Embed Size (px)
Citation preview

British Journal of Industrial Medicine 1991;48:258-266
Neurological long term consequences of deep diving
K Todnem, H Nyland, H Skeidsvoll, R Svihus, P Rinck, B K Kambestad, T Riise, J A Aarli
AbstractForty commercial saturation divers, mean age34-9 (range 24-49) years, were examined one toseven years after their last deep dive (190-500metres of seawater). Four had by then losttheir divers' licence because of neurologicalproblems. Twenty seven (68%) had been selec-ted by neurological examination and electro-encephalography before the deep dives. Thecontrol group consisted of 100 men, mean age34 0 (range 22-48) years. The divers reportedsignificantly more symptoms from thenervous system. Concentration difficulties andparaesthesia in feet and hands were common.They had more abnormal neurological find-ings by neurological examination compatiblewith dysfunction in the lumbar spinal cord orroots. They also had a larger proportion ofabnormal electroencephalograms than thecontrols. The neurological symptoms andfindings were highly significantly correlatedwith exposure to deep diving (depth included),but even more significantly correlated to airand saturation diving and prevalence ofdecompression sickness. Visual evoked poten-tials, brainstem auditory evoked potentials,and magnetic resonance imaging of the braindid not show more abnormal findings in thedivers. Four (10%) divers had had episodes ofcerebral dysfunction during or after the dives;two had had seizures, one had had transitorycerebral ischaemia and one had had transitoryglobal amnesia. It is concluded that deep div-
Norwegian Underwater Technology Centre, BergenK Todnem, B K KambestadDepartment of Neurology, University ofBergenK Todnem, H Nyland, H Skeidsvoll, J A AarliDepartment of Radiology, Rogaland Central Hos-pital, StavangerR SvihusDepartment of Medical Technology, SINTEF,Trondheim and MR Centre, Medical Section,University ofTrondheimP RinckSection for Medical Informatics and Statistics,University of Bergen, NorwayT Riise
ing may have a long term effect on the nervoussystem of the divers.
Diving to below 180 metres of seawater (msw) hasbeen performed both as simulated onshore dives-for example, the Sagittaire and Atlantis series'-andas open sea dives. It has been concluded that diverscan be safely compressed to depths as great as 686metres of seawater (msw).' Since 1980 eightsimulated deep dives from 350 to 500 msw, corres-ponding to ambient pressures of 3 6 to 5 1 MPa, havebeen performed at the Norwegian Underwater Tech-nology Centre.The increased hyperbaric pressure influences the
nervous system during deep dives. The divers mayexperience hand tremor, postural instability, gastro-intestinal problems, somnolence, and cognitive dys-function. The neurological symptoms and signs thatmay occur have been termed the high pressureneurological syndrome (HPNS). This syndrome hasbeen known for more than twenty years.'The sea bed of the Norwegian continental shelf
with oil and gas resources is situated between 70 and400 msw. Despite progress in robot technology thework ofhuman divers is still required on underwaterinstallations at these depths.We have previously studied the immediate
neurological effects of deep diving.78 This reportappears to be the first follow up study of deep diversto evaluate possible long term consequences of deepdiving. The investigation was part of the Nationalresearch programme on long term health effects ofdiving.
Materials and methodsDIVERS AND DIVESForty male divers, mean age 34-9 (range 24-49)years, were examined one to seven years after theirlast deep dive. These subjects comprised all Nor-wegian deep divers reported to us at the time exceptfor one who did not want to participate. The deepdivers were part of a cross sectional study of 156commercial divers.9 The divers were examined atleast two weeks after their last dive.Deep diving was defined as diving below 180 msw.
Twenty five divers had participated in one deep dive,
258
on January 2, 2020 by guest. Protected by copyright.
http://oem.bm
j.com/
Br J Ind M
ed: first published as 10.1136/oem.48.4.258 on 1 A
pril 1991. Dow
nloaded from

Neurological long term consequences of deep diving
Table 1 The deepest dive made by the divers
No of divers Diving depths (msw)
2 1905 2007 3004 35013 3606 4503 500
msw= Metres of seawater.
eight in two, three in three, and four in four deepdives. The dives comprised mostly simulated dives ina hyperbaric facility. The rest were sea dives. Table 1shows the greatest depths reached by each diver.
EXPOSURE TO DIVING AND EXPOSURE INDICES
One diver had participated in one simulated diveonly, but had never worked as a diver. The others hadbeen commercial divers from one to 23 years (mean11 years). Mean duration of air diving was 583 (range45-2331) days, and mean time in saturation was 378(range 14-706) days. Thirteen of the 40 divers (33%)had stopped diving at the time of the examination.Four had lost their divers' licence because ofneurological problems, and nine wanted a new job.Twenty seven still worked as divers.Exposure indices (total number of days) for air
diving and saturation diving were calculated for eachdiver. Exposure indices for deep diving were cal-culated from days in saturation and the greatestdepth reached. Total diving was calculated from thesum of the described indices. As the exposure was
lognormally distributed, logarithmic transformationwas used in the risk factor analysis.
CONTROLSThe control group consisted of 100 men, mean age
34 0 (range 22-48) years. The inclusion criteria forthe control subjects were age between 20 and 50, noexperience of diving, and health standards compar-
able with requirements for a diving certificate. Thecontrol group consisted of offshore personnel andpolice officers. Some 170 offshore workers were
invited to participate by advertising. Fifty threeresponded and were examined. The rest of thecontrol group was recruited from advertising among270 policemen. The first 50 responders were
examined. Informed consent was obtained from allparticipants. All expenses were refunded but no
salary was paid.
