-
8/13/2019 Nausea and Vomitting
1/24
NAUSEA and VOMITTING
current_medical_diagnosis_treatment
Nausea & Vomiting
Nausea is a vague, intensely disagreeable sensation of sickness
or "queasiness" that may or
may not be followed by vomiting and is distinguished from
anorexia. Vomiting often follows,
as does retching (spasmodic respiratory and abdominal
movements). Vomiting should be
distinguished from regurgitation, the effortless reflux of
liquid or food stomach contents; and
from rumination, the chewing and swallowing of food that is
regurgitated volitionally after
meals.
The medullary vomiting center (which contains histamine
H1-receptors and muscarinic
cholinergic receptors) may be stimulated by four different
sources of afferent input: (1)
Afferent vagal and splanchnic fibers from the gastrointestinal
viscera are rich in serotonin 5-
HT3receptors; these may be stimulated by biliary or
gastrointestinal distention, mucosal or
peritoneal irritation, or infections. (2) Fibers of the
vestibular system, which have high
concentrations of histamine H1and muscarinic cholinergic
receptors. (3) Higher central
nervous system centers; here, certain sights, smells, or
emotional experiences may induce
vomiting. For example, patients receiving chemotherapy may
develop vomiting in
anticipation of its administration. (4) The chemoreceptor
trigger zone, located outside the
blood-brain barrier in the area postrema of the medulla, which
is rich in opioid, serotonin 5-
HT3, neurokinin 1 (NK1) and dopamine D2receptors. This region
may be stimulated by drugs
and chemotherapeutic agents, toxins, hypoxia, uremia, acidosis,
and radiation therapy.Although the causes of vomiting are many, a
simplified list is provided in Table 141.
Table 141. Causes of nausea and vomiting.
Visceral afferent
stimulation
Infections
Mechanical obstruction
Gastric outlet obstruction: peptic ulcer disease,
malignancy,
gastric volvulus
Small intestinal obstruction: adhesions, hernias, volvulus,
Crohn's disease, carcinomatosis
Dysmotility
Gastroparesis: diabetic, medications (metformin, acarbose,
pramlintide, exenatide), postviral, postvagotomy
Small intestine: scleroderma, amyloidosis, chronic
intestinal
pseudo-obstruction, familial myoneuropathies
Peritoneal irritation
Peritonitis: perforated viscus, appendicitis,
spontaneousbacterial peritonitis
-
8/13/2019 Nausea and Vomitting
2/24
Viral gastroenteritis: Norwalk agent, rotavirus
"Food poisoning": toxins fromBacillus cereus, Staphylococcus
aureus, Clostridium perfringens
Hepatitis A or B
Acute systemic infections
Hepatobiliary or pancreatic disorders
Acute pancreatitis
Cholecystitis or choledocholithiasis
Topical gastrointestinal irritants
Alcohol, NSAIDs, oral antibiotics
Postoperative
Other
Cardiac disease: acute myocardial infarction, congestive
heart
failure
Urologic disease: stones, pyelonephritis
CNS disorders Vestibular disorders
Labyrinthitis, Meniere's syndrome, motion sickness, migraine
Increased intracranial pressure
CNS tumors, subdural or subarachnoid hemorrhage
Migraine
Infections
Meningitis, encephalitis
Psychogenic
Anticipatory vomiting, bulimia, psychiatric disorders
Irritation of chemoreceptor
trigger zone
Antitumor chemotherapy
Drugs and medications
Calcium channel blockers
Opioids
Anticonvulsants
Antiparkinsonism drugs
-Blockers, antiarrhythmics, digoxin
Nicotine
Oral contraceptives
Cholinesterase inhibitors
Radiation therapy
Systemic disorders
-
8/13/2019 Nausea and Vomitting
3/24
Diabetic ketoacidosis
Uremia
Adrenocortical crisis
Parathyroid disease
Hypothyroidism
Pregnancy
Paraneoplastic syndrome
NSAIDs, nonsteroidal anti-inflammatory drugs; CNS, central
nervous system.
