Embed Size (px)
Citation preview
8/10/2019 Necrotizing Sialometaplasia -
http://slidepdf.com/reader/full/necrotizing-sialometaplasia- 1/33
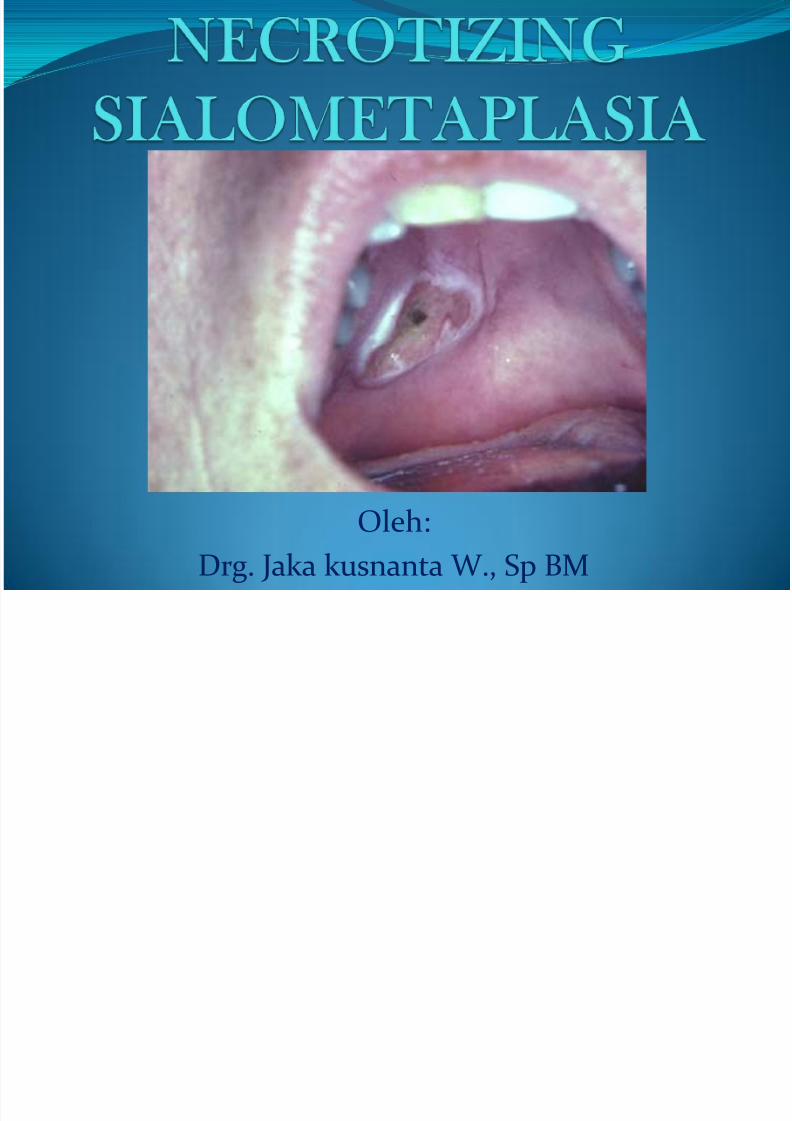
Oleh:
Drg. Jaka kusnanta W., Sp BM
8/10/2019 Necrotizing Sialometaplasia -
http://slidepdf.com/reader/full/necrotizing-sialometaplasia- 2/33
Necrotizing sialometaplasia is a benign ulcerative lesion found mostly on the
posterior hard palate. It is due to a necrosis of
minor salivary glands due to trauma (often palatal
infiltrations of local anaesthetic or trauma during
intubation).
8/10/2019 Necrotizing Sialometaplasia -
http://slidepdf.com/reader/full/necrotizing-sialometaplasia- 3/33
is a nonneoplastic inflammatory
condition of the salivary glands.The clinical and histopathologic
features of necrotizingsialometaplasia often simulate
those of malignancies such assquamous cell carcinoma or
salivary gland malignancy .
