Embed Size (px)
Citation preview
AbstractAlthough food insecurity and malnutrition have become policy priorities in Nepal, the precise relationship between these two challenges needs to be elucidated. This study’s objective was to assess the prevalence of, and association between household food insecurity and nutritional status among children aged 12-48 months and their mothers in Baitadi district in Nepal. We analyzed cross-sectional data on 2106 households from August 2009. The data set included information on demographic variables, household food insecurity, child care and feeding practices, use of preventative services as well as height, weight and hemoglobin levels of the children and their mothers. More than four-fifths (83.9%) of households reported some level of food insecurity. Prevalence of stunting, wasting, underweight and anemia among children were 61.7%, 10.4%, 45.7%, and 29.6% respectively. Among mothers, prevalence of underweight (BMI<18.5 kg/m2) and anemia were 22.8% and 20.3% respectively. Controlling for potential confounders, household food insecurity was associated only with stunting among children and anemia among mothers. Children from food insecure households were 51% more likely to be stunted compared to children from food secure households and mothers from food insecure households were 78 % more likely to be anemic compared to mothers from food secure households. Our results demonstrate the high prevalence of malnutrition among preschool children and their mothers in the Baitadi district. The significant association between household food insecurity and childhood stunting as well as maternal anemia highlights the importance of addressing malnutrition through interventions that enhance household food security.
IntroductionFood insecurity is a persistent challenge in Nepal. The country has been unable to produce sufficient amounts of food to meet the needs of the population since 2005. (1) The situation is particularly dire in the Mid and Far Western Hill and Mountain Regions, where recent estimates reveal that 23.6% of the population is food insecure. (2) These figures combined with the high national prevalence of stunting (49%), underweight (39%) and wasting (13%) among preschool children (3), make food insecurity and malnutrition a major concern among policy makers, legislators, nutritionists and public health professionals in the country. Discussions
and policy decisions have begun to focus on the high prevalence of food insecurity and malnutrition in Nepal, and the possible causal link between these two challenges; however, the precise relationship between these indices among different populations in the country needs more research. A recent study found no significant association between household food insecurity and stunting, underweight and anemia among preschool children in one of the lowland “Terai” districts of Nepal (4). However, this lack of association cannot be generalized across the country because of the varying topography, lifestyle, levels of development and access to resources across the country.
HouseHold food InsecurIty Is HIgHly prevAlent And predIcts stuntIng Among prescHool cHIldren And AnemIA Among tHeIr motHers, In BAItAdI dIstrIct of nepAl
nepAl nutrItIon And food securIty BulletIn
Iss.
2

Helen Keller International, Nepal, 20102
The relationship between household food insecurity and malnutrition in different parts Nepal needs to be elucidated. The objective of this study was to assess the association between household food insecurity and malnutrition among children aged 12 – 48 months, as well as the nutritional status of their mothers, in rural communities in the Baitadi district of Nepal.
methods This study is based on a secondary data analysis of a cross-sectional, baseline assessment for a prospective trial to evaluate the impact of a community-based program. The program is called “Action Against Malnutrition through Agriculture” (AAMA) and it is currently being implemented in the Baitadi district, located in the Far Western region of Nepal. The district is divided into 12 sub-districts called “Ilakas”. Each “Ilaka” is further divided into municipalities called village development councils (VDCs), which are comprised of several “wards” (villages). The AAMA project uses an integrated model that combines homestead food production (home garden and small animal husbandry) with a behavior change communication package to promote optimal feeding and care practices, as well as better use of preventive health services, to prevent malnutrition in preschool children and women of reproductive age. The project is funded by the United States Agency for International Development (USAID) and is implemented by Helen Keller International (HKI) in partnership with the Ministries of Health and Agriculture in Nepal, and two Nepali NGOs: the Nepali Technical Assistance Group at the national level and Snehi Mahila Jagaron Kendra in Baitadi district.
The AAMA project used a multi-stage cluster randomized control design to assign households in selected “Ilakas” to receive either the AAMA project activities (project communities) or no AAMA project activities (control communities) for a period of four years. Baseline data were collected in August 2009 and involved 2106 households with children aged 12-48 months.