Complications of vomiting include dehydration, hypokalemia,
metabolic alkalosis, aspiration,rupture of the esophagus
(Boerhaave's syndrome), and bleeding secondary to a mucosal
tear
at the gastroesophageal junction (Mallory-Weiss syndrome).
Clinical Findings
Symptoms and Signs
Acute symptoms without abdominal pain are typically caused by
food poisoning, infectious
gastroenteritis, drugs, or systemic illness. Inquiry should be
made into recent changes in
medications, diet, other intestinal symptoms, or similar
illnesses in family members. The
acute onset of severe pain and vomiting suggests peritoneal
irritation, acute gastric or
intestinal obstruction, or pancreaticobiliary disease.
Examination may reveal fever, focal
tenderness or rigidity, guarding, or rebound tenderness.
Persistent vomiting suggestspregnancy, gastric outlet obstruction,
gastroparesis, intestinal dysmotility, psychogenic
disorders, and central nervous system or systemic disorders.
Vomiting that occurs in the
morning before breakfast is common with pregnancy, uremia,
alcohol intake, and increased
intracranial pressure. Vomiting immediately after meals strongly
suggests bulimia or
psychogenic causes. Vomiting of undigested food one to several
hours after meals is
characteristic of gastroparesis or a gastric outlet obstruction;
physical examination may reveal
a succussion splash. Patients with acute or chronic symptoms
should be asked about
neurologic symptoms that suggest a central nervous system cause
such as headache, stiff
neck, vertigo, and focal paresthesias or weakness.
Special Examinations
With vomiting that is severe or protracted, serum electrolytes
should be obtained to look for
hypokalemia, azotemia, or metabolic alkalosis resulting from
loss of gastric contents. Flat
and upright abdominal radiographs are obtained in patients with
severe pain or suspicion of
mechanical obstruction to look for free intraperitoneal air or
dilated loops of small bowel. If
mechanical small intestinal or gastric obstruction is thought
likely, a nasogastric tube is
placed for relief of symptoms. The cause of gastric outlet
obstruction is best demonstrated by
upper endoscopy, and the cause of small intestinal obstruction
is best demonstrated with
abdominal CT imaging. Gastroparesis is confirmed by nuclear
scintigraphic studies or 13C-
octanoic acid breath tests, which show delayed gastric emptying
and either upper endoscopyor barium upper gastrointestinal series
showing no evidence of mechanical gastric outlet
-
8/13/2019 Nausea and Vomitting
4/24
obstruction. Abnormal liver function tests or elevated amylase
or lipase suggest
pancreaticobiliary disease, which may be investigated with an
abdominal sonogram or CT
scan. Central nervous system causes are best evaluated with
either head CT or MRI.
Treatment
General Measures
Most causes of acute vomiting are mild, self-limited, and
require no specific treatment.
Patients should ingest clear liquids (broths, tea, soups,
carbonated beverages) and small
quantities of dry foods (soda crackers). For more severe acute
vomiting, hospitalization may
be required. Patients unable to eat and losing gastric fluids
may become dehydrated, resulting
in hypokalemia with metabolic alkalosis. Intravenous 0.45%
saline solution with 20 mEq/L
of potassium chloride is given in most cases to maintain
hydration. A nasogastric suction tube
for gastric decompression improves patient comfort and permits
monitoring of fluid loss.
Antiemetic Medications
Medications may be given either to prevent or to control
vomiting (see above). Combinations
of drugs from different classes may provide better control of
symptoms with less toxicity in
some patients. All of these medications should be avoided in
pregnancy. (For dosages, see
Table 142.)
Table 142. Common antiemetic dosing regimens.
