Embed Size (px)
Citation preview
Interventional Treatment
of Stroke
Andrew F. Ducruet, MD Barrow Neurological Institute
2018 BNI Stroke Rehab Symposium
October 13, 2018

Disclosures
• Consultant: Medtronic, Penumbra,
Cerenovus
Lecture Overview
• Introduction
• Current State of Interventional
Stroke treatment
• Recent Clinical Studies
• Case Studies
• Future Directions
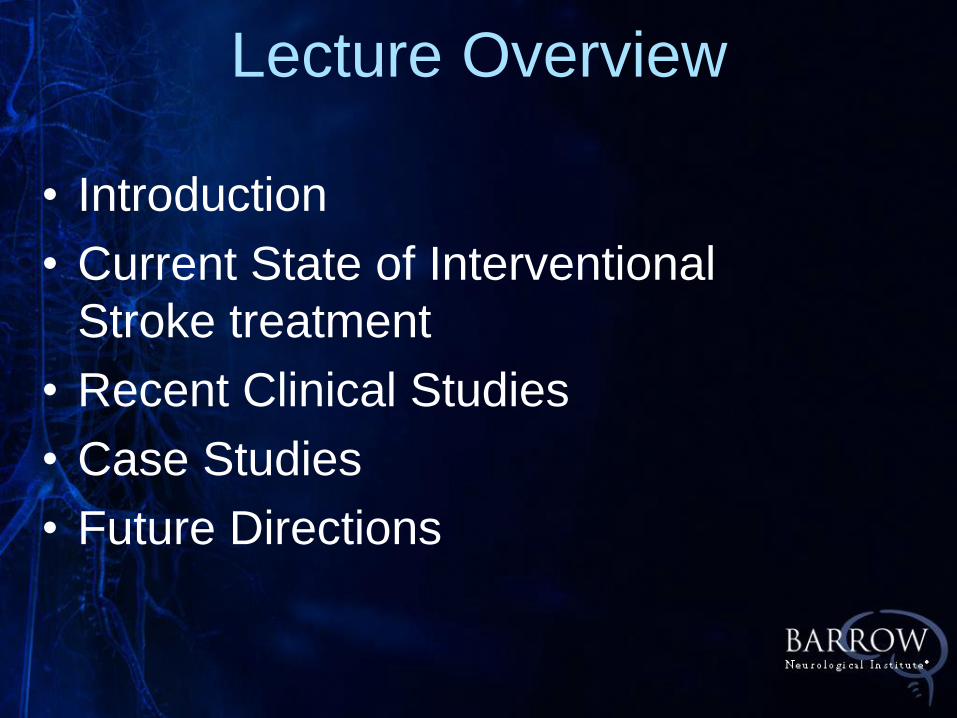
BNI Endovascular Stroke Volume
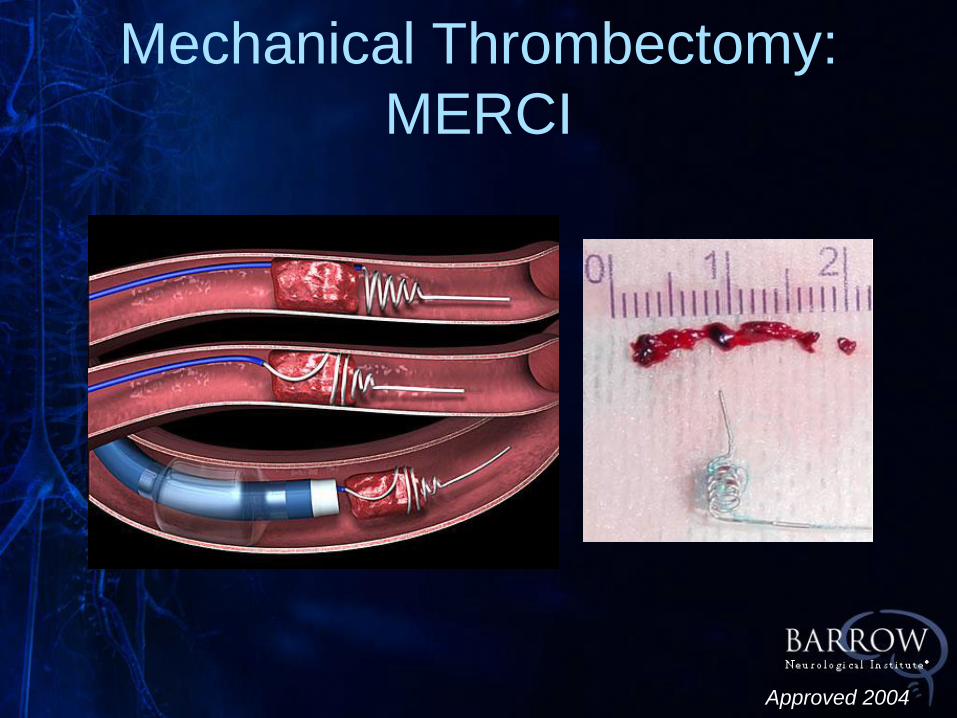
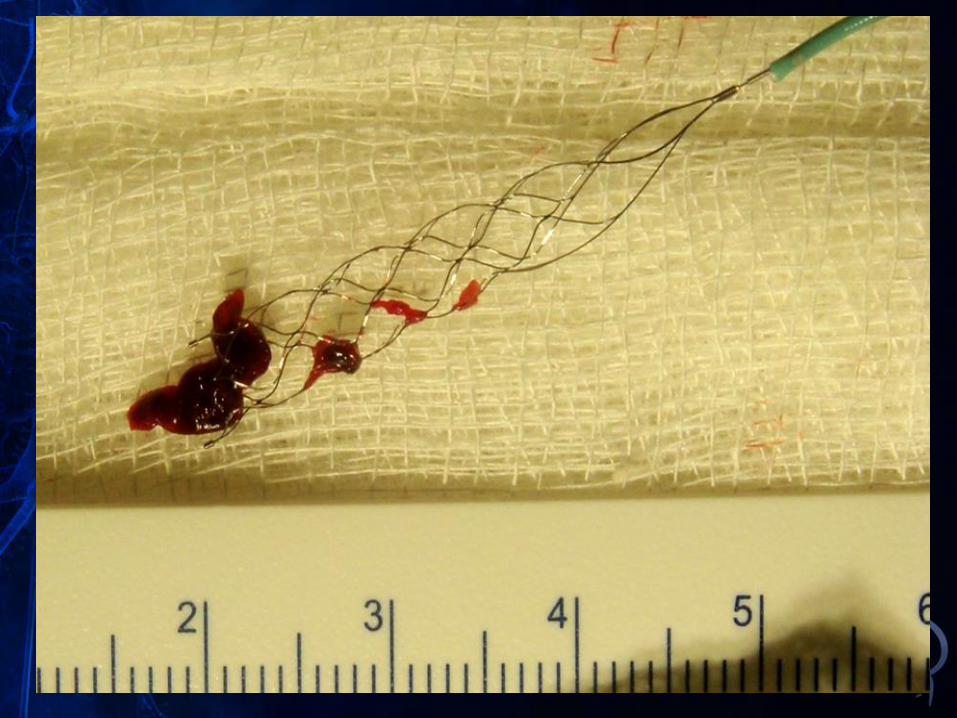
Mechanical Thrombectomy:
MERCI
Approved 2004
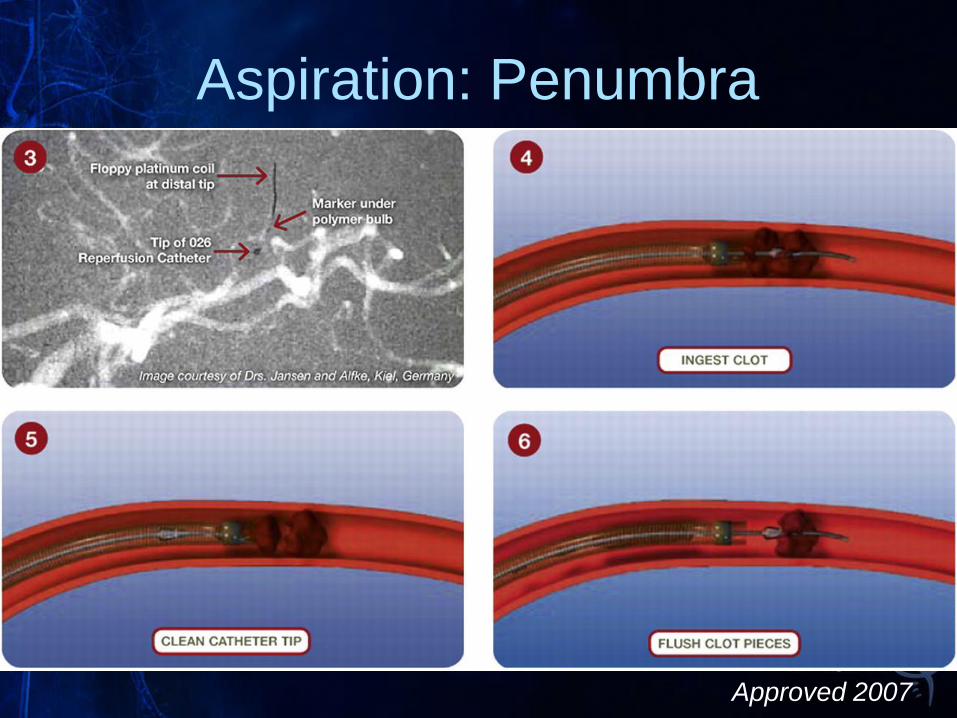
Aspiration: Penumbra
Approved 2007
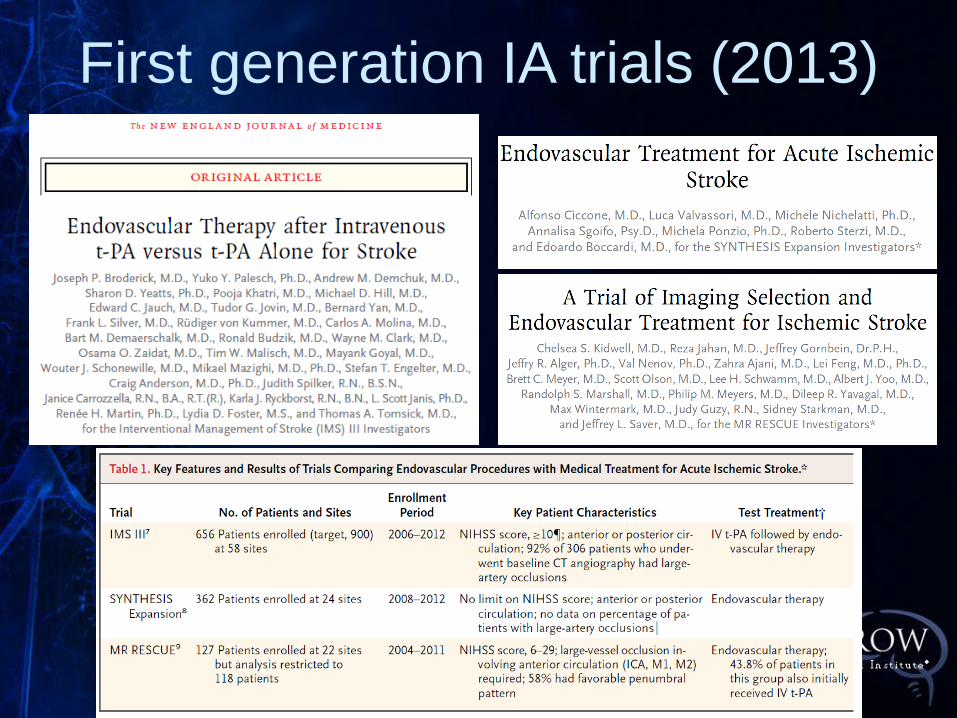
First generation IA trials (2013)
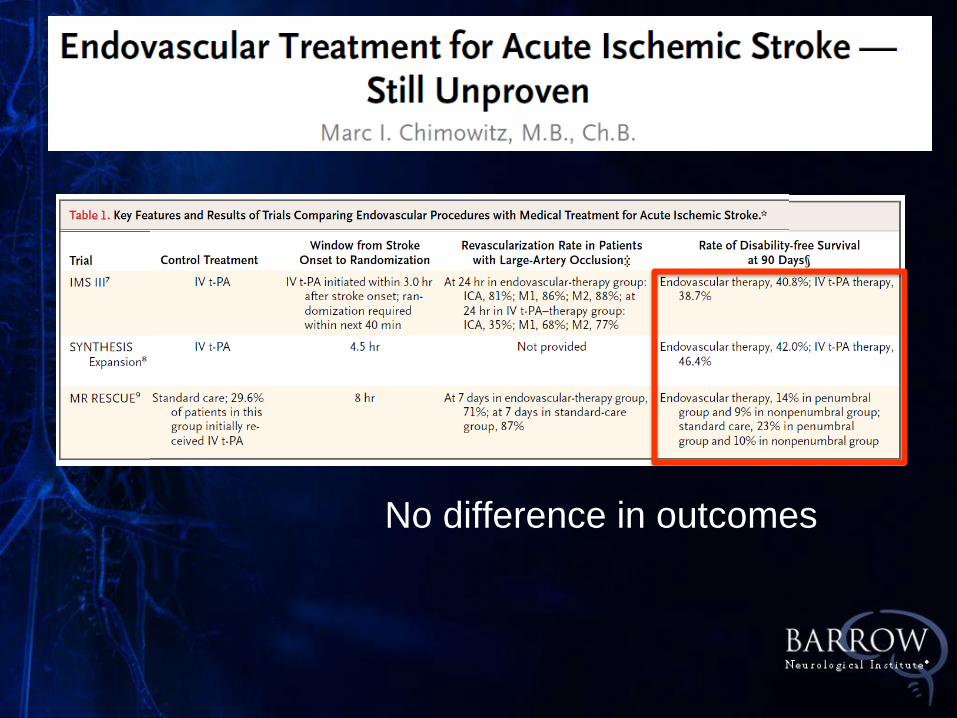
No difference in outcomes
Limits of 1st generation IA trials
• Improper patient selection
• Only 47% of patient had baseline CTA or
MRA documenting an occlusion
• Outdated devices incomplete
recanalization
• Only 27% TICI 2B/3
• Significant delays to reperfusion
• Mean 325 minutes in the endovascular cohort
with a strong time-treatment interaction • Every 30 minutes delay 10% worse outcomes
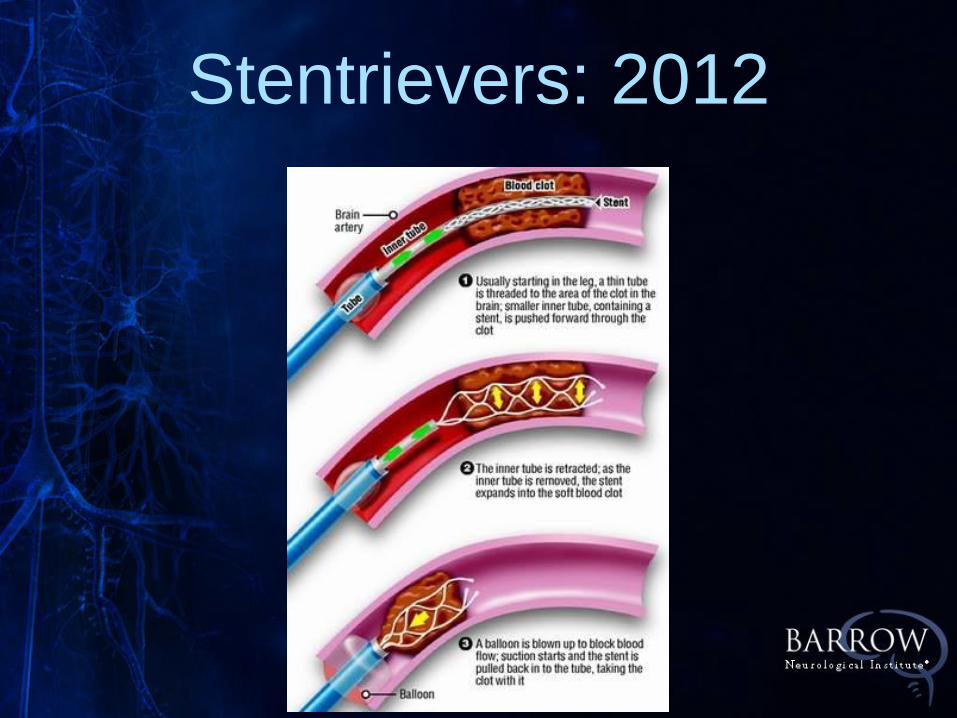
Stentrievers: 2012