Information collected through interviews with mothers of children included socio-demographic characteristics, infant and young child feeding (IYCF) practices,
hygiene practices, and use of preventive health services, including participation in growth monitoring, and receipt of immunizations, vitamin A capsules and deworming tablets. Household food insecurity was assessed using the Household Food Insecurity Access Scale (HFIAS) developed by the Food and Nutrition Technical Assistance (FANTA) project (5). Mothers were asked to recall responses to each question on the HFIAS tool over the 12 months prior to the survey.
Weight and height or length and of children and mothers were measured according to standard WHO procedures (6). Hemoglobin of children and mothers was measured using Hemocue analyzer. Z scores of weight for age (WAZ), weight for height (WHZ) and height for age (HAZ) were computed using the 2006 WHO growth standards and underweight, wasting and stunting among children were defined as WAZ <-2, WHZ <-2 and HAZ <-2 respectively (7). Height and weight of mothers were used to compute BMI using the formula: BMI (kg/m2) = weight / [height] 2. Maternal nutritional status was classified according to BMI categories as underweight (BMI < 18.5 kg/m2), normal (BMI 18.5 ≤ 23.0 kg/m2), at risk of overweight (BMI 23.0 ≤ 25.0 kg/m2), overweight (BMI 25.0 ≤ 30.0 kg/m2) and obese (BMI > 30 kg/m2) (8). Mothers who were pregnant at the time of the survey were excluded from all the analyses that involved maternal weight or BMI. Anemia was defined as hemoglobin < 110 g/L for children and pregnant mothers, and hemoglobin < 120 g/L for non-pregnant mothers, after adjusting for the influence of altitude on hemoglobin using appropriate WHO reference values (9).
Bivariate comparisons of food insecure and food secure households were made using a chi-square test for proportions and independent-sample t test for means. Multivariate logistic regression models were used to control for confounding variables such as maternal age, parity, marital status and education; household caste and wealth index; and child’s age, gender, participation in growth monitoring, vitamin A supplementation in the previous six months, completion of DPT, and measles immunization. Maternal weight and height were also included in all child models and
Helen Keller International, Nepal, 2010 3
Worried over Unable to eat Ate limited Ate non- Ate less Skipped Ran out Went to bed household preferred variety of preferred than a meal of food without food supply foods foods foods usual food
n = 2106 n = 2072 n = 2072 n = 2042 n = 2106 n = 2106 n = 2106 n = 2030Never 25.1 44.6 56.0 46.8 69.9 77.5 52.6 80.6Rarely - 21.5 19.4 18.9 8.8 19.2 42.9 13.1Sometimes 50.0 29.3 22.2 28.5 19.8 2.8 3.8 5.7Often 24.4 4.5 2.4 5.9 1.4 0.5 0.8 0.6
Table1 : Proportion of households that experienced specific food insecurity related conditions in the 12 months preceding the survey1
1Values are percentages
Child feeding practices, use of preventive health services and household food insecurityTable 2 presents the indicators of child feeding practices and use of preventive health services for children in our sample. Over 80% of the mothers in our sample were still breastfeeding at the time of the survey. Less than half of the mothers (44.9%) had initiated breastfeeding
the maternal anemia model. In addition, maternal hemoglobin was included in the child anemia model. Dummy variables identifying each “Ilaka” and proxy sample weights were included in all regression models to account for clustering Data was analyzed using SPSS version 18.0 (SPSS) and Stata version 11.0 (StataCorp).
The protocol for the study was reviewed and approved by the Nepal Health Research Council (NHRC), Kathmandu, Nepal.