Dosage Route
Serotonin 5-HT3antagonists
Ondansetron 832 mg or 0.15 mg/kg once daily IV
8 mg twice daily PO
Granisetron 1 mg or 0.01 mg/kg once daily IV
2 mg once daily PO
Dolasetron 100 mg or 1.8 mg/kg once daily IV
100 mg once daily PO
Palonosetron 0.25 mg once as a single dose 30 min before start
of
chemotherapy
IV
Corticosteroids
Dexamethasone 820 mg once daily IV
420 mg once or twice daily PO
Methylprednisolone 40100 mg once daily IV
Dopamine receptor antagonists
Metoclopramide 1020 mg or 0.5 mg/kg every 68 hours IV
1020 mg every 68 hours PO
-
8/13/2019 Nausea and Vomitting
5/24
Prochlorperazine 510 mg every 46 hours PO, IM, IV
25 mg suppository every 6 hours PR
Promethazine 25 mg every 46 hours PO, PR, IM,IV
Trimethobenzamide 250 mg every 68 hours PO
200 mg every 68 hours IM, PR
Sedatives
Diazepam 25 mg every 46 hours PO, IV
Lorazepam 12 mg every 46 hours PO, IV
IV, intravenously; PO, orally; IM, intramuscularly; PR, per
rectum.
Serotonin 5-HT3-receptor antagonists
Ondansetron, granisetron, dolasetron, and palonosetron are
effective in preventing
chemotherapy- and radiation-induced emesis when initiated prior
to treatment. Single-dose
administration schedules are as effective as multiple-dose
regimens. Although serotonin
antagonists are effective for the prevention of postoperative
nausea and vomiting, less
expensive alternatives (eg, dexamethasone or droperidol) are
equally effective.
Corticosteroids
Corticosteroids (eg, dexamethasone) have antiemetic properties,
but the basis for these effects
is unknown. These agents enhance the efficacy of serotonin
receptor antagonists for
preventing acute and delayed nausea and vomiting in patients
receiving moderately to highly
emetogenic chemotherapy regimens. For the prevention of
postoperative nausea and
vomiting, corticosteroids, serotonin antagonists, and droperidol
have efficacy; however,
combinations of these agents have additive benefit.
Neurokinin receptor antagonists
Aprepitant is a highly selective antagonist for NK1-receptors in
the area postrema. It is used
in combination with corticosteroids and serotonin antagonists
for the prevention of acute and
delayed nausea and vomiting with highly emetogenic chemotherapy
regimens. Combinedtherapy with aprepitant prevents acute emesis in
8090% and delayed emesis in > 70% of
patients treated with highly emetogenic regimens.
Dopamine antagonists
The phenothiazines, butyrophenones, and substituted benzamides
have antiemetic properties
that are due to dopaminergic blockade as well as to their
sedative effects. High doses of these
agents are associated with antidopaminergic side effects,
including extrapyramidal reactions
and depression. These agents are used in a variety of
situations. Cases of QT prolongation
leading to ventricular tachycardia (torsades de pointes) have
been reported in several patients
receiving droperidol, hence electrocardiographic monitoring is
recommended before and afteradministration.
-
8/13/2019 Nausea and Vomitting
6/24
Antihistamines and anticholinergics
These drugs (eg, meclizine, dimenhydrinate, transdermal
scopolamine) may be valuable in
the prevention of vomiting arising from stimulation of the
labyrinth, ie, motion sickness,
vertigo, and migraines. They may induce drowsiness.
Sedatives
Benzodiazepines are used in psychogenic and anticipatory
vomiting.
Cannabinoids
Marijuana has been used widely as an appetite stimulant and
antiemetic. Pure 9-
tetrahydrocannabinol (THC) is the major active ingredient in
marijuana and is available by
prescription as dronabinol. In doses of 515 mg/m2, oral
dronabinol is effective in treatingnausea associated with
chemotherapy, but it is associated with central nervous system
sideeffects in most patients.
The_Washington_Manual_of_Medical
Nausea and Vomiting
GENERAL PRINCIPLES
Etiology
Nausea and vomiting may result from side effects of medications,
systemic illnesses,central nervous system (CNS) disorders, and
primary GI disorders.
Vomiting that occurs during or immediately after a meal can
result from acute pyloricstenosis (e.g., pyloric channel ulcer) or
from functional disorders.
Vomiting within 30 to 60 minutes after a meal may suggest
gastric or duodenalpathology.