EDUCATIONEleven divers (28%) had had a formal education ofnine years, 20 (50%) 12 years and nine (23%) more
than 12 years. In the control group four (4%) had hada formal education of nine years, 52 (52%) 12 years
and 44 (44%) more than 12 years. Statistical analysisshowed that the controls had had more years offormal education than the divers (p = 0-0001,Pearson x' test).
SMOKING HABITSTwenty three per cent of the divers and 39% of thecontrols smoked cigarettes (p = 0 1, Pearson X% test).The difference between the two groups was notstatistically significant.
USE OF ALCOHOLThis was graded from 1 (low) to 4 (high) in acombined measure of how frequently the subjectsdrank alcohol and the amount. When the divers weregrouped according to use of alcohol, the mean figures(%; controls in parentheses) were: grade 1: 12 (22);grade 2: 20 (35); grade 3: 45 (35); grade 4: 23 (8). Thedivers drank significantly more alcohol than thecontrols (p = 0-028, Pearson x' test).
INTERVIEWA standardised interview was carried out by oneneurologist, focusing upon education, previousdiseases, and a full diving history including com-plications possibly associated with diving. Subjectswere also interviewed about symptoms from thecentral (CNS), the peripheral (PNS), and the auto-nomic (ANS) nervous system, and their use oftobacco and alcohol.
Fatigue, mood lability, irritability, concentrationdifficulties, recent and long term memory problems,work management problems, headache, and dizzi-ness were defined as CNS symptoms. Problems ofshort term memory were defined as inability toremember appointments, problems with control ofpersonal belongings, and extensive use of memoryaids. Long term problems ofmemory were defined aspoor memory for written material and earlier events.The questions were answered with "no" or ''yes"',and graded according to the number of positiveanswers. In cases of "yes" the subjects' own opinionwas that they had a real problem, or that the relevantfunction had decreased significantly over the pastfive years. Results of neuropsychological testing arenot included in this presentation, but have beenpublished previously.'0
Paraesthesia and pain in feet and hands andmuscular weakness were considered as PNS symp-toms.Symptoms from the ANS were defined as cardiac
palpitation, excessive sweating, chest oppression,sexual dysfunction, orthostatic hypotension, andepisodes of diarrhoea and constipation. In eachsubject these symptoms may have had causes notoriginating in the ANS. This was controlled for byfurther questions. If other relevant causes werefound, the symptoms were not attributed to the
259
on January 2, 2020 by guest. Protected by copyright.
http://oem.bm
j.com/
Br J Ind M
ed: first published as 10.1136/oem.48.4.258 on 1 A
pril 1991. Dow
nloaded from

Todnem, Nyland, Skeidsvoll, et al
ANS. Symptoms from the PNS and the ANS weregraded from 1 ("I never have this symptom") to 4 ("Ihave this symptom every day").We calculated a score for neurological symptoms
in each subject. The score ranged from 0 in thesubject without symptoms to 100 in the subject withsymptoms in all variables. The individual scoreswere transformed to a mean score for divers andcontrols.
EXAMINATIONSA standard neurological examination was performedby one neurologist according to a previously definedprotocol." The findings were classified as eithernormal or abnormal. Muscle stretch reflexes were
graded as symmetric, asymmetric, or increased.Abdominal muscle reflexes were graded as normal,asymmetric, or absent. Plantar reflexes were gradedas symmetric, asymmetric, or inverted (Babinskipositive). The same scoring system was used as forsymptoms. The score ranged from 0 in the subjectwith no abnormal neurological findings to 100 in thesubject with abnormal findings in all variables. Theindividual scores were transformed to a mean score
for divers and controls.Visual evoked potentials (VEPs) were examined
with checkerboard reversal stimulation using a DisaNeuromatic 2000 C and a monitor subtending avisual field size of 11' x 8.80 and check size of 1'.Luminance and contrast were held constant. Twohundred signals were averaged and N75, P100, andN145 latencies were analysed.
Brain stem auditory evoked potentials (BAEPs)were tested with the same machine. Rarefactionclicks 60 dB above click hearing threshold were usedand the contralateral ear was masked with white noiseat 50 dB. Click stimulation was 10 Hz and 2000epochs were averaged. Each ear was tested twice andI-V, I-III, and III-V latencies were analysed.The electroencephalograms (EEGs) were 16 or 21
channel recordings from a Siemens-Elema Mino-graph. Electrode placement was according to the 10-20 system. All EEGs were recorded at the same
neurophysiological laboratory and read indepen-dently by two neurophysiologists. If they disagreedon an EEG, it was not accepted as abnormal.Magnetic resonance imaging (MRI) of the brain
and brainstem was performed in 25 divers using a
Philips Gyroscan S5 operating at a field strength of0 5 tesla, and with the following protocol: MRI slicethickness 7 mm, field of view 250 mm, and acquisi-tion time 100%. Ti weighted transverse images useda repetition time (TR) of 1500 ms and echo delay time(TE) of30 ms. T2 weighted transverse images used a
TR of 1500 ms and a TE of 50/100 ms. Ten diverswere examined with the same protocol and in thesame machine, which was then expanded to a mag-
netic field strength of 1-5 tesla.
Eighteen controls were examined in the 1 5 teslamachine and with a slightly different protocol.Images were evaluated by at least two readers. If thereaders disagreed on a high signal intensity change, itwas not accepted as abnormal.
STATISTICAL METHODSThe Pearson x' test and Fisher's exact two tailed testwere adopted for comparisons between groups ofcategorical variables. Student's t test was applied forcomparison of continuous variables with approx-imately normal distribution. Multiple linear regres-sion analysis (neurological symptoms and findings,VEP, BAEP, MRI) and logistic regression analysis(EEG) were used to evaluate the relation betweenrisk factors and the different test results. A stepwiseprocedure eliminated the covariation between riskfactors. The significance of each risk factor in thelinear regression was calculated by Fisher's test. Forthe logistic regression the significance was tested by ax2 statistic. The stepwise procedure at each stepincluded the risk factor with the highest partialcorrelation if its F or x2 statistic was significant.'2
ETHICAL CONSIDERATIONSPermission to establish a register for deep divers andcontrols was given by The Data Inspectorate. Allsubjects were informed that their medical data wouldbe available to themselves in the future, and would bekept in special files in the hospital. The data would beused for scientific purpose only. If otherwise, theywould be asked.
ResultsAll results refer to one set of data and do not includerepetitive examinations.
MEDICAL HISTORYTable 2 presents the medical history one to sevenyears after the deep dives, together with tests of
Table 2 Medical history in divers and controls
Divers Controls Group(n= 40) (n= 100) differencesNo (%) No (%) p Value
Episodes of cerebraldysfunctiont 4 (10) 0 (0) 0.006*
Cerebral concussion 16 (40) 33 (33) 0 44Viral meningitis 0 (0) 1 (1) 1-00Other viral diseasest 26 (65) 42 (42) 0.02*Lumboischialgia 16 (40) 36 (36) 0 7
*Significant differences between the groups, Fisher's exact twotailed test.tEpisodes compatible with transitory cerebral ischaemia, seizures,and transitory global amnesia; all occurred during or after the deepdives.Once or more a year.
260
on January 2, 2020 by guest. Protected by copyright.
http://oem.bm
j.com/
Br J Ind M
ed: first published as 10.1136/oem.48.4.258 on 1 A
pril 1991. Dow
nloaded from

Neurological long term consequences of deep diving
differences between the two groups. Viral infections,defined as episodes with fever and common coldsymptoms, occurred significantly more often in thedivers than in the controls. No group differencesin allergy and pulmonary diseases, gastrointestinaldiseases, hypertension, cancer, or mental disorderswere found. No one had a history of birth injury,cerebral haemorrhage, diabetes mellitus, anginapectoris, or myocardial infarction.Table 3 shows the divers' complications in connec-
tion with diving. The figures refer to total numbersof complications one to seven years after the deepdives, and not before the deep dives. Fourteen (35%)of the divers had experienced decompression sick-ness 2 (DCS 2), and 26 (65%) had experienced DCS1 or 2, or both. Decompression sickness 1 wasdefined as musculoskeletal pain, and DCS 2 asneurological symptoms occurring in or after decom-pression from a dive.Four divers (none ofthe controls) had experienced
episodes of cerebral dysfunction during or after theirdeep dives.Diver 1 had allergies (strawberries, acetylsalicylic
acid). He had had anaphylactic reactions to insectbites twice as a child. During the bottom phase in adive to 450 msw he developed a severe episodicitching all over his body without focal localisation.No visible skin reaction occurred. On the second dayof decompression (418 msw), when sitting writing,he suddenly felt an unpleasant itching localised on hishead combined with rotating vertigo, severe nausea,and bilateral myoclonic jerks in the arms. He thenbecame unconscious for about 30 seconds and fellfrom his chair. On awakening, he had tunnel vision,complete hearing loss, and a feeling that he could notbreathe. All symptoms disappeared in five minuteswithout amnesia. Four hours later, while lying in hisbed, he again experienced sudden severe nausea anddizziness, but remained conscious. For the rest of thedive he suffered from gradually decreasing skinitching, almost resistant to medical treatment. Noneof the other divers had similar symptoms. Theoxygen content of the breathing gas during bottomtime was 0 4 bar and during decompression 0 5 bar.
Table 3 Complications related to diving in 40 deep divers
Number of episodes for each diver
Complication 1 2-5 >5 Total (%)
DCS 2; brain symptoms 8 1 9 (23)DCS 2; spinal cordsymptoms 2 2 1 5 (13)
DCS 1 + 2 11 13 2 26(65)Unconsciousness;Not DCS 7 1 8 (20)
Skin bends 3 4 6 13 (33)Lung complications 2 2 4 (10)
DCS = Decompression sickness.
Neurological findings and EEG immediately afterthe dive were unchanged. Electronystagmographydisclosed a nystagmus to the right that was notpresent before the dive; EEG four weeks after thedive showed short episodes with slow wave (5-7 Hz)activity in the left temporal region.One year later he experienced a similar episode
without obvious provocation. When talking he sud-denly noticed itching, which spread from his head tohis chest and both arms; he felt unable to think, andhad moderate vertigo and blurred vision. He laydown, and developed myoclonic jerks in the chestmuscles and slight breathing difficulties. Thesesymptoms lasted for 30 minutes, but his head andarms felt numb for another 10 hours. Treatment withantihistamines had no effect. A neurological examin-ation showed no new findings. An EEG containedslow wave (5-7 Hz) activity and sharp potentials inboth frontal and temporal regions but no definiteepileptiform pattern. A brain scan by MRI one yearlater was normal. He has had no further episodes.Diver 2 had a mild cerebral concussion when he
was five years old. He had had a hypoxic incidentduring diving with five minutes of unconsciousness14 years before a deep dive to 360 msw. No clinicalabnormalities were discovered after this dive. OneEEG had been normal before the deep dive. An EEGimmediately after the deep dive contained episodeslasting 3-30 seconds with rhythmic theta (4-5 Hz)activity and sharp potentials in the right temporalregion as previously described (diver 88). The EEGcontinued to be abnormal with episodic slow activityin the right temporal region. Six months after thedive he had two nocturnal episodes of focal left sidedjerks lasting a few seconds. Two years after the divehe had several nocturnal episodes with an unpleasantfeeling in his head spreading all over his body,followed by severe asymmetrical jerks in his arms andlegs. The subsequent neurological examination wasnormal and MRI brain scan showed no abnor-malities. The episodes were diagnosed as simplepartial epileptic seizures.Diver 3 participated in a dive to 500 msw, and then
had DCS with musculoskeletal pain. Mild diffuseslow activity (4-6 Hz) occurred in his EEG after thedive (normal before). His EEG was not investigatedfurther at this time.Four years after the dive he collided with a parked
bus when cycling. He was briefly unconscious, had afracture of the dens epistropheus, and compressionfractures of the sixth and seventh cervical vertebra.He had amnesia for the event and dysaesthesia inboth hands, but no other abnormal findings.
Six years after the dive when he was working as asupervisor on a diving ship, he had an 18 hourepisode with severely impaired short term memory.When admitted to hospital two days later, he hadmild ataxia and nystagmus. Neurological examina-
261
on January 2, 2020 by guest. Protected by copyright.
http://oem.bm
j.com/
Br J Ind M
ed: first published as 10.1136/oem.48.4.258 on 1 A
pril 1991. Dow
nloaded from

Todnem, Nyland, Skeidsvoll, et al
Table 4 Neurological symptoms
Mean score (% (SD))
Symptoms Divers Controls p Value
CNS 11 1(165) 43(74) 0001*PNS 67(113) 20(57) 0.002*ANS 8-1 (6-8) 5 7 (5-6) 0.038*
*Significant differences between the groups, Student's t test.
tion five days later was normal. An EEG showeddiffuse slow wave activity. No abnormal findingswere seen on MRI brain scan.Diver 4 had had a head injury with skull fracture
and three days of unconsciousness two years beforetwo dives to 210 msw. There were no residualfindings. Six years after the dives he had two episodeswith generalised tonic clonic seizures. Hisneurological examination, EEG, and MRI brain scanwere normal.
PRESENT SYMPTOMSTable 4 shows the present symptoms from the CNS,PNS, and ANS ascertained from the interviews.The divers had significantly more symptoms than
the controls. The most prominent CNS symptomwas concentration difficulty (mean score in divers 25,mean score in controls 4 (p = 0-0006, Fisher's exacttest)). The most prominent PNS symptom wasparaesthesia in the feet and hands (mean score indivers 12, mean score in controls 4 (p = 0-008,Fisher's exact test)). There was no single prominentANS symptom.
ABNORMAL NEUROLOGICAL FINDINGSTable 5 shows the abnormal neurological findings.The divers had significantly more abnormal findingsfrom the motor system, sensory system, and stretchreflexes than the controls. The most prominentabnormal findings were from the sensory system,with reduced sensitivity to cotton wool in the leftlower leg (mean score in divers 8, mean score incontrols 0 (p = 0-02, Fisher's exact test)). Reducedsensitivity to pin pricks in the left lower leg alsooccurred significantly more often in the divers (meanscore in divers 10, mean score in controls 1(p = 0-02, Fisher's exact test)). No single findingfrom the motor system or stretch reflexes prevailedsignificantly.Four divers (10%) and one control (1%) had
sensory/motor disturbances compatible with dys-function of the lumbar spinal cord or roots. Onediver's findings were moderate, the others were mild.Two divers (5%) and one control (1 %) had sensory/motor findings compatible with mild peripheralpolyneuropathy.
Table 5 Abnormal neurologicalfindings
Mean score (% (SD))Site ofabnormalfindings Divers Controls p Value
Cranial nerves 0 9 (2 4) 0 4 (2-5) 0-31Motor system 2-2 (3 0) 1-2 (1 8) 0-01*Sensory system 4 2 (13 3) 0 8 (3-4) 0.02*Stretch reflexes 1-2 (2-4) 0-4 (1 3) 0.01*Plantarreflexes 5 0(190) 1 5(11 1) 018Abdominal reflexes 8 8 (22 3) 7 0 (23-6) 0-69
*Significant differences between the groups, Student's t test.
RISK FACTOR ANALYSISThe possible causes for neurological symptoms andsigns in this study were considered to be age, use ofalcohol, a history of cerebral concussion and lumbo-ischialgia, previous episodes ofDCS 2, total numberof episodes of DCS 1 or 2, or both (DCS 1 + 2),exposure to air and saturation diving, and exposureto deep diving. Individual subject scores were usedfor neurological symptoms and findings byneurological examination. In these analyses step zeropresents the partial correlation of each risk factor onthe tested variable. In further steps the factor withthe highest partial correlation appears. Some of therisk factors could be internally associated (for ins-tance, divers with long exposure to saturation divingmay also have performed more air diving and deepdiving). Only factors with independent effects occurin further steps.Table 6 presents the risk factor analysis for
neurological symptoms and signs. Significantlycorrelated with neurological symptoms wereprevious episodes of DCS 2, exposure to saturationdiving, total diving, deep diving, and air diving, DCS1 + 2, previous cerebral concussion, and lumbo-ischialgia. Saturation diving, cerebral concussion,lumboischialgia, and DCS 2 were independentlysignificant.
Significantly correlated with abnormal findings inthe neurological examination were exposure to airdiving, total diving, saturation diving, and deepdiving, DCS 1 + 2, DCS 2, and age. Air diving andage were independently significant.
