Embed Size (px)
Citation preview

Imaging the Future of Stroke: I. IschemiaDavid S. Liebeskind, MD
Envisioning the future of stroke appears daunting considering the milestones already achieved in stroke imaging. A historicalperspective on the developments in stroke care provides a striking narrative of how imaging has transformed diagnosis, therapy,and prognosis of cerebrovascular disorders. Multimodal imaging techniques such as CT and MRI, incorporating parenchymaldepictions, illustration of the vasculature, and perfusion data, can provide a wealth of information regarding ischemic patho-physiology. Key elements of ischemic pathophysiology depicted with imaging include vascular occlusion, compensatory collateralflow, resultant hemodynamic conditions that reflect these sources of blood flow, and the neurovascular injury that ensues. Themantra of “time is brain” has been perpetuated, but this does not provide an entirely accurate reflection of ischemic patho-physiology and imaging insight shows far more than time alone. Maximizing the potential of perfusion imaging will continue toexpand the nascent concept that cerebral ischemia may be completely reversible in certain scenarios. Novel modalities provide afertile ground for discovery of therapeutic targets and the potential to assess effects of promising strategies. Beyond clinical trials,imaging has become a requisite component of the neurological examination enabling tailored stroke therapy with the use ofdetailed neuroimaging modalities. In this first article on ischemia, the focus is on the most recent imaging advances andexploring aspects of cerebral ischemia where imaging may yield additional therapeutic strategies. A subsequent article will reviewrecent and anticipated imaging advances in hemorrhage. These thematic overviews underscore that imaging will undoubtedlycontinue to dramatically shape the future of stroke.
Ann Neurol 2009;66:574–590
Envisioning the future of stroke appears dauntingwhen one considers the milestones already achieved instroke imaging. A historical perspective on the devel-opments in stroke care provides a striking narrative ofhow imaging has transformed diagnosis, therapy, andprognosis of cerebrovascular disorders. When the jour-nal Stroke was introduced almost 40 years ago, com-puted tomography (CT) and magnetic resonance im-aging (MRI) did not exist. Diagnostic imagingrevolved around angiography, accompanied by echoen-cephalography, thermography, radioisotope techniques,and skull films. Clinical semiology was used to guidetreatments largely supportive in nature, without target-ing specific pathophysiology. CT and MRI, followingshortly thereafter, revolutionized the field by providingsnapshots of ischemia and hemorrhage in the brain(Fig 1). Such images inspired exhaustive efforts to es-tablish neuroprotection to save brain, yet the nextbreakthrough was once again heralded by imaging andthe introduction of diffusion-weighted imaging (DWI)two decades later.1,2 As DWI and magnetic resonanceangiography (MRA) made it possible to chronicleevolving infarction caused by arterial occlusion, throm-bolysis provided the first effective treatment to ceasethis devastating process. During the past two decades,perfusion imaging and many other techniques have
flourished. Stroke imaging now accounts for thousandsof publications per year, and imaging has become acentral facet in the management of stroke patients. Inthis first article on ischemia, the focus is on the mostrecent imaging advances and exploring aspects of cere-bral ischemia where imaging may yield additional ther-apeutic strategies. A subsequent article will review re-cent and anticipated imaging advances in hemorrhage.These thematic overviews underscore that imaging willundoubtedly continue to dramatically shape the futureof stroke.
Imaging the Pathophysiology of IschemiaMultimodal imaging techniques such as CT and MRI,incorporating parenchymal depictions, illustration ofthe vasculature, and perfusion data, can provide awealth of information regarding ischemic pathophysi-ology. Imaging goals in stroke typically addresswhether a stroke is the likely diagnosis, if the primaryprocess is ischemic or hemorrhagic, where the lesion issituated, what is the likely mechanism, what treatmentsmay be indicated, and what can be expected fromprognosis. Although extensive information is availablefrom experimental stroke models in the laboratory,knowledge of cerebral ischemic pathophysiology in hu-mans is now readily available from what has become
From the Department of Neurology, University of California LosAngeles Stroke Center, Los Angeles, CA.
Address correspondence to Dr Liebeskind, UCLA Stroke Center,710 Westwood Plaza, Los Angeles, CA 90095. E-mail:[email protected]
Potential conflict of interest: Nothing to report.
Received Feb 11, 2009, and in revised form Jun 8. Accepted forpublication Jun 12, 2009. Published online, in Wiley InterScience(www.interscience.wiley.com). DOI: 10.1002/ana.21787
NEUROLOGICAL PROGRESS
574 © 2009 American Neurological Association

routine imaging of stroke patients. CT and MRI mayprovide slightly different information depending onspecific technical parameters, yet understanding theunderlying pathophysiology is paramount in optimiz-ing care. Accurate interpretation of stroke imaging re-sults is also critically dependent on sound knowledge ofischemic pathophysiology, because erroneous conclu-sions may result from incorrect assumptions about thebiology. In recent years, the surge of stroke imaginghas provided novel insight and led to further discovery.Key elements of ischemic pathophysiology that can bedepicted with imaging include vascular occlusion, com-pensatory collateral flow, resultant hemodynamic con-ditions that reflect these sources of blood flow, and theneurovascular injury that ensues.3
OcclusionObstruction of the cerebral circulation is typically theinitial event and most obvious feature of cerebral isch-emia. It is important to note that such vascular ob-struction can be caused by partial or subtotal luminalcompromise (stenosis), or alternatively, completeblockage of the vessel lumen that limits all antegrade orforward blood flow (occlusion). Even in cases withcomplete occlusion of an artery, it has been noted thattram-tracking may be present with small, persistentchannels of flow lining the peripheral aspects of theclot along the vessel wall.4 These diminutive flowroutes visible with transcranial Doppler ultrasound(TCD) or angiographic techniques may play an impor-tant role in allowing thrombolytic access to the clotsurface. Although ischemia is typically associated witharterial occlusion, venous obstruction can also result inischemia. For all occlusive lesions, the anatomy orstructural aspects of the obstruction are likely less im-portant than the actual flow implications.
Collateral CirculationVessel occlusion may be inconsequential because of theincredible redundancy of the circulatory system and ex-istence of rich collateral networks.5 Collateral circula-tion in the arteries and veins of the brain provides nu-merous alternative routes for blood flow in the settingof obstruction. Because of the complex configurationand often diminutive caliber of collateral vessels, illus-tration of collaterals has often relied on conventionalangiography. Progressive refinements in noninvasiveimaging approaches over the last decade have made itpossible to depict such features with CT angiography(CTA) and MRA.6 Noninvasive imaging of collateralflow patterns at the circle of Willis have been validatedwith respect to conventional angiography using severaltechniques including CTA, phase contrast and time-of-flight MRA, and TCD.6,7 Timing of such studies,however, is critical as such flow patterns may rapidlychange. In contrast with traditional descriptions ofWillisian anatomy that include explicit definitions forfetal or persistent posterior cerebral artery (PCA) sup-ply from the posterior communicating artery, serial an-giographic studies demonstrate that flow in such seg-ments can rapidly alter such appearances.8 Forinstance, the posterior communicating artery is typi-cally dilated in the setting of acute middle cerebral ar-tery (MCA) occlusion and often diminishes in caliberonce the occlusion recanalizes.
Collaterals are recruited at the onset of ischemia be-cause of intraluminal pressure gradients. The small sizeof collateral anastomoses that has evaded many imagingapproaches may be viewed as illogical for this criticaladaptive response to ischemia, but in recent years, wehave learned that such features serve as the perfectsensing mechanism to upregulate arteriogenesis.9 Infact, increased flow across these small flow routescauses marked elevation in fluid shear stress, a key vari-able in vascular homeostasis. Increased fluid shear stressand mechanical stimulation of the vessel wall causes cy-tokine release and vascular remodeling to dilate thevessel. These processes may be evident as early as thefirst few hours after acute stroke onset and continueinto subacute or chronic stages of ischemia. The cere-bral venous system also adapts by retaining blood vol-ume to maximize oxygen and nutrient exchange.
Recent correlative imaging studies of collateral circu-lation in acute and chronic ischemia have demon-strated that the occlusive lesion may be incompletelycharacterized without consideration of collaterals. Forinstance, internal carotid artery (ICA) occlusion mayhave dramatically different effects on downstream per-fusion depending on collaterals. The traditional desig-nation of a stenosis or occlusion as either asymptomaticor symptomatic must also account for collaterals. Untilrecently, strokes contralateral to an ICA occlusion havebeen overlooked, yet mechanistic studies suggest that
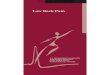
Fig 1. Noncontrast computed tomographic scan of the brainfrom 1974 (A) and magnetic resonance image of the brainfrom 5 years later (B) provided novel depictions of the humanbrain, albeit at limited resolution.
Liebeskind: Imaging the Future of Stroke 575