Delayed vomiting after a meal with undigested food from a
previous meal can suggestgastric outlet obstruction or
gastroparesis.
Symptoms lasting longer than 1 month in duration are considered
chronic(Gastroenterology 2001;120:261).
P.585
DIAGNOSIS
Clinical Presentation
History
Bowel obstruction and pregnancy should be ruled out. Medication
lists should be scrutinized, and systemic illnesses (acute and
chronic)
should be evaluated as etiologies or contributing factors.
TREATMENT
-
8/13/2019 Nausea and Vomitting
7/24
Correction of fluid and electrolyte imbalances is an important
supportive measure. Oral intake should be withheld or limited to
clear liquids. Many patients with self-
limited illnesses require no further therapy.
NG decompression may be required for patients with bowel
obstruction or protractednausea and vomiting of any etiology.
Patients with protracted nausea and vomiting may sometimes
require enteral feedingthrough jejunal tubes, or rarely even total
parenteral nutrition.
Medications
Empiric pharmacotherapy is often initiated while investigation
is in progress, or when the
etiology is thought to be self-limited.
Phenothiazines and related agents. Prochlorperazine (Compazine),
5 to 10 mg PO tid-qid, 10 mg IM or IV q6h, or 25 mg PR bid;
promethazine (Phenergan), 12.5 to 25.0
mg PO, IM, or PR q4-6h; and trimethobenzamide (Tigan), 250 mg PO
tid-qid, 200 mg
IM tid-qid, or 200 mg PR tid-qid are effective. Drowsiness is a
common side effect,
and acute dystonic reactions or other extrapyramidal effects may
occur. Dopamine antagonists include metoclopramide (10 mg PO 30
minutes before meals
and at bedtime, or 10 mg IV prn), a prokinetic agent that also
has central antiemetic
effects. Drowsiness and extrapyramidal reactions may occur, and
a warning has been
issued by the FDA regarding the risk of tardive dyskinesia with
high dose or long-
term use; tachyphylaxis may limit long-term efficacy.
Domperidone is an alternate
agent that does not cross the blood-brain barrier and therefore
has no CNS side
effects; however, it is not uniformly available.
Antihistaminic agents are most useful for nausea and vomiting
related to motionsickness, but may also be useful for other causes.
Agents used include
diphenhydramine (Benadryl, 25 to 50 mg PO q6-8h, or 10 to 50 mg
IV q2-4h),
dimenhydrinate (Dramamine, 50 to 100 mg PO or IV q4-6h), and
meclizine (Antivert,
12.5 to 25 mg 1 hour before travel).
Serotonin 5-HT3receptor antagonists. Ondansetron (Zofran, 0.15
mg/kg IV q4h forthree doses or 32 mg IV infused over 15 minutes
beginning 30 minutes before
chemotherapy) is effective in chemotherapy-associated emesis. It
can also be used in
emesis that is refractory to other medications (4 to 8 mg PO or
IV up to q8h),
especially the sublingual formulation. Granisetron (Kytril, 10
mcg/kg IV for one to
three doses 10 minutes apart, or 1 mg PO bid) is also
effective.
Neurokinin-1 (NK-1) receptor antagonist. Aprepitant (Emend, 125
mg PO day 1, 80mg PO days 2 and 3) is an alternative agent
currently indicated only for
chemotherapy-induced nausea and vomiting.
common_symptoms_guide
Nausea-Vomiting (Pediatric)
HISTORYDESCRIPTORS
GENERAL DESCRIPTORS: refer to inside cover.
CHARACTER: type and amount of vomiting; how frequent.
AGGRAVATING FACTORS: fright; excitement; certain foods
(specify); possibility of drugor poison ingestion, or head
injury.
-
8/13/2019 Nausea and Vomitting
8/24
Relieving Factors: burping the infant.
ASSOCIATED SYMPTOMS
Fever; weight loss; headache; earache; sore throat; vomiting
blood; abdominal distention;
diarrhea; decrease in bowel movements; crying on urination; dark
urine.
MEDICATIONS
Any.