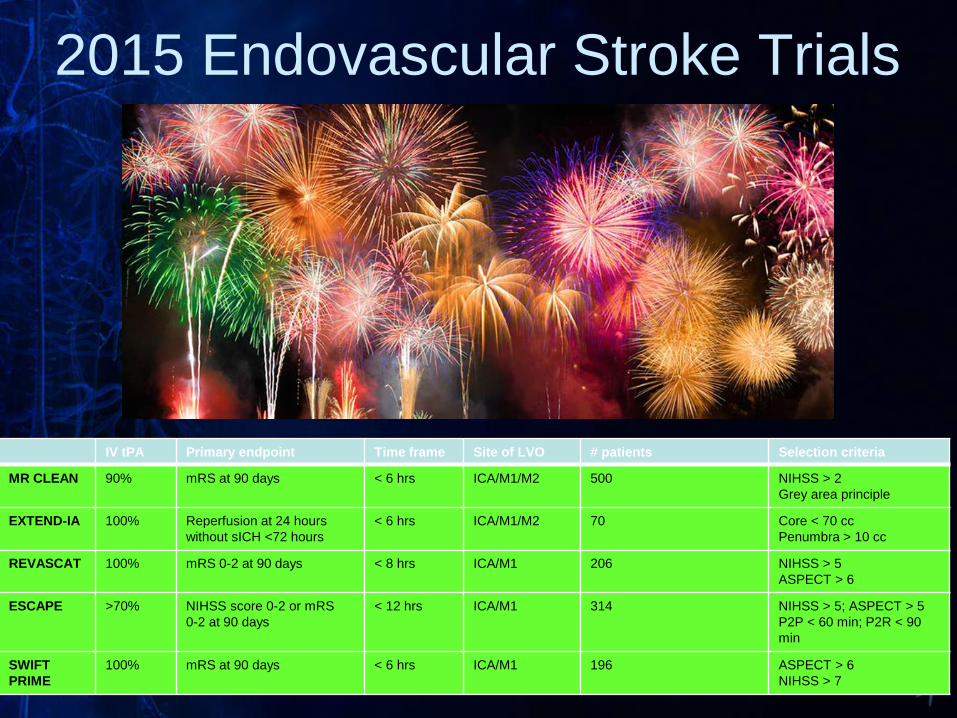
IV tPA Primary endpoint Time frame Site of LVO # patients Selection criteria
MR CLEAN 90% mRS at 90 days
< 6 hrs ICA/M1/M2 500 NIHSS > 2
Grey area principle
EXTEND-IA 100%
Reperfusion at 24 hours
without sICH <72 hours
< 6 hrs
ICA/M1/M2
70 Core < 70 cc
Penumbra > 10 cc
REVASCAT 100% mRS 0-2 at 90 days < 8 hrs ICA/M1 206 NIHSS > 5
ASPECT > 6
ESCAPE >70% NIHSS score 0-2 or mRS
0-2 at 90 days
< 12 hrs ICA/M1 314 NIHSS > 5; ASPECT > 5
P2P < 60 min; P2R < 90
min
SWIFT
PRIME
100% mRS at 90 days < 6 hrs ICA/M1 196 ASPECT > 6
NIHSS > 7
2015 Endovascular Stroke Trials
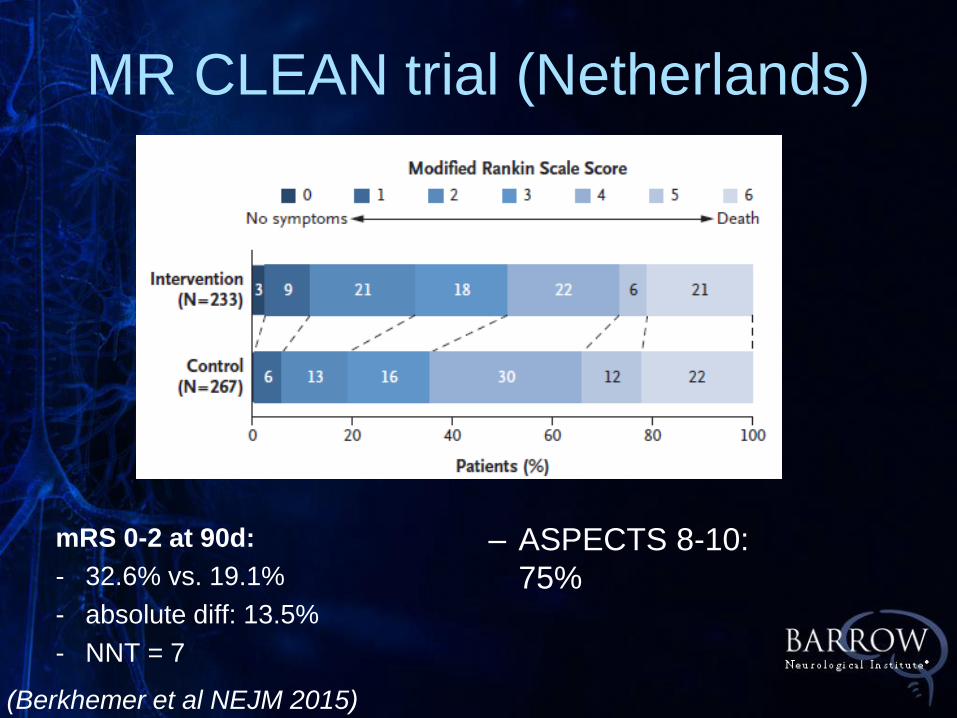
MR CLEAN trial (Netherlands)
– ASPECTS 8-10:
75%
(Berkhemer et al NEJM 2015)
mRS 0-2 at 90d:
- 32.6% vs. 19.1%
- absolute diff: 13.5%
- NNT = 7
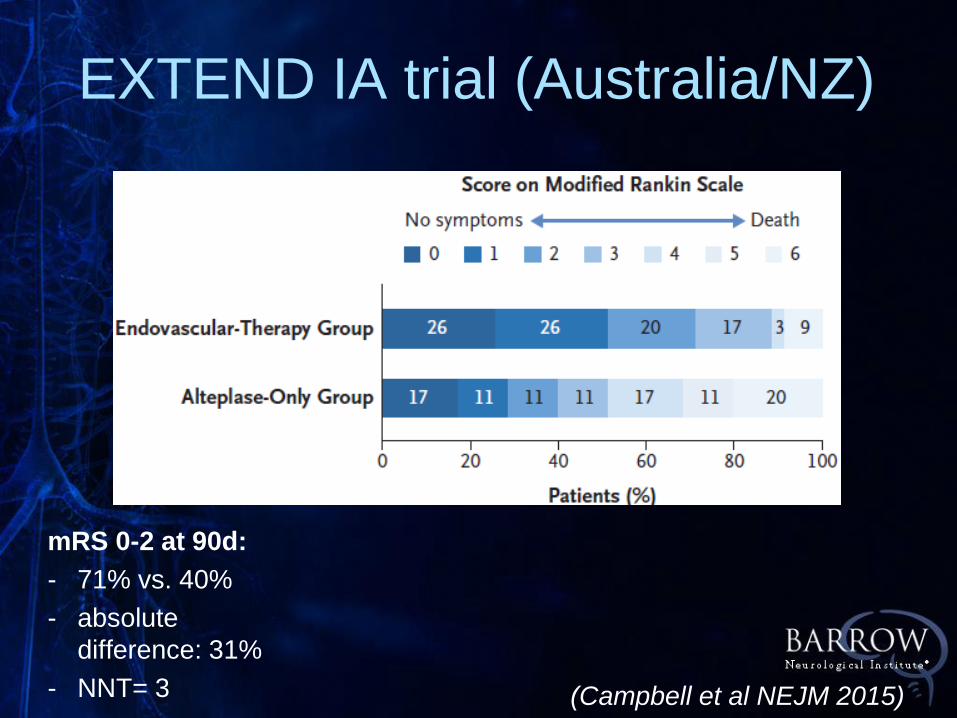
EXTEND IA trial (Australia/NZ)
(Campbell et al NEJM 2015)
mRS 0-2 at 90d:
- 71% vs. 40%
- absolute
difference: 31%
- NNT= 3
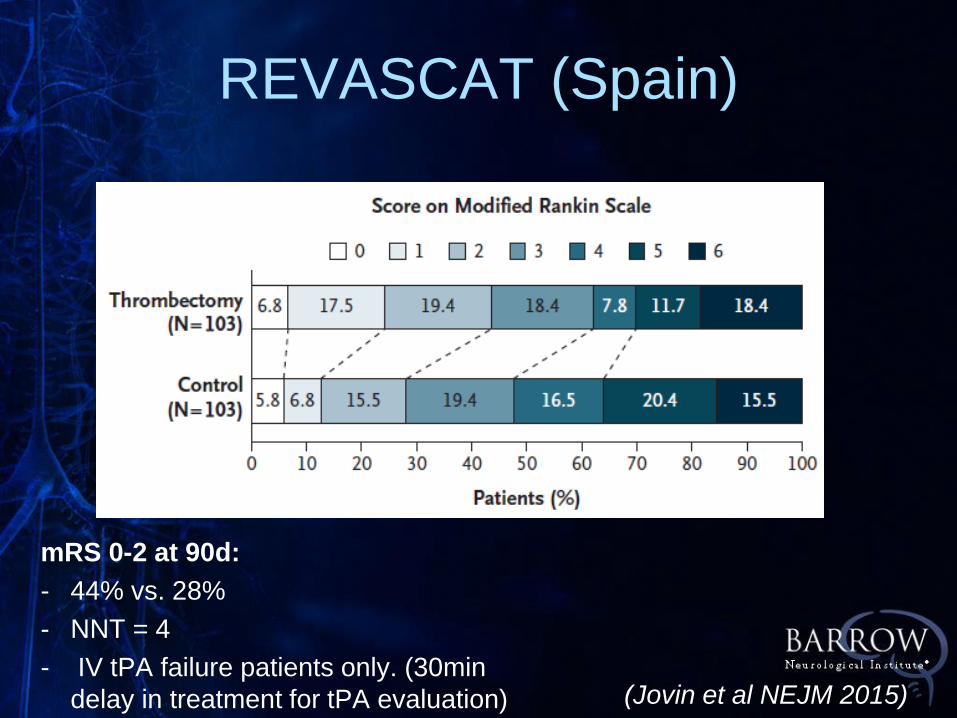
REVASCAT (Spain)
(Jovin et al NEJM 2015)
mRS 0-2 at 90d:
- 44% vs. 28%
- NNT = 4
- IV tPA failure patients only. (30min
delay in treatment for tPA evaluation)
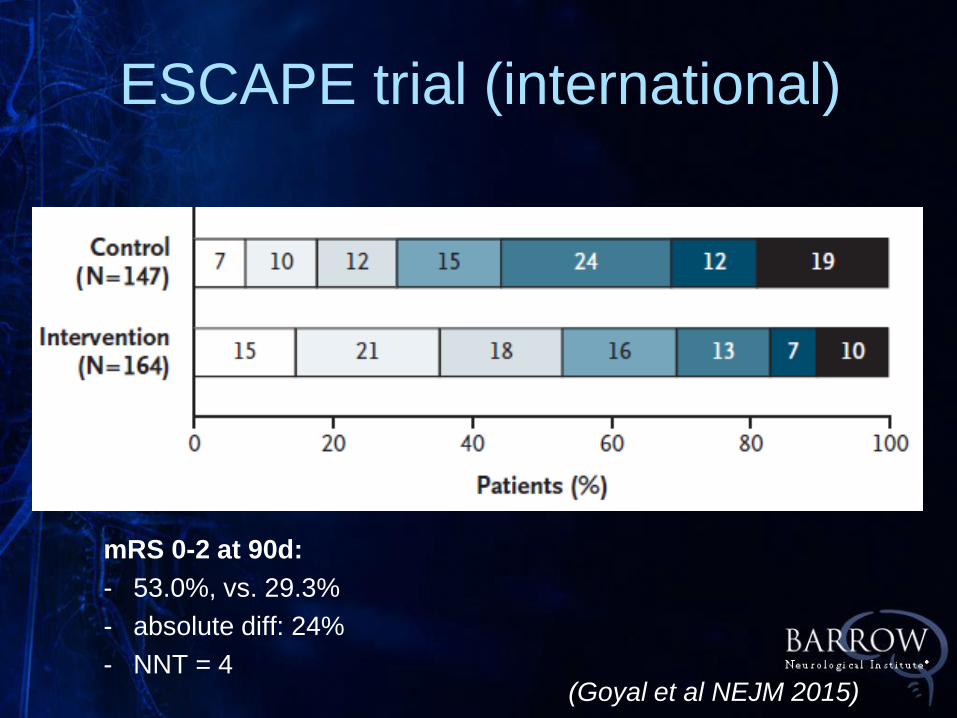
(Goyal et al NEJM 2015)