hypoperfusion and emboli are closely intertwined.10
Collateral flow visible at angiography is a potent deter-minant of tissue fate, even beyond measures of down-stream perfusion evident on noninvasive techniques.11
HemodynamicsThe balance of occlusion and collaterals determines thehemodynamic milieu or blood flow changes that chal-lenge the brain. Depending on the time course, suchchanges may have radically discrepant effects. Long-standing hemodynamic compromise may elicit collat-eral development and preconditioning to adapt to re-current ischemia. Alternatively, abrupt cessation offlow may initiate a complex series of hemodynamic se-quelae that precipitate extensive tissue damage.
Despite extensive investigation on stroke hemody-namics several decades ago, the advent of CT and MRIled to increasing attention centered on neurological tar-gets. Decreased reliance on diagnostic angiography andthe protracted crusade to realize neuroprotection de-tracted from hemodynamic investigations until perfu-sion imaging was introduced. In recent years, perfusionimaging has been able to validate in humans what wasknown of blood flow in ischemic animal models. Lowperfusion hyperemia, the rapid expansion of the venouscirculation in response to reduced arterial inflow, hasbeen illustrated in acute stroke cases.12 Venous collapsein the ischemic core and peripheral displacement ofblood volume caused by venous diversion have alsobeen studied.13 The decline in local cerebral blood vol-ume (CBV) and venous collapse results in increaseddownstream resistance that further aggravates the mar-ginal inflow pressure of arterial collaterals. Progressiveischemia after initial increases in CBV may be ex-plained by this moving wavefront of hemodynamic in-stability originating in the core and moving toward the
boundary of what has been termed benign oligemia (Fig2). Notably, by strict definition, oligemia refers to vol-ume, not flow, and such areas peripheral to the pen-umbra typically have increased or normal CBV. Perfu-sion imaging may show such dynamic features, yet ithas been most often used in various incarnations ofmismatch, where differences between the surroundingperfusion abnormality and the underlying ischemiccore may be used as a surrogate for salvageable penum-bra. This dynamic perspective where hemodynamics inthe territory are constantly evolving within the earlyhours of ischemic onset is radically different from priorconceptions where specific ischemic thresholds mea-sured by perfusion parameters dictate inevitable tissuedamage from the onset.
Neurovascular InjuryTissue injury has been of prime interest as it relates toneurological outcome, yet imaging has provided someimportant lessons. Identification of irreversible isch-emic injury in the brain has repeatedly been proposedas a potential surrogate measure of clinical outcome.The timing of such lesion measurements is extremelyimportant as many stages ensue from the initial appear-ance of early ischemic changes to subacute edema andsubsequent resolution as an area of encephalomalacia.After more than 35 years of discerning early ischemicchanges on CT as a manifestation of evolving infarc-tion, recent correlation with CT perfusion has demon-strated that some increased water content may becaused by increased CBV, not intracellular swelling.14
These findings may be markers of ischemia but do notcarry the same prognostic implications. DWI providesrapid delineation of cytotoxic edema, yet lesion pat-terns are probably most informative about underlyingmechanisms (Fig 3). Punctate lesions within an arterial
Fig 2. Hypothetical model of progressive changes in ischemic pathophysiology (arrow from top to bottom), including venous factorsthat affect cerebral blood volume (CBV) and cerebral perfusion pressure (CPP). Peripheral zones are spared from infarction becauseof benign hyperemia, characterized by increased CBV.
576 Annals of Neurology Vol 66 No 5 November 2009

territory may point to a particular source of emboli, yetattempts to separate hypoperfusion and emboli haveproved difficult.15 Reflexive interpretation of DWIfindings has often prompted a narrow-minded searchfocused solely on arterial emboli and resultant occlu-sions. Complex patterns of blood flow, however, mayalso result in such lesions. Simply stated, small, discretelesions do not necessarily reflect distal emboli alone be-cause hypoperfusion may cause borderzone ischemia.
The focus on DWI has reinforced traditional de-scriptions of the ischemic cascade that commence withion pump failure in membranes of the neuron that fa-cilitate cytotoxic edema, but earlier sequelae may affectvascular structures such as endothelia. Ischemic endo-thelium may limit tissue perfusion by obliterating ef-fective luminal flow because of swelling and loss of reg-ulatory function. Oxygen and other strategies mayprovide vasoprotection, and thereby enhance neuropro-tection.16 Recognition of the neurovascular unit as atherapeutic target may encourage development of otherimaging techniques as well.
After collateral failure or increasing ischemic severity,infarct growth may extend to the limits of the vascularterritory or stop at a point where flow is sufficient tomeet metabolic demands. Ischemic lesion volume hasbeen used as a potential surrogate in past studies, yetpatients may have excellent outcomes despite extensivetissue injury. Lesion location also appears to be critical,as some ischemic strokes may even be “silent” in cer-tain areas of the brain. Refinement of the neurologicalexamination may demonstrate the importance of suchlesions, yet atlas-building will undoubtedly improveclinical-radiographic correlation in the future. Mostcommonly, areas of ischemic injury may be intermixedwith reperfusion. This may be associated with hemor-rhagic transformation (HT), vasogenic edema, or in-flammation. Imaging of subacute stroke may thereforeshow complex and myriad patterns of injury. Detailingrestoration or repair within a certain region of thebrain may be quite difficult with even the most ad-vanced imaging techniques. Overall, the time course of
neurovascular injury varies widely from individual toindividual.
Time Is Brain?The mantra of “time is brain” has been perpetuatedthroughout the stroke community, but this does notprovide an entirely accurate reflection of ischemicpathophysiology. Undoubtedly, ischemic injury in thebrain may evolve quite rapidly within only the firsthours or minutes in select cases, but the time coursevaries markedly across individuals. Time is measuredfrom symptom onset in almost all cases, yet this doesnot reflect stroke onset. In fact, symptoms will becomemanifest only once collaterals fail to compensate forhypoperfusion. Transient symptoms may reflect thebrief transition from dependence on antegrade to ret-
Fig 4. Schematic illustrating the relation between time andbrain lost, noting marked dissimilarity between (A) pathophys-iology measured from time from vascular occlusion (TFVO)and (B) measures utilizing time from symptom onset (TFSO).Each individual curve represents unique temporal features of aparticular case, including baseline brain volume, time tosymptom onset or collateral failure, degree of collateral depen-dence influenced by lesion location, and resultant infarct vol-ume. Rapid decompensation caused by poor collaterals inabrupt cardioembolic occlusion (A, 1) may lead to large in-farcts at very early time points, whereas progressive ischemiaand robust collateralization in intracranial atherosclerosis (A,2) may be manifest with a long time window and smallerinfarct volumes. In the absence of imaging, time alone mea-sured from symptom onset (B, circle) is often used to groupthese identical curves and calculate brain lost based on a lin-ear, rather than a biologically plausible sigmoid, model.
Fig 3. Diffusion-weighted imaging lesion patterns in acuteischemic stroke, including isolated lenticulostriate infarction(left), bilateral middle cerebral artery lesions caused by cardio-embolism (middle), and borderzone ischemia caused by rightinternal carotid artery hypoperfusion (right).
Liebeskind: Imaging the Future of Stroke 577

rograde, collateral flow in a vascular territory. In mostcases, the time of vascular occlusion is never knownand may have occurred hours, days, or weeks in ad-vance. At the most extreme example, asymptomaticMCA occlusion demonstrates that time may be alto-gether irrelevant.
It remains important to encourage patients, the pub-lic, and everyone potentially involved in the triage of astroke patient to demonstrate the “need for speed” andrapidly intervene; however, imaging insight shows farmore than time alone.17–19 The amount of brain lostor burden of ischemic injury can be averaged based ontime from symptom onset to any standard time point,yet this dynamic process is not linear and defies suchcalculations in any particular case. Hour to hour andeven minute to minute, the evolution of ischemic in-jury may vary dramatically. When one averages across apopulation, summary statistics can be generated, butpredicting CT or DWI lesion growth at the bedsidedefies such models. When time from symptom onset ismeasured, we are essentially resetting relative times tocollateral failure, demarcating the initial downward in-flection in sigmoid curves of time versus brain (Fig 4).Even when measured from symptom onset, why does atime window even exist?20 Some have speculated thattissue vulnerability to withstand specific ischemic in-jury can be marked by time. Alternatively, time may beimportant because the hemodynamic process continuesto evolve during this critical period. For instance, in-travenous or intraarterial thrombolysis may be most ef-fective early on because collateral perfusion is adequate.Several hours later, venous collapse and hemodynamicfailure may limit reperfusion even if clot disruption isachieved. This would suggest that effective thromboly-sis may be limited by hemodynamics, not evolving clotcomposition. This may explain why some cases maybenefit from recanalization many hours later in MCA
occlusion or why basilar occlusions can be treated upto 24 hours from symptom onset.21 Even within therestricted time window of 3 hours for intravenousthrombolysis, time may not be on one’s side as poorcollateral flow and extensive hypodensity on CT mayoccur within the first hour or two after symptom onset(Fig 5). The time course of hemodynamic failure andwindow for reperfusion may vary across vascular terri-tories as well. When looking at imaging results, it maybe impossible to distinguish timing altogether (Fig 6).From a therapeutic standpoint, even “late” cases withmismatch pose a dilemma because these cases may notbe prone to failure, thereby altering the risk/benefit ra-tio. Furthermore, time constraints for thrombolysismay differ from windows for other therapeutic strate-gies. If one utilizes hemodynamic augmentation ratherthan thrombolysis, time restrictions may vary.22 Alto-gether, time to imaging remains paramount, becausewithout rapid imaging, one must act rapidly based ontime alone.
Vessel ImagingVascular PathologyAtherosclerosis is the primary culprit of most ischemicstrokes, but many types of vascular abnormalities maybe identified with recent advances in imaging. Fromthe venous circulation to the most proximal sites ofarterial emboli in the heart, CT and MRI can providedetailed information. Cardiac imaging with visualiza-tion of all proximal arteries to the cerebral circulationin one acquisition will likely become routine in thenext few years. Wall motion abnormalities and otherfunctional lesions such as patent foramen ovale can bestudied with cine techniques.23 Hemodynamic evalua-tion of cardiac function may also be assessed withevolving techniques. Enhanced resolution and propergating will be required to thoroughly evaluate the pos-sibility of intracardiac thrombi at risk for embolization.Similarly, the utility of noninvasive modalities such asCT and MRI to evaluate aortic arch atheromatous dis-ease will require further refinement.
Recent work on imaging of the proximal cervicoce-phalic arteries has rapidly expanded to address severalkey questions regarding identification of vulnerable orhigh-risk lesions. Intimal-medial thickness has beenstudied for many years with ultrasound as a marker ofvascular risk and now increasingly with CT andMRI.24 Plaque characterization may be achieved withCTA, black-blood MRI, T1 MRI, and with variousnovel contrast agents such as iron oxide particles thatmay delineate active inflammation or instability.25–27
In parallel, prominent calcifications signifying poten-tially stable yet chronic disease is easily visualized aswell. Calcified plaque on carotid CTA may be associ-ated with reduced risk for subsequent stroke possibly
Fig 5. Extensive computed tomographic hypodensity (A) anddiffusion-weighted imaging evidence of ischemia (B) in the leftmiddle cerebral artery territory in a 40-year-old man within75 minutes of witnessed onset of right hemiparesis and apha-sia.
578 Annals of Neurology Vol 66 No 5 November 2009