ENVIRONMENTAL HISTORY
Recent contact with others suffering from vomiting,
hepatitis.
PHYSICAL EXAMINATIONMEASURE: pulse, weight, height. Compare to
growth chart.
EYES: fundi absent venous pulsations, or papilledema.
NECK: stiffness.
ABDOMEN: check for distention, masses, apparent
tenderness.P.252
RECTAL: stool for occult blood.
SKIN: turgor; purpura.
SPECIAL: if possible, check vomitus for occult blood.
GENERAL CONSIDERATIONS
Abdominal pain see ABDOMINAL PAIN (PEDIATRIC).
Abdominal trauma see TRAUMA.
DIAGNOSTIC ISSUES -----HISTORY PHYSICAL EXAM
ACUTE
GASTROENTERITIS OR
SYSTEMIC INFECTION(seeDIARRHEA,
ACUTE for other
considerations)
Acute vomiting and fever often
accompanying many childhood
infections (e.g., otitis media,
tonsillitis, kidney infection).Diarrhea may be noted.
Fever is common. Normal
abdominal examination.
Abnormal ear or throat exam
may be present.
HEPATITISAs in acute gastroenteritis above.
Dark urine and a contact with
someone who has had hepatitis may
be noted.
Hepatic tenderness or
enlargement.
GASTROINTESTINAL OBSTRUCTIONHigh bowel obstruction
(pyloric stenosis orduodenal atresia)
Persistent vomiting with large
amounts of food in vomitus. No bilein vomitus. May vomit
blood.
Weight loss. Decreased skin
turgor may be noted as well asa flaccid abdomen by
-
8/13/2019 Nausea and Vomitting
9/24
Usually noted in first 3 months of
life.
examination.
Lower bowel obstruction
(intussusception,
Hirschsprung's disease,
meconium plug)
Green bile in vomitus. Abdominal
distention. Decrease or cessation of
bowel movement. Rare in the child
over 2 years of age.
Abdominal distention and
hyperresonance. Absent bowel
sounds alternating with high
pitched rushes. Stools may bepositive for occult blood.
NORMAL INFANTILE REGURGITATION(gastroesophageal reflux) Variable
amount and frequency of
vomiting; common in premature
infants. Often related to excessive
stimulation after feeding. May be
relieved by burping the infant
frequently or changing feeding
schedule.
Normal examination.
CEREBRAL IRRITATION(meningitis, brain tumor,
severe head injury)
Head holding, headache, lethargy, or
projectile vomiting may be noted.
Symptoms progress over hours to
days.
Fever, decreased pulse, and
stiff neck are common.
Bulging fontanels or
papilledema may be noted.
FOLLOWING POISON OR MEDICATION INGESTIONHistory of ingestion may
be noted. May be normal.
RESULTING FROM METABOLIC DISEASE (gluten sensitivity,
phenylketonuria)
Newborns may begin vomiting soon
after birth or later in life as certain
foods are introduced.
Weight loss and decreased
skin turgor may be present.
UNCLEARThe older child may vomit from
fright, excitement, or to get
attention.
Normal
Kochar_Clinical_Medicine_for_Students
Nausea and Vomiting
Monica Ziebert
Nausea is the subjective disagreeable sensation of the need to
vomit that may or may not
result in vomiting. Vomiting (emesis) is the forcible expulsion
of the upper gastrointestinal
contents through the mouth. This is different from
regurgitation, which is the passive passage
of the gastric contents into the mouth. Vomiting is controlled
by the vomiting center in the
medulla and is triggered by afferent neural pathways from the
gastrointestinal (GI) tract in
response to distention, mucosal injury, peritoneal irritation or
infection. Other non-GI sources
of input include the cerebral cortex, when noxious thoughts,
emotional experiences, sights, orsmells provoke vomiting. The
vestibular apparatus signals the vomiting center during motion
-
8/13/2019 Nausea and Vomitting
10/24
sickness and inner ear disorders. Finally, the chemoreceptor
trigger zone within the medulla
provides input to the vomiting center in response to bloodborne
stimuli (such as drugs, toxins,
and metabolic disorders) provoke vomiting.