8/10/2019 Necrotizing Sialometaplasia -
http://slidepdf.com/reader/full/necrotizing-sialometaplasia- 4/33
Tanda dan gejalaGejala :
Ulcerasi yg sakit di palatum
Tanda:Lokasi : bagian tengah palatum durum
di antara raphe palatal dan tepi gingiva
Biasanya di daerah molarPada bbrp kasus ditemukan juga di
bibir dan retromolar pad
8/10/2019 Necrotizing Sialometaplasia -
http://slidepdf.com/reader/full/necrotizing-sialometaplasia- 5/33
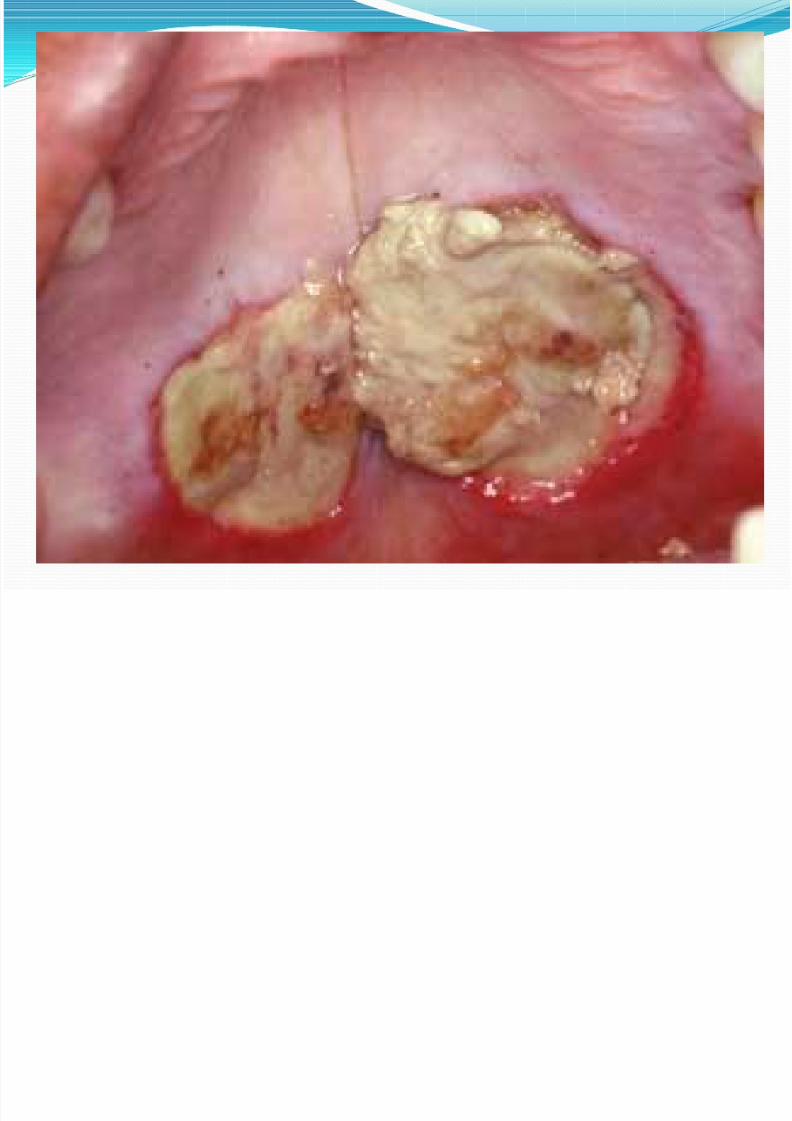
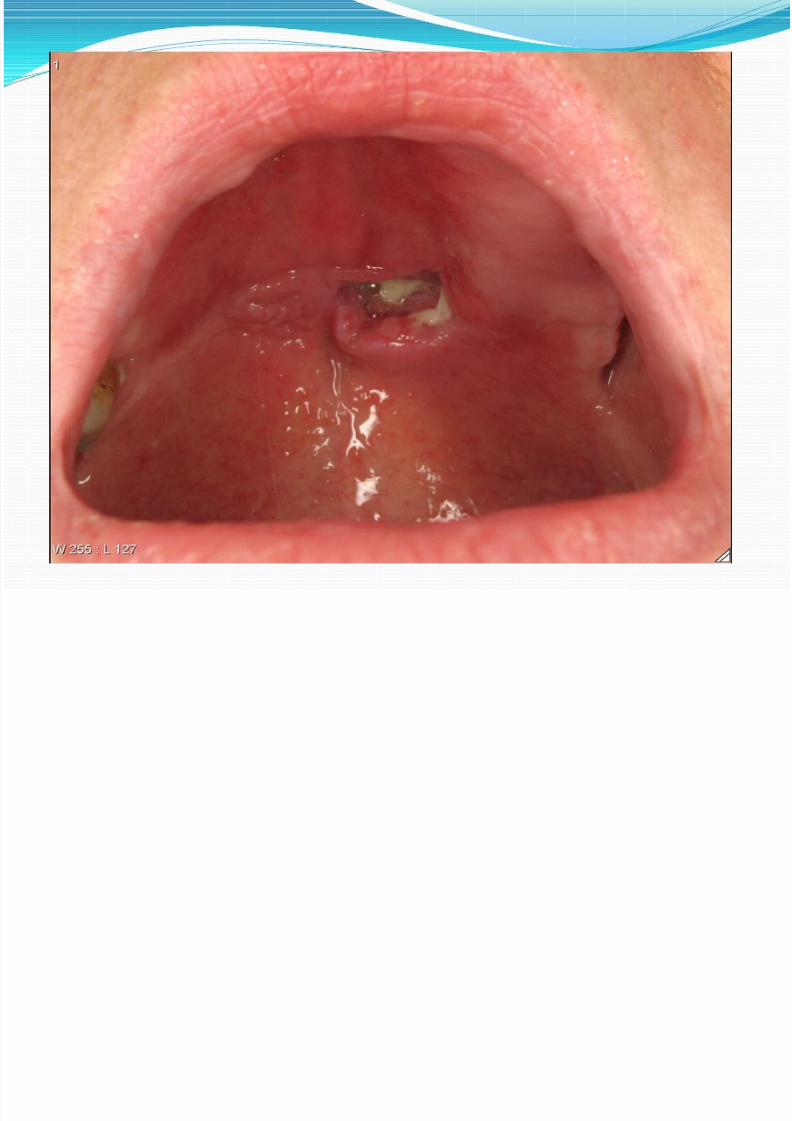
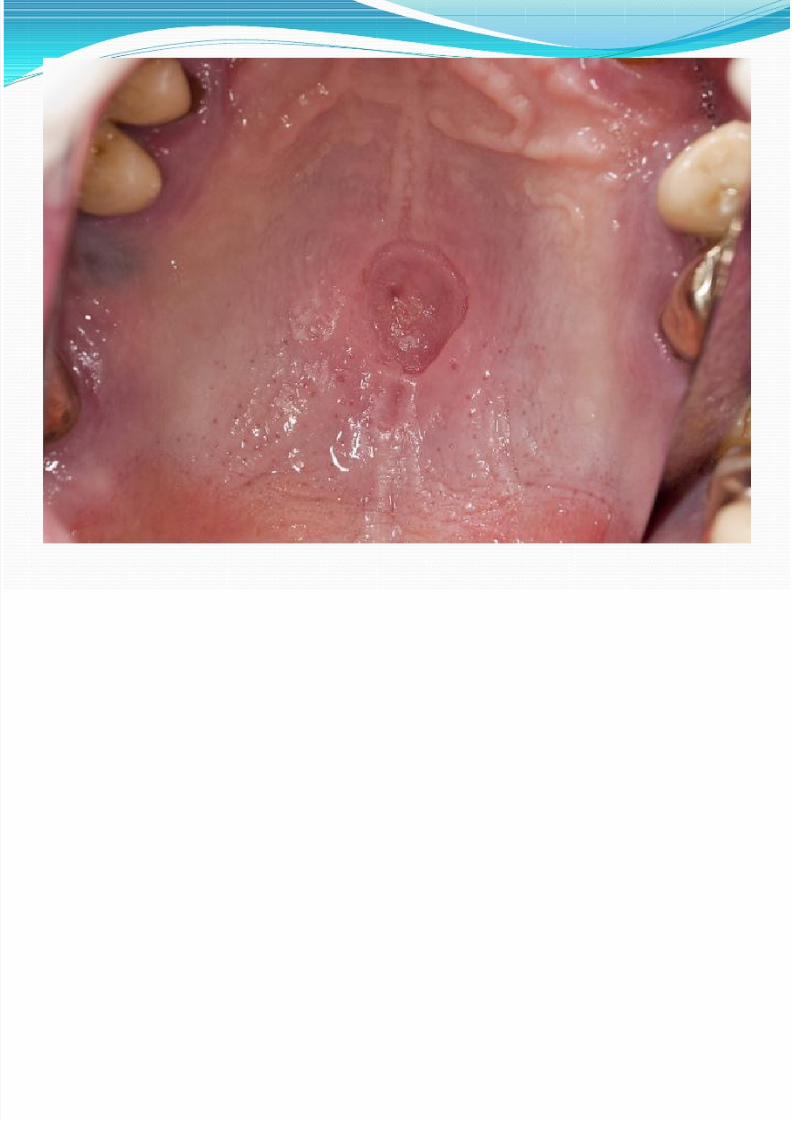
Jumlah : satu
Ukuran : diameter bisa mencapai 2 cmBentuk: bulat dg tepi tdk beraturan
Jaringan dasar : tulang palatalDasar lesi : kekuningan disertai debris
necrotik
Tepi lesi : masuk kedalam ataumenonjol disertai indurasi
8/10/2019 Necrotizing Sialometaplasia -
http://slidepdf.com/reader/full/necrotizing-sialometaplasia- 6/33
8/10/2019 Necrotizing Sialometaplasia -
http://slidepdf.com/reader/full/necrotizing-sialometaplasia- 7/33
8/10/2019 Necrotizing Sialometaplasia -
http://slidepdf.com/reader/full/necrotizing-sialometaplasia- 8/33
8/10/2019 Necrotizing Sialometaplasia -
http://slidepdf.com/reader/full/necrotizing-sialometaplasia- 9/33
Pathophysiology
Necrotizing sialometaplasia was first