ELECTROENCEPHALOGRAPHYSeven (18%) of the divers and five (5%) of thecontrols had an abnormal EEG (p = 0 039,Student's t test). The EEG changes consisted offocalor diffuse slow wave activity and sharp potentials.(Twenty eight of the divers had had a normal EEGbefore the deep dives. The other 12 had not beenexamined. The previous results are not included inthis study.)Three of the four divers with episodes of cerebral
dysfunction had an abnormal EEG. An abnormal
262
on January 2, 2020 by guest. Protected by copyright.
http://oem.bm
j.com/
Br J Ind M
ed: first published as 10.1136/oem.48.4.258 on 1 A
pril 1991. Dow
nloaded from
Neurological long term consequences of deep diving
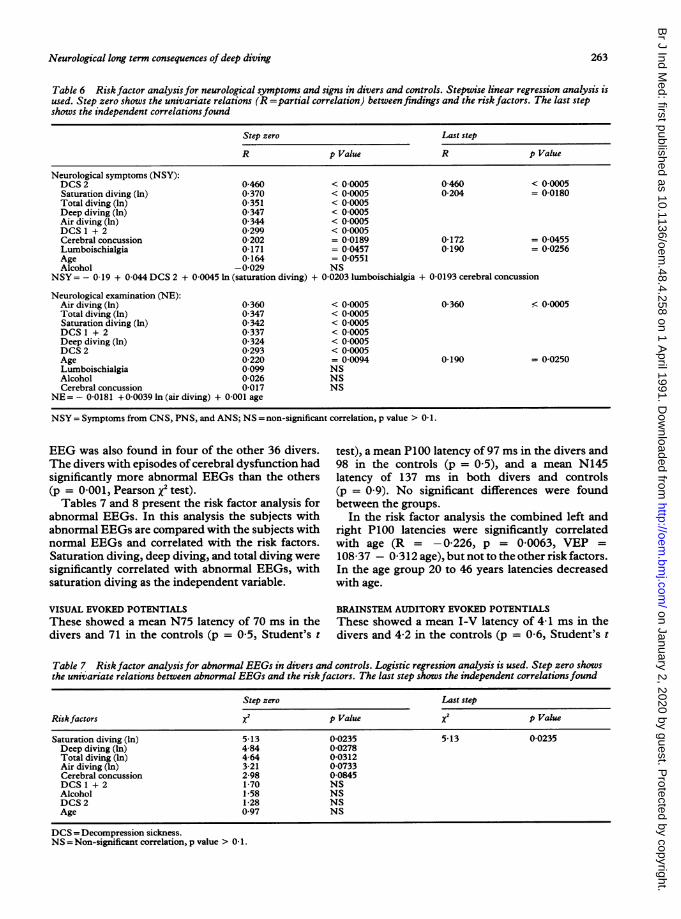
Table 6 Risk factor analysisfor neurological symptoms and signs in divers and controls. Stepwise linear regression analysis isused. Step zero shows the univariate relations (R =partial correlation) between findings and the risk factors. The last stepshows the independent correlations found
Step zero Last step
R p Value R p Value
Neurological symptoms (NSY):DCS 2 0-460 < 0-0005 0-460 < 0-0005Saturation diving (In) 0 370 < 0 0005 0-204 = 00180Total diving (In) 0 351 < 0 0005Deep diving (In) 0 347 < 0-0005Air diving (In) 0 344 < 0 0005DCS 1 + 2 0 299 < 0-0005Cerebral concussion 0-202 = 0-0189 0-172 = 0 0455Lumboischialgia 0 171 = 0-0457 0 190 = 0-0256Age 0 164 = 0-0551Alcohol -0-029 NS
NSY= - 019 + 0-044 DCS 2 + 0-0045 In (saturation diving) + 0-0203 lumboischialgia + 0-0193 cerebral concussion
Neurological examination (NE):Air diving (In) 0-360 < 0 0005 0-360 < 0 0005Total diving (In) 0-347 < 0-0005Saturation diving (In) 0 342 < 0-0005DCS I + 2 0 337 < 0-0005Deep diving (In) 0 324 < 0-0005DCS 2 0293 < 00005Age 0 220 = 0-0094 0 190 = 00250Lumboischialgia 0 099 NSAlcohol 0 026 NSCerebral concussion 0 017 NS
NE= - 00181 +0-0039 In (air diving) + 0-001 age
NSY = Symptoms from CNS, PNS, and ANS; NS = non-significant correlation, p value > 0 1.
EEG was also found in four of the other 36 divers.The divers with episodes of cerebral dysfunction hadsignificantly more abnormal EEGs than the others(p = 0-001, Pearson x test).Tables 7 and 8 present the risk factor analysis for
abnormal EEGs. In this analysis the subjects withabnormal EEGs are compared with the subjects withnormal EEGs and correlated with the risk factors.Saturation diving, deep diving, and total diving weresignificantly correlated with abnormal EEGs, withsaturation diving as the independent variable.
test), a mean P100 latency of 97 ms in the divers and98 in the controls (p = 0-5), and a mean N145latency of 137 ms in both divers and controls(p = 0 9). No significant differences were foundbetween the groups.
In the risk factor analysis the combined left andright P100 latencies were significantly correlatedwith age (R = -0-226, p = 0-0063, VEP =
108-37 - 0-312 age), but not to the other risk factors.In the age group 20 to 46 years latencies decreasedwith age.
VISUAL EVOKED POTENTIALS BRAINSTEM AUDITORY EVOKED POTENTIALSThese showed a mean N75 latency of 70 ms in the These showed a mean I-V latency of 4-1 ms in thedivers and 71 in the controls (p = 0-5, Student's t divers and 4-2 in the controls (p = 0-6, Student's t
Table 7 Risk factor analysis for abnormal EEGs in divers and controls. Logistic regression analysis is used. Step zero showsthe univariate relations between abnormal EEGs and the riskfactors. The last step shows the independent correlationsfound
Step zero Last step
Riskfactors x2 p Value X2 p Value
Saturation diving (In) 5 13 0-0235 5-13 0-0235Deep diving (In) 4-84 0-0278Total diving (In) 4-64 0-0312Air diving (In) 3-21 0-0733Cerebral concussion 2-98 0-0845DCS 1 + 2 170 NSAlcohol 1-58 NSDCS2 1-28 NSAge 0-97 NS
DCS =Decompression sickness.NS = Non-significant correlation, p value > 0 1.
263
on January 2, 2020 by guest. Protected by copyright.
http://oem.bm
j.com/
Br J Ind M
ed: first published as 10.1136/oem.48.4.258 on 1 A
pril 1991. Dow
nloaded from

Todnem, Nyland, Skeidsvoll, et al
Table 8 Relative riskfor abnormal EEGs
Amount of Relative risksaturation diving (95% CI)
Saturation diving (In) X 1X + 2 1-61 (103 - 244)X + 4 2-58(1-06 - 594)X + 6 415(109 - 1448)
X= Logarithmic transformation of an occasionally chosen amountof days in saturation.
test), a mean I-III latency of 2 2 ms in both diversand controls (p = 0-2), and a mean III-V latency of1-9 ms in the divers and 1 7 in the controls (p = 0 1).No significant differences were found between thegroups. In the risk factor analysis BAEP (combinedmeasure of left and right I-V latencies) was notsignificantly correlated with any of the risk factors.
MAGNETIC RESONANCE IMAGING OF THE BRAIN ANDBRAIN STEMThis was performed in 37 divers and 49 controls.Seven (19%) of the divers and 21 (43%) of thecontrols had high signal intensity changes. Thecontrols had significantly more high signal intensitychanges (p = 0-045, Pearson x2 test). (Twelve of thedivers had had a MRI without high signal intensitychanges and nine had had a normal computedtomography (CT) of the brain before the deep dives.The others had not been examined. No previousresults are included in this study.) The four diverswho had lost their divers' licence because ofneurological disturbances all had a normal MRI.
In the risk factor analysis the number ofhigh signalintensity changes was significantly correlated withincrease in age (R = 0-261, p = 0-017). The diverswith the longest saturation diving exposure had thefewest MRI changes (R = -0 273, p = 0 010). Nosignificant correlation with the prevalence ofDCS orany of the other factors was found.
DiscussionFour (10%) ofthe divers had lost their divers' licencebecause of neurological disturbances, but were stillfully employed. One to seven years after the deepdives, however, they had significantly more symp-toms from the nervous system than the controls.They also had more abnormal findings byneurological examination and more abnormal EEGsthan the controls, but the evoked potentials and theMRI brain scans had no more abnormalities than thecontrol group. It is necessary to take into considera-tion the facts that 27 (68%) of the divers had had atleast one neurological examination and EEG, andmany had also had MRI or CT ofthe brain before thedeep dives. They had been partly selected for deep
diving on the basis of the medical data. Accordingly,they should be considered the most healthy diversbefore the deep dives.The controls were invited by advertising to par-
ticipate. Neurological examination of a normalpopulation has disclosed minor sensory and motordisturbances, slight ataxic signs, and disturbedreflexes." Such findings occur more often in olderpeople with a definite increase in men from age 35.Accordingly it was necessary in this study to includea control group comparable with the divers. Thecontrol group does not necessarily represent anaverage of the invited groups in all respects. Forinstance, the controls had more years of formaleducation than the divers. Many policemen have acollege education before the police academy. Collegeeducation is not mandatory for divers, and they aremostly qualified by professional courses or in thenavy. The average intellectual level of the divers wasslightly above what is found in a normal population.'0The divers drank significantly more alcohol than thecontrols, but the factor analysis showed that alcoholconsumption was not a major pathogenetic factor inthese cases, probably because none ofthe divers werealcohol abusers.The divers reported significantly more symptoms
from the nervous system than the controls. Concen-tration difficulties and paraesthesia were the mostprominent symptoms. The divers are more informedof neurological symptoms because of their educationand training. The symptoms were, however, stronglycorrelated with DCS 2, saturation diving, deepdiving (depth included), air diving, DCS 1 + 2,episodes of previous cerebral concussion, andlumboischialgia (table 6, step zero), and consequen-tly could not be attributed to the different knowledgebetween the two groups. The exposure indicesappear to be internally related, and DCS 2 andsaturation diving only were independently correlatedto the symptoms in addition to previous cerebralconcussion and lumboischialgia. This means thatdivers who have had DCS 2 have an increased risk ofgetting more neurological symptoms, and divers withlong exposure to saturation diving have an increasedrisk also in the absence of clinical DCS 2. The reasonmay be due to subclinical episodes ofDCS, influenceof the hyperbaric pressure, or other factors. Theseresults also correspond with findings from neuro-psychological examination of deep saturation and airdivers.'0 13One notable finding is the four divers (10%) who
had experienced episodes of cerebral dysfunction.Diver 1 had his first episode early in the decompres-sion phase from a deep dive. Accordingly, theepisode was most probably directly related to thedive, and caused by transitory gas emboli reducingbrain stem blood flow.'4'5 It has been shown by invivo imaging by single photon emission tomography
264
on January 2, 2020 by guest. Protected by copyright.
http://oem.bm
j.com/
Br J Ind M
ed: first published as 10.1136/oem.48.4.258 on 1 A
pril 1991. Dow
nloaded from

Neurological long term consequences of deep diving
that in divers with DCS 2 or cerebral arterial gasembolism, areas of cerebral hypoperfusion mayoccur and persist up to 14 months.""'8 Anotherpossible cause for this episode may have been anadverse effect ofthe oxygen content,'920 although thisis less likely as neurological symptoms rarely occurbelow 3 bar of oxygen. A vasovagal syncope or anepileptic seizure are other less likely causes.