because of reduced emboligenic potential.28 Manystudies have embarked on detecting lipid-laden plaqueat the carotid bulb that may be prone to rupture orhemorrhage. Similar techniques for evaluation of theintracranial circulation await further development. Inthe future, one may expect to differentiate risk for in-tracranial atherosclerotic disease based on direct imag-ing of such plaques in the arteries at the base of thebrain. Recent work has highlighted the potential roleof MRI to characterize vasculitis in the intracranial vas-culature, manifest as frank enhancement of the vesselwall.29 These approaches may complement the currentrole of conventional angiography for vasculitis whereonly luminal irregularities may be seen with no infor-mation about the vessel wall itself. Intramural lesionssuch as dissection have been easily identified with such
noninvasive techniques for many years now. Asidefrom predilection for certain sites in the circulation andguidance from classic clinical features to suggest thisdiagnosis, dissection is readily identified by the spiral-ing crescent of intramural hematoma on fat-saturationT1-weighted MRI or other noninvasive techniques.Often subtle lesions with this highly specific configu-ration of dissection can be seen on other sequencessuch as fluid-attenuated inversion recovery images (Fig7). Small-vessel disease remains elusive, often identifiedonly by the ischemic lesions in subcortical zones. Al-though direct imaging of small vessels in the brain can-not be reliably achieved, associated findings such as ce-rebral microbleeds and the newly recognizedpathological role of Virchow–Robin spaces is expand-ing current knowledge.30 Previously considered nor-
Fig 6. Detailed imaging of acute middle cerebral artery stroke (left to right: diffusion-weighted imaging, fluid-attenuated inversionrecovery, time-to-peak perfusion magnetic resonance imaging) shows that one cannot tell time from images because marginal tissuedamage may be present at 19 hours (left) compared with more extensive injury at 100 minutes (right).
Fig 7. Fluid-attenuated inversion recovery images showing the hyperintense, spiraling crescent sign of dissection in the right petrousinternal carotid artery (three sequential axial images from left) and associated borderzone infarction in downstream right parietalregion (far right).
Liebeskind: Imaging the Future of Stroke 579

mal, Virchow–Robin spaces are now being revisited asa possible marker of small-vessel disease.
In coming years, detailed imaging of such vascularpathology may help stratify risk, allowing more in-formed decisions about potential therapeutic interven-tions. Adding this imaging data may help identify un-stable or symptomatic lesions, revising the standarddefinitions that have been used in carotid disease fordecades. These techniques may also be used to monitortreatment, as in the case of statin therapy for carotidplaque regression.
Stenosis and OcclusionA broad array of imaging modalities from ultrasoundand angiography to CTA and MRA now make it pos-sible to characterize focal narrowings or stenoses inthe cerebral circulation. The most common measureof grading stenoses, measurement of luminal caliberreduction, has principally relied on the North Amer-ican Symptomatic Carotid Endarterectomy Trial(NASCET) method in the extracranial carotid arteryand the Warfarin-Aspirin Symptomatic IntracranialDisease (WASID) method in the intracranial circula-tion. Most noninvasive technologies have been vali-dated against the gold standard of conventional an-giography, and a plethora of reports have includedmultiple modalities evaluated at once. Simple correla-tions between angiographic techniques are often re-ported, yet proper evaluation requires elimination ofbias and rigorous trial design as in the Stroke Out-comes and Neuroimaging of Intracranial Atheroscle-rosis (SONIA) study.31–33 Rough correlations acrossmodalities have been substantiated, but exact agree-ment is almost never achieved. Aside from othermethodological issues, the inherent nature or physicalbasis of the technique must be considered. For in-stance, CTA utilizes relatively prolonged acquisition
after contrast injection, thereby providing maximalanatomic detail of the lumen. MRA techniques gen-erally accentuate flow features; therefore, a moderatestenosis based on luminal caliber may show poor dis-tal flow caused by hemodynamic effects. Inaccuracyof stenosis measures on time-of-flight MRA may sim-ply be caused by pronounced flow reduction. Evenglobal reductions in cerebral blood flow may limitMRA depiction, as often seen on time-of-flight MRAin elderly patients (Fig 8). In short, CTA accentuatesanatomy and MRA emphasizes flow. Dynamic, phasecontrast and quantitative MRA all capitalize on thisaspect. Although the management of extracranial andnow intracranial stenoses has revolved solely aroundsingle measures of percentage luminal reduction, non-invasive and conventional angiography may better de-fine how tandem stenoses, lesion length, tortuosity,and other morphology may influence downstreamflow.
The complex configuration of the intracranial circu-lation and limited capacity to reliably discern flow insmall, distal vessels without conventional angiographyhas limited our understanding of key mechanisms instroke caused by intracranial atherosclerosis. Althoughcombinations of noninvasive techniques includingTCD with embolus detection, angiographic studies,and perfusion imaging may be used to serially evaluatethese cases, such an intensive battery has not been an-alyzed to date.34 Current therapeutic approaches, in-cluding angioplasty and stenting, have been basedsolely around presence of symptoms and solitary mea-sures for degree of stenosis.35 Recent work has demon-strated that asymptomatic intracranial stenoses havelow risk for stroke, and that angiographic collateralflow beyond a stenosis remains the most potent predic-tor of recurrent ischemia.36,37 Future research will de-fine the role of collaterals, arterial emboli, perforator
Fig 8. The effects of global cerebral blood flow may be evidentin the perceived quality of time-of-flight magnetic resonanceangiography, with limited depiction of distal vessels in a 90-year-old man (A) compared with detailed illustration of theintracranial circulation in a 26-year-old woman with mi-graine (B).
Fig 9. Axial source image (A) and coronal maximal intensityprojection (MIP) view (B) of computed tomographic angiogra-phy in acute left middle cerebral artery (MCA) occlusion (ar-rows). Opacification in more distal segments of the proximalMCA on axial source images (A) because of collaterals may bemistaken for patency of the MCA unless MIP views (B) areviewed.
580 Annals of Neurology Vol 66 No 5 November 2009

compromise, and in-stent restenosis utilizing the latestimaging technology. Severe intracranial disease may ex-ist without hemodynamic impairment, as chronicMCA occlusions may show no abnormalities onpositron emission tomography.38 Such compensated le-sions are often seen with moyamoya syndrome, the ul-timate model of acute-on-chronic ischemia in humans.Recurrent ischemia eventually stabilizes after gradualocclusion of multiple proximal arteries. The progressivecompensation in CBV allows such patients to avoidmajor strokes, despite extensive mismatch on perfusionimaging.39 Recurrent ischemia in MCA stenosis typi-cally results in small infarcts along the borderzones.40
These lesions may be caused by emboli or hypoperfu-sion, which typically coexist.15 After surgical revascu-larization, perfusion patterns and arterial territoriesmay completely shift.41,42
Complete occlusion can be illustrated with mostmodalities. More dramatic flow effects evident onTCD or MRA may focus attention on a particular ves-sel, whereas the exquisite anatomic detail of CTA mustbe carefully inspected to avoid missing an occlusion. Asthe entire vascular circuit may be visualized with CTA,including enhancement of collaterals at the distal endof the occlusion and the deep middle cerebral vein,proper evaluation on thin maximum intensity projec-tion images may be required (Fig 9). CTA is extremelyvaluable for rapid evaluation of potential occlusion inmost stroke patients.43 For more than two decades, thepresence of a hyperdense artery on noncontrast CT hasbeen used as a sign of MCA occlusion. More recently,this finding has been described in the ICA andPCA.44,45 Others have demonstrated that, althoughthis finding is a marker of poor outcome, intravenousthrombolysis may be effective with such lesions.46 Hy-
perdense arteries on CT associated with clot are oftenmistakenly described as early ischemic findings, andvarious mimics exist as well. Increased use of gradient-recalled echo (GRE) MRI has stimulated interest inblooming artifact or hypointensity in and around a ves-sel containing thrombus. Age of the clot, amount ofthrombus, location, and local flow conditions all affectappearance of this finding. Only recently hasradiographic-pathological correlation investigated howclot composition affects appearance on CT and MRI.The first descriptive series of clots extracted from hu-mans with acute ischemic strokes noted that thrombirich in red cell content appear hyperdense on CT andhypointense on GRE.47 It was also noted that clotsmay be obtained from vessels that do not manifest suchfindings indicative of thrombosis. Further developmentof thrombolysis and thrombectomy devices will likelyspur further work on imaging of clot composition invivo.
Collaterals and Other Flow RoutesAn overwhelming focus on arterial obstruction by clotsor stenoses has detracted from imaging of actual isch-emia and related flow phenomena. Slowing of flow im-mediately upstream from an occlusion may be seen ashyperintensity on fluid-attenuated inversion recovery(Fig 10A). Diversion of flow into adjacent territories toprovide collateral support may also be evident, either asipsilateral prominence of the PCA in MCA occlusionor as conspicuous flow voids on GRE in collateral ves-sels. These MRI findings reflect flow diversion mani-fest on TCD.48 Other indicators of flow abnormalitiesinclude absence of flow voids downstream from an oc-cluded vessel. On GRE, phase mismapping that is nor-mally present with robust flow may disappear.49 Thisbright stripe or hyperintensity at the margin of the ves-sel is an artifact that is produced by relatively fasterflowing blood being “mismapped” by the MRI to theedge of the vessel also indicating the direction of flow.On rare occasion, flow reversal or retrograde collateralflow in the MCA may be discerned by the flippedphase-mismapping artifact in vessels entering the Syl-vian fissure from the PCA. Slow, retrograde flow be-yond an occlusion is frequently seen as fluid-attenuatedinversion recovery vascular hyperintensity (see Fig10B).50 Other conspicuous vessel findings include de-oxygenation seen as hypointensity on GRE in drainingveins of the ischemic territory, either over the hemi-spheric convexity or through the basal venous circuit.
PerfusionThe perfusion status of downstream regions in the set-ting of ischemia determines tissue injury, shapes recan-alization, influences effective reperfusion, and impor-tantly, mitigates HT. Limited hypodensity, or a highAlberta Stroke Program Early CT Score (ASPECTS),
Fig 10. Fluid-attenuated inversion recovery of M2 segmentalocclusion of the middle cerebral artery demonstrates vascularhyperintensity immediately proximal to the occlusion (A)caused by slow flow and serpiginous vascular hyperintensitydistal to the occlusion (B) from slow, retrograde collateralflow.
Liebeskind: Imaging the Future of Stroke 581

