• Used plastics containers and bags litter the entire
Municipal.
• Some occupiers keep livestock in high density
areas, causing unwanted irritation and nuisance
to neighbors.
Morogoro Municipal has three times ranked the 12th
out of the 13 Municipalities in Tanzania mainland in
the Environmental Sanitation Competitions organized
by the Ministry of Health due to the aforementioned
reasons and other factors such as dilapidated public
abattoirs, an unfenced public cemetery, the presence
of an old and poorly rehabilitated main market, poorly
rehabilitated unpaved roads with poor storm water
drains and the presence of many “squatter areas”.
Always insist to be served hot, hygienically prepared food
Morogoro Health Newsletter - No.5
8
The residents of Morogoro Municipal should take
full responsibility of their health and the cleanliness of
their Municipality by forming partnership with the
Municipal authority to reverse the current trend.
In 2003, the Municipality, with the assistance from
the Danish Embassy through DANIDA, has come up
with a new approach which is the Sustainable
Morogoro Program (SUMO). If the program is
supported, it will be part of the solution of the
problem.
One of SUMO’s main objectives is to address the
Solid Waste (SW) problem in the Municipality
through a more participative, effective and efficient
management to be known as the Morogoro
Sustainable Solid Waste Program already in place
since July 2005. The program is mainly Community
Based Organizations (CBOs) engaging women and
youths in managing SW in partnership with the
Municipality.
This is expected to offer, apart from ownership,
economic empowerment to the CBOs thus
contributing towards “MKUKUTA” (Poverty
Reduction Programme).
The CBOs are expected to get their earnings
through fees which they will collect from households
and in turn clean streets, drains and open spaces as
well as serve as an eye for Health Officers in matters
pertaining to the observance of health regulations
within their areas of jurisdiction. They will also
collect from the households selected Skip Bucket
areas and in turn pay Skip Bucket empting fees to the
Municipality. These fees are to be collected and
operated in a special account and be used by the
Municipality to sustain recurrent, dumpsite
management and replacement costs.
The CBOs will be selected through competitive and
transparent local tendering at the ward level by the
Ward Development Committee (WDC). Selected
CBOs will in turn be endorsed by the Municipal
Council Tender Board to formalize the tendering
process. They will also be assisted with initial grant
for basic equipment and working gear required.
Monitoring and Evaluation (M&E) will be done at
the local level by the respective WDCs. M&E by the
Centre will be done through the Wards and the Skip
Bucket emptying fund.
This article aims at raising awareness of the new
process to all stakeholders in order to solicit
cooperation in its implementation and at the same
time offer room for views and suggestions for
improvement.
Our conviction is that “we can make a change if we
do it together“.
CHMT
Morogoro Municipality
HHOOMMEE BBAASSEEDD CCAARREE IINN KKIILLOOSSAA DDIISSTTRRIICCTT
Kilosa District has started to implement Home
Based Care (HBC) for People Living with HIV/AIDS
(PLWHA) and chronic illnesses.
The chronic illnesses are:
HIV/AIDS, Diabetes mellitus, Epilepsy, Carcinoma,
Tuberculosis, Mental illness and Heart diseases
Morogoro Health Newsletter – No.5
9
The program was initiated due to the following:
The number of patients with HIV/AIDS and
chronic illness has increased. The hospital bed
occupancy due to HIV/AIDS and related diseases
is 50 – 60%.
Enable health workers to assist to build capacity
at all levels of community and family on how to
help patients through HBC.
Specific objectives of the program are:
To reduce pains for PLWHA and chronic illness.
To facilitate family members who provide care
for PLWHA to attend to other responsibilities.
To provide counseling to PLWHA and other
chronic illness and their families.
Distribute HBC supplies, equipments and drugs
to trained community HBC provider.
Sensitize and motivate community to establish
and maintain HBC services focusing on felt
needs and sense of ownership.
Promote awareness on infection prevention, care
and support of chronic illnesses in the
community.
14 Clinical Officers and 28 Public Health Nurses
received 21-day-training on HBC. They started to
implement the program in their health facilities.