reported to involve the minor salivary glandsof the oral cavity, particularly those of thepalate. Seventy-five percent of all cases
occur on the posterior palate.
Most areunilateral, with one third occurring in abilateral or midpalatal location. Reports ofthis entity in the minor glands of the
retromolar pad area, buccal mucosa,tongue, incisive canal, and labial mucosafollowed
8/10/2019 Necrotizing Sialometaplasia -
http://slidepdf.com/reader/full/necrotizing-sialometaplasia- 10/33
In addition, necrotizing
sialometaplasia is recognized in theparotid and submandibular salivaryglands, minor mucous glands in the
lung,nasal cavity,
larynx,trachea,
nasopharynx, and maxillary sinus.Similar lesions are identified in the
breast; the condition is referred to asposttraumatic lobular metaplasia of thebreast.
8/10/2019 Necrotizing Sialometaplasia -
http://slidepdf.com/reader/full/necrotizing-sialometaplasia- 11/33
Pathogenesis The initial cause is unknown, but
necrotizing sialometaplasia is due torestriction of blood supply or damage to
the salivary tissue. The lesion usually
occurs at the juncture of the hard andsoft palate. Because of the damaged
appearance of the tissue, the patient may
be extremely anxious after noticing thislesion , tooth brushing of the lesion may
produce exudate or bleeding , adding to