Differential Diagnosis
There are a myriad of causes of nausea and vomiting, which can
be included in the
differential diagnosis. They range from mild, quickly resolving
illnesses to serious, life-threatening conditions. The causes can
be classified according to conditions within the GI
tract and conditions outside the GI tract (Table 21.1).
The history and physical examination provide clinic clues that
will narrow the large
differential diagnosis associated with the causes of nausea and
vomiting (Table 21.2). The
history should reveal information on symptom characteristics
such as severity, duration of
symptoms, frequency, provocative features such as relationship
to meals and medications,
and the quality and quantity of vomits. Acute onset of nausea
and vomiting in the setting of
severe abdominal pain usually points to a gastrointestinal cause
such as obstruction or
peritoneal irritation from one of the inflammatory conditions
(appendicitis, cholecystitis, and
pancreatitis). Acute symptoms without abdominal pain can be due
to gastroenteritis,
medications, central nervous system (CNS) conditions like
hemorrhage and infection, andmyocardial infarction.
Chronic nausea and vomiting can occur in GI conditions
associated with impaired motor
function (dysmotility), CNS diseases, and systemic illnesses
ranging from malignancy to
endocrinopathies. Intermittent and recurrent symptoms suggest
cyclic vomiting syndrome, a
rare disorder of unknown etiology but strongly related to
migraine headaches. Nausea and
vomiting that occurs mostly in the morning favors pregnancy,
alcohol use, uremia, and
increased intracranial pressure. Provocative features such as
knowing the relationship of
symptoms to eating can be helpful. The onset of nausea and
vomiting immediately after
eating strongly suggests an eating disorder, whereas
postprandial symptom onset can point to
obstruction or gastroparesis. In gastroparesis, patients will
also often complain of early
satiety. The vomitus might even contain ingested food from the
previous day. Small bowel
obstruction is associated with large volumes of bilious emesis
with colicky periumbilical
pain. Other important distinguishing quality features of the
vomitus are whether it is feculent
or projectile. A feculent vomitus occurs in a distal small bowel
obstruction while projectile
vomiting
P.117
occurs in pyloric (or gastric outlet) obstruction or in
intracerebral process causing increased
intracranial pressure. Pyloric obstruction may also produce a
sensation of epigastric fullness,
blunt pain, nausea, and weight loss and can lead to the vomiting
of food consumed even days
before. Table 21.1 Causes of nausea and vomiting
Conditions within the GI
tract Conditions outside the GI tract
Obstructive
Pyloric obstruction Small bowel
obstruction
Colonic obstruction
Enteric infections
Pregnancy
Hyperemesis gravidarum
Cardiopulmonary disease
Myocardial infarction
Medications
Cancerchemotherapy
Antibiotics Digoxin Oral hypoglycemics Oral contraceptives
Nonsteroid anti-
-
8/13/2019 Nausea and Vomitting
11/24
Viral gastroenteritis Bacterial gastroenteritis Hepatitis
Inflammatory diseases
Cholecystitis Pancreatitis Appendicitis
Impaired motility
Gastroparesis Intestinal pseudo-
obstruction
Functional dyspepsia Gastroesophageal
reflux
Irritable bowelsyndrome
Malignancy
Pancreatic cancer Metastatic disease Radiation therapy
Mucosal injury
Peptic ulcer disease Gastritis Esophagitis
Cardiomyopathy
Labyrinthine diesease
Motion sickness Viral Labyrinthitis Malignancy
Intracerebral disorders (increased
intracranial pressure)
Brain tumor Hemorrhage Abscess Pseudotumor cerebri
Seizure disorders
Demyelinating diseases
Migraine
CNS infections
Meningitis Encephalitis
Cyclic vomiting syndrome
Psychiatric illness
Anorexia and bulimia Depression Anxiety Psychogenic
inflammatory drugs
Beta blockers Opioids Theophylline Iron supplements
Toxins
Ethanol
Endocrine/metabolic disease
Uremia Liver failure Ketoacidosis Thyroid and
parathyroid disease
Adrenalinsufficiency
Nephrolithiasis (renal colic)
Postoperative vomiting
Adapted from Kaspar DL.Harrison's Principles of Internal
Medicine,16th ed. New York:
McGraw-Hill, 2004. With permission.