mRS 0-2 at 90d:
- 53.0%, vs. 29.3%
- absolute diff: 24%
- NNT = 4
ESCAPE trial (international)
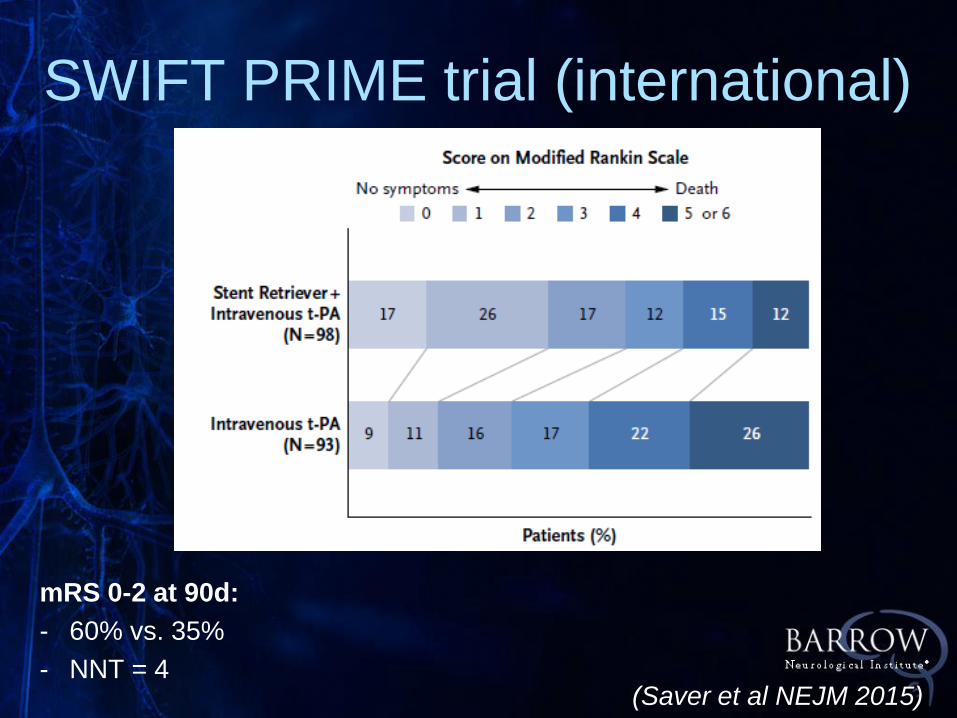
SWIFT PRIME trial (international)
(Saver et al NEJM 2015)
mRS 0-2 at 90d:
- 60% vs. 35%
- NNT = 4
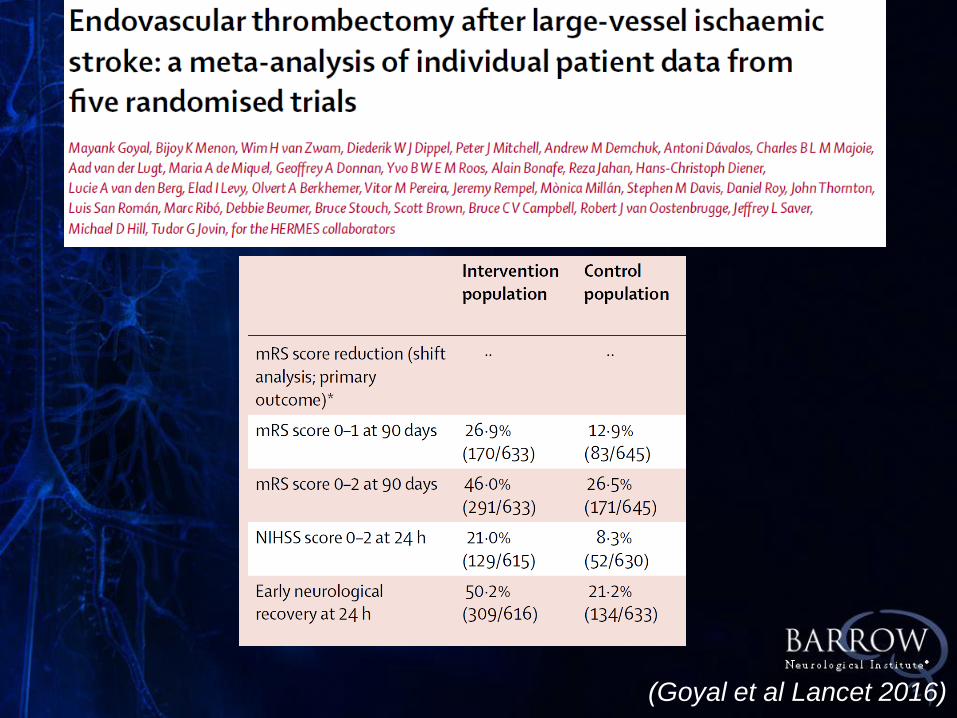
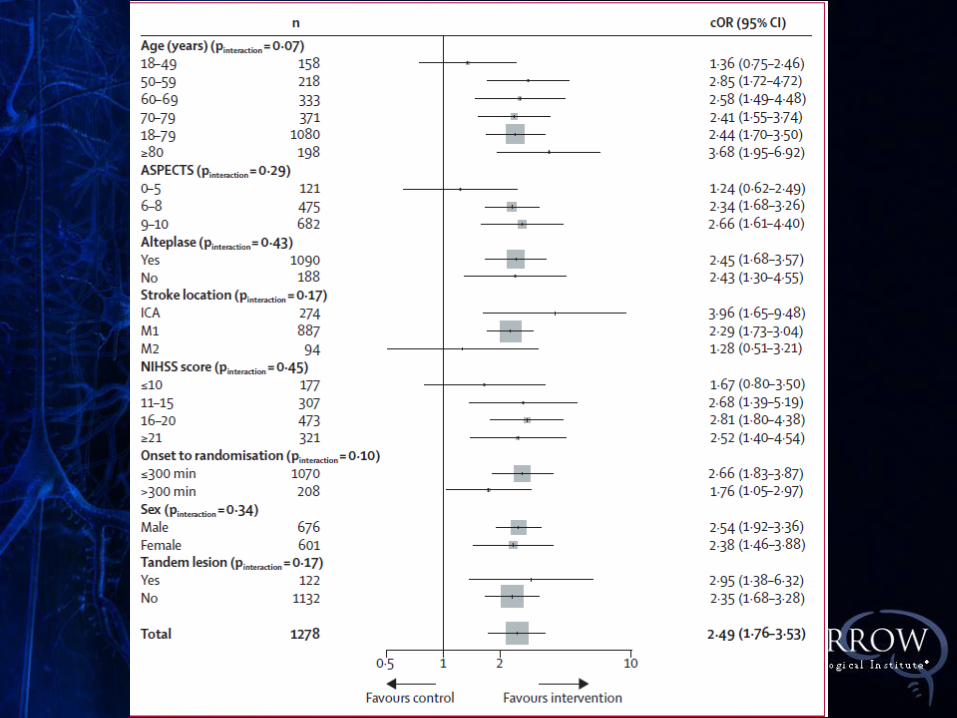
(Goyal et al Lancet 2016)
BNI Vascular Neurology

BESTU: October 2017
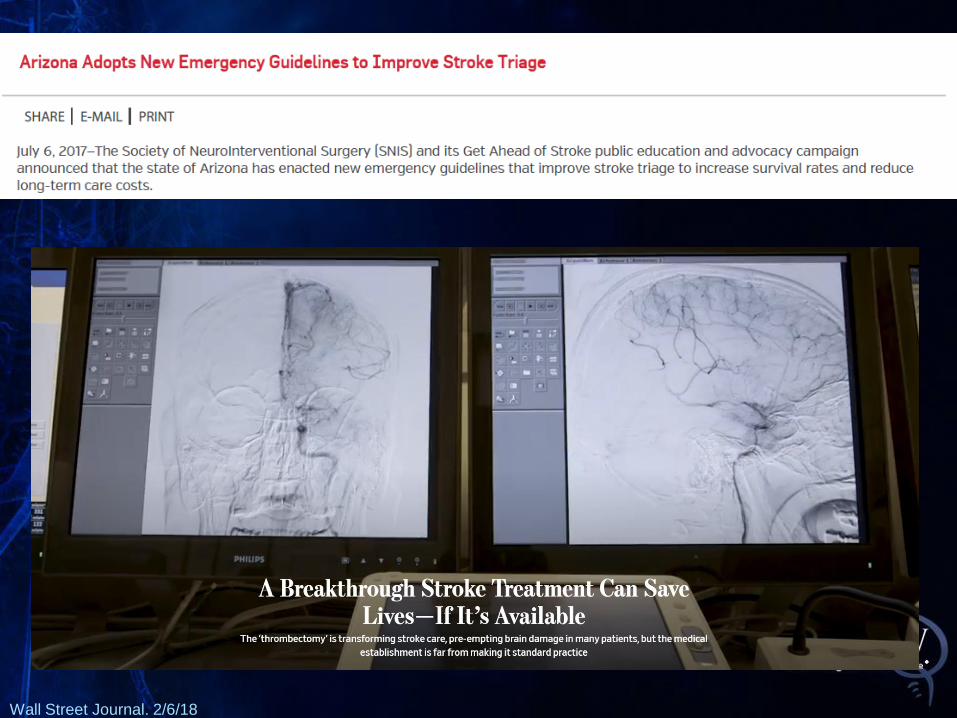
Wall Street Journal. 2/6/18
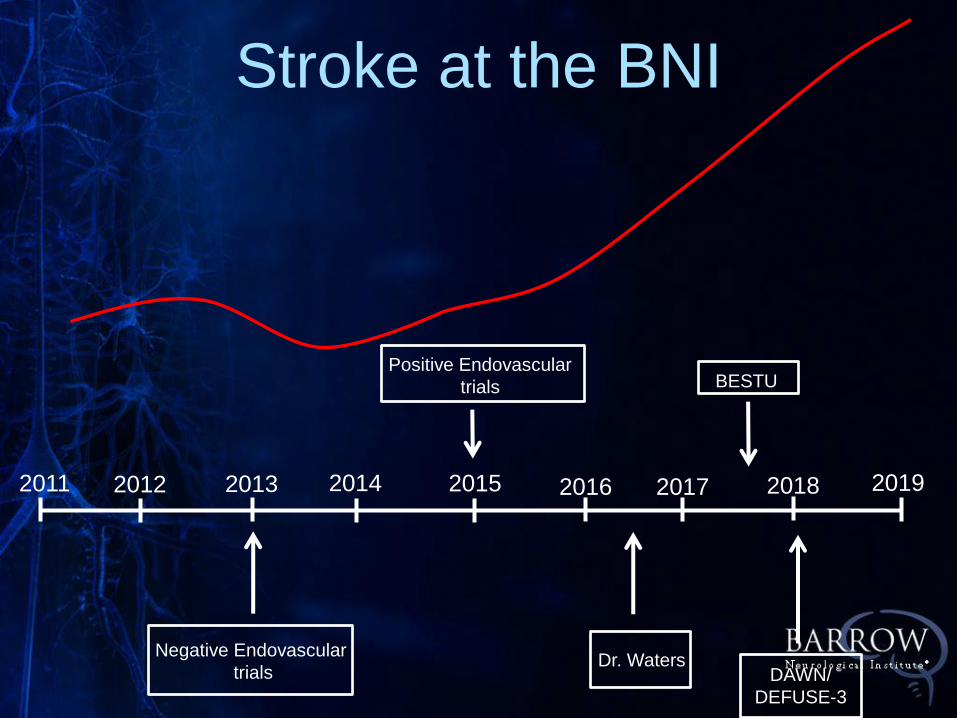
Stroke at the BNI
Positive Endovascular
trials
2011 2015 2014 2013 2012 2017 2016 2019
Negative Endovascular
trials
2018
BESTU
DAWN/
DEFUSE-3
Dr. Waters
Endovascular Stroke
Treatment in 2018:
Techniques
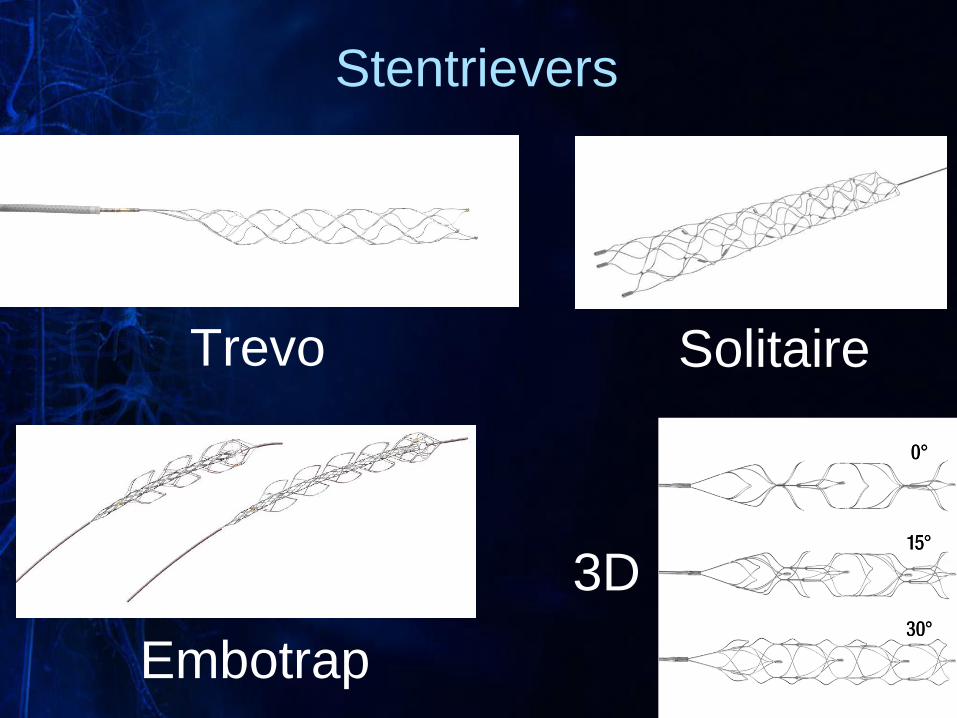
Stentrievers
Trevo Solitaire
Embotrap
3D
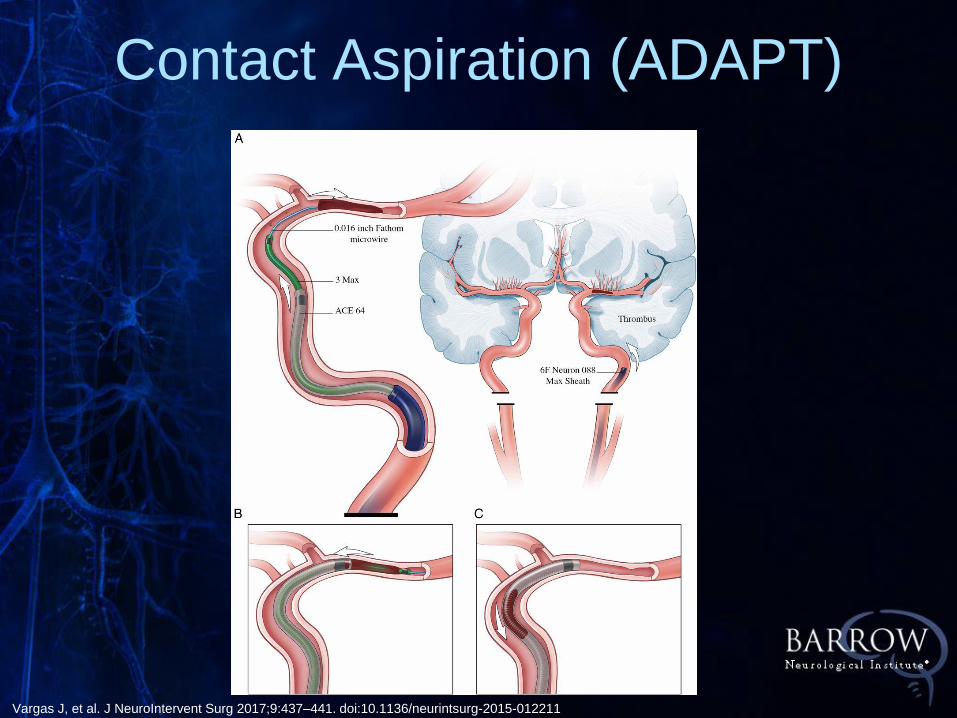
Contact Aspiration (ADAPT)
Vargas J, et al. J NeuroIntervent Surg 2017;9:437–441. doi:10.1136/neurintsurg-2015-012211
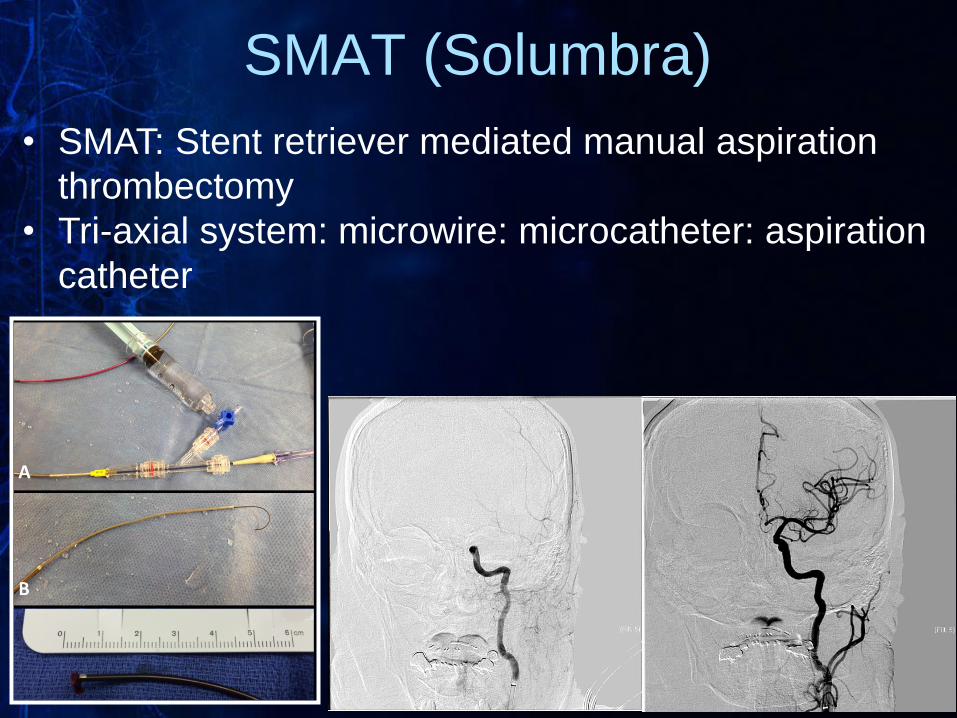
• SMAT: Stent retriever mediated manual aspiration
thrombectomy
• Tri-axial system: microwire: microcatheter: aspiration
catheter
SMAT (Solumbra)

Recent Endovascular Stroke
Clinical Trials
DAWN Trial
N Engl J Med. 2018 Jan 4;378(1):11-21.