the frightening appearance.
8/10/2019 Necrotizing Sialometaplasia -
http://slidepdf.com/reader/full/necrotizing-sialometaplasia- 12/33
Etiology:
The cause of necrotizingsialometaplasia is not known, but it isusually preceded by trauma. It is locally
destructive, with inflammation to anarea of tissue resulting in damage andischemic necrosis. This may occur not
only in the salivary glands but also insinus/nasal tracts and the respiratorytract.
8/10/2019 Necrotizing Sialometaplasia -
http://slidepdf.com/reader/full/necrotizing-sialometaplasia- 13/33
In most cases of necrotizing
sialometaplasia, the etiology is believedto be related to vascular ischemia.Cases are reported in which vascular
compression is caused by a necroticmyocutaneous reconstruction flap,embolization from carotid
endarterectomy, sickle cellanemia,Buerger disease,or Raynaudphenomenon.
8/10/2019 Necrotizing Sialometaplasia -
http://slidepdf.com/reader/full/necrotizing-sialometaplasia- 14/33
The association of adjacent neoplasia
that results in ischemic necrosis of theglandular elements and the histologicfeatures of necrotizing sialometaplasiasupports this pathogenic mechanism.In an experimental study in a ratmodel, local anesthetic injectionsinduced necrotizing sialometaplasia.