The identification of associated symptoms can be the key to
further narrowing the
differential. Neurologic symptoms such as vision changes,
headache, photophobia, and
vertigo will point to a CNS or labyrinthine cause. The presence
of other GI symptoms like
constipation and diarrhea can be important. For example,
diarrhea along with nausea and
vomiting suggests gastroenteritis. The presence of constipation
can lead to a consideration of
colon obstruction or pseudo-obstruction. The latter condition is
impaired motility of either the
small bowel and colon resulting retention of food residue,
abdominal distention, pain, and
altered bowel movements. Pseudo-obstruction can be idiopathic or
caused by inheritedconditions or systemic diseases including a
malignant or paraneoplastic process.
-
8/13/2019 Nausea and Vomitting
12/24
Table 21.2 Clinical clues associated with the causes of nausea
and vomiting
Clinical clues Possible cause of nausea and vomiting
Duration
Acute onset GI tract:Obstruction
Gastroenteritis
Inflammatory condition
Non-GI tract:Toxins and medications
Meningitis
CNS hemorrhage
Myocardial infarction
QualityBilious Small bowel obstructionFeculent Small bowel
obstruction or rarely colonicProjectile Pyloric obstruction or
intracerebral conditionHematemesis Peptic ulcer disease, esophageal
varices, esophagitis (GERD), Mallory-Weiss tearPartially digested
food Gastroparesis or pyloric obstruction
QuantityLarge volumes Small bowel obstruction
Frequency
Only in the morning Pregnancy, intracerebral condition, uremia,
and alcohol useRecurrent and intermittent Cyclic vomiting
syndrome
Provocative features
Immediately after eating Eating disorder (bulimia)>1 hour
after eating Gastroparesis or pyloric obstructionWhile a passenger
in car Motion sicknessRecumbent posture Intracranial involving the
posterior fossaAfter taking medications MedicationsRecent picnic
with potato salad Bacterial gastroenteritis (food poisoning )
Associated symptomsCrampy, colicky pain Obstructive
conditionsAbdominal pain relieved with vomiting Pyloric
obstruction
Bloating Colonic obstruction or pseudo-obstructionEpigastric
pain radiating to back PancreatitisRight upper quadrant abdominal
pain CholecystitisRight lower quadrant abdominal pain
AppendicitisAbdominal pain radiating to groin Nephrolithiasis
(renal colic)Jaundice, dark urine, light stools Hepatitis or
choledocholithiasisConstipation Colonic obstruction or
pseudo-obstructionDiarrhea, myalgia, headache Viral
gastroenteritisChest pain and diaphoresis Myocardial
infarctionHeadache Migraine, meningitis, gastroenteritis, or
intracerebral process
Neck stiffness, photophobia, altered mental status
Meningitis
Vertigo and ataxia LabyrinthitisVertigo and tinnitus Mnire's
disease
-
8/13/2019 Nausea and Vomitting
13/24
Altered mental status CNS infection or toxin ingestionMissed
menstrual period Early pregnancy
Associated comorbid conditions
Diabetes Ketoacidosis or gastroparesis
History of abdominal surgery Small bowel obstructionHeart
disease Myocardial infarctionKidney disease UremiaPeptic ulcer
disease Pyloric obstructionPregnancy Hyperemesis gravidarum, acute
fatty liver, HELLP syndromeMigraine headaches Cyclic vomiting
syndromePhysical exam findings
Fever Infection or inflammatory conditionsQuiet bowel sounds
Pseudo-obstructionHigh-pitched bowel sounds Mechanical
obstructionSuccussion splash Pyloric obstruction
Tympanic abdomen Obstructive conditionsRebound and guarding
Inflammatory disordersPapilledema Intracerebral disorders
Nystagmus Labrynthine disorderKernig and Brudzinski signs
MeningitisTachycardia, gallops, edema CardiomyopathyDental enamel
erosion BulimiaAdapted from Tierney LM, Henderson M. The Patient
History: Evidence-based approach.