on CT facilitates recanalization with thrombolysis.51
Even when CTA source images are used to judge theextent of injury at baseline, CTA may predict goodfunctional outcome if the ASPECTS is preserved. Sim-ilar correlates have been demonstrated with DWI AS-PECTS.52 Collateral perfusion beyond an occlusion,therefore, not only preserves tissue at risk for infarc-tion, but aids recanalization. This concept that down-stream flow influences what happens upstream is animportant facet that underscores the dynamics and in-terrelated aspects of ischemia, a radically different ap-proach than solely considering mismatch or the elusivepenumbra as a target to be salvaged only by removingthe arterial occlusion. For the last decade, perfusionimaging in ischemic stroke has been equated with mis-match and the identification of the vulnerable regionof brain. The penumbra, aptly termed as a shadow caston the brain by vascular physiology, has been describedas residing or emanating from brain parenchyma itself.Selective neuronal loss in the penumbra may occur, yetone should not forget that, in acute ischemic stroke,the primary process is vascular. Mismatch is, therefore,a moving target that may be largely influenced by he-modynamics, including preconditioning and factorsthat alter blood flow immediately after occlusion. Thefocus on arterial occlusion and extensive use of CT andMRI perfusion imaging has largely eliminated consid-eration of specific vascular structures that may be evi-dent on angiography. For instance, arterial collateralsor venous drainage patterns cannot be identified withperfusion imaging, yet these are important features vis-ible at angiography. Recent development of a novelpostprocessing technique now makes it possible to gen-erate perfusion parameter maps directly from conven-tional angiography (Fig 11), allowing feeding or drain-
ing vessels to be simultaneously identified.53
Perfusion information is often inferred from infarctpatterns or summarily described by a single parameter,rather than delving into the mathematics of flow orunderlying biology. For instance, DWI lesion patternssuch as borderzone infarcts may implicate hypoperfu-sion, and cause is often inferred.54 This may be mis-leading without further confirmatory diagnostic studiesas a transient ischemic attack (TIA) ascribed to embo-lism because of a small punctate lesion on DWI maybe caused by hypoperfusion downstream from large-artery stenosis. The presence of DWI lesions in TIAhas received much attention, yet the biological deter-minants have been neglected as opposed to the empha-sis on revising clinical definitions and prognostica-tion.55–58 Furthermore, infarct size has not always beenan accurate predictor of outcome.59 Monitoring treat-ment with DWI or diffusion tensor imaging and evo-lution of such lesions will be fruitful in comingyears.60,61 Consideration of perfusion in further detail,such as multiparametric analyses, may provide insighton lesion evolution.62 Many perfusion algorithms havebeen used, yet most predictive models have been basedon finding a single optimal parameter.63,64 Perfusionimaging data obtained from first-pass contrast bolustechniques (including CT, MRI, and angiography) arealways described by a curve of contrast concentrationover time, with specific measurements yielding distinctblood flow parameters. Technical differences, includingaccounting for delay and dispersion, may alter calcula-tion of parameters such as CBV.65 Multiparametricmodels of infarct prediction have also failed to considerthe bidirectional nature of CBV changes that evolveover time. Interestingly, substantially more informationis provided by current multiparametric perfusion data
Fig 11. Perfusion angiography images generated from an oblique projection of right internal carotid artery injection at angiographyshows blood flow changes in standard perfusion parameters beyond a right middle cerebral artery occlusion. CBF � cerebral bloodflow; CBV � cerebral blood volume; MTT � mean transit time; CPP � cerebral perfusion pressure.
582 Annals of Neurology Vol 66 No 5 November 2009

compared with older techniques focused solely on CBFmeasurement in animal models. Similarly, arterial spinlabeled MRI focusing on CBF measures may missother important aspects. CBF may be the least dra-matic change during earlier stages of ischemia. Perfu-sion must be considered as flow involving arteries, mi-crocirculation, and veins. Flow is only partiallydetermined by pressure, and resistance has a prominentrole. Multiparametric analyses may better character-ize such individual features. For this reason, time-to-peak on MRI cannot be compared with CBV on CT.Even when specific measures are obtained with identi-cal technical specifications, mathematical errors can-not be overlooked.66 Ultimately, understanding thebiology of perfusion patterns will be critical in devel-oping novel treatments.64,67,68 Even at baseline, onemust consider variables such as hydration status, headpositioning, and serial changes caused by increasingdownstream resistance that influence perfusion imagingpatterns. These studies will also clarify the potentialand limitations of collateral therapeutic strategies suchas induced hypertension or augmentation of pressuresin collapsible veins to reduce downstream resis-tance.22,69–71
ReperfusionReversing IschemiaMaximizing the potential of perfusion imaging willcontinue to expand the nascent concept that cerebralischemia may be completely reversible in certain sce-narios. During the earliest epochs, DWI lesions may bereversible (Fig 12), and even extensive perfusion abnor-malities can be eradicated without arterial recanaliza-tion. These features that have been demonstrated withvenous ischemia may also occur with arterial occlusionif imaged early. Most stroke imaging studies in the pastfocused on infarction and others on later stages of re-pair.72 When an arterial occlusion is identified early,the goal should be to improve perfusion converting po-tential strokes to TIA. Even when CBV appears col-lapsed because of failure to detect low flow with severe
delays, prompt intervention may lead to reversal in iso-lated cases.
No ReflowNow that arterial revascularization strategies abound,the greatest enigma has been recanalization withoutreperfusion. One may expect that removing the arte-rial occlusion should allow pressure to adequately per-fuse downstream reaches, yet resistance has been ne-glected. Such resistance is not necessarily mediated byarteriolar autoregulation, but by the microcirculationand dynamic changes in the venous circulation in thehours that ensue after arterial occlusion.13 No reflowhas been known in the heart and observed in animalstroke models many years ago, yet only recently rec-ognized in the brain. After arterial recanalization, an-giography often shows poor distal perfusion with ta-pered arteries, yet no evidence of distal embolicocclusion. Plugging of the microcirculation has beenpreviously implicated, and reperfusion injury remainslargely unexplored despite concern that this remains acritical issue in acute stroke.73 Imaging of animalmodels has shown that the postischemic blood flowresponse to functional activation is severely attenuatedfor several hours.74 Future studies will be able to ex-plore the role of other factors such as age, sex, andhyperglycemia influencing reperfusion in the micro-circulation and the concept of cerebral ischemic post-conditioning.75–77 Postconditioning suggests thatgradual reperfusion may be more effective than sud-den revascularization. Most importantly, imaging canimprove medical decision making by providing en-hanced estimates that balance risk and benefit of at-tempted reperfusion.
Hemorrhagic TransformationHemorrhagic conversion of an ischemic lesion remainsthe most feared complication of reperfusion. Numer-ous imaging studies have correlated baseline imagingfeatures with subsequent HT.78,79 HT is known to re-sult from severe ischemia exacerbated by reperfusion.80
Leukoaraiosis and associated perfusion abnormalitieshave been studied in this context.81,82 Progressive isch-emia over time caused by impaired perfusion, perme-ability derangements in the blood–brain barrier, andineffective reperfusion after recanalization may all bestudied with imaging.67 Discussion of these imagingapproaches is included in the companion article onhemorrhage.
Innovative DimensionsVessel ImagingThe growth of endovascular therapy has increased theuse of conventional angiography, providing an idealopportunity to perform correlative studies with nonin-
Fig 12. Serial diffusion-weighted imaging of acute left middlecerebral artery occlusion shows an initial subcortical abnormal-ity (A) and complete reversal (B, C) 5 days after treatmentwith intravenous thrombolysis.
Liebeskind: Imaging the Future of Stroke 583

vasive angiographic techniques and perfusion imaging.Continued refinement of CTA and enhanced MRAwill likely yield improved resolution and detection ofincreasingly subtle vascular changes. In diminutive ves-sels, endothelial imaging may show ischemic changes aswell.83 Further validation of quantitative MRA across aspectrum of clinical scenarios will finally move charac-terization beyond isolated measures of stenosis, probingthe amount of flow beyond such lesions.84 Detectionof emboli with TCD offers advantages that no othermodality can address, and increased use of this ap-proach in conjunction with other modalities will un-doubtedly grow in coming years. Such monitoringproximal and distal to specific lesions may disclose theculprit emboligenic lesion with certainty (Fig 13).
PerfusionNumerous aspects of perfusion imaging await furtherdevelopment, although routine use of CT and MRItechniques is already widespread. Several modifications in CT perfusion imaging are being explored including
progressively increased spatial coverage with higher res-olution, reduced contrast requirements, and minimizedradiation effects.85–89 Whole-brain CT perfusion is be-ing developed with several approaches, including up to256 detector rows.85,86 The effects of different biolog-ical factors on CT or MRI perfusion such as proximalstenoses and baseline differences in regional blood floware also under study.90,91 Selective arterial spin labelingwill also be able to show regional differences in perfu-sion.92 Of particular interest is the variation of perfu-sion in white matter and different ischemic thresh-olds.93,94 Regional variation in blood flowabnormalities and topography is already under investi-gation with the development of perfusion atlases.95 Be-cause of the practical constraints of acute stroke imageacquisition, maximal use of perfusion data is a key pri-ority. Currently, permeability maps that denote regionsof contrast leakage in the blood–brain barrier and flowin the microcirculation with flow heterogeneity mapscan be generated from routine perfusion acquisitions(Fig 14). Recent postprocessing modifications allowidentical mathematical approaches to be applied toboth CT and MRI techniques to provide these maps.Prediction of hemorrhage and arteriogenesis can bestudied with these approaches.
ParenchymaDetection of tissue abnormalities associated with isch-emia is also advancing with improved image acquisi-tion and postprocessing. An adaptive smoothing filterof unenhanced CT images may aid recognition of earlyhypoattenuation.96 Sodium MRI may be able to detectextremely early ischemic changes.97 Magnetizationtransfer MRI can also show microstructural damageand possibly selective cellular loss in the salvaged pen-umbra.98 Increasing availability of higher Tesla
Fig 13. Transcranial Doppler ultrasonography with embolusdetection in proximal and terminal segments of the left inter-nal carotid artery confirmed that emboli were emanating fromthis dissection illustrated on angiography.
Fig 14. Permeability image (A) showing blood–brain barrierdisruption in the basal ganglia and flow heterogeneity map(B) showing slowing of microcirculatory blood flow in subcor-tical regions derived from standard perfusion imaging data setacquired in acute ischemic stroke.
584 Annals of Neurology Vol 66 No 5 November 2009

strength MRI units may also improve tissue character-ization, yet comparisons in lesion volume may need toaccount for field strength.99
Functional ImagingBeyond perfusion, numerous other functional imagingapproaches are being developed to study cerebral isch-emia. Diaschisis in the contralateral cerebellum has re-cently been illustrated with MRI of MCA stroke.100
Functional activation studies are also being explored inthe acute phase, although challenges include account-ing for hemodynamic effects and practical aspects suchas testing paradigms while triaging for revasculariza-tion. Deoxygenation of blood flow and penumbralidentification based on T2* sensitivity to an oxygenchallenge are also being studied.101 Magnetic resonancespectroscopy may show serial changes inN-acetylaspartate and lactate.102 Recent magnetic reso-nance spectroscopy investigation has shown that theapparent diffusion coefficient and mean transit timecorrelate with lactate but not N-acetylaspartate, sug-gesting these two parameters are markers of ischemiabut not neuronal loss.103 MRI methods have recentlybeen developed to measure temperature, pH, and evennoise associated with physiological activity.104–106 In-flammation in the ischemic brain associated with leu-kocyte activation and macrophage infiltration may beimaged with ultrasmall paramagnetic iron oxide parti-cles.107–110 Such imaging may be useful in chroniclingangiogenesis and neurogenesis upregulated during thesubacute phase.111 Imaging research on inflammationwill likely be advanced with novel positron emissiontomographic ligands. Innovative imaging approaches inearly stages of development include chemical shift im-aging, hyperpolarization, and paramagnetic chemicalexchange saturation transfer.112–115
Monitoring TherapyThese novel imaging strategies for vessel imaging, as-sessment of perfusion, and parenchyma, and functionalaspects may be extremely useful in monitoring thera-peutic interventions. Serial imaging at baseline, afterrevascularization, before discharge, and during repair isalready under way at several centers. Future correlationwith serology and the use of fusion techniques for con-ventional angiography with CT or MRI will furtherenrich knowledge of ischemia in humans. Severalgroups have already implemented advanced imaging tomonitor the effects of hyperoxia, statins, and othermedications. The potential benefits of hyperoxia foracute ischemia have been illustrated with magnetic res-onance spectroscopy and other MRI techniques.116–118
MRI has been used to illustrate potential beneficial ef-fects of statin therapy.119,120 Sildenafil has also beenshown on MRI to induce angiogenesis and axonal re-modeling after stroke.121 Cellular trafficking of endog-
enous responses or therapeutic delivery of stem cellsmay capitalize on the use of superparamagnetic ironoxide molecules.122,123 The effects of osmotherapy andhemodynamic interventions can already be assessedwith serial MRI.124 In the future, perfusion image ac-quisition with varying head position may provide fur-ther insight.
Trials and TribulationsMulticenter Stroke ImagingImaging has played a central role in several large mul-ticenter trials of acute stroke therapy. Imaging has beenused as selection criteria and detailed in numerous sub-group analyses, yet clinical outcome has alwaystrumped imaging. Most trials have been imaging oftherapy and not necessarily trials of imaging. As a re-sult, many stroke imaging techniques remain unvali-dated. It remains difficult to simultaneously evaluatenovel imaging technologies and stroke therapies in thesame clinical trial. Some have attributed the numerousfailures of stroke trials to heterogeneity that may becharacterized by imaging, yet the costs frequently detertrialists from including intensive imaging approaches.In the future, stroke trials may benefit from using im-aging to classify cases from a diagnostic perspective totailor therapy rather than trialing a single therapyamidst heterogeneity.125 Unfortunately, the imagingapproaches are often quite reductionist, addressing theneed to construct a single primary outcome measure.This defies the enormous prowess of information con-tained in imaging of cerebral ischemia. Negative trialresults may consequently lead imaging to be viewed assuperfluous and subsequently removed altogether fromclinical trials of stroke therapy.
The Diffusion and Perfusion Imaging for Under-standing Stroke Evolution (DEFUSE) trial recentlydemonstrated that specific mismatch patterns may beused to predict outcome with thrombolysis up to 6hours from symptom onset.126 Furthermore, a mis-match ratio of 2.6 provided the greatest sensitivity(90%) and specificity (83%) for identifying patients inwhom reperfusion was associated with a favorable re-sponse.127 MRA-DWI mismatch was also shown to bea useful predictor of patients likely to benefit fromreperfusion.128 Overall, mismatch was associated withfavorable clinical response and smaller infarcts when re-canalization was achieved.129 The Echoplanar ImagingThrombolysis Evaluation Trial (EPITHET) random-ized cases within a 6-hour epoch for thrombolysis, yetgenerated debate because of the equivocal imaging re-sults.130–132 In the Desmoteplase in Acute IschemicStroke (DIAS-2) trial, imaging results differed betweensites that utilized CT versus MRI perfusion imaging,raising more questions about imaging techniques.133
Results from stroke imaging trials are often based on
Liebeskind: Imaging the Future of Stroke 585

averages or summary statistics, and correlations may beestablished, yet the subtleties and details of imaging of-ten remain buried. Site differences in technique mayconfound trial conduct, and current efforts for stan-dardization aim to improve on these limitations.66,134
Even when detailed lesion volumes are used rather thangross visual estimates, much variability persists.135 Forinstance, detailed measures on CT perfusion usually re-quire manual region-of-interest selection based on pre-sumed arterial territories, often avoiding the corticalsurface to exclude large vessels (Fig 15). Depending onthese factors, the resultant averaged value of each per-fusion parameter may vary. Finally, choice of an opti-mal control for a given patient remains unclear. Con-tralateral homologous regions may be best to accountfor age, sex, comorbidities, and other patient-specificfactors. Such issues affect MRI as well. Voxel-basedpredictions may provide incredible power from a sta-tistical perspective, yet such values may be discordantwith clinical outcome despite such power. Penumbralselection and predictive models, therefore, may bequite complicated. In fact, many other factors such asdemographics, baseline or index stroke features, otherimaging patterns, treatment details, subsequent medicalcare, and complications to day 90 may defy predictivemodels. Many imaging predictive models have beenbased on cardioembolic stroke cases in the UnitedStates and have limited utility in stroke because of in-tracranial atherosclerosis among Asian patients. Futureimaging trials must therefore account for such differ-ences. Even when predictive values reach 80%, onemust question whether this can be used to appropri-ately exclude patients from therapy in acute stroke.Most often, a decision about revascularization is made
after detailed imaging, yet a go/no-go paradigm is un-realistic because the risk/benefit may continue to evolvebecause of the dynamic nature of stroke pathophysiol-ogy. Serial risk/benefit assessments, therefore, may bemore appropriate in the management of individualcases.
n of 1 and Tailored Stroke TherapyUnlike the seemingly controlled framework of a clini-cal trial, stroke imaging is usually acquired, interpreted,and implemented case by case on a daily basis. This nof 1 approach often considers numerous factors andimaging subtleties unanswered by prior trials. Imaginghas become a requisite component of the neurologicalexamination as one simply cannot evaluate and managea stroke patient in effective fashion without the use ofdiagnostic neuroimaging capabilities. Such tailoredstroke therapy often places tremendous emphasis onimaging findings, typically evaluated by the clinician inreal time.
The impact of stroke imaging on clinical manage-ment is of paramount importance. Neurologists orother clinicians must often rely on subtle imaging fea-tures guided by key examination findings at the bed-side. Despite reverence for blinding in clinical trials,interpretation of imaging in practice should be any-thing but blinded, based on clinical correlation. Imag-ing information must be maximally extracted from ev-ery image, such as detecting evolving edema fromMRA source images when other sequences are unavail-able. Guidelines on stroke imaging and suggested pa-rameters typically revolve around timelines for imageacquisition, yet many questions about interpretationand subsequent decision making remain unanswered.
Fig 15. Identical computed tomographic perfusion imaging acquisition in three acute stroke cases shows how relatively subjectiveapproaches may alter quantitative blood flow measurements on mean transit time (MTT) maps. Semiautomated approaches to mapstandard arterial territories such as the posterior cerebral artery (A) may yield erroneous values. Manually subsegmented portions ofthe middle cerebral artery territory (B) may show radically different values depending on choice of homologous region used as a con-trol. Cortical regions are inadvertently ignored by measures (B) that attempt to avoid large-vessel influences. Measurements derivedfrom automated region-of-interest sectors around the cortical surface (C) may ignore underlying vascular anatomy and fail to ac-count for entire subcortical regions.
586 Annals of Neurology Vol 66 No 5 November 2009

Optimal management of the wake-up patient or latetime window case continues to baffle clinicians. Forboth TIA and stroke, time to imaging is key becausethe information from images is critical.136 Increasinguse of telestroke to organize acute stroke services em-phasizes imaging as an essential component, and ongo-ing research will explore the practice of stroke imagingin this new context.137
ConclusionsImaging of stroke has continued to accelerate our rap-idly expanding knowledge of ischemic pathophysiol-ogy. Novel modalities provide a fertile ground for dis-covery of therapeutic targets and the potential to assesseffects of promising strategies. The information gar-nered from imaging of ischemia and the cerebral cir-culation discussed in this article has also yielded insighton potential future breakthroughs in hemorrhage to bediscussed in the second article of this series.
References1. Le Bihan D, Breton E, Lallemand D, et al. Separation of dif-
fusion and perfusion in intravoxel incoherent motion MR im-aging. Radiology 1988;168:497–505.
2. Moseley ME, Mintorovitch J, Cohen Y, et al. Early detectionof ischemic injury: comparison of spectroscopy, diffusion-,T2-, and magnetic susceptibility-weighted MRI in cats. ActaNeurochir Suppl (Wien) 1990;51:207–209.
3. Liebeskind DS. Holistic imaging of acute stroke: seeing thebig picture. Ann Neurol 2007;61:501–503.
4. Otsuka Y, Waki R, Yamauchi H, et al. Angiographic demar-cation of an occlusive lesion may predict recanalization afterintra-arterial thrombolysis in patients with acute middle cere-bral artery occlusion. J Neuroimaging 2008;18:422–427.
5. Liebeskind DS. Collateral circulation. Stroke 2003;34:2279–2284.
6. Liebeskind DS. Collaterals in acute stroke: beyond the clot.Neuroimaging Clin N Am 2005;15:553–573, x.
7. Hendrikse J, Klijn CJ, van Huffelen AC, et al. Diagnosingcerebral collateral flow patterns: accuracy of non-invasive test-ing. Cerebrovasc Dis 2008;25:430–437.
8. Liebeskind DS, Sansing LH. Willisian collateralization. Neu-rology 2004;63:344.
9. Bondke A, Buschmann IR. Visualization of therapeutic arte-riogenesis by MR angiography: functional measurements aresuperior to surrogate parameters. J Magn Reson Imaging2007;26:215, author reply 216.
10. Lee SJ, Lee KS, An JY, et al. The lesion patterns and mech-anisms of ischemic stroke contralateral to the internal carotidartery occlusive disease. Eur Neurol 2008;60:27–31.
11. Bang OY, Saver JL, Buck BH, et al. Impact of collateral flowon tissue fate in acute ischaemic stroke. J Neurol NeurosurgPsychiatry 2008;79:625–629.
12. Tomita M, Gotoh F, Amano T, et al. “Low perfusion hyper-emia” following middle cerebral arterial occlusion in cats ofdifferent age groups. Stroke 1980;11:629–636.
13. Pranevicius M, Pranevicius O. Cerebral venous steal: bloodflow diversion with increased tissue pressure. Neurosurgery2002;51:1267–1274.
14. Parsons MW, Pepper EM, Bateman GA, et al. Identificationof the penumbra and infarct core on hyperacute noncontrastand perfusion CT. Neurology 2007;68:730–736.
15. Caplan LR, Wong KS, Gao S, Hennerici MG. Is hypoperfu-sion an important cause of strokes? If so, how? CerebrovascDis 2006;21:145–153.
16. Liebeskind DS. Vasoprotection in ischemic tolerance. In:Schaller BJ, ed. Ischemic tolerance of the brain. ResearchSignpost, 2009. Kerala, India.
17. Alexandrov AV, Rubiera M. Use of neuroimaging in acutestroke trials. Expert Rev Neurother 2009;9:885–895.
18. Del Zoppo GJ, Saver JL, Jauch EC, Adams HP Jr on behalf ofthe American Heart Association Stroke Council. Expansion ofthe time window for treatment of acute ischemic stroke withintravenous tissue plasminogen activator. A Science AdvisoryFrom the American Heart Association/American Stroke Asso-ciation. Stroke 2009 May 28.
19. Saver JL, Albers GW, Dunn B, et al. Stroke Therapy Aca-demic Industry Roundtable (STAIR) Recommendations forExtended Window Acute Stroke Therapy Trials. Stroke 2009;40:2594–2600.
20. Donnan GA, Baron JC, Ma H, Davis SM. Penumbral selec-tion of patients for trials of acute stroke therapy. Lancet Neu-rol 2009;8:261–269.
21. Wunderlich MT, Goertler M, Postert T, et al. Recanalizationafter intravenous thrombolysis: does a recanalization time win-dow exist? Neurology 2007;68:1364–1368.
22. Liebeskind DS. Collateral therapeutics for cerebral ischemia.Expert Rev Neurother 2004;4:255–265.
23. Setser RM, Kim JK, Chung YC, et al. Cine delayed-enhancement MR imaging of the heart: initial experience. Ra-diology 2006;239:856–862.
24. Saba L, Sanfilippo R, Pascalis L, et al. Carotid artery wall thick-ness and ischemic symptoms: evaluation using multi-detector-row CT angiography. Eur Radiol 2008;18:1962–1971.
25. Yoshida K, Narumi O, Chin M, et al. Characterization of ca-rotid atherosclerosis and detection of soft plaque with use ofblack-blood MR imaging. AJNR Am J Neuroradiol 2008;29:868–874.
26. Cappendijk VC, Kessels AG, Heeneman S, et al. Comparisonof lipid-rich necrotic core size in symptomatic and asymptom-atic carotid atherosclerotic plaque: initial results. J Magn Re-son Imaging 2008;27:1356–1361.
27. Yamada N, Higashi M, Otsubo R, et al. Association betweensignal hyperintensity on T1-weighted MR imaging of carotidplaques and ipsilateral ischemic events. AJNR Am J Neurora-diol 2007;28:287–292.
28. Uwatoko T, Toyoda K, Inoue T, et al. Carotid artery calcifi-cation on multislice detector-row computed tomography. Ce-rebrovasc Dis 2007;24:20–26.
29. Kuker W, Gaertner S, Nagele T, et al. Vessel wall contrastenhancement: a diagnostic sign of cerebral vasculitis. Cerebro-vasc Dis 2008;26:23–29.
30. Rouhl RP, van Oostenbrugge RJ, Knottnerus IL, et al.Virchow-Robin spaces relate to cerebral small vessel disease se-verity. J Neurol 2008;255:692–696.
31. Bash S, Villablanca JP, Jahan R, et al. Intracranial vascularstenosis and occlusive disease: evaluation with CT angiogra-phy, MR angiography, and digital subtraction angiography.AJNR Am J Neuroradiol 2005;26:1012–1021.
32. Feldmann E, Wilterdink JL, Kosinski A, et al. The StrokeOutcomes and Neuroimaging of Intracranial Atherosclerosis(SONIA) trial. Neurology 2007;68:2099–2106.
33. Ishimaru H, Ochi M, Morikawa M, et al. Accuracy of pre-and postcontrast 3D time-of-flight MR angiography in pa-tients with acute ischemic stroke: correlation with catheter an-giography. AJNR Am J Neuroradiol 2007;28:923–926.
Liebeskind: Imaging the Future of Stroke 587