Tobacco use is suggested as a possibleetiologic risk factor for necrotizingsialometaplasia.
8/10/2019 Necrotizing Sialometaplasia -
http://slidepdf.com/reader/full/necrotizing-sialometaplasia- 15/33
Epidemiology: Men are reported to develop necrotizing
sialometaplasia more often than women by a2:1 ratio. The palatal salivary glands are
involved in 75% of cases, and thesubmandibular and sublingual glands arerarely involved (but there are reported casesthat do involve these areas). The initial
lesion may present as a tissue swelling and within several weeks develop into the crater-like lesion presented in the case study.
8/10/2019 Necrotizing Sialometaplasia -
http://slidepdf.com/reader/full/necrotizing-sialometaplasia- 16/33
whites outnumbered cases in blacks by a
ratio of 4.9:1..The average age of patients withnecrotizing sialometaplasia in the Armed
Forces Institute of Pathology (AFIP)registry is 47.9 years, with a range of 17-80 years. The average age is 43.1 years forfemale patients and 50.3 years for male
patients. A case of necrotizingsialometaplasia in an 18-month-old infantis reported
8/10/2019 Necrotizing Sialometaplasia -
http://slidepdf.com/reader/full/necrotizing-sialometaplasia- 17/33
Mortality/Morbidity
The lesions of necrotizing sialometaplasiaoften are painless; less frequently, they causepain and numbness. The clinical appearance
that suggests cancer is the significantfeature of this lesion. The clinical picturesshow a patient with a lesion thought to be
cancer who underwent biopsy and wasmonitored for 9 weeks. Over that time,regression of the lesion can be seen
8/10/2019 Necrotizing Sialometaplasia -
http://slidepdf.com/reader/full/necrotizing-sialometaplasia- 18/33
History Most cases of necrotizing sialometaplasia appear
to arise spontaneously, whereas others areassociated with a history of trauma, vomiting,
radiation therapy, or surgery. An association with
neoplasia, such as parotid tumors, false vocal cordsquamous cell carcinoma, and maxillary sinuscarcinoma, is also reported. Cases associated withinflammatory conditions such as relapsing
polychondritis and acute and chronic sinusitishave been noted to occur in the subglottic andsinus regions, respectively.
8/10/2019 Necrotizing Sialometaplasia -
http://slidepdf.com/reader/full/necrotizing-sialometaplasia- 19/33
PhysicalNecrotizing sialometaplasia manifests as a
swelling with or without ulceration inanatomic sites that have mucous or serousglandular tissue.
The typical clinical presentation ofnecrotizing sialometaplasia is that of acrateriform ulcer of the palate that simulatesa malignant process. These ulcerated lesionsare 1-3 cm and are usually unilateral, butbilateral synchronous lesions andmetachronous lesions can occur.
8/10/2019 Necrotizing Sialometaplasia -
http://slidepdf.com/reader/full/necrotizing-sialometaplasia- 20/33
Some lesions of necrotizing sialometaplasia maypresent as a submucosal swelling, without ulceration
of the overlying mucosa. An intact surface mucosa maybe noted in an evolving lesion at the time of diagnosis,although most cases are accompanied by mucosalulceration. Erosion of the palatal bone may occur in
either ulcerated or nonulcerated lesions. Examination of a biopsy specimen is usually required
to establish the correct diagnosis and to exclude amalignant or infectious process or an inflammatory
condition such as Wegener granulomatosis.Extranodal lymphoma also may be considered in theclinical differential diagnosis of a palatal swelling orulceration.