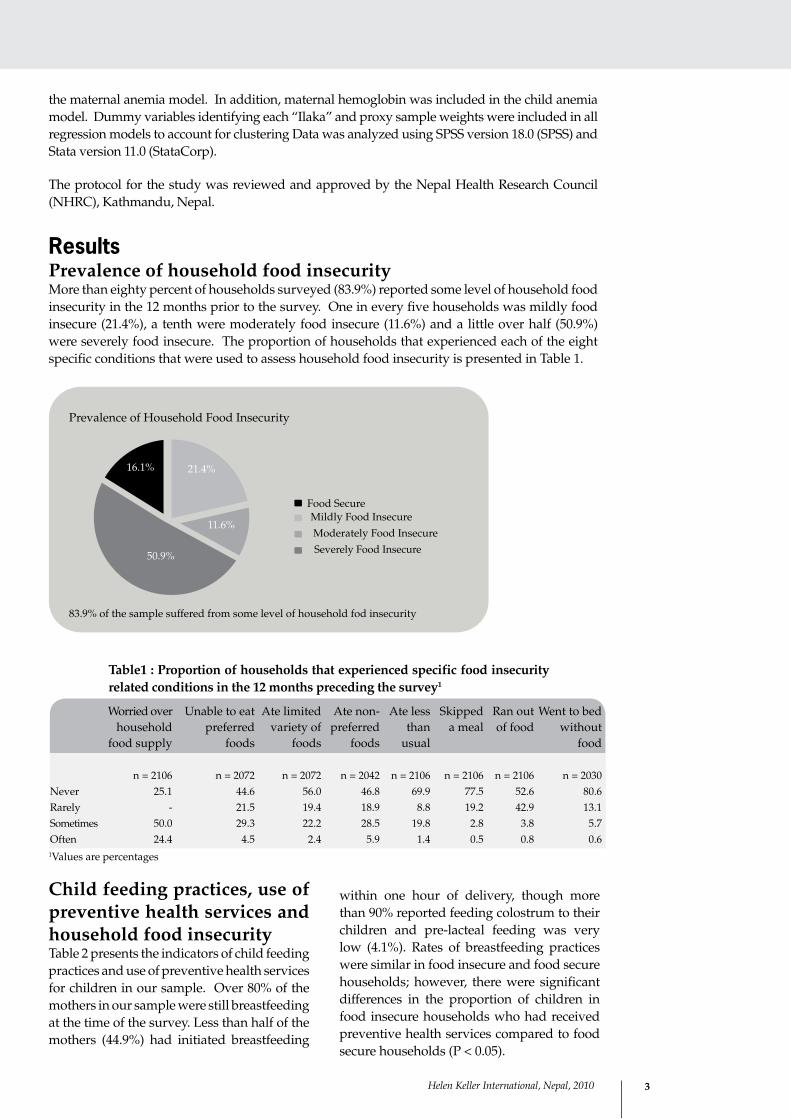
resultsPrevalence of household food insecurity More than eighty percent of households surveyed (83.9%) reported some level of household food insecurity in the 12 months prior to the survey. One in every five households was mildly food insecure (21.4%), a tenth were moderately food insecure (11.6%) and a little over half (50.9%) were severely food insecure. The proportion of households that experienced each of the eight specific conditions that were used to assess household food insecurity is presented in Table 1.
Prevalence of Household Food Insecurity
83.9% of the sample suffered from some level of household fod insecurity
Food SecureMildly Food InsecureModerately Food InsecureSeverely Food Insecure
16.1% 21.4%
11.6%
50.9%
within one hour of delivery, though more than 90% reported feeding colostrum to their children and pre-lacteal feeding was very low (4.1%). Rates of breastfeeding practices were similar in food insecure and food secure households; however, there were significant differences in the proportion of children in food insecure households who had received preventive health services compared to food secure households (P < 0.05).