• 500 patients (pivotal); 50 sites
• 6-24 hours
• NIHSS > 9
• ICA or M1 occlusion
• Medical therapy vs. thrombectomy (Trevo)
DAWN Trial
N Engl J Med. 2018 Jan 4;378(1):11-21.
• Clinical Imaging Mismatch (CIM)
• Core defined on DWI or rCBF maps
(RAPID)
• 0-20 cc core & NIHSS >= 10 (≥ 80yr)
• 0-30 cc core & NIHSS >= 10 (< 80yr)
• 31-50 cc core & NIHSS ≥ 20 (< 80yr)
DAWN Trial
N Engl J Med. 2018 Jan 4;378(1):11-21.
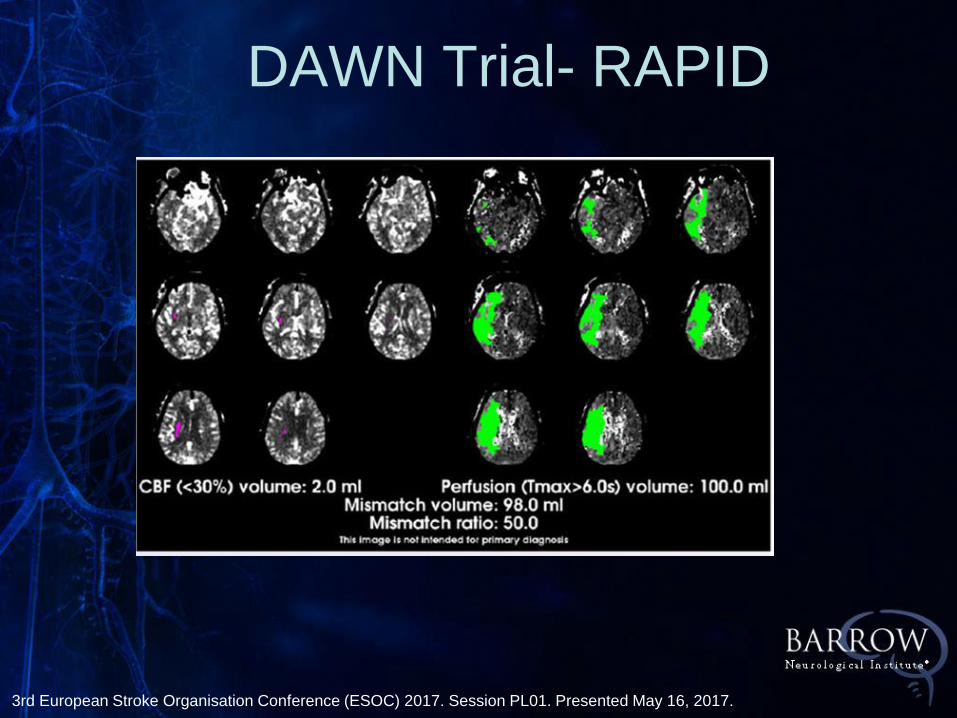
3rd European Stroke Organisation Conference (ESOC) 2017. Session PL01. Presented May 16, 2017.
DAWN Trial- RAPID
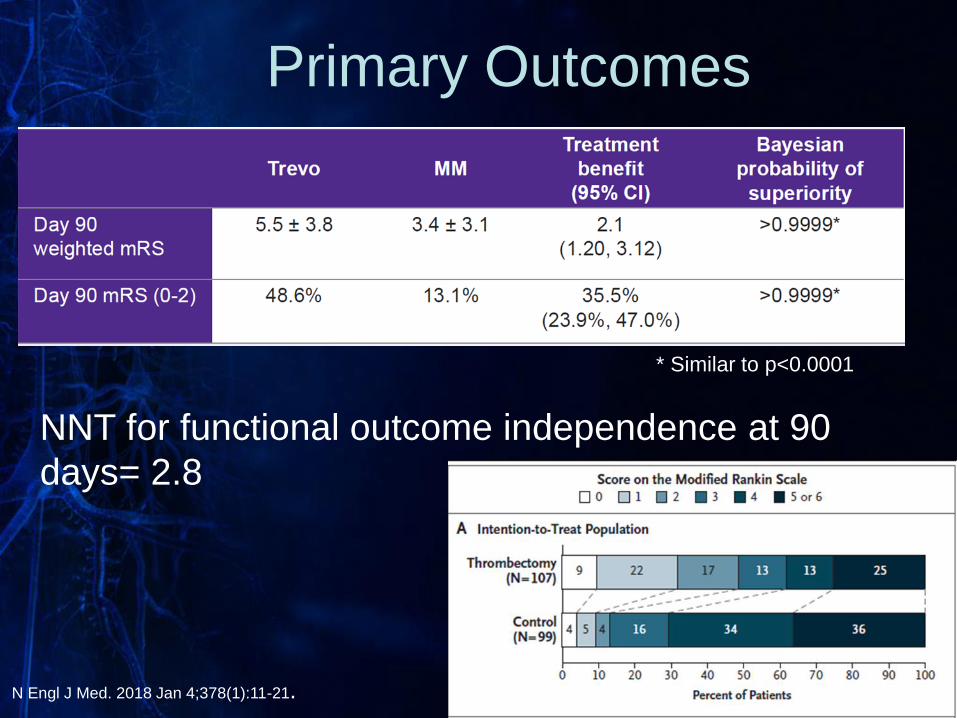
Primary Outcomes
NNT for functional outcome independence at 90
days= 2.8
* Similar to p<0.0001
N Engl J Med. 2018 Jan 4;378(1):11-21.
DAWN Trial Conclusions
• Thrombectomy associated with higher
functional independence compared to
medical therapy
• Treatment effect size in DAWN is highest
of any stroke trial
• Thrombectomy in patients > 6h showed
comparable safety profile to thrombectomy
performed < 6h
DEFUSE-3
N Engl J Med. 2018 Feb 22;378(8):708-718.
DEFUSE-3 Design
• Age 18-90 years
• ICA or M1 occlusion
• Treatment between 6-16 hours last known
well
• NIHSS ≥6
• Perfusion imaging required
• Initial infarct volume <70cc • Ratio of ischemic tissue to infarct of >1.8
• Absolute value of penumbra of >15cc
• Any FDA-approved thrombectomy device
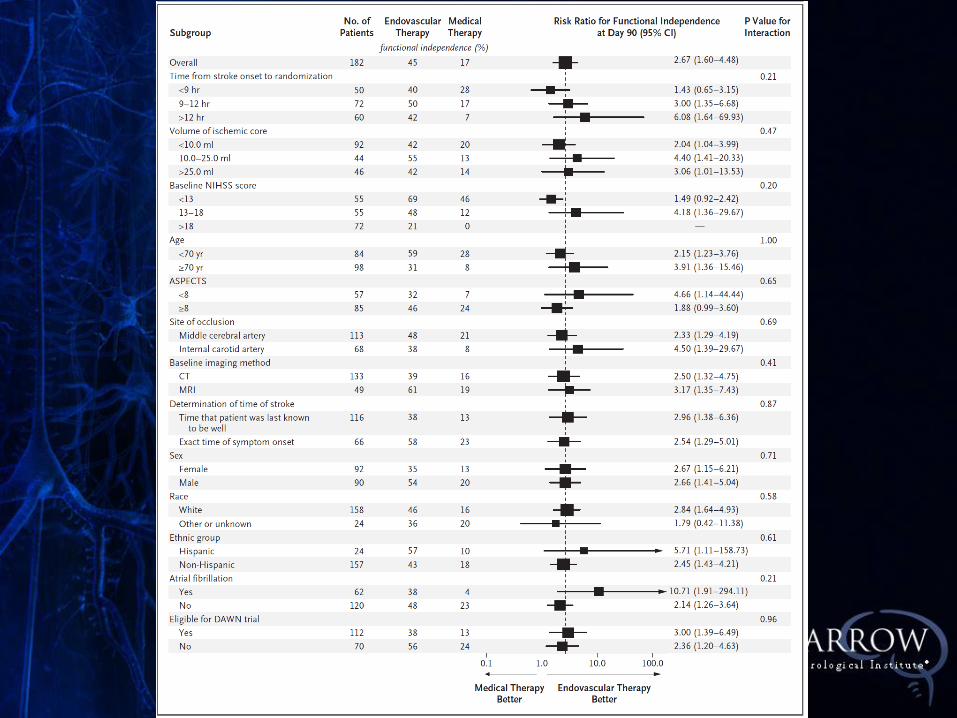
N Engl J Med. 2018 Feb 22;378(8):708-718.
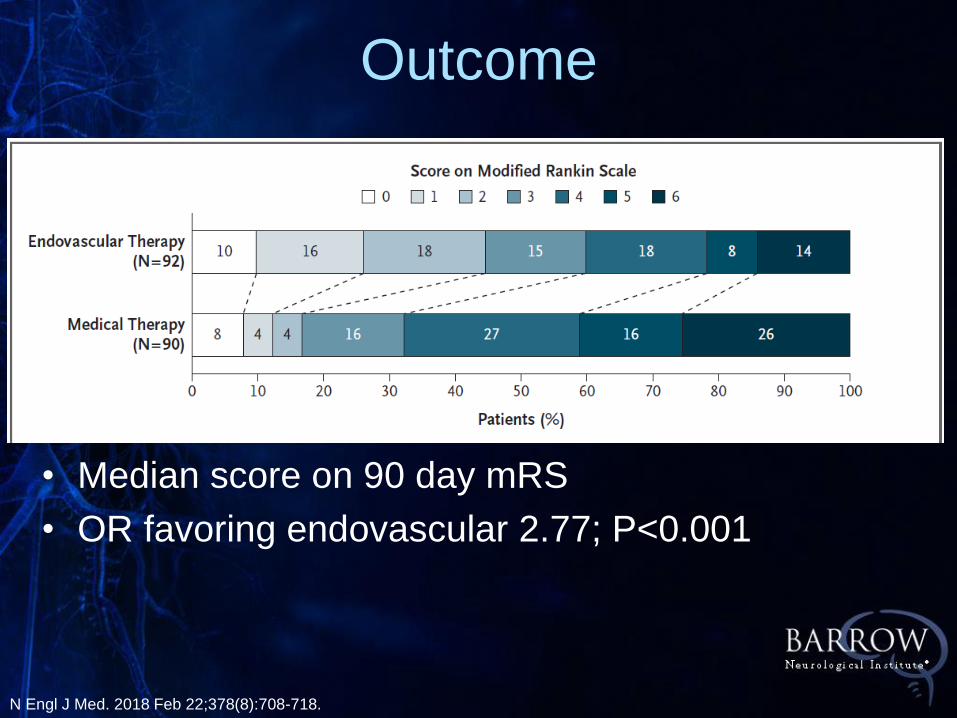
• Median score on 90 day mRS
• OR favoring endovascular 2.77; P<0.001
Outcome
N Engl J Med. 2018 Feb 22;378(8):708-718.
DEFUSE-3 Findings
• More inclusive than DAWN
• 40% of DEFUSE patients would not
qualify for DAWN
• Larger Core infarcts than DAWN
(70 vs. 50)
• Milder Symptoms (NIHSS ≥ 6)
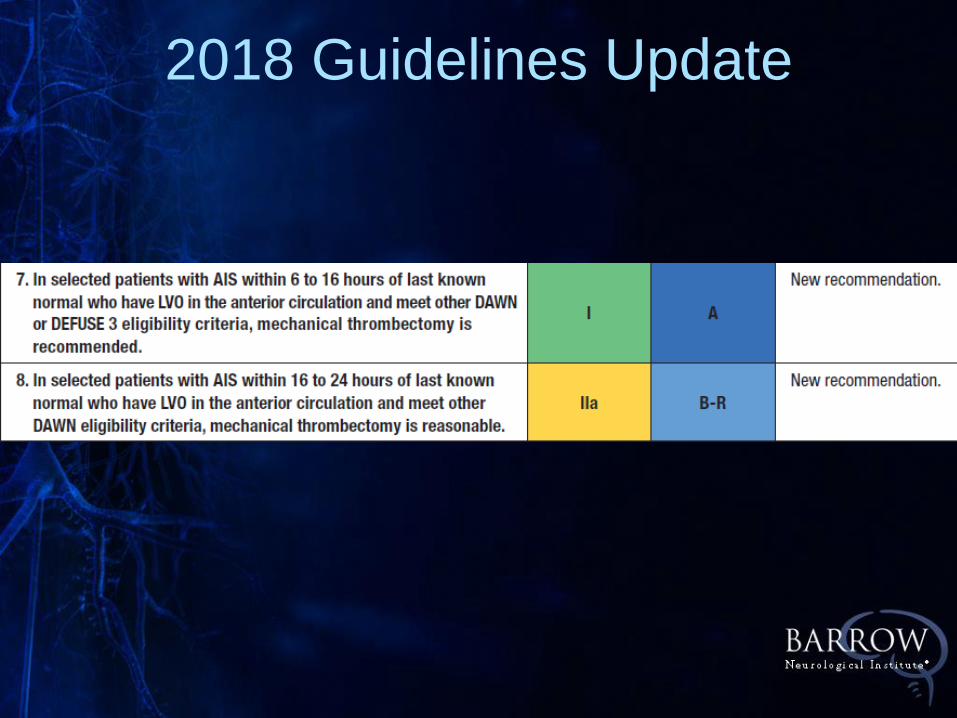
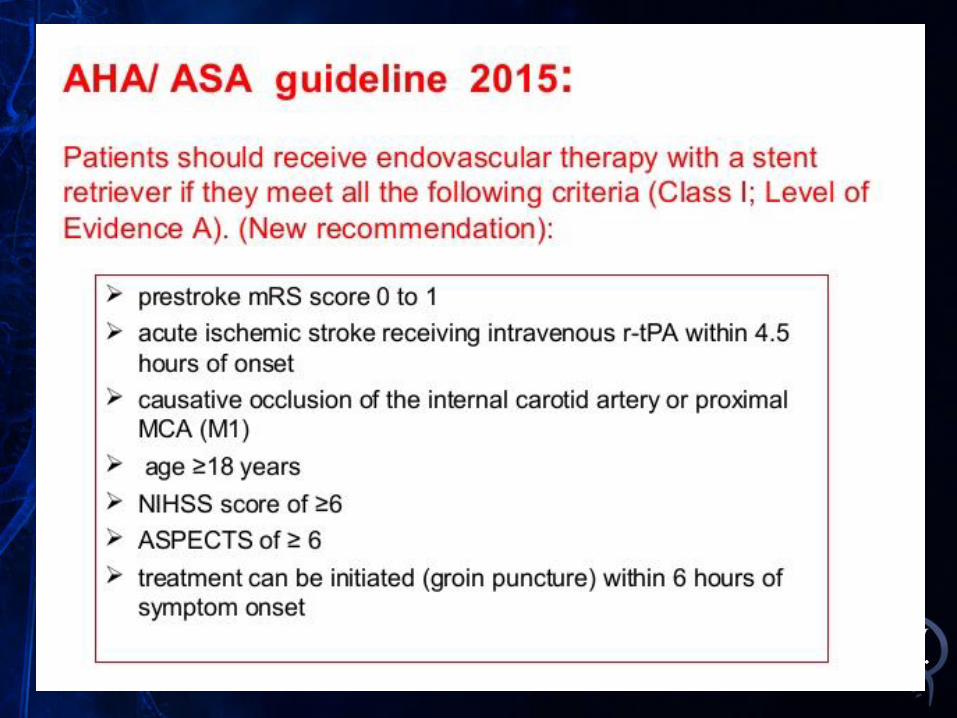
2018 Guidelines Update
Aspiration vs. Stentriever
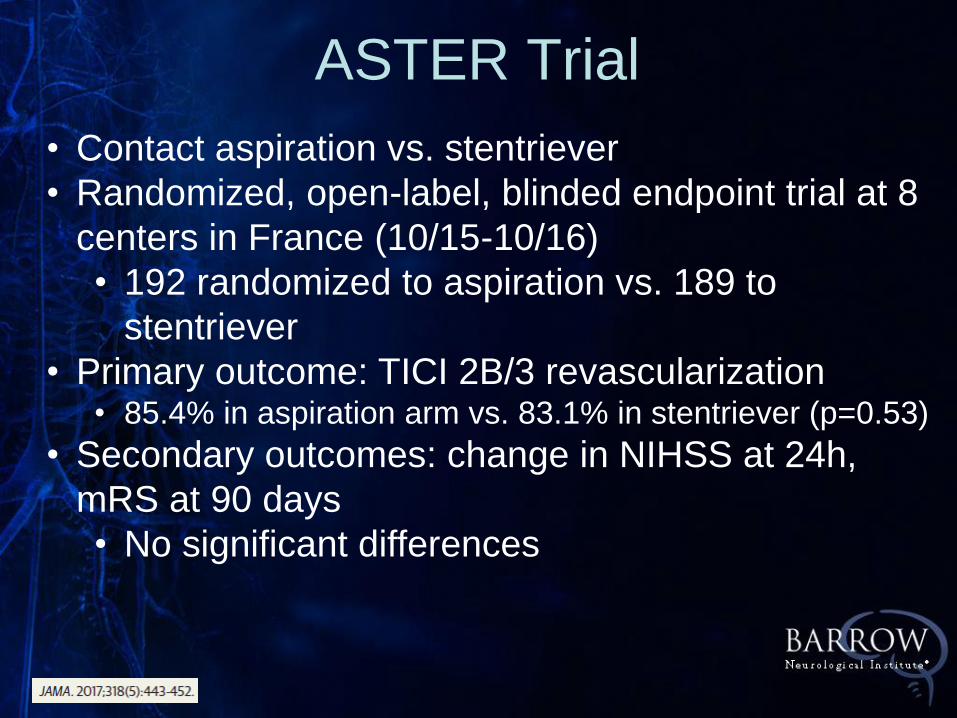
• Contact aspiration vs. stentriever
• Randomized, open-label, blinded endpoint trial at 8
centers in France (10/15-10/16)
• 192 randomized to aspiration vs. 189 to
stentriever
• Primary outcome: TICI 2B/3 revascularization • 85.4% in aspiration arm vs. 83.1% in stentriever (p=0.53)
• Secondary outcomes: change in NIHSS at 24h,
mRS at 90 days
• No significant differences
ASTER Trial
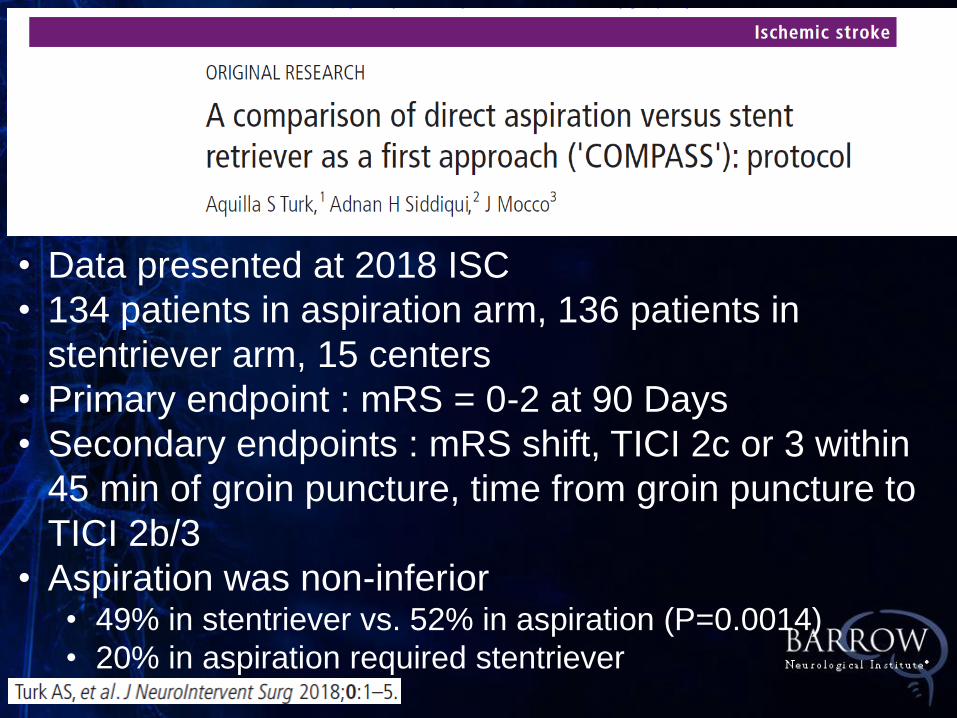
• Data presented at 2018 ISC
• 134 patients in aspiration arm, 136 patients in
stentriever arm, 15 centers
• Primary endpoint : mRS = 0-2 at 90 Days
• Secondary endpoints : mRS shift, TICI 2c or 3 within
45 min of groin puncture, time from groin puncture to
TICI 2b/3
• Aspiration was non-inferior • 49% in stentriever vs. 52% in aspiration (P=0.0014)
• 20% in aspiration required stentriever
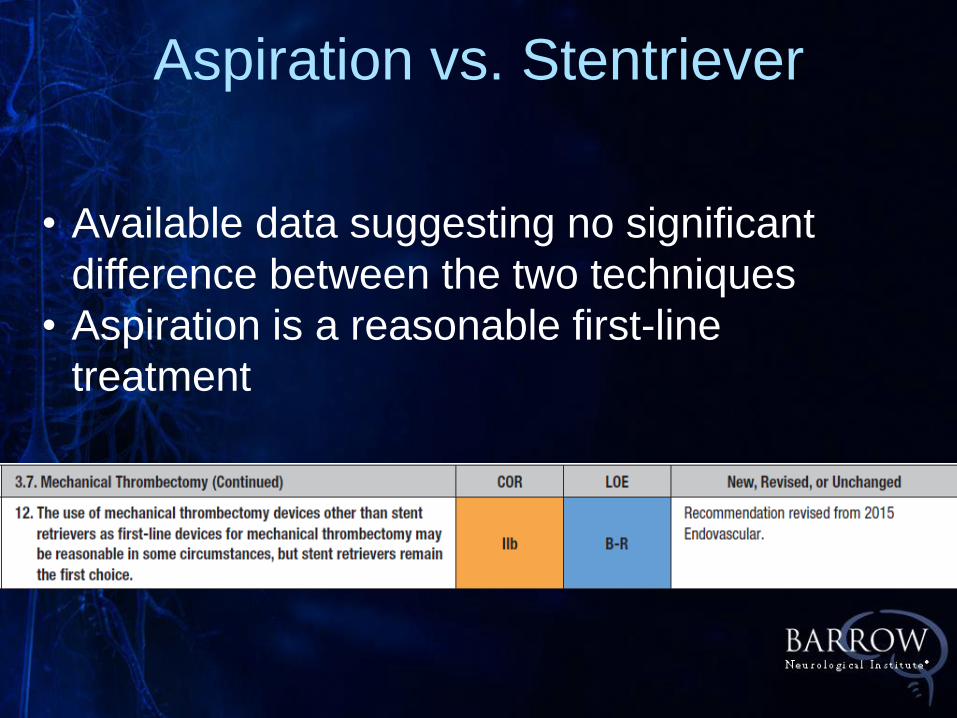
Aspiration vs. Stentriever
• Available data suggesting no significant
difference between the two techniques
• Aspiration is a reasonable first-line
treatment

The Future
• Larger Core infarcts
• Low NIHSS
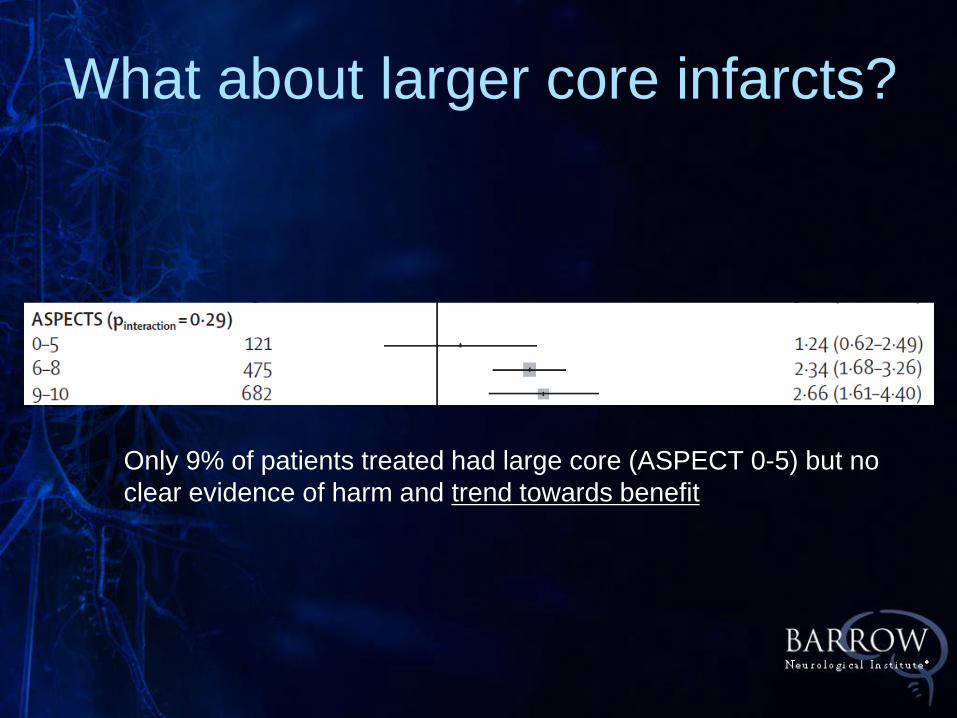
What about larger core infarcts?