8/10/2019 Necrotizing Sialometaplasia -
http://slidepdf.com/reader/full/necrotizing-sialometaplasia- 21/33
Differential Diagnoses Aphthous Stomatitis
Behcet Disease
Squamous Cell Carcinoma
Syphilis
Wegener Granulomatosis
8/10/2019 Necrotizing Sialometaplasia -
http://slidepdf.com/reader/full/necrotizing-sialometaplasia- 22/33
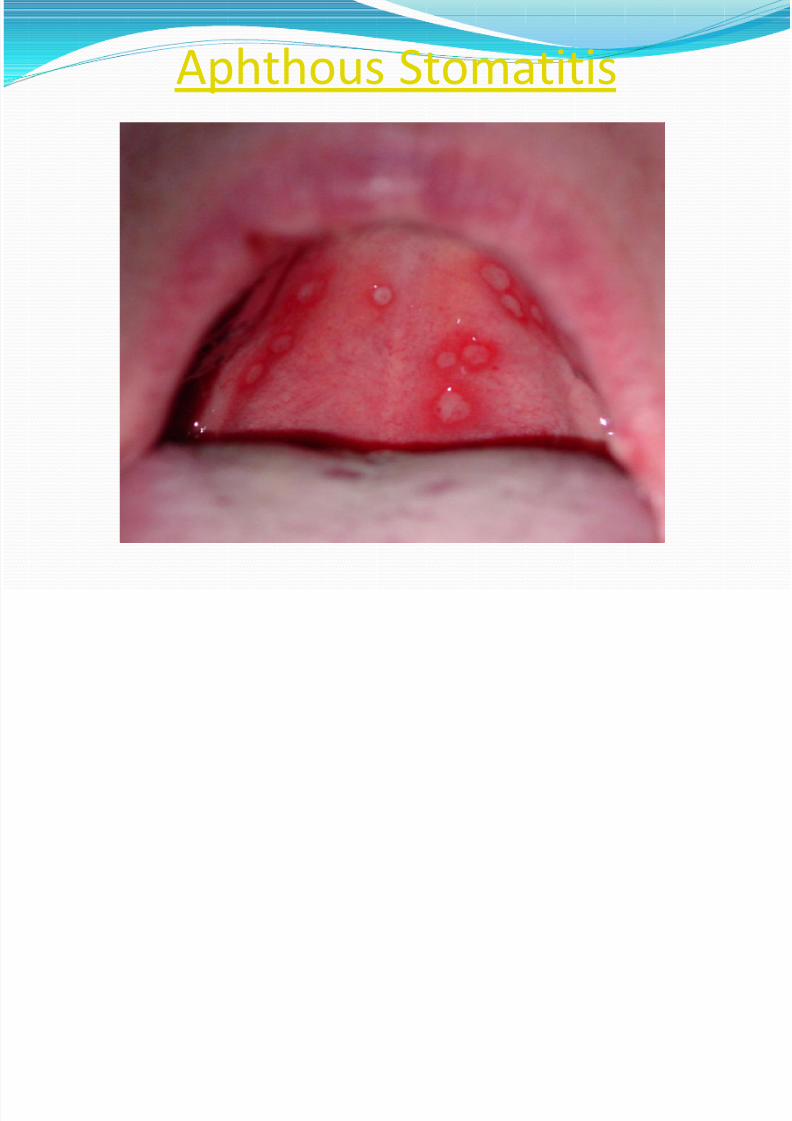
Aphthous Stomatitis
8/10/2019 Necrotizing Sialometaplasia -
http://slidepdf.com/reader/full/necrotizing-sialometaplasia- 23/33
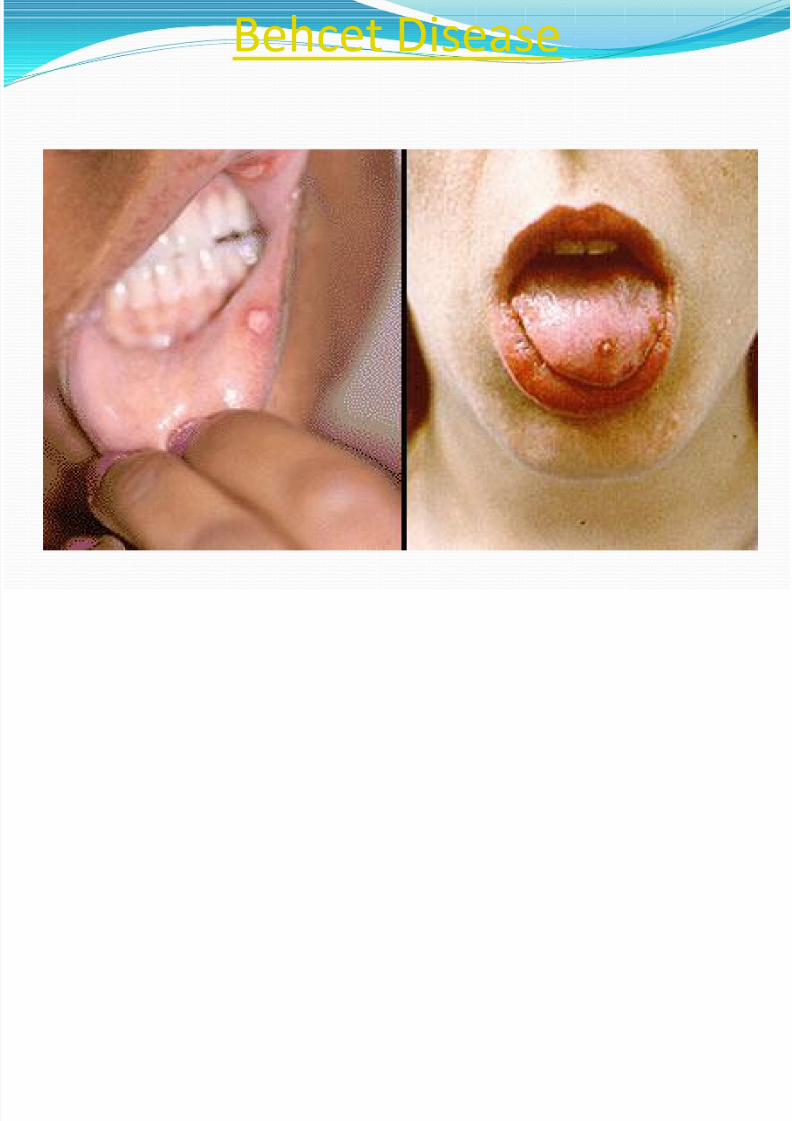
Behcet Disease
8/10/2019 Necrotizing Sialometaplasia -