The Ministry of Health through the National AIDS
Control Program provided 14 bicycles for HBC
providers; Drugs were purchased for 14 health
facilities, including one hospital, 5 health centers and
8 dispensaries. Funds were also received for
procurement of sugar and floor for the heath facilities
in the program.
Benefits to be realized from HBC are:
The community is sensitized to desist from
discriminating PLWHA.
Reduced hospital bed occupancy through HBC.
HIV/AIDS infection is reduced.
Community members looking after patients by
HBC saves time for other productive ventures.
Through HBC and Antiretroviral (ARV) therapy,
many patients recover and return to normal life.
Other supportive services for HBC patients are:
Prevention of opportunistic infection by using
supplied drugs.
Provision for enriched meals and ensuring good
ventilation of their houses.
Promotion of personal hygiene practices and
clean environment.
Encouraging frequent physical exercises.
Building capacity of HBC providers.
Providing recreational facilities, such as indoor
games, film / video shows etc.
Spiritual support.
Legal support.
Economic / financial support.
Community education in ARV therapy
fundamentals.
Through HBC, HIV/AIDS patients receive ARV
according to World Health Organization (WHO) guide
lines. The district intends to role over this program to
the remaining 49 health facilities in three years.
Dr. W. Munuo
Home based care coordinator
Kilosa
Support mental disordered people in the community by Home Based Care

Morogoro Health Newsletter - No.5
10
OOVVEERRVVIIEEWW OOFF HHEEAALLTTHH OOPPEERRAATTIIOONNAALL RREESSEEAARRCCHH MMAANNAAGGEEMMEENNTT BBYY
TTAANNZZAANNIIAA--JJAAPPAANN MMOORROOGGOORROO HHEEAALLTTHH PPRROOJJEECCTT
Recently a “Collection (Corpus) of the 1st
Operational Research Reports” was produced as an
outcome of practical management trainings for the
Regional and Council Health Management Teams
(RHMT and CHMTs) in Morogoro Region, through
Morogoro Health Project (MHP) whose main
objective is to strengthen managerial capabilities in
district health services in the region.
The introduction of the Health Sector Reform
(HSR), in Tanzania, requires district health managers
to pursue “Evidence-based Plans”, which involve
processes of capturing and analyzing local health
problems and reflecting them in their Comprehensive
Council Health Plans (CCHPs). Consequently,
Operational Research (OPR) implementation for the
purpose of getting evidence became a unique but an
essential challenging activity by Morogoro Region
RHMT and CHMTs. Analytical attitude and thinking,
which could be acquired through OPR management,
are necessary for health managers to respond to newly
demanded expectations from the Public Sector
Reforms agenda by the government.
With strong demands from the Health Management
Teams the MHP has been, since September 2004,
facilitating the process of conducting actual OPR by
RHMT and CHMTs in respective districts. This is in
addition to providing them with essential technical
skills and involving also Frontline Health Workers
(FLHWs) and the community. After the operational
research, interventions were planned and, where
applicable, included in CCHPs.
The researched topics (involved team in bracket)
and the respective planned interventions in the year
2005/6 were:
1) High perinatal deaths in Morogoro Municipality
(RHMT) - Intervention: Strengthen model perinatal
ward
2) Factors influencing utilization of ITNs among
Under-Fives in Morogoro Urban (Municipal
CHMT) - Intervention: Sensitization meetings to
hamlet leaders on ITNs use
3) Exploration of utilization pattern of health
services by pregnant mothers during delivery in
Morogoro District (Morogoro CHMT)
- Intervention: Orient FLHWs on focused antenatal
care
4) Factors influencing low coverage of ITNs in
Malaria control in Mvomero District (Mvomero
CHMT) - Intervention: Sensitization of private sector
on ITNs sale
5) Determining factors that influence diarrhoea
disease epidemic among households in three
divisions in Kilosa District (Kilosa CHMT)
- Intervention: Community sensitization on cholera
control
6) Determining performance of health
interventions in addressing cholera outbreaks in
Ifakara Division in Kilombero District (Kilombero
CHMT) - Intervention: Participatory Hygiene and
Sanitation Transformation (PHAST) training for
community and health assistants
7) Determining factors influencing high morbidity
and mortality to Under-Five Children in Mwaya
Division in Ulanga District (Ulanga CHMT)
- Intervention: Training on Community IMCI
In November 2004, the MHP established OPR
Working Group (WG), composed of one OPR Contact
Person from each RHMT and CHMT. Through

Morogoro Health Newsletter – No.5
11
intensive discussions in regular WG meetings, the
members developed rapport among themselves, and
accommodated suggestions and constructive
criticisms to improve the quality of their researched
topics. Consequently they are strengthening their
communication and team building skills, which are
directly applied by the health management team of
each WG member. The WG members are the
important instrumental agents in the OPR
management.
In summary, OPR management created
‘confidence’ among the health managers, which is
essential to accomplish their challenging managerial
tasks by means of required technical skills. Thus, it
can be concluded that OPR management is among the
most effective strategies to strengthen managerial
capacity of the regional and district health managers
under the decentralization process of Public Sector
Reforms in Tanzania.
In view of the significance of sharing research
results with the community and various authorities of
relevant levels in order to maximize the benefit from
the research, the CHMTs and RHMT decided to
organize information dissemination activities with
stakeholders by using most cost-effective means in the
respective districts. The OPR WG acknowledges that
“Morogoro Health Newsletter” is one among such
means and appreciates for the space allocated for OPR
activities in the Newsletter.
Appreciation is expressed to the RHMT and
CHMTs for their dedication, to the Regional and
District administrative authorities for their support and
cooperation throughout the research exercise, to the
FLHWs and the communities for their cooperation
during data collection.
It is believed that the health managers in Morogoro
Region would further develop their managerial
capacity by perpetually continuing the OPR
implementation which would have positive impacts
toward many optimal directions to actualize better
health services and hence better health status of the
people of Morogoro Region and Tanzania generally.
Ms. E. Fukushi
Technical Advisor & OPR-WG Organizer
Morogroro Health Project
IMPORTANT EVENTS : August – December 2005 AUGUST 1st – 5th, 2005 Regional Medical Officers’ Conference
Theme: “Non-communicable diseases: a challenge to Tanzania people” Venue: Mtwara
AUGUST 8th, 2005 Nane Nane (Farmers’ Day)
Theme: “Quality farming is an important tool for reduction of all types of poverty”
Venue: Mbeya (national) and Morogoro (zonal)
OCTOBER 2nd – 23rd, 2005 Final Evaluation of Morogoro Health Project (MHP) Good achievements were reported, and the Project has been extended for one year up to March 2007.
OCTOBER 14th, 2005 Nyerere Day NOVEMBER 18th, 2005 Opening of Kilosa Health Information Resource Centre DECEMBER 1st, 2005 World AIDS Day Theme: “Stop AIDS: keep promise” Venue: Songea, Ruvuma
DECEMBER 9th, 2005 Independence Day DECEMBER 14th, 2005 General Election Day of the United Republic of Tanzania

Morogoro Health Newsletter - No.5
12
CARTOON The significance of Food Safety to the Community Author/Drawing: Mr. N. Masaoe & Mr. J. Bundu
Articles or letters to the Editor should be addressed to:- The Editor Morogoro Health Newsletter P.O.BOX 110, MOROGORO or, P.O.BOX 1193, MOROGORO FAX 023 - 2614148
Or
Could be sent to the respective District Medical Officer or Municipal Medical Officer as follows:-
P.O.BOX 166, Morogoro Municipality P.O.BOX 1862, Morogoro P.O.BOX 14, Kilosa P.O.BOX 47, Ifakara, Kilombero P.O.BOX 4, Mahenge, Ulanga
PUBLISHED BY THE EDITORIAL BOARDMOROGORO HEALTH NEWSLETTER
P.O.BOX 110, MOROGORO
M H P
Morogoro Health Project
• Our esteemed readers, we invite views and suggestions on a name you deem suitable for this Newsletter.
• Also we invite your contribution of articles to be included in the Newsletter for the next issue due for July 2006: the articles should be related to health or opinions andsuggestions on how health services are rendered in Morogoro Region and are not to exceed 400 words.
The food is fresh and served hot.
Why do you eat street vendor’s food? Don’t you have enough money? That’s the problem …
you eat everything.
What about its hygiene?





