Only 9% of patients treated had large core (ASPECT 0-5) but no
clear evidence of harm and trend towards benefit
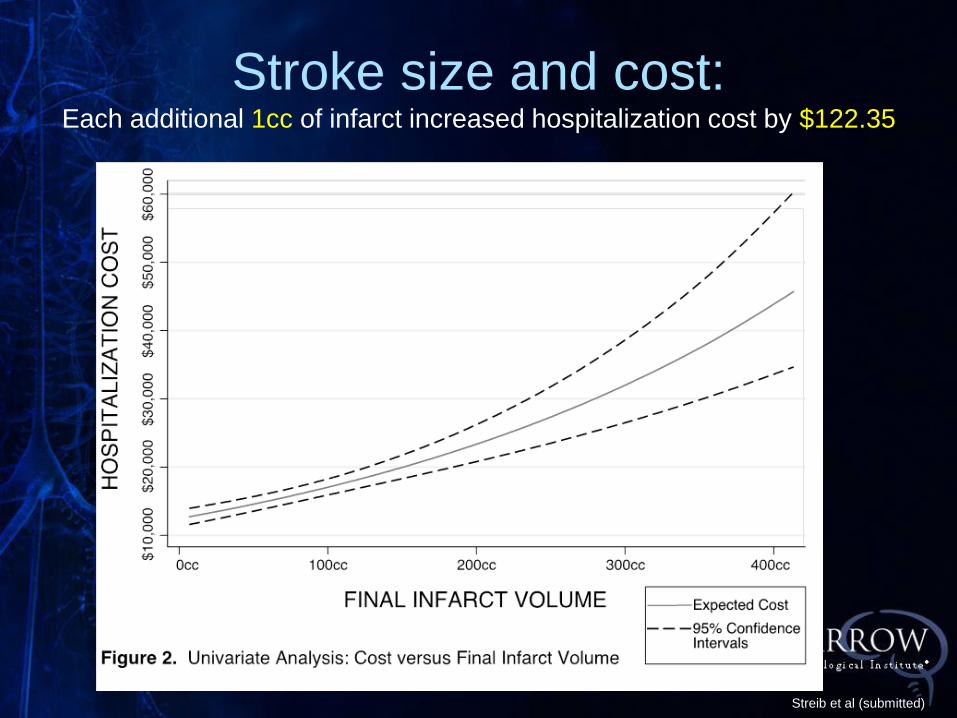
Stroke size and cost: Each additional 1cc of infarct increased hospitalization cost by $122.35
Streib et al (submitted)
Case 1: Large Core Infarct
• 37 year old male last known well 14-16
hours prior to admission, with history of
altercation at a party
• Awoke with right MCA syndrome
• NIHSS = 19
• CTA shows tandem occlusion right
MCA/ICA
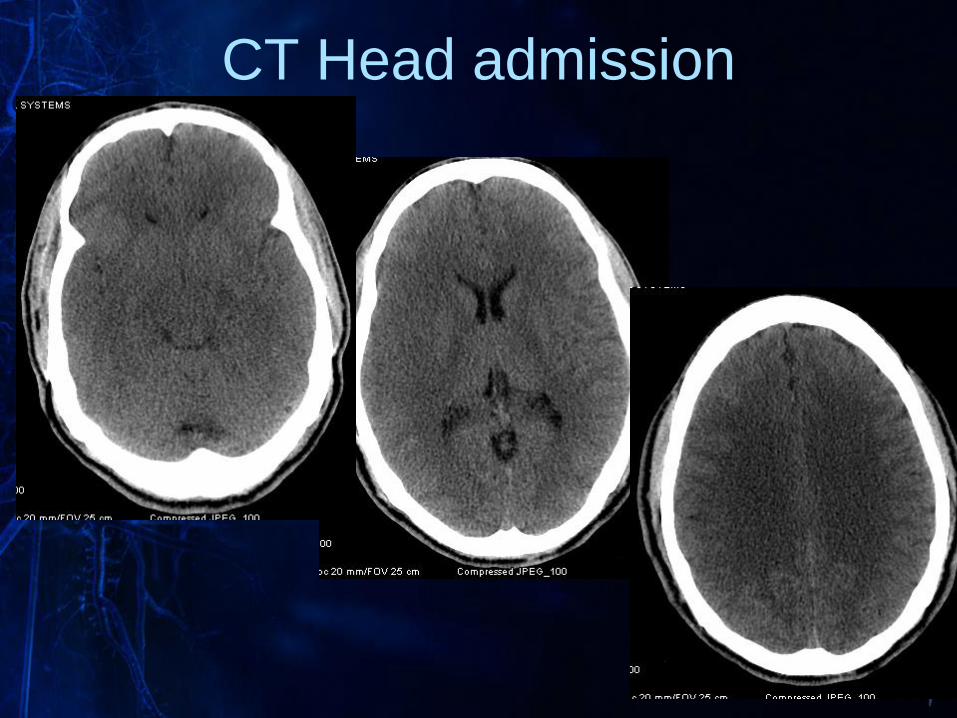
CT Head admission
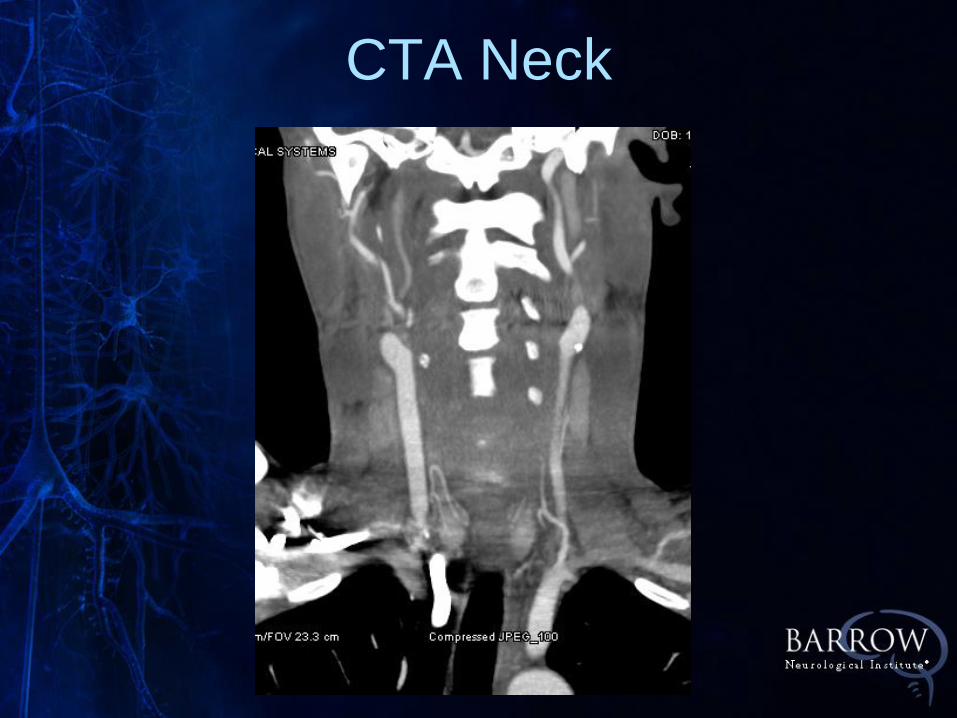
CTA Neck
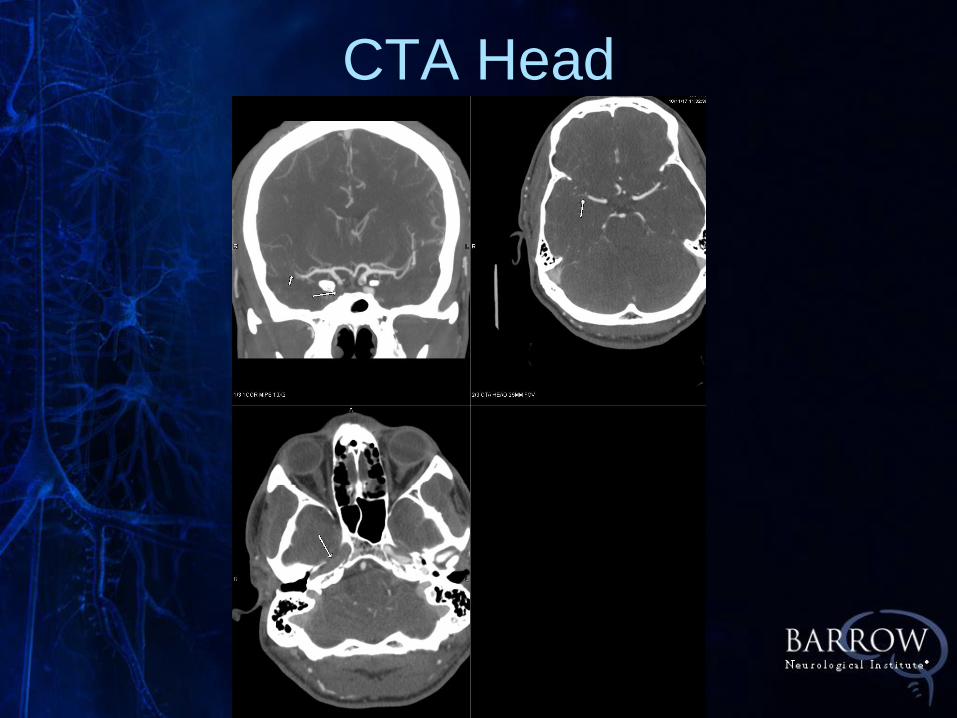
CTA Head
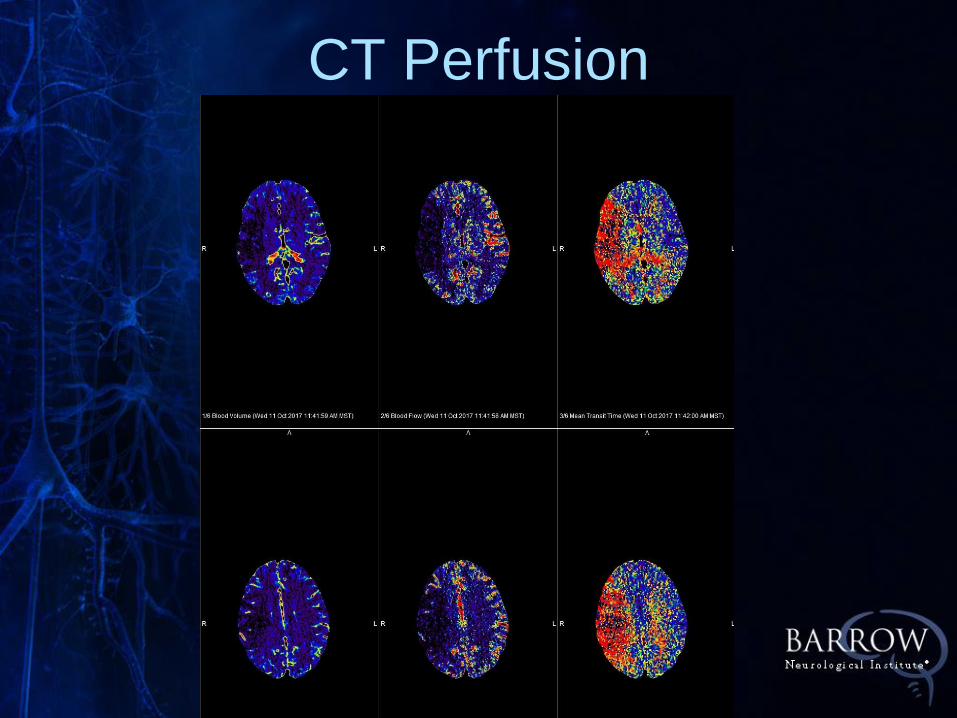
CT Perfusion
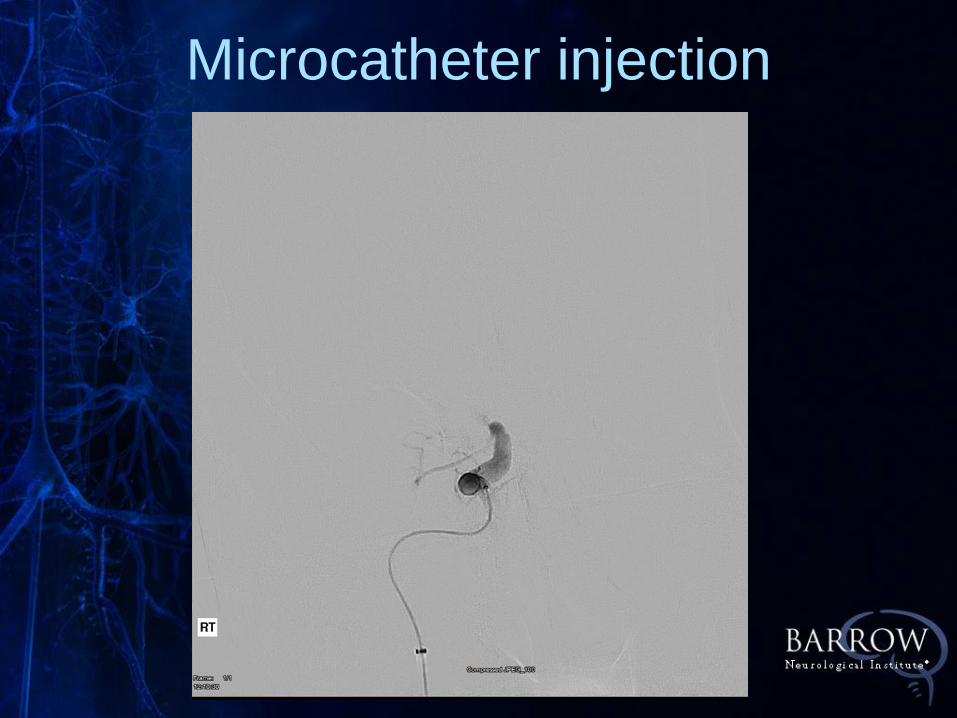
Microcatheter injection
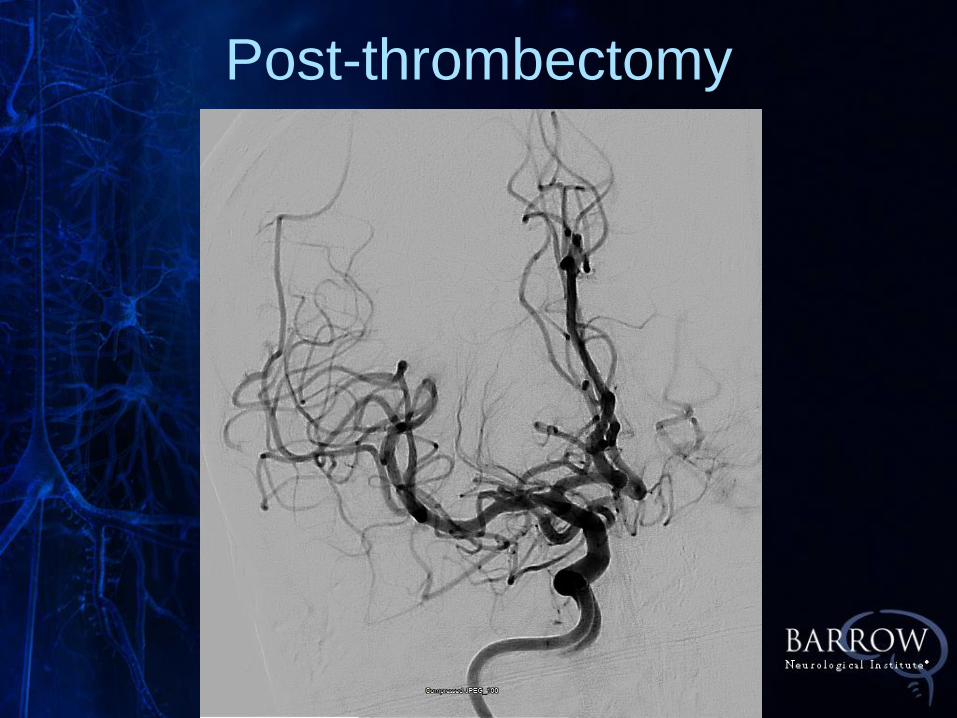
Post-thrombectomy
Post-Thrombectomy MRI
• Showed rapid improvement over next
several days
• Discharged on day 5 intact except
4+/5 in left hand
• Lost to follow-up
Case #1
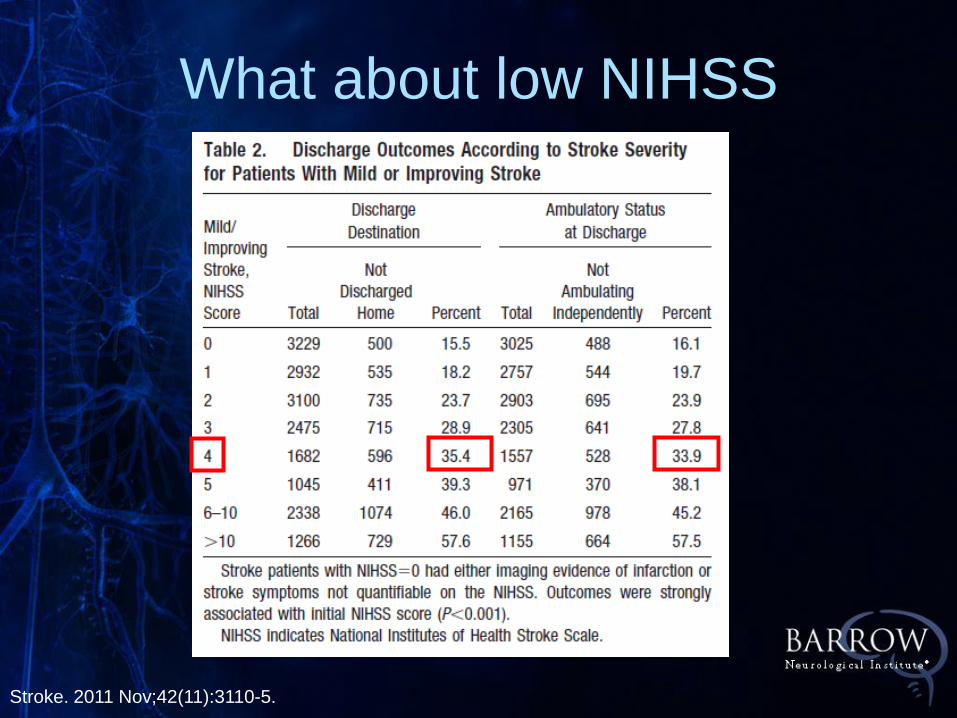
What about low NIHSS
Stroke. 2011 Nov;42(11):3110-5.
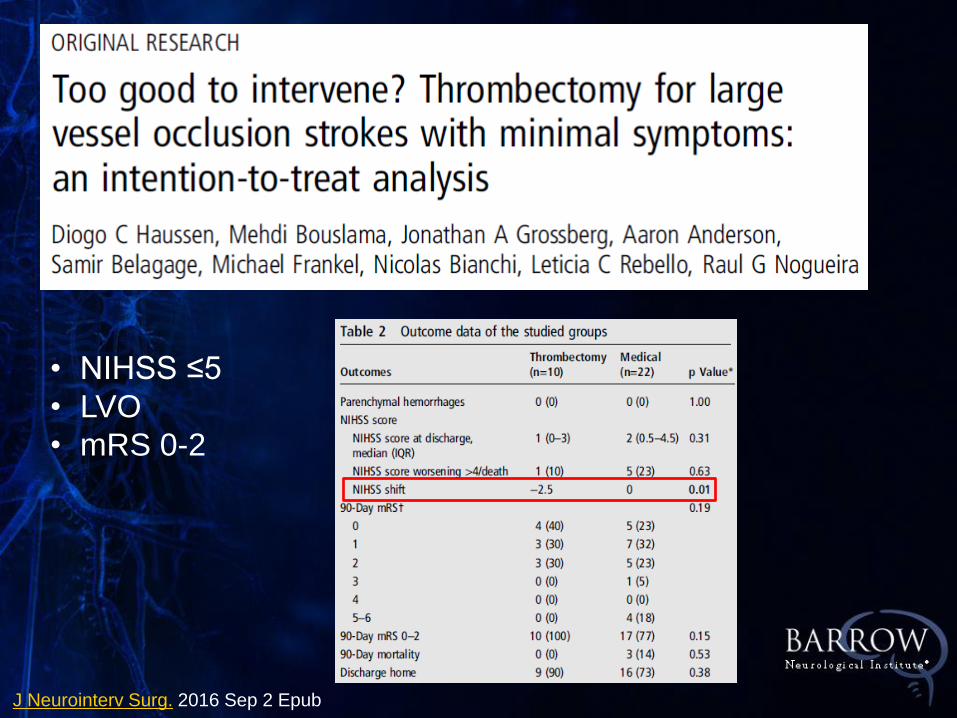
J Neurointerv Surg. 2016 Sep 2 Epub
• NIHSS ≤5
• LVO
• mRS 0-2
• 52 yo male with hypertension
• Onset of facial droop, slurred speech
mild left sided drift at work
• Urgicare ER
• 9.5 hours post-onset
• NIHSS = 4
Case #2: Low NIHSS
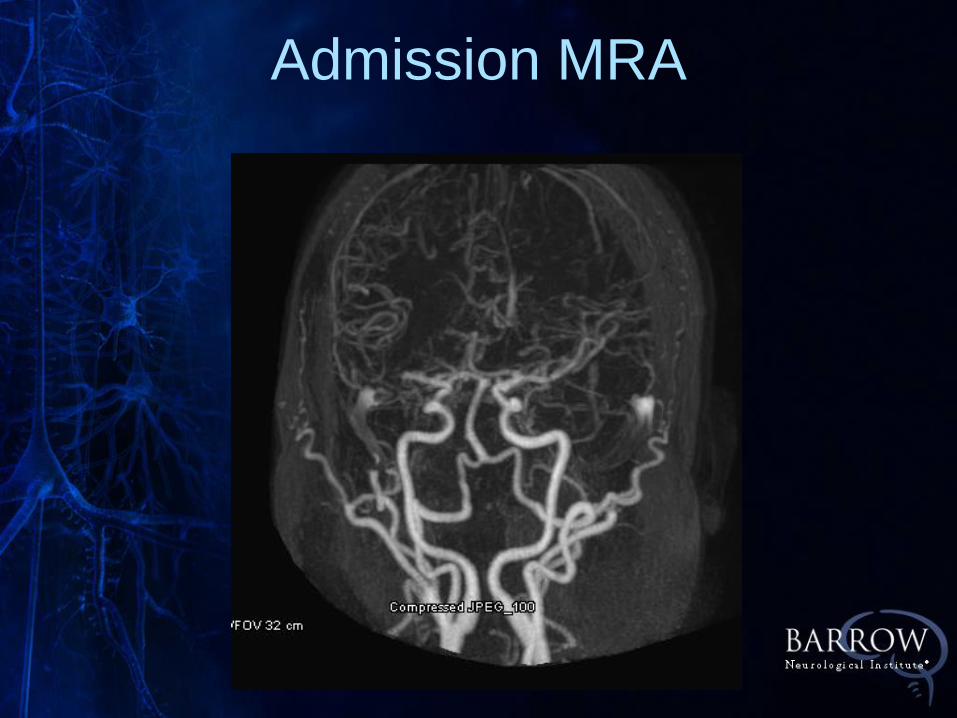
Admission MRA
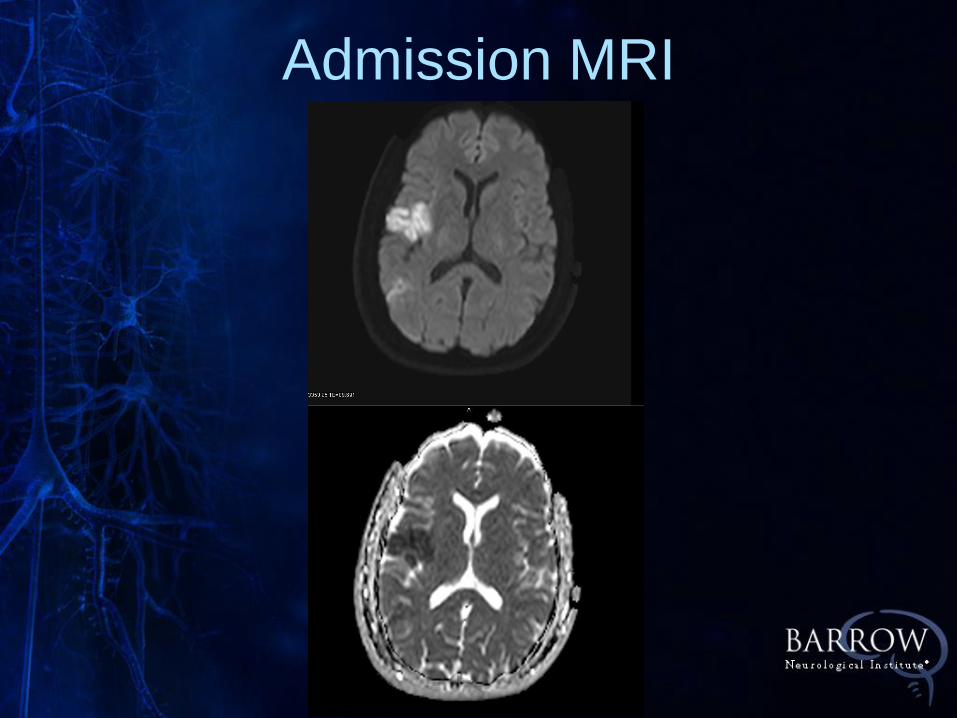
Admission MRI
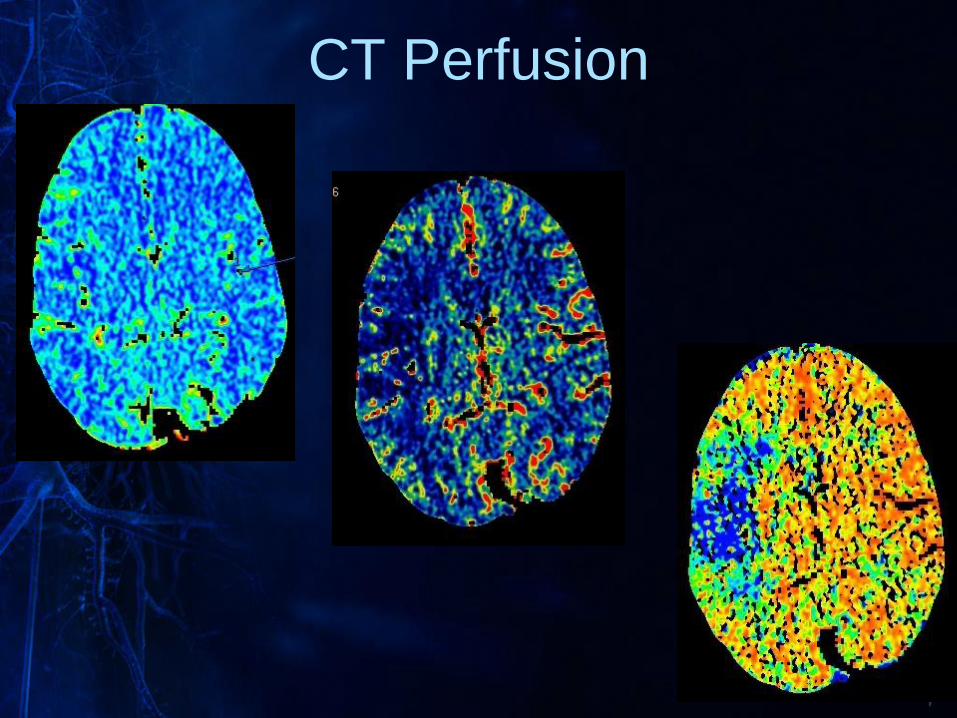
CT Perfusion
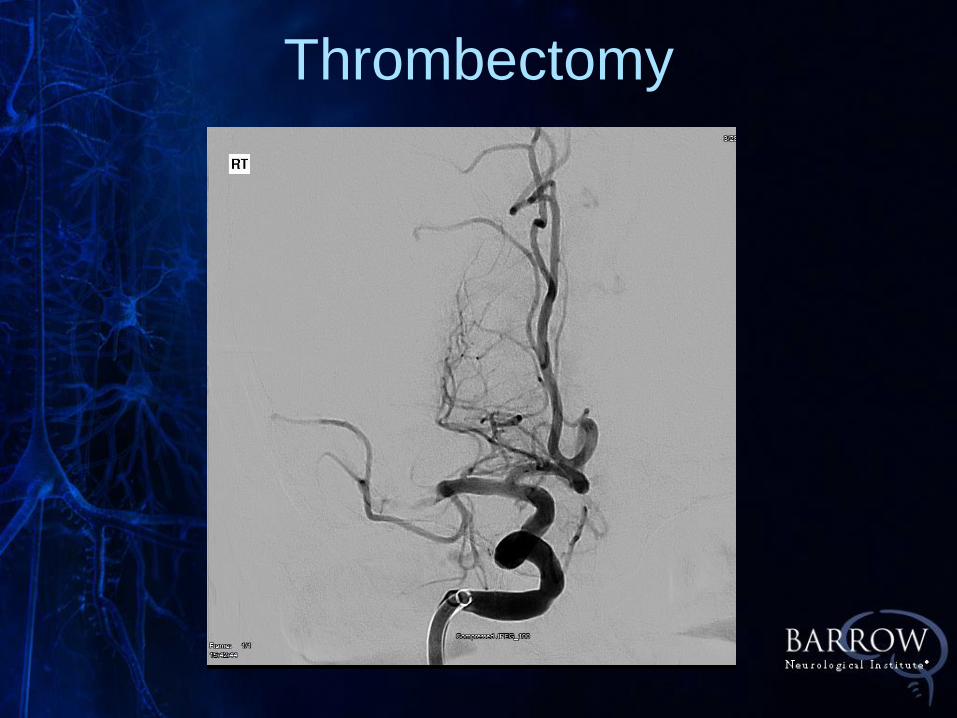
Thrombectomy
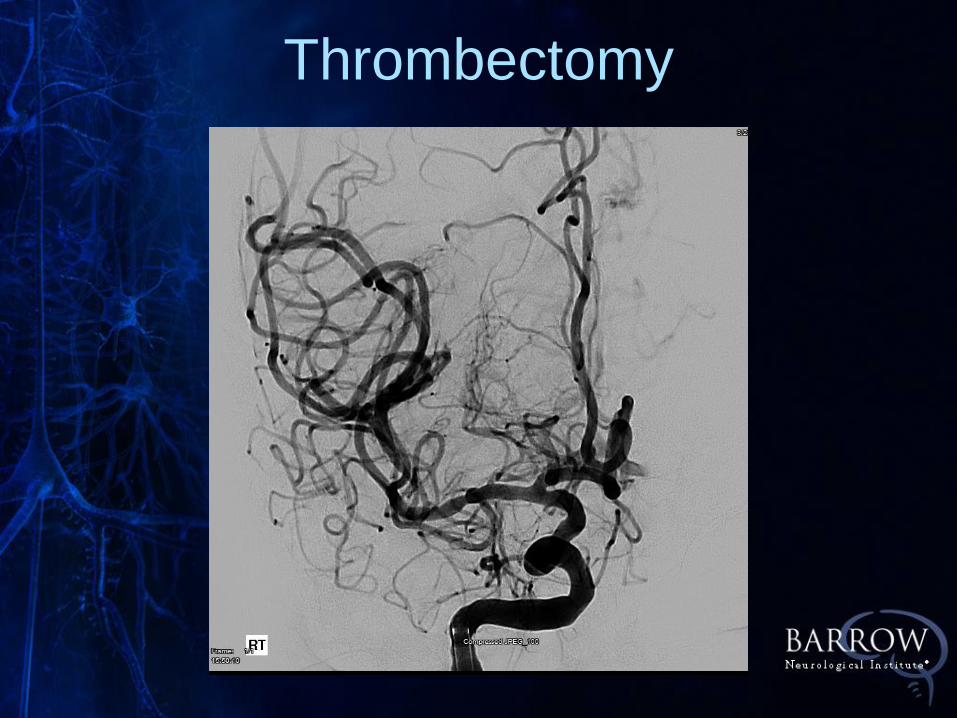
Thrombectomy
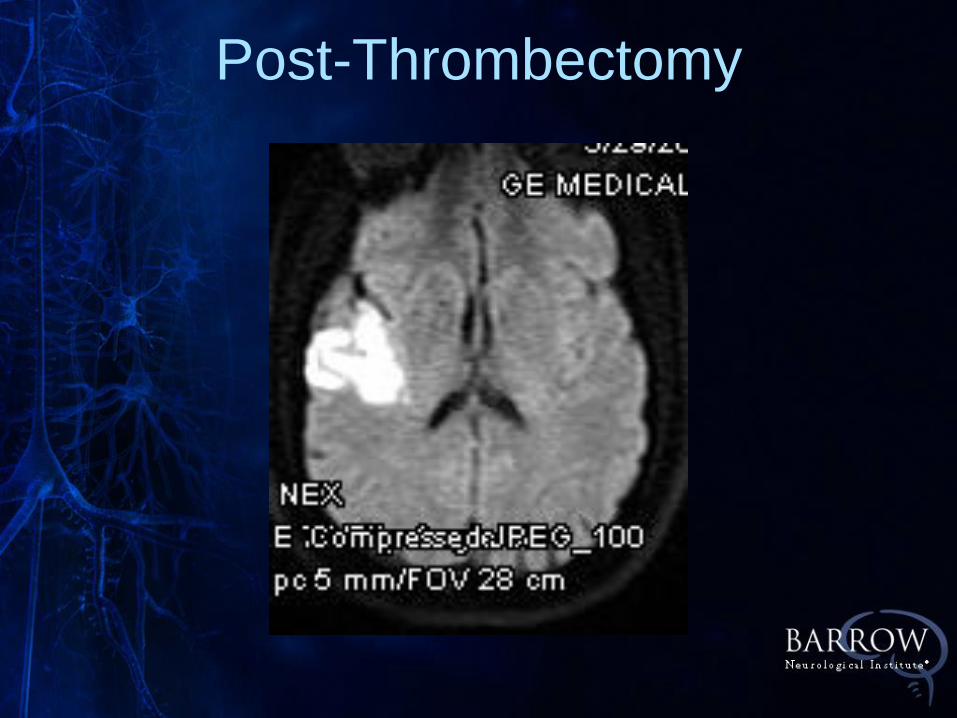
Post-Thrombectomy
• Immediate improvement of drift and
facial ,speech rapidly normalized
• Discharged home neurologically
intact following workup for AFib
Case #2
• 44 yo otherwise healthy male
• Onset of dizziness, dysphagia,
left facial numbness beginning
on 7/25 in the afternoon
• In the ER, CT head normal,
NIHSS 0.
Case #3:Low NIHSS, Basilar
• Admitted to MGMC due to
difficulty with balance
• MRA and CTA suggestive of
proximal basilar occlusion
Case #3:Low NIHSS, Basilar
• On admission to SJHMC, he has
severe vertigo when sitting up
accompanied by nausea /vomiting,
lateral gaze nystagmus
• NIHSS = 0
Case #3
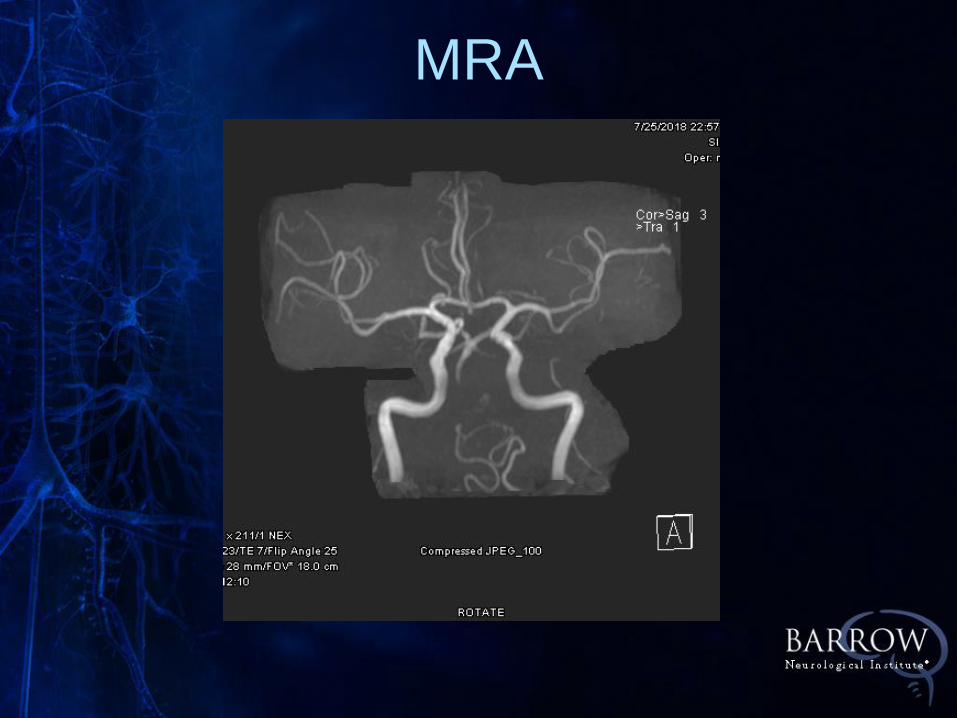
MRA
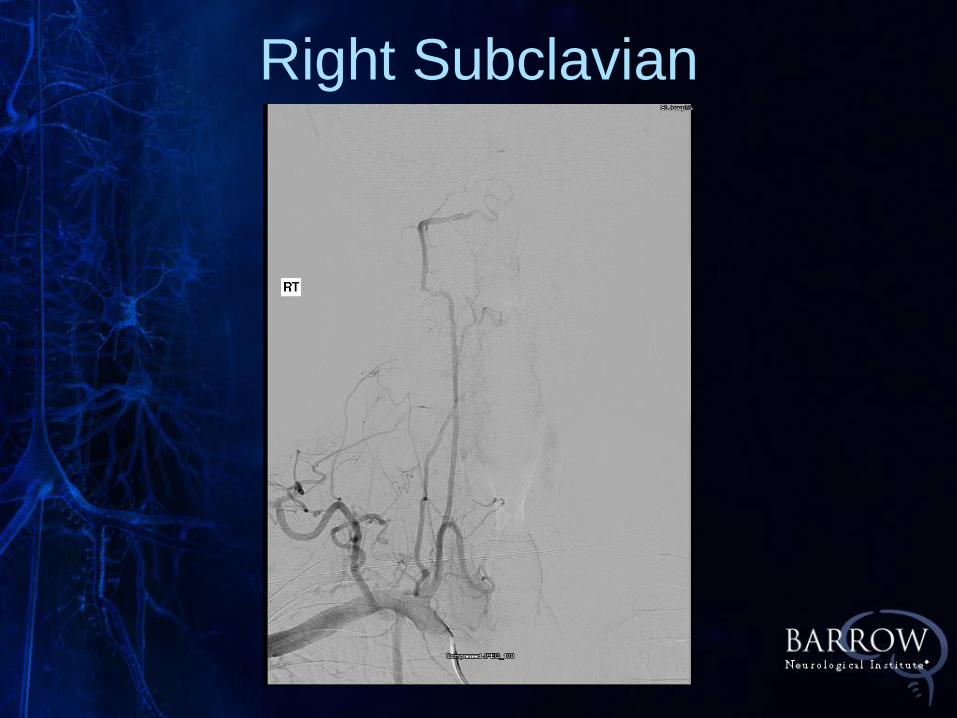
Right Subclavian
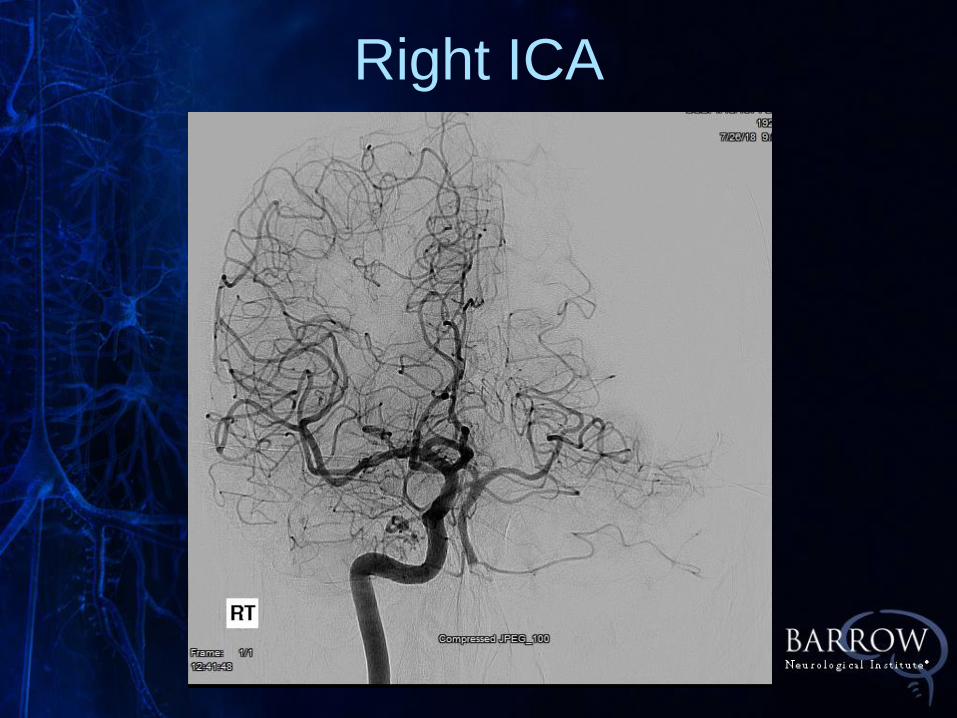
Right ICA
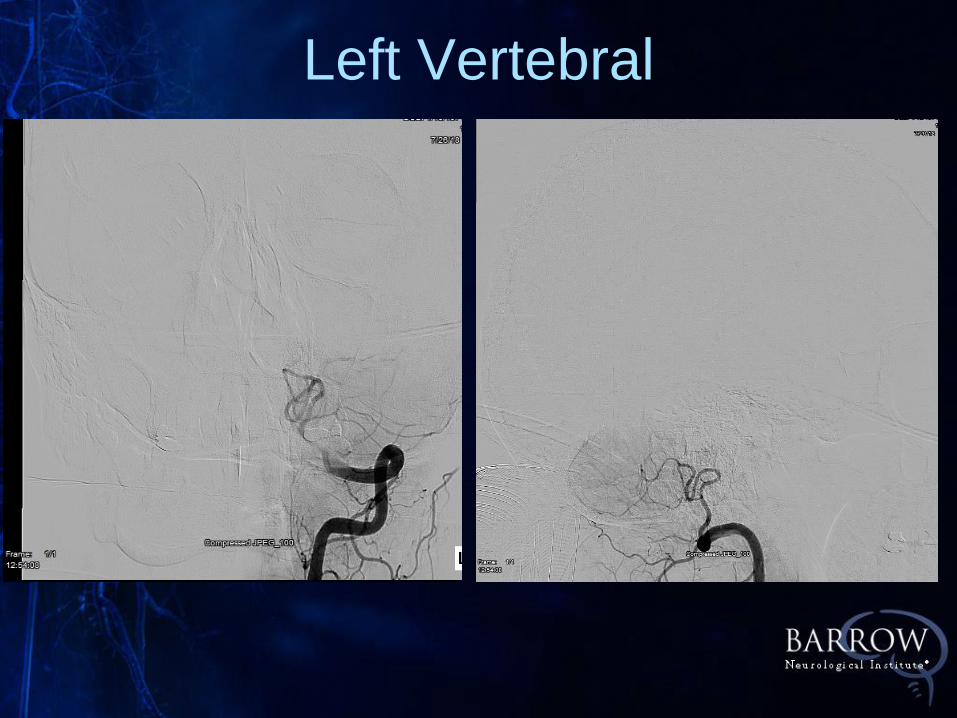
Left Vertebral
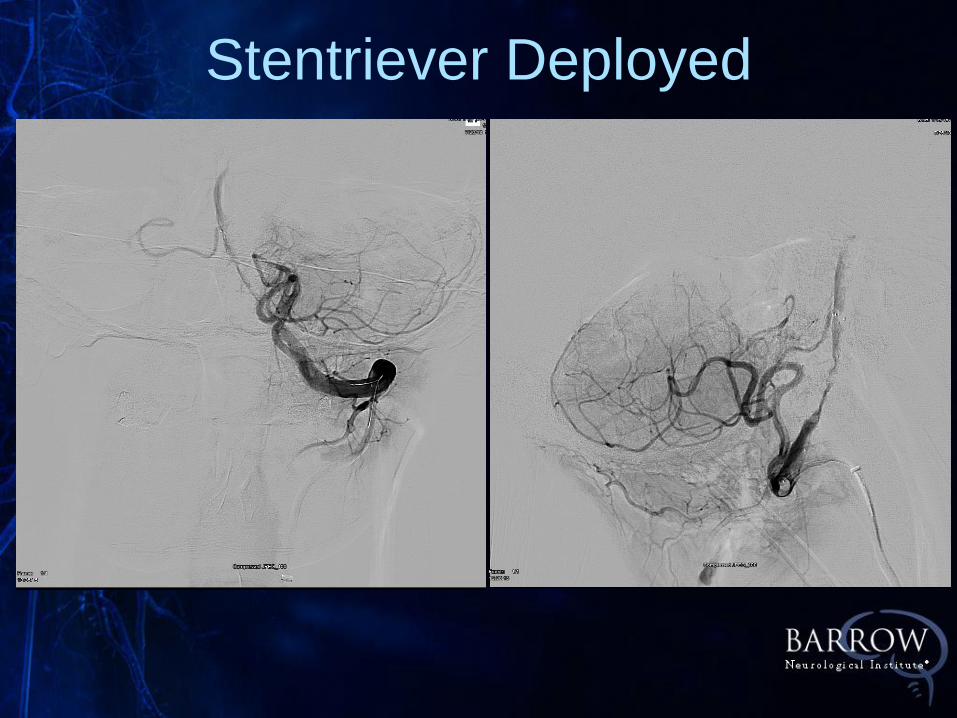
Stentriever Deployed
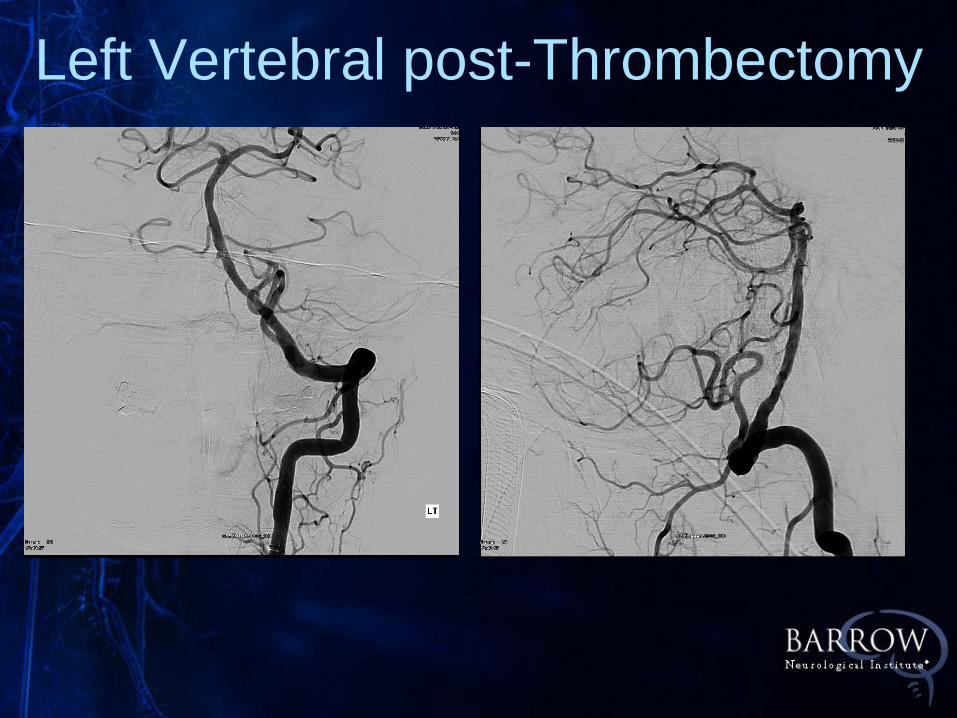
Left Vertebral post-Thrombectomy
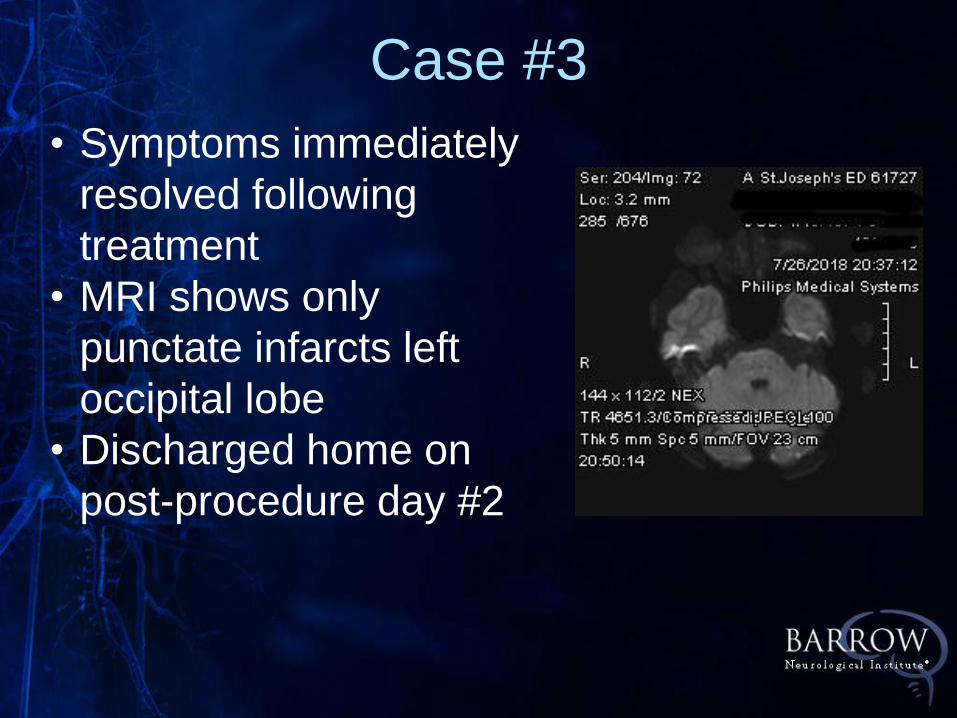
• Symptoms immediately
resolved following
treatment
• MRI shows only
punctate infarcts left
occipital lobe
• Discharged home on
post-procedure day #2
Case #3
Future Directions
• IN EXTREMIS: Montpelier
• Clinically severe stroke and
ASPECTS 0-5
• Low NIHSS (<6) and M1 occlusion