New York: McGraw-Hill, 2004.
Nausea and vomiting are also associated with many medications
and co-existing medical
conditions ranging from pregnancy to diabetes mellitus.
Pregnancy is associated with
hyperemesis gravidum, severe nausea, and vomiting occurring in
the first trimester. Two
other conditions associated with nausea and vomiting and
pregnancy, acute fatty liver and
HELLP (hemolysis, elevated liver tests, low platelets) syndrome,
occur in the second and
third trimester. Diabetics are prone to an impaired motility
disorder known as gastroparesis or
chronic delayed gastric emptying.
Pyloric (or gastric outlet) obstruction in adults is most
commonly associated with peptic ulcer
disease.
The physical examination should be guided by the information
from the history. If a GI tract
cause is suspected, then a focused abdominal and rectal exam
will be essential. For example,bowel sounds may be quiet or absent
in patients with a pseudo-obstruction, whereas high-
pitched bowel sounds could suggest an early mechanical bowel
obstruction. A distended and
tympanic abdomen suggests a bowel obstruction. Tenderness to
palpation with rebound or
guarding raises the strong possibility of an inflammatory
disorder with associated peritoneal
signs. A succussion splash can be heard during auscultation of
the abdomen in patients with a
gastric outlet obstruction or gastroparesis when the patient is
passively shaken. Rectal
examination can reveal melena or hematochezia to suggest GI
hemorrhage from a specific
cause like peptic ulcer disease (PUD) or gastritis or from a
complication of vomiting like a
Mallory-Weiss tear. If a non-GI tract cause is suspected, then
the physical examination
findings should complement the history. For example, in patients
with a suspected
intracerebral condition caused by increased intracranial
pressure, the neurologic examinationP.120
-
8/13/2019 Nausea and Vomitting
14/24
may reveal papilledema, focal neurologic deficits, or visual
field cuts. For example,
pseudotumor cerebri is a condition affecting obese young women
and characterized with
intracranial hypertension not caused by a mass. Patients present
with headache, nausea, and
pulsatile tinnitus. On examination, they will universally have
papilledema and many will
have a sixth nerve deficits.
EvaluationThe evaluation of nausea and vomiting begins with an
assessment of the acuity and severity
of symptoms and any immediate complications. Certain causes and
complications of nausea
and vomiting are emergencies and as such must be recognized
immediately in order that
urgent diagnostic tests and therapy are provided. These
conditions include obstruction, intra-
abdominal perforation, peritonitis, myocardial infarction, CNS
infection, intracranial
hemorrhage, toxic ingestion, aspiration, and gastrointestinal
hemorrhage.
Severe or protracted nausea and vomiting can present with
orthostatic hypotension and
lethargy secondary to dehydration and electrolyte disturbances
such as hypokalemia,
azotemia, or metabolic alkalosis. These also must be addressed
as soon as possible.In the nonurgent presentation of nausea and
vomiting, the findings from the thorough history
and examination will point to a gastrointestinal or
nongastrointestinal cause and guide the
selection of appropriate tests such as routine hematologic
tests, biochemical screening, drug
levels, toxicology, imaging (plain abdominal radiograph,
ultrasounds, computed tomography
scans, magnetic resonance imaging), gastric emptying studies,
and endoscopy.
Sleisenger_2010
Nausea, retching, and vomiting may occur separately or together.
When they occur together
they are often in sequence, as manifestations of the various
physiologic events that
integrate the emetic reflex. Vomiting is a complex act that
requires central neurologic
coordination, whereas nausea and retching do not imply
activation of the vomiting reflex.
When nausea, retching, or vomiting manifest as isolated
symptoms, their clinical
significance may differ from the stereotypical picture of
emesis.[1,2]
Nausea is an unpleasant subjective sensation that most people
have experienced at some
point in their lives and usually recognize as a feeling of
impending vomiting in the
epigastrium or throