Embed Size (px)
Citation preview

Eric Eggenberger DO Neuro-Ophthalmology
Neuro-ophthalmology: 5 new-ish things (controversies)

Neuro-ophthalmology: 5 new things1.Retinal ischemia 2.Ocular myasthenia gravis 3.Vergence/sagging eye 4.Optic neuritis x 3 5.Giant cell arteritis

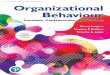
TMVL DWI %
BRAO DWI %
CRAO DWI %
Hellenius et al Ann Neurol 2012
66 18% DWI+
46 33% DWI+
Lauda et al CV Dis 2015
68 16% DWI+
44 31% DWI+
101 53% DWI+
Golsari et al Stroke 2017
35 12% DWI+
8 12% DWI+
69 76% DWI+
+DWI% AVG 38% 15% 27% 62%
RAO & TMVL: MRI DWI

Acute Retinal Ischemia Management• Stroke referral: 3 days (or 7 days with emboli source)
•ABCD >2-3; clinical, labs
AHA Stroke 2009; Biousse, Nahab, Newman. Ophth 2018
Vascular imagingMRI with DWI
Echo & EKG/monitor

44-♂ Transient Diplopia
5
Binocular? Vertical vs horizontal? Co-morbidities? Associated symptoms?
Episodic Diplopia
Episodic Misalignment
Episodic Malfusion

?Fatigue“Make
everything as simple as
possible, but not simpler”
*Albert Einstein
Everything is worse with fatigue!

Ocular MG Generalization
*50% +Ab *Natural Hx: ~50% generalize !Risk/time: 2 years: 15%, 3 years: 6% generalize
**70% +Ab (MSU + UM cohort) **33/158 (21%) converted to GMG 10 (30%) converted >2years
*Oosterhuis, JNNP 1989;52:1121; Glob. MG. 1999. Bever. Ann Neurol 1983 **Nagia, Lemos, Abusamra, Cornblath, Eggenberger. Opthalmology 2015

OMGRate: Rating Scale for Ocular Myasthenia Gravis
Wong S, Xhepa S, Miranda E, Lee H, Burke A, DelArti L, Cornblath W, Eggenberger E, Barnett C. J Neuro-Ophth, in press

OMGRate-e: Eye Movements
1 point 1 point
1 point
1 point2 points
1 point
1 point
1 point
3 points
3 points

OMGRate-e: Lids
1 point
2 points

Correlation: OMGRATS-e and -q & MG-QOL = 0.65, i.e. good
OMGRATS-questionnaire good indicator of QOL
010
2030
4050
0 20 40 60totalMGQOLscore
Fittedvalues OMGRATSqwithweighteddiplopiascores
020
4060
0 20 40 60totalMGQOLscore
Fittedvalues OMGRATSe&OMGRATSqweighted

• Pupil-sparing • Painless • Variable
MG Conclusion
1. Cogan Lid Twitch 2. Enhancement of Ptosis
70% +Ab 21% (33/158) convert *30% convert >2yrs

13
Binocular Horizontal Diplopia
Alternate Cover Distance

2. Parinaud Dorsal Midbrain Syndrome Convergence retraction “nystagmus”
1.CRN 2.LND 3.Lid 4.SWJ 5.Vergence 6.Vertical 7.Skew

LR-SR Band
100 Pts w/o strabismus LR-SR band: 95% coronal T1WI 70% Coronal CT LR-SR Bowing ⍺ age (50, 9-81 yrs)
Patel et al. AJNR 2014
EOM: Sagging EyeEOM: Sagging Eye

Optic Neuritis
Papillitis 35%
Retrobulbar neuritis
65%
• Evaluation? • OCT • MRI

NMOSD Core Character1.Optic neuritis: 33% <20/200
Wingerchuk et al. Neurology 2015
2. Acute myelitis 3. Area postrema syndrome: hiccups or nausea and vomiting 4. Acute brainstem syndrome 5. Narcolepsy or acute diencephalic syndrome with MRI lesions 6. Symptomatic cerebral syndrome with typical MRI

NMOSD Dx Criteria+Aquaporin-4 IgG1. >1 core clinical characteristic2. Positive AQP4-IgG using best available method (cell-based assay)3. Exclusion of alternative diagnosis
Wingerchuk et al. Neurology 2015

MOG-IgG:October 2017Mayo Labs
Optic Neuritis #3
Antel NEJM 2004

MOG Optic Neuritis: Clinical n=87
MOG Ab-Positive Optic Neuritis. Chen, Flanagan, JIitprapaikulsan, Lopez-Chiriboga, Fryer, Leavitt, Weinshenker, McKeon, Tillema, Lennon, Tobin, Keegan, Luchinetti, Kantarci, McClelland, Lee, Bennett, Pelak, Chen, VanStavern, Adesina, Eggenberger, Acierno, Wingerchuk, Brazis, Sagan, Pittock. AJO 2018
57% female; median age onset 31 (2–79) Yrs
63% Unilateral optic neuritis: Average VA nadir: count fingers Average final VA: 20/30
5 patients (6%) <20/200 in either eye
86% Disc edema and pain