Helen Keller International, Nepal, 20104
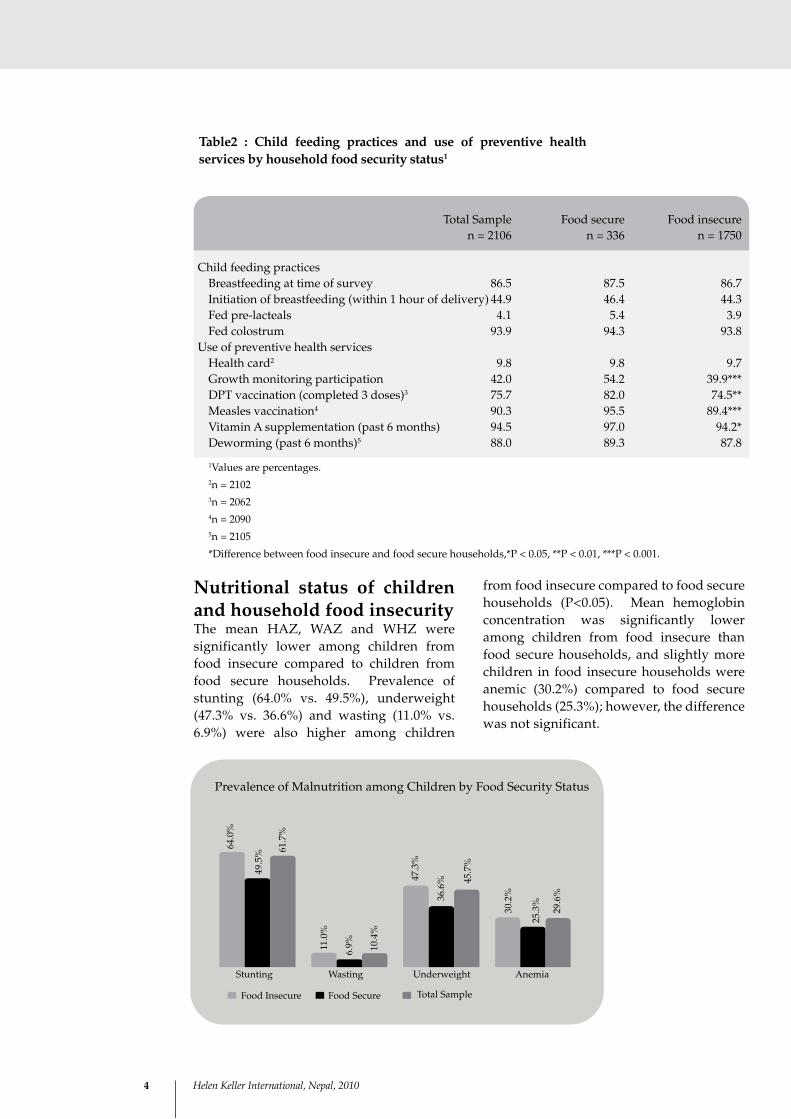
Nutritional status of children and household food insecurityThe mean HAZ, WAZ and WHZ were significantly lower among children from food insecure compared to children from food secure households. Prevalence of stunting (64.0% vs. 49.5%), underweight (47.3% vs. 36.6%) and wasting (11.0% vs. 6.9%) were also higher among children
Total Sample Food secure Food insecure n = 2106 n = 336 n = 1750
Child feeding practices Breastfeeding at time of survey 86.5 87.5 86.7 Initiation of breastfeeding (within 1 hour of delivery) 44.9 46.4 44.3 Fed pre-lacteals 4.1 5.4 3.9 Fed colostrum 93.9 94.3 93.8Use of preventive health services Health card2 9.8 9.8 9.7 Growth monitoring participation 42.0 54.2 39.9*** DPT vaccination (completed 3 doses)3 75.7 82.0 74.5** Measles vaccination4 90.3 95.5 89.4*** Vitamin A supplementation (past 6 months) 94.5 97.0 94.2* Deworming (past 6 months)5 88.0 89.3 87.8
Table2 : Child feeding practices and use of preventive health services by household food security status1
1Values are percentages.2n = 21023n = 20624n = 20905n = 2105
*Difference between food insecure and food secure households,*P < 0.05, **P < 0.01, ***P < 0.001.
from food insecure compared to food secure households (P<0.05). Mean hemoglobin concentration was significantly lower among children from food insecure than food secure households, and slightly more children in food insecure households were anemic (30.2%) compared to food secure households (25.3%); however, the difference was not significant.