http://slidepdf.com/reader/full/necrotizing-sialometaplasia- 24/33
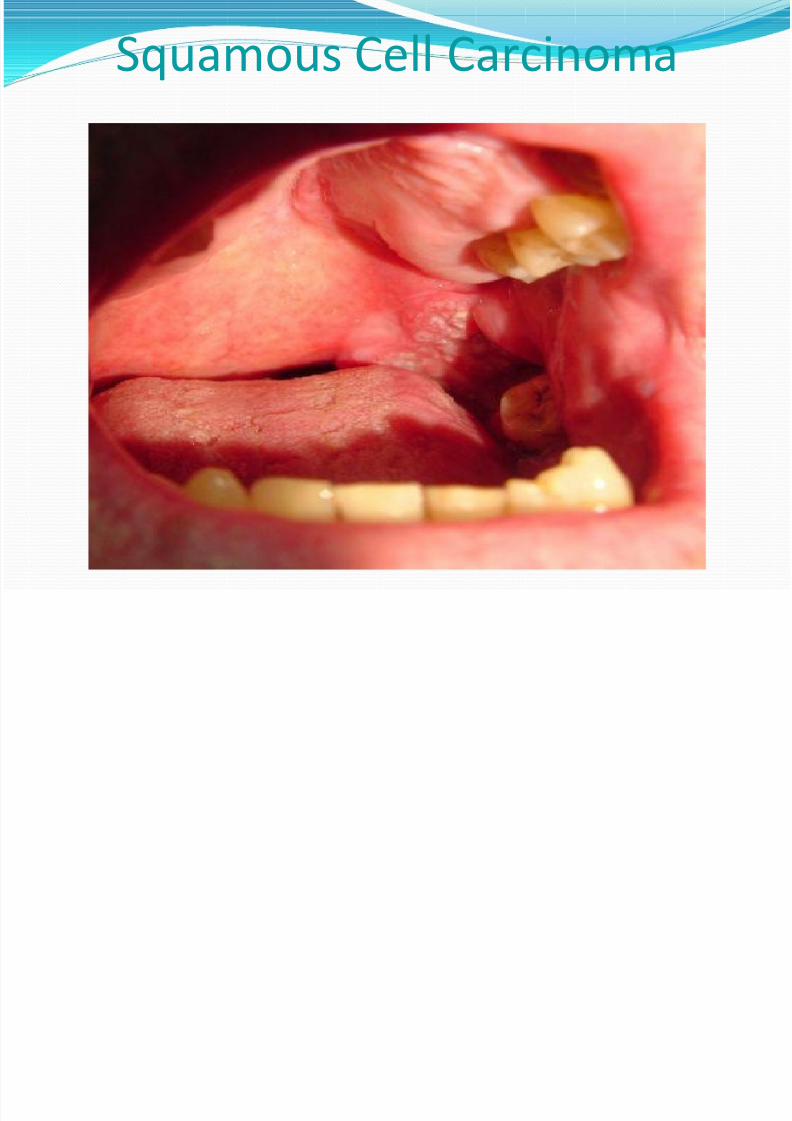
Squamous Cell Carcinoma

8/10/2019 Necrotizing Sialometaplasia -
http://slidepdf.com/reader/full/necrotizing-sialometaplasia- 25/33
Syphilis
8/10/2019 Necrotizing Sialometaplasia -
http://slidepdf.com/reader/full/necrotizing-sialometaplasia- 26/33
Procedur to work up
Imaging Studies
A definitive tissue diagnosis of
necrotizing sialometaplasia shouldexclude the need for radiographicimaging. If erosion of the palatal bone
occurs with or without perforation,radiologic examination may beperformed.