Median attacks 3 (1–8) Followup 2.9 yrs (0.5–24 yrs) Annualized relapse rate 0.8
1 patient diagnosed MS (MOG-IgG index 2.8 (<2.5))
MOG Ab-Positive Optic Neuritis. Chen, Flanagan, JIitprapaikulsan, Lopez-Chiriboga, Fryer, Leavitt, Weinshenker, McKeon, Tillema, Lennon, Tobin, Keegan, Luchinetti, Kantarci, McClelland, Lee, Bennett, Pelak, Chen, VanStavern, Adesina, Eggenberger, Acierno, Wingerchuk, Brazis, Sagan, Pittock. AJO 2018
MOG Optic Neuritis: Clinical n=87
0%
12.5%
25%
37.5%
50%
ON + Neuro Recurrent ON CRION Single ON
12%16%
30%41%

MOG Optic Neuritis: CSF
↑WBC 44% (24/50), median 4 (0 - 568)
↑Protein 42%, median 46 (19-181)
0 Oligoclonal bands (0/45)
MOG Ab-Positive Optic Neuritis. Chen, Flanagan, JIitprapaikulsan, Lopez-Chiriboga, Fryer, Leavitt, Weinshenker, McKeon, Tillema, Lennon, Tobin, Keegan, Luchinetti, Kantarci, McClelland, Lee, Bennett, Pelak, Chen, VanStavern, Adesina, Eggenberger, Acierno, Wingerchuk, Brazis, Sagan, Pittock. AJO 2018

MOG Optic Neuritis Therapy n=87
Acute: 83% IVMP 9% IVMP + PLEX 3% IVMP + IVIG 3% No Tx 1% IVIG
Chronic: 61% Chronic Tx •MMF •Azathioprine •Rituximab
MOG Ab-Positive Optic Neuritis. Chen, Flanagan, JIitprapaikulsan, Lopez-Chiriboga, Fryer, Leavitt, Weinshenker, McKeon, Tillema, Lennon, Tobin, Keegan, Luchinetti, Kantarci, McClelland, Lee, Bennett, Pelak, Chen, VanStavern, Adesina, Eggenberger, Acierno, Wingerchuk, Brazis, Sagan, Pittock. AJO 2018

0/177 AQP4-IgG; but 3/177 MOG-IgG
Initial VA 20/50, 20/50, HM 3/3 Disc edema 3/3 Final VA 20/20 (1 PBO, 2 prednisone)
0/3 MRI lesions; 0/3 MS
Chen, Tobin, Majed, Jitprapaikulsan, Fryer, Leavitt, Flanagan, McKeon, Pittock. JAMA Ophth 2018
AQP4 & MOG in the ONTT n=3

Optic Neuritis x 3• MRI + Labs • AQP-4, MOG-IgG Ab • Disc edema, MRI features
• Acute Tx: IVMP, PLEX • Most AQP4 & MOG are recurrent • AQP-4 poor prognosis untreated • MOG: ideal treatment?

Mayo Fla Photo: Jason Calhoun
78♀ VA Loss OS•20/20, 20/100 •RAPD OS •8 & 0/10 HRREvaluation? Labs? MRI? Doppler? CT?

27
Benjamin, Goodman, AJM 1979; Huston AIM 1978; Machado Arth Rheum 1988
Fever
Anorexia/Wt Loss
Myalgia
J Claudication
Scalp Tender
TA Tender
Headache
0% 23% 45% 68% 90%
GCA Symptoms

GCA Dx: CRP & ESR
Parikh, Miller, Lee, Savino, Vacarezza, Cornblath, Eggenberger, Antonio, Golnik, Kardon, Wall. Ophth 2006
Sens
iitivi
ty76%
99%
1.7%
+ESR +CRP +ESR +CRP
-ESR -CRP
98%
0.8%
15%
N = 119 +TAB
+ESR -CRP
+CRP -ESR
86%

Inflammation Endurance
Malaszewski, Younge, Fritzlen et al. Mod Path 2017;30:788
Time
Gran
ulom
a Va
scul
itis
71%67%
50%
25%
3 Mo 6 Mo 9 Mo 12 Mo
70%75%
44% 44%
N = 40

GCA: Tocilizumab 162mg sc q week
Week 52 remission: Tocilizumab 53 - 56% vs 14 - 18% prednisone
Stone et al. Tocilizumab in GCA. NEJM 2017

Inciting event
Exact pathophysiology
Early remission/prognostic markers
Biopsy vs angiography
GCA Unmet Needs

• Afferent 1.GCA 2.MOG Ab 3.Retinal ischemia
• Efferent 4.Sagging eye 5.Myasthenia
N-O New-ish Things