11.0
%
6.9% 10
.4%
Prevalence of Malnutrition among Children by Food Security Status
64.0
%
49.5
% 61.7
%
47.3
%
36.6
% 45.7
%
30.2
%
25.3
%
29.6
%
Stunting Wasting Underweight Anemia
Food Insecure Food Secure Total Sample
Helen Keller International, Nepal, 2010 5
In the multivariate analysis, household food insecurity was only associated with stunting among children (P < 0.05). Children from food insecure households were 51% more likely to be stunted compared to children from food secure households [OR (95% CI): 1.51 (1.15 – 1.99)]. Being stunted was also positively associated with child’s age and maternal parity, but negatively associated with maternal age, weight and height as well as household wealth (particularly upper compared to lower tercile of wealth index) (P < 0.05). After controlling for confounding variables, neither underweight nor anemia was associated with household food insecurity.
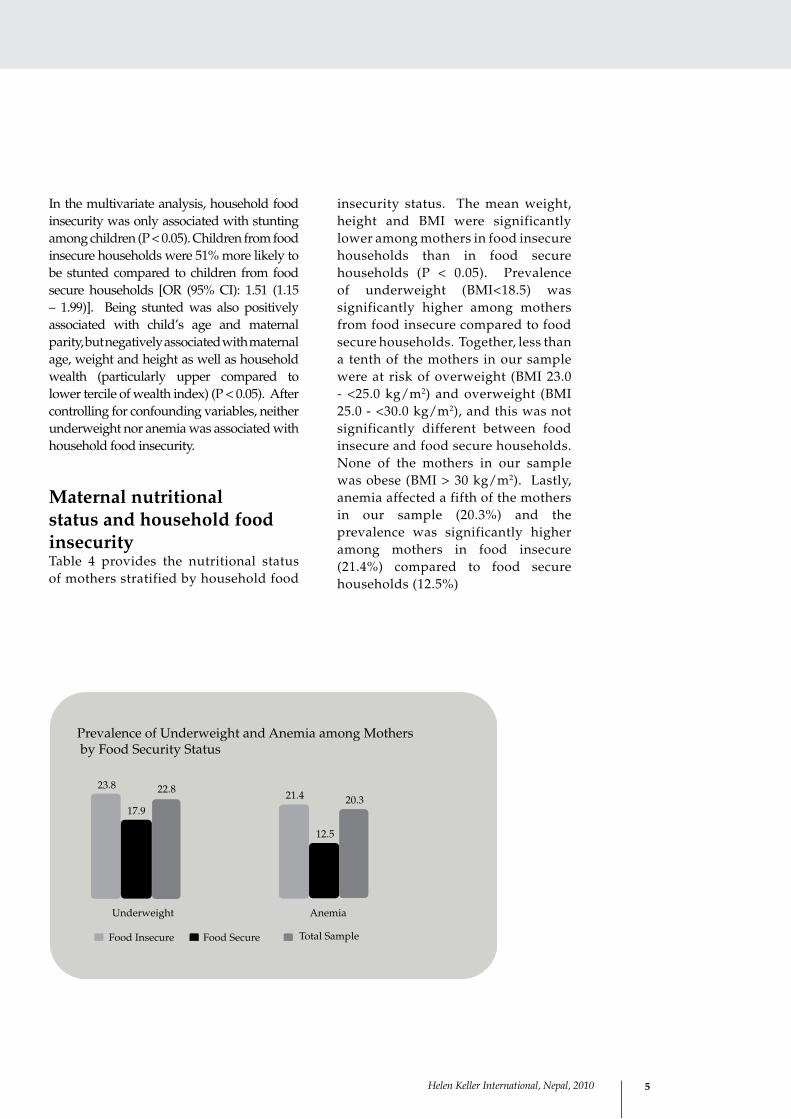
Maternal nutritional status and household food insecurity Table 4 provides the nutritional status of mothers stratified by household food
insecurity status. The mean weight, height and BMI were significantly lower among mothers in food insecure households than in food secure households (P < 0.05). Prevalence of underweight (BMI<18.5) was significantly higher among mothers from food insecure compared to food secure households. Together, less than a tenth of the mothers in our sample were at risk of overweight (BMI 23.0 - <25.0 kg/m2) and overweight (BMI 25.0 - <30.0 kg/m2), and this was not significantly different between food insecure and food secure households. None of the mothers in our sample was obese (BMI > 30 kg/m2). Lastly, anemia affected a fifth of the mothers in our sample (20.3%) and the prevalence was significantly higher among mothers in food insecure (21.4%) compared to food secure households (12.5%)
23.821.4
17.9
12.5
22.820.3
Underweight Anemia
Prevalence of Underweight and Anemia among Mothersby Food Security Status
Food Insecure Food Secure Total Sample

Helen Keller International, Nepal, 20106
After adjusting for potential confounding factors, only anemia among mothers was significantly associated with household food insecurity. Mothers from food insecure households were 1.78 times more likely to be anemic compared to mothers from food secure households [OR (95% CI): 1.78 (1.21 – 2.63)]. Maternal anemia was also inversely associated with the weight of the mother and household socio-economic status (P < 0.05). Although maternal underweight was not associated with household food insecurity, it was significantly associated with maternal education and caste even after controlling for confounders. Mothers with no education were 33% more likely to be underweight compared to mothers with some formal education (P < 0.05), and mothers from lower caste families were 51% more likely to be underweight compared to those from higher caste families (P < 0.05).
discussion and conclusionsThe results of this study demonstrate the high prevalence of household food insecurity and malnutrition of preschool children and their mothers in the Baitadi district of Nepal. The main findings show that household food insecurity was positively associated with stunting in children and anemia in mothers, even after adjusting for potential confounding factors. Although, there was a significant association between household food insecurity and underweight among children and their mothers, this association was not significant in the multivariate analysis. Childhood anemia was not associated with household food insecurity in either the bivariate or multivariate analysis.
The significant association between household food insecurity and stunting among preschool children observed in our
study is consistent with results from studies in other developing countries including Bangladesh (10) Pakistan (11), and Columbia (12). Conversely, a recent study conducted by our team in the lowland “terai” regions of Nepal, found no association between household food insecurity and stunting among preschool children (4); however, the lack of consistency between the findings may be due to differences in methods between studies, including differences in study design, sample size, study population, the food insecurity assessment tools and confounding variables adjusted in the multivariate models. The lack of a statistically significant association between household food insecurity and anemia is consistent with our previous findings from the “terrai” regions of Nepal (4). It is possible that factors other than iron deficiency or dietary intake may influence anemia in these populations. The finding that food insecurity is associated with anemia among mothers is consistent with previous studies; (13) Similarly, the lack of a significant association between household food insecurity and BMI among mothers is also fitting with studies from Tanzania (14), Uganda (15), Malaysia (16) and Trinidad and Tobago (17), which reveal inconsistent results, indicating that the association between household food insecurity and women’s nutritional status likely depends on numerous contextual factors.
In summary, this study reveals that among our sample in Baitadi district, Nepal, there is a significant association between household food insecurity and childhood stunting, as well as maternal anemia, even when controlling for confounding. These findings emphasize the importance of an integrated approach to addressing malnutrition that includes interventions that enhance household food security.
Helen Keller International, Nepal, 2010 7
references1 Food Security Monitoring Task Force
National Planning Commission, the Government of Nepal. The Food Security Atlas of Nepal, July 2010.
2 World Food Programme, Nepal Food Security Bulletin Issue No. 27, January-March 2010.
3 Ministry of Health and Population/Macro International Inc. “Nepal Demographic and Health Survey.” Kathmandu: MOHP, 2006.
4 Osei A, Pandey P, Spiro D, Nielson J, Shrestha R, Tulukdar Z, Quinn V, Haselow N. “Household food insecurity and nutritional status of children aged 6-23 months in Kailali district of Nepal.” Food and Nutrition Bulletin. 2010. Accepted for publication.
5 Coates J, Swindale A, Bilinksy P. Household food insecurity access scale (HFIAS) for measurement of food access: indicator guide, version 2. Washington DC: Food and Nutrition Technical Assistance (FANTA), Academy for Educational Development, 2006.
6 World Health Organisation, Physical Status: the use and interpretation of anthropometry. Report of WHO Expert Committee, Geneva: World Health Organisation 1995.
7 World Health Organisation Multicentre Growth Reference Study Group. “WHO child growth standards based on length/height, weight and age.” Acta Paediatrica. 2006;450:76S-85.
8 World Health Organisation. “Expert Consultation: Appropriate body-mass index for Asian populations and its implications for policy and intervention strategies.” Lancet 2004;363:157–63.
9 World Health Organization/United Nation’s Children’s Fund/United Nation’s University. Iron Deficiency Anemia: assessment, prevention and control. A guide for programme managers. Geneva: WHO, 2001 [Distribution no. 01.3].
10 Saha KK, Frongillo EA, Alam DS, Arifeen SE, Persson LA, Rasmussen KM. “Household food security is associated with growth of infants and young children in rural Bangladesh.” Public Health Nutrition 2009;12:1556-1562.
11 Baig-Ansari N, R. M., Bhutta ZA, Badruddin SH. “Child’s gender and household food insecurity are associated with stunting among young Pakistani children residing in urban squatter settlements. .” Food and Nutrition Bulletin 2006:27(2):114-127.
12 Hackett M, Melgar-Quinonez H, Alvarez MC. “Household food insecurity associated with stunting and underweight among preschool children in Antioquia, Colombia.” Rev Panam Salud Publica. 2009;25:506-510.
13 Eicher-Miller HA, Mason AC, Weaver CM, McCabe GP, Boushey CJ. “Food insecurity is associated with iron deficiency anemia in US adolescents.” American Journal of Clinical Nutrition. 2009;90(5):1358-1371.
Helen Keller International, Nepal, 20108
14 Leyna, Germana H., Elia J Mmbaga, Kagoma S Mnyika, Akhtar Hussain and Knut-Inge Klepp. “Food insecurity is associated with food consumption patterns and anthropometric measures but not serum micronutrient levels in adults in rural Tanzania,” Public Health Nutrition, Jan 2009;12(1): 1-7.
15 Chaput, Jean-Philippe, Jo-anne Gilbert and Angelo Tremblay. “Relationship between Food Insecurity and Body Composition in Ugandans Living in Urban Kampala.” Journal of the
American Dietic Association 2007, 107 ed.: 1978-1982.
16 Shariff, Z Mohd and GL Khor. “Obesity and household food insecurity: evidence from a sample of rural households in Malaysia.” European Journal of Clinical Nutrition, 2005: 1049–1058.
17 Gulliford, Martin C., Deepak Mahabir and Brian Rocke. “Food insecurity, food choices, and body mass index in adults: nutrition transition in Trinidad and Tobago.” International Journal of Epidemiology, 2003: 508–516.
Helen Keller International, nepal
PO Box 3752, Patan Dhoka RoadKathmandu, NEPAL www.hki.org
david spiroCountry [email protected]
pooja pandey ranaDirector of [email protected]
Helen Keller International Asia pacific regional office
Phnom Pehn - CambodiaWebsite: www.hki.org
nancy J. HaselowVice President and Regional Director for Asia [email protected]
Akoto K. oseiRegional Nutrition Advisor for Asia [email protected]
Helen Keller International,
Headquarters (global)
new york - usAvictoria QuinnSenior Vice President – [email protected]
Jennifer nielsenNutrition Program Manager (Global)[email protected]
© 2010 Helen Keller InternationalReprints or reproductions of portions or all of this document are encouraged provided due acknowledgment is given to the publication and publisher. Projects carried out by HKI-Nepal in collaboration with the above organizations are funded by the United States Agency for International Development (USAID). The opinions expressed herein are those of the author(s) and do not necessarily reflect the views of the US Agency for International Development.
for information and correspondence contact