8/10/2019 Necrotizing Sialometaplasia -
http://slidepdf.com/reader/full/necrotizing-sialometaplasia- 27/33
Procedures Incisional biopsy is necessary to establish
the diagnosis of necrotizing sialometaplasia.
An inadequate biopsy specimen may lead tothe misdiagnosis of squamous cellcarcinoma or mucoepidermoid carcinoma.Findings in a superficial or limited biopsy
specimen may be misinterpreted as anonspecific ulcer or pseudoepitheliomatoushyperplasia of the surface mucosa.
8/10/2019 Necrotizing Sialometaplasia -
http://slidepdf.com/reader/full/necrotizing-sialometaplasia- 28/33
8/10/2019 Necrotizing Sialometaplasia -
http://slidepdf.com/reader/full/necrotizing-sialometaplasia- 29/33
Pseudoepitheliomatous hyperplasia of
the overlying mucosa can also bepresent, but the cytologic features ofthe squamous component are usually
bland. Occasionally, isolated mucouscells may be entrapped within thesquamous islands; these cells should
not be confused with those ofmucoepidermoid carcinoma.
8/10/2019 Necrotizing Sialometaplasia -
http://slidepdf.com/reader/full/necrotizing-sialometaplasia- 30/33
The microscopic differential diagnosis
for necrotizing sialometaplasiaincludes mucoepidermoid carcinomaand squamous cell carcinoma. Some
believe that subacute necrotizingsialadenitis is yet another entity thatoccurs within the spectrum ofnecrotizing sialometaplasia; it should
be distinguished from necrotizingsialometaplasia.
8/10/2019 Necrotizing Sialometaplasia -
http://slidepdf.com/reader/full/necrotizing-sialometaplasia- 31/33
Treatment
Analgesics may be needed, as well as
elimination of alcohol and tobacco
when usage is noted. There is no
surgical intervention, but a biopsy withmicroscopic evaluation is needed to
rule out other more serious disease
states so that early intervention may betaken.
8/10/2019 Necrotizing Sialometaplasia -
http://slidepdf.com/reader/full/necrotizing-sialometaplasia- 32/33
The lesion usually heals after
several weeks without anytreatment. In some cases, though,the tissue may take months to fully
respond. A bland baking soda and water mixture is often suggested
along with analgesics. Dietcounseling and nutritionalevaluation is crucial as well.
8/10/2019 Necrotizing Sialometaplasia -
http://slidepdf.com/reader/full/necrotizing-sialometaplasia- 33/33
PrognosisThe prognosis for necrotizing sialometaplasia isexcellent. Spontaneous resolution usually occurs
within weeks, although in the case presented, thelesion took more than 9 weeks to reach completehealing.
The average healing time for necrotizingsialometaplasia of the minor salivary glands of the
hard and soft palates is approximately 5 weeks.The size of the lesion and whether or not bonyperforation has occurred are clinical parametersthat may influence the healing time.





