In diver 2 the seizures occurred at six months andtwo years after the deep dive. His EEG containedepileptiform patterns shortly after the dive, makingthe deep dive a probable cause for the seizures. Onlyone predive EEG was recorded and this was normal.His earlier hypoxic incident may have made his brainmore susceptible to injury from the deep dive.Diver 3 had an episode of transient global amnesia
six years after the deep dive. On admission to thehospital he had transient clinical findings of slightataxia and nystagmus, which are not commonlyfound in patients with transient global amnesia."2123This condition has been described in patients from34 to 92 years of age, but most commonly in theelderly. It is presumably caused by ischaemia of thehippocampus and related structures supplied inparticular by the posterior cerebral artery.22 23 As wellas the deep dive, his previous head injury could be acontributing factor to this episode. For diver 4, whohad experienced two episodes ofgeneralised seizures,his severe head injury is the most plausible cause forthe seizures.The divers had significantly more abnormal find-
ings from the motor and sensory system than thecontrols. The findings were compatible with dys-function in the lumbar spinal cord or nerve roots.Neuropathological examinations have discloseddegenerative lesions in the spinal cord both in a casewith spinal DCS and in cases with no history ofDCS.2425 As seen from table 6 these findings showhighly significant correlations with air and saturationdiving, DCS 1 + 2, deep diving (depth included),DCS 2, and age. The exposure indices in this analysisare also internally related and only air diving and agewere independently correlated to the neurologicalfindings. This means that air diving is statisticallymore strongly correlated than the other exposureindices. The findings were in most cases minor andshould by themselves not influence ordinary workingcapacity. Similar neurological findings have beenreported before in air divers.'32627 Deep diving wasnot independently correlated with the symptoms andsigns.Abnormal EEGs were found more often in this
group of divers than among the controls despite thefact that most divers (68%) had a normal EEG beforetheir deep dive. Exposure to saturation diving anddeep diving (depth included) were significantlycorrelated with the occurrence of abnormal EEGs.We have earlier reported abnormal EEGs in divers
immediately after deep diving.8 This has also beenreported in divers who have never performed deepdives.'328 The changes in EEG represent neuronaldysfunction29 and may have contributed to theepisodes of cerebral dysfunction experienced bysome of the divers.
Brain scans by MRI showed significantly morehigh signal intensity changes in the controls than inthe deep divers, and age was independently respon-sible for the changes in MRIL30 The reason for thisdifference is probably that many of the divers hadbeen selected for deep diving on the basis of having anormal MRI or cerebral CT. High signal intensitychanges represent vascular ectasia, dilated peri-vascular spaces, alteration of myelin, and gliosis."The significance of these changes is disputed as theyare found in both neurologically ill patients and incontrol subjects. The changes in older subjectscorrelate with hypertension, diabetes mellitus,hypercholesterolaemia, and cardiac diseases.32 In alarger study of saturation divers we found no sig-nificant difference in MRI brain scans betweendivers and controls (unpublished observations). Wehave previously reported that deep diving to 360 mswgave no immediate changes in MRI brain scans in 18divers.8 The four divers in this study who lost theirlicence because of neurological disturbances all hadMRI brain scans without high signal intensitychanges. This supports previous evidence that nomajor structural changes in the brain occur fromdeep diving.One to seven years after the deep dives the divers
had more symptoms and signs from the nervoussystem, and more abnormal EEGs than the controls.Four divers had experienced episodes of cerebraldysfunction during or after the deep dives. Thefindings had highly significant correlations with deepdiving, but they were more strongly correlated withordinary saturation diving, air diving, and DCS.Most deep divers have performed a lot of ordinarysaturation diving and air diving, and this makes theinterpretation difficult. This was a cross sectionalstudy of a small subject population, which could beinterpreted cautiously. The findings are, however, ofmedical concern. Special attention should be given tothe selection of divers,33 and long term follow upprogrammes should be available for deep divers.
We are indebted to Statoil, Norsk Hydro, and theRoyal Norwegian Council for Scientific and Indus-trial Research who are financing the programme onlong term health effects of diving. We are alsoindebted to Svein Eidsvik MD, Royal NorwegianNavy, Alf Brubakk MD, Department of BiomedicalEngineering, University of Trondheim, the parti-cipating divers and controls, and the staff of theNorwegian Underwater Technology Centre for helpand collaboration in this investigation.
265
on January 2, 2020 by guest. Protected by copyright.
http://oem.bm
j.com/
Br J Ind M
ed: first published as 10.1136/oem.48.4.258 on 1 A
pril 1991. Dow
nloaded from

Todnem, Nyland, Skeidsvoll, et al
Requests for reprints to: Kari Todnem, NUTEC,PO Box 6, N-5034 Ytre Laksevag, Norway.
1 Bennett PB. The high pressure nervous syndrome in man. In:Bennett PB, Elliott DH, eds. The physiology and medicine ofdiving. London: Bailliere Tindall, 1982:262-96.
2 Bennett PB, McLeod M. Probing the limits of human deepdiving. Philos Trans R Soc Lond fBiol 1 1984;304:105-17.
.-3 Zaltsman GL. Hyperbaric epilepsy and narcosis. Leningrad:Sechenov Institute of Evolutionary Physiology and Bio-chemistry, USSR Academy of Sciences, 1968:1-258.
4 Fructus X, Naquet R, Gosset A, Fructus P, Brauer RW. Lesyndrome nerveux des hautes pressions. Marseille Medical1969;6:509-12.
5 Brauer RW, Dimov S, Fructus X, Fructus P, Gosset A, NaquetR. Syndrome neurologique et electrographique des hautepressions. Rev Neurol 1969;121:264-5.
6 Bennett PB, Towse EJ. The high pressure nervous syndromeduring a simulated oxygen-helium dive to 1500 ft. Electro-encephalogr Clin Neurophysiol 1971;31:383-93.
7 Aarli JA, Vaernes R, Brubakk AO, Nyland H, Skeidsvoll H,T0njum S. Central nervous dysfunction associated with deep-sea diving. Acta Neurol Scand 1985;71:2-10.
8 Todnem K, Nyland H, Dick APK, et al. Immediate neurologicaleffects of diving to a depth of 360 metres. Acta Neurol Scand1989;80:333-40.
9 Todnem K, Nyland H, Kambestad BK, Aarli JA. Influence ofoccupational diving upon the nervous system: an epidemi-ological study. Br J Ind Med 1990;47:708-14.
10 Vernes RJ, Klove H, Ellertsen B. Neuropsychologic effects ofsaturation diving. Undersea Biomed Res 1989;16:233-51.
11 Skre H. Neurological signs in a normal population. Acta NeurolScand 1972;48:575-606.
12 Dixon WJ, Brown MB, Engelman L, et al. BMDP StatisticalSoftware. Berkeley: University of California Press, 1985.
13 Dolmierski R, Kwiatkowski SR, Nitka J, Palubicki J, Laba L.Neurological, psychiatric and psychological examinations ofdivers in the light of their professional work. Bull Inst MaritTrop Med Gdynia 1981;32:141-52.
14 Toole JF, Cole M. Ischemic cerebrovascular disease. In: BakerAB, Baker LH, eds. Clinical Neurology. Philadelphia: Harper& Row, 1983;2(15):1-51.
15 Bender MB, Rudolph SH, Stacy CB. The neurology ofthe visualand oculomotor systems. In: Baker AB, Baker LH, eds.Clinical Neurology. Philadelphia: Harper & Row, 1983;1(12):1-132.
16 Macleod MA, Adkisson GH, Fox MJ, Pearson RR. 99Tc"-
HMPAO single photon emission tomography in the diagnosisof cerebral barotrauma. Br J Radiol 1988;61:1106-9.
17 Adkisson GH, Hodgson M, Smith F, et al. Cerebral perfusiondeficits in dysbaric illness. Lancet 1989;8655:119-22.
18 Adkisson GH, Hodgson M, Macleod MA, Sykes JJW, PearsonRR. Cerebral perfusion deficits in dysbaric illnesses: Followup studies in 18 divers. In: Bitterman N, Lincoln R, eds.Proceedings of the XVth meeting of the European UnderseaBiomedical Society. Eilat, Israel, 1989:55-60.
19 Donald KW. Oxygen poisoning in man. Br Med J 1947;1:667-72, 712-17.
20 Clark JM. Oxygen toxicity. In: Bennett PB, Elliott DH, eds. Thephysiology and medicine of diving. London: Bailliere Tindall,1982:200-38.
21 Miller Fisher C, Adams RD. Transient global amnesia. ActaNeurol Scand 1964;40:1-83.
22 Shuping JR, Rollinson RD, Toole JF. Transient global amnesia.Ann Neurol 1980;7:281-5.
23 Shuttleworth EC, Wise GR. Transient global amnesia due toarterial embolism. Arch Neurol 1973;29:340-2.
24 Palmer AC, Calder IM, McCallum RI, Mastaglia FL. Spinalcord degeneration in a case of "recovered" spinal decompres-sion sickness. Br Med J 1981;283:888.
25 Palmer AC, Calder IM, Hughes JT. Spinal cord degeneration indivers. Lancet 1987;72:1365-6.
26 Rozsahegyi I. Late consequences of the neurological forms ofdecompression sickness. Br J Ind Med 1959;16:311-7.
27 Rozsahegyi I, Roth B. Participation of the central nervoussystem in decompression. Industrial Medicine and Surgery1966;35:101-10.
28 Kwiatkowski SR. Analysis of the EEG records among divers.Bull Inst Marit Trop Med Gdynia 1979;30:131-5.
29 Martin JH. Cortical neurons, the EEG, and the mechanisms ofepilepsy. In: Kandel ER, Schwartz JH, eds. Principles ofneural science. Amsterdam: Elsevier, 1985:636-47.
30 Drayer BP. Imaging of the aging brain. Part I. Normal findings.Part II. Pathologic conditions. Radiology 1988;166:785-806.
31 Awad IA, Johnsen PC, Spetzler RF, Hodak JA. Incidentalsubcortical lesions identified on magnetic resonance imagingin the elderly. Postmortem pathological correlations. Stroke1986;17:1090-7.
32 Lechner H, Schmidt R, Bertha G, Justich E, Offenbacher H,Schneider G. Nuclear magnetic resonance image white matterlesions and risk factors for stroke in normal individuals. Stroke1988;19:263-5.
33 Todnem K, Nyland H, Riise T, et al. Analysis of neurologicsymptoms in deep diving: Implications for selection of divers.Undersea Biomed Res 1990;17:95-107.
Accepted 1 October 1990
266
on January 2, 2020 by guest. Protected by copyright.
http://oem.bm
j.com/
Br J Ind M
ed: first published as 10.1136/oem.48.4.258 on 1 A
pril 1991. Dow
nloaded from