34. Tan TY, Chen TY. Detection of microembolic signals usingpower M-mode Doppler sonography in acute stroke patientswith intracranial artery stenosis. J Clin Ultrasound 2008;36:422–426.
35. Zaidat OO, Wolfe T, Hussain SI, et al. Interventional acuteischemic stroke therapy with intracranial self-expanding stent.Stroke 2008;39:2392–2395.
36. Nahab F, Cotsonis G, Lynn M, et al. Prevalence and progno-sis of coexistent asymptomatic intracranial stenosis. Stroke2008;39:1039–1041.
37. Liebeskind DS, Cotsonis GA, Saver JL, et al. Collateral flowgreatly impacts the risk of stroke with intracranial atheroscle-rosis. Stroke 2007;38:477.
38. Tanaka M, Shimosegawa E, Kajimoto K, et al. Chronic mid-dle cerebral artery occlusion: a hemodynamic and metabolicstudy with positron-emission tomography. AJNR Am J Neu-roradiol 2008;29:1841–1846.
39. Surikova I, Meisel S, Siebler M, et al. Significance of theperfusion-diffusion mismatch in chronic cerebral ischemia. JMagn Reson Imaging 2006;24:771–778.
40. Wang X, Lam WW, Fan YH, et al. Topographic patterns ofsmall subcortical infarcts associated with MCA stenosis: adiffusion-weighted MRI study. J Neuroimaging 2006;16:266–271.
41. Kim JM, Lee SH, Roh JK. Changing ischaemic lesion patternsin adult moyamoya disease. J Neurol Neurosurg Psychiatry2009;80:36–40.
42. Jefferson AL, Glosser G, Detre JA, et al. Neuropsychologicaland perfusion MR imaging correlates of revascularization in acase of moyamoya syndrome. AJNR Am J Neuroradiol 2006;27:98–100.
43. Zubkov AY, Uschmann H, Rabinstein AA. Rate of arterialocclusion in patients with acute ischemic stroke. Neurol Res2008;30:835–838.
44. Krings T, Noelchen D, Mull M, et al. The hyperdense pos-terior cerebral artery sign: a computed tomography marker ofacute ischemia in the posterior cerebral artery territory. Stroke2006;37:399–403.
45. Ozdemir O, Leung A, Bussiere M, et al. Hyperdense internalcarotid artery sign: a CT sign of acute ischemia. Stroke 2008;39:2011–2016.
46. Qureshi AI, Ezzeddine MA, Nasar A, et al. Is IV tissue plas-minogen activator beneficial in patients with hyperdense arterysign? Neurology 2006;66:1171–1174.
47. Liebeskind DS, Yong WH, Sanossian N, et al. CT and MRIearly vessel signs reflect clot composition in acute stroke.Stroke 2008;39:564.
48. Kim YS, Meyer JS, Garami Z, et al. Flow diversion in trans-cranial Doppler ultrasound is associated with better improve-ment in patients with acute middle cerebral artery occlusion.Cerebrovasc Dis 2006;21:74–78.
49. Liebeskind DS, Sanossian N, Alger JR, et al. Gradient-echoMRI phase mismapping reveals angiographic correlates inacute ischemic stroke. Stroke 2006;37:637.
50. Sanossian N, Saver JL, Alger JR, et al. Angiography revealsthat fluid-attenuated inversion recovery vascular hyperintensi-ties are due to slow flow, not thrombus. AJNR Am J Neuro-radiol 2009;30:564–568.
51. Tsivgoulis G, Saqqur M, Sharma VK, et al. Association ofpretreatment ASPECTS scores with tPA-induced arterial re-canalization in acute middle cerebral artery occlusion. J Neu-roimaging 2008;18:56–61.
52. Kimura K, Iguchi Y, Shibazaki K, et al. Large ischemic lesionson diffusion-weighted imaging done before intravenous tissueplasminogen activator thrombolysis predicts a poor outcomein patients with acute stroke. Stroke 2008;39:2388–2391.
53. Liebeskind DS, Szilagyi G, Black SE, Buck BH. Perfusionangiography: a novel technique for characterization of perfu-sion in cerebral ischemia. Stroke 2008;39:576.
54. Yong SW, Bang OY, Lee PH, Li WY. Internal and corticalborder-zone infarction: clinical and diffusion-weighted imag-ing features. Stroke 2006;37:841–846.
55. Coutts SB, Eliasziw M, Hill MD, et al. An improved scoringsystem for identifying patients at high early risk of stroke andfunctional impairment after an acute transient ischemic attackor minor stroke. Int J Stroke 2008;3:3–10.
56. Kang DW, Lattimore SU, Latour LL, Warach S. Silent isch-emic lesion recurrence on magnetic resonance imaging predictssubsequent clinical vascular events. Arch Neurol 2006;63:1730–1733.
57. Sylaja PN, Coutts SB, Krol A, et al. When to expect negativediffusion-weighted images in stroke and transient ischemic at-tack. Stroke 2008;39:1898–1900.
58. Sorimachi T, Ito Y, Morita K, Fujii Y. Thin-section diffusion-weighted imaging of the infratentorium in patients with acutecerebral ischemia without apparent lesion on conventionaldiffusion-weighted imaging. Neurol Med Chir (Tokyo) 2008;48:108–113.
59. Tomycz ND, Holm MB, Horowitz MB, et al. Extensivebrainstem ischemia on neuroimaging does not preclude mean-ingful recovery from locked-in syndrome: two cases of endo-vascularly managed basilar thrombosis. J Neuroimaging 2008;18:15–17.
60. Shibazaki K, Iguchi Y, Kimura K, et al. New asymptomaticischemic lesions on diffusion-weighted imaging after cerebralangiography. J Neurol Sci 2008;266:150–155.
61. Alexander AL, Lee JE, Lazar M, Field AS. Diffusion tensorimaging of the brain. Neurotherapeutics 2007;4:316–329.
62. Kane I, Carpenter T, Chappell F, et al. Comparison of 10different magnetic resonance perfusion imaging processingmethods in acute ischemic stroke: effect on lesion size, pro-portion of patients with diffusion/perfusion mismatch, clinicalscores, and radiologic outcomes. Stroke 2007;38:3158–3164.
63. Provenzale JM, Shah K, Patel U, McCrory DC. Systematicreview of CT and MR perfusion imaging for assessment ofacute cerebrovascular disease. AJNR Am J Neuroradiol 2008;29:1476–1482.
64. Sparacia G, Iaia A, Assadi B, Lagalla R. Perfusion CT in acutestroke: predictive value of perfusion parameters in assessing tis-sue viability versus infarction. Radiol Med 2007;112:113–122.
65. Salluzzi M, Frayne R, Smith MR. Is correction necessary whenclinically determining quantitative cerebral perfusion parame-ters from multi-slice dynamic susceptibility contrast MR stud-ies? Phys Med Biol 2006;51:407–424.
66. Wintermark M, Albers GW, Alexandrov AV, et al. Acutestroke imaging research roadmap. Stroke 2008;39:1621–1628.
67. Bang OY, Saver JL, Alger JR, et al. Patterns and predictors ofblood-brain barrier permeability derangements in acute isch-emic stroke. Stroke 2009;40:454–461.
68. Heiss WD, Sobesky J. Comparison of PET and DW/PW-MRI in acute ischemic stroke. Keio J Med 2008;57:125–131.
69. Liebeskind DS. Of mice and men: essential considerations inthe translation of collateral therapeutics. Stroke 2008;39:e187–e188, author reply e189.
70. Shin HK, Nishimura M, Jones PB, et al. Mild induced hy-pertension improves blood flow and oxygen metabolism intransient focal cerebral ischemia. Stroke 2008;39:1548–1555.
71. Han JH, Leung TW, Lam WW, et al. Preliminary findings ofexternal counterpulsation for ischemic stroke patient withlarge artery occlusive disease. Stroke 2008;39:1340–1343.
72. Cramer SC. Repairing the human brain after stroke: I. Mech-anisms of spontaneous recovery. Ann Neurol 2008;63:272–287.
588 Annals of Neurology Vol 66 No 5 November 2009

73. Pan J, Konstas AA, Bateman B, et al. Reperfusion injury fol-lowing cerebral ischemia: pathophysiology, MR imaging, andpotential therapies. Neuroradiology 2007;49:93–102.
74. Zhou C, Shimazu T, Durduran T, et al. Acute functional re-covery of cerebral blood flow after forebrain ischemia in rat.J Cereb Blood Flow Metab 2008;28:1275–1284.
75. Kruyt ND, Nys GM, van der Worp HB, et al. Hyperglycemiaand cognitive outcome after ischemic stroke. J Neurol Sci2008;270:141–147.
76. Ribo M, Molina CA, Delgado P, et al. Hyperglycemia duringischemia rapidly accelerates brain damage in stroke patientstreated with tPA. J Cereb Blood Flow Metab 2007;27:1616–1622.
77. Pignataro G, Meller R, Inoue K, et al. In vivo and in vitrocharacterization of a novel neuroprotective strategy for stroke:ischemic postconditioning. J Cereb Blood Flow Metab 2008;28:232–241.
78. Singer OC, Humpich MC, Fiehler J, et al. Risk for symptom-atic intracerebral hemorrhage after thrombolysis assessed bydiffusion-weighted magnetic resonance imaging. Ann Neurol2008;63:52–60.
79. Bang OY, Buck BH, Saver JL, et al. Prediction of hemor-rhagic transformation after recanalization therapy using T2*-permeability magnetic resonance imaging. Ann Neurol 2007;62:170–176.
80. Rosell A, Foerch C, Murata Y, Lo EH. Mechanisms andmarkers for hemorrhagic transformation after stroke. ActaNeurochir Suppl 2008;105:173–178.
81. Ay H, Arsava EM, Rosand J, et al. Severity of leukoaraiosisand susceptibility to infarct growth in acute stroke. Stroke2008;39:1409–1413.
82. Mandell DM, Han JS, Poublanc J, et al. Selective reduction ofblood flow to white matter during hypercapnia correspondswith leukoaraiosis. Stroke 2008;39:1993–1998.
83. Barber PA, Foniok T, Kirk D, et al. MR molecular imaging ofearly endothelial activation in focal ischemia. Ann Neurol2004;56:116–120.
84. Conway SA, Bowling SM, Geyer JD, et al. Quantitative mag-netic resonance angiography of the cerebrovasculature in phys-iologic and pathologic states. J Neuroimaging 2008;18:34–37.
85. Murayama K, Katada K, Nakane M, et al. Whole-brain per-fusion CT performed with a prototype 256-detector row CTsystem: initial experience. Radiology 2009;250:202–211.
86. Youn SW, Kim JH, Weon YC, et al. Perfusion CT of thebrain using 40-mm-wide detector and toggling table techniquefor initial imaging of acute stroke. AJR Am J Roentgenol2008;191:W120–W126.
87. Kamena A, Streitparth F, Grieser C, et al. Dynamic perfusionCT: optimizing the temporal resolution for the calculation ofperfusion CT parameters in stroke patients. Eur J Radiol2007;64:111–118.
88. Langner S, Stumpe S, Kirsch M, et al. No increased risk forcontrast-induced nephropathy after multiple CT perfusionstudies of the brain with a nonionic, dimeric, iso-osmolal con-trast medium. AJNR Am J Neuroradiol 2008;29:1525–1529.
89. Wiesmann M, Berg S, Bohner G, et al. Dose reduction indynamic perfusion CT of the brain: effects of the scan fre-quency on measurements of cerebral blood flow, cerebralblood volume, and mean transit time. Eur Radiol 2008;18:2967–2974.
90. Serafin Z, Kotarski M, Karolkiewicz M, et al. Reproducibilityof dynamic computed tomography brain perfusion measure-ments in patients with significant carotid artery stenosis. ActaRadiol 2009;50:226–232.
91. Matsushima S, Kubota T, Yamada K, et al. Effect of vascularstenosis on perfusion-weighted imaging; differences betweencalculation algorithms. J Magn Reson Imaging 2008;27:1103–1108.
92. Hendrikse J, van Osch MJ, Rutgers DR, et al. Internal carotidartery occlusion assessed at pulsed arterial spin-labeling perfu-sion MR imaging at multiple delay times. Radiology 2004;233:899–904.
93. Murphy BD, Fox AJ, Lee DH, et al. White matter thresholdsfor ischemic penumbra and infarct core in patients with acutestroke: CT perfusion study. Radiology 2008;247:818–825.
94. Arakawa S, Wright PM, Koga M, et al. Ischemic thresholdsfor gray and white matter: a diffusion and perfusion magneticresonance study. Stroke 2006;37:1211–1216.
95. Nowinski WL, Qian G, Kirgaval Nagaraja BP, et al. Analysisof ischemic stroke MR images by means of brain atlases ofanatomy and blood supply territories. Acad Radiol 2006;13:1025–1034.
96. Takahashi N, Lee Y, Tsai DY, et al. Improvement of detectionof hypoattenuation in acute ischemic stroke in unenhancedcomputed tomography using an adaptive smoothing filter.Acta Radiol 2008;49:816–826.
97. Jones SC, Kharlamov A, Yanovski B, et al. Stroke onset timeusing sodium MRI in rat focal cerebral ischemia. Stroke 2006;37:883–888.
98. Tourdias T, Dousset V, Sibon I, et al. Magnetization transferimaging shows tissue abnormalities in the reversible penum-bra. Stroke 2007;38:3165–3171.
99. Kosior RK, Wright CJ, Kosior JC, et al. 3-Tesla versus 1.5-Tesla magnetic resonance diffusion and perfusion imaging inhyperacute ischemic stroke. Cerebrovasc Dis 2007;24:361–368.
100. Liu Y, Karonen JO, Nuutinen J, et al. Crossed cerebellardiaschisis in acute ischemic stroke: a study with serialSPECT and MRI. J Cereb Blood Flow Metab 2007;27:1724 –1732.
101. Santosh C, Brennan D, McCabe C, et al. Potential use ofoxygen as a metabolic biosensor in combination with T2*-weighted MRI to define the ischemic penumbra. J CerebBlood Flow Metab 2008;28:1742–1753.
102. Munoz Maniega S, Cvoro V, Chappell FM, et al. Changes inNAA and lactate following ischemic stroke: a serial MR spec-troscopic imaging study. Neurology 2008;71:1993–1999.
103. Cvoro V, Wardlaw JM, Marshall I, et al. Associations be-tween diffusion and perfusion parameters, N-acetyl aspartate,and lactate in acute ischemic stroke. Stroke 2009;40:767–772.
104. Marshall I, Karaszewski B, Wardlaw JM, et al. Measurementof regional brain temperature using proton spectroscopicimaging: validation and application to acute ischemic stroke.Magn Reson Imaging 2006;24:699–706.
105. Sun PZ, Zhou J, Sun W, et al. Detection of the ischemicpenumbra using pH-weighted MRI. J Cereb Blood FlowMetab 2007;27:1129–1136.
106. Wang HH, Menezes NM, Zhu MW, et al. Physiological noisein MR images: an indicator of the tissue response to ischemia?J Magn Reson Imaging 2008;27:866–871.
107. Buck BH, Liebeskind DS, Saver JL, et al. Early neutrophilia isassociated with volume of ischemic tissue in acute stroke.Stroke 2008;39:355–360.
108. Nighoghossian N, Wiart M, Cakmak S, et al. Inflammatoryresponse after ischemic stroke: a USPIO-enhanced MRI studyin patients. Stroke 2007;38:303–307.
Liebeskind: Imaging the Future of Stroke 589

109. Saleh A, Schroeter M, Ringelstein A, et al. Iron oxide particle-enhanced MRI suggests variability of brain inflammation atearly stages after ischemic stroke. Stroke 2007;38:2733–2737.
110. Kim J, Kim DI, Lee SK, et al. Imaging of the inflammatoryresponse in reperfusion injury after transient cerebral ischemiain rats: correlation of superparamagnetic iron oxide-enhancedmagnetic resonance imaging with histopathology. Acta Radiol2008;49:580–588.
111. Ding G, Jiang Q, Li L, et al. Angiogenesis detected after em-bolic stroke in rat brain using magnetic resonance T2*WI.Stroke 2008;39:1563–1568.
112. Takasawa M, Moustafa RR, Baron JC. Applications of nitro-imidazole in vivo hypoxia imaging in ischemic stroke. Stroke2008;39:1629–1637.
113. Heckl S. Future contrast agents for molecular imaging instroke. Curr Med Chem 2007;14:1713–1728.
114. Wu Y, Zhou Y, Ouari O, et al. Polymeric PARACEST agentsfor enhancing MRI contrast sensitivity. J Am Chem Soc 2008;130:13854–13855.
115. McCarney ER, Armstrong BD, Lingwood MD, Han S. Hy-perpolarized water as an authentic magnetic resonance imagingcontrast agent. Proc Natl Acad Sci U S A 2007;104:1754–1759.
116. Singhal AB, Ratai E, Benner T, et al. Magnetic resonancespectroscopy study of oxygen therapy in ischemic stroke.Stroke 2007;38:2851–2854.
117. Shin HK, Dunn AK, Jones PB, et al. Normobaric hyperoxiaimproves cerebral blood flow and oxygenation, and inhibitsperi-infarct depolarizations in experimental focal ischaemia.Brain 2007;130:1631–1642.
118. Henninger N, Bouley J, Nelligan JM, et al. Normobaric hy-peroxia delays perfusion/diffusion mismatch evolution, reducesinfarct volume, and differentially affects neuronal cell deathpathways after suture middle cerebral artery occlusion in rats.J Cereb Blood Flow Metab 2007;27:1632–1642.
119. Nicholas JS, Swearingen CJ, Thomas JC, et al. The effect ofstatin pretreatment on infarct volume in ischemic stroke. Neu-roepidemiology 2008;31:48–56.
120. Ding G, Jiang Q, Li L, et al. MRI of combination treatmentof embolic stroke in rat with rtPA and atorvastatin. J NeurolSci 2006;246:139–147.
121. Ding G, Jiang Q, Li L, et al. Magnetic resonance imaginginvestigation of axonal remodeling and angiogenesis after em-bolic stroke in sildenafil-treated rats. J Cereb Blood FlowMetab 2008;28:1440–1448.
122. Walczak P, Zhang J, Gilad AA, et al. Dual-modality monitor-ing of targeted intraarterial delivery of mesenchymal stem cellsafter transient ischemia. Stroke 2008;39:1569–1574.
123. Sykova E, Jendelova P. Migration, fate and in vivo imaging ofadult stem cells in the CNS. Cell Death Differ 2007;14:1336–1342.
124. Chen CH, Xue R, Zhang J, et al. Effect of osmotherapy withhypertonic saline on regional cerebral edema following exper-imental stroke: a study utilizing magnetic resonance imaging.Neurocrit Care 2007;7:92–100.
125. Moustafa RR, Baron JC. Pathophysiology of ischaemic stroke:insights from imaging, and implications for therapy and drugdiscovery. Br J Pharmacol 2008;153(suppl 1):S44–S54.
126. Albers GW, Thijs VN, Wechsler L, et al. Magnetic resonanceimaging profiles predict clinical response to early reperfusion:the diffusion and perfusion imaging evaluation for under-standing stroke evolution (DEFUSE) study. Ann Neurol2006;60:508–517.
127. Kakuda W, Lansberg MG, Thijs VN, et al. Optimal defini-tion for PWI/DWI mismatch in acute ischemic stroke pa-tients. J Cereb Blood Flow Metab 2008;28:887–891.
128. Lansberg MG, Thijs VN, Bammer R, et al. The MRA-DWImismatch identifies patients with stroke who are likely to ben-efit from reperfusion. Stroke 2008;39:2491–2496.
129. Olivot JM, Mlynash M, Thijs VN, et al. Relationships be-tween infarct growth, clinical outcome, and early recanaliza-tion in diffusion and perfusion imaging for understandingstroke evolution (DEFUSE). Stroke 2008;39:2257–2263.
130. Davis SM, Donnan GA, Parsons MW, et al. Effects of alte-plase beyond 3 h after stroke in the Echoplanar ImagingThrombolytic Evaluation Trial (EPITHET): a placebo-controlled randomised trial. Lancet Neurol 2008;7:299–309.
131. Sandercock P, Wardlaw J, Dennis M, et al. EPITHET—where next? Lancet Neurol 2008;7:570–573.
132. Schellinger PD. EPITHET: failed chance or new hope? LancetNeurol 2008;7:286–287.
133. Hacke W, Furlan AJ, Al-Rawi Y, et al. Intravenous desmote-plase in patients with acute ischaemic stroke selected by MRIperfusion-diffusion weighted imaging or perfusion CT (DIAS-2): a prospective, randomised, double-blind, placebo-controlled study. Lancet Neurol 2009;8:141–150.
134. Provenzale JM, Wintermark M. Optimization of perfusionimaging for acute cerebral ischemia: review of recent clinicaltrials and recommendations for future studies. AJR Am JRoentgenol 2008;191:1263–1270.
135. Rivers CS, Wardlaw JM, Armitage PA, et al. Acute ischemicstroke lesion measurement on diffusion-weighted imaging—important considerations in designing acute stroke trials withmagnetic resonance imaging. J Stroke Cerebrovasc Dis 2007;16:64–70.
136. Lavallee PC, Meseguer E, Abboud H, et al. A transientischaemic attack clinic with round-the-clock access(SOS-TIA): feasibility and effects. Lancet Neurol 2007;6:953–960.
137. Wardlaw JM, Farrall AJ, Perry D, et al. Factors influencingthe detection of early CT signs of cerebral ischemia: aninternet-based, international multiobserver study. Stroke 2007;38:1250–1256.
590 Annals of Neurology Vol 66 No 5 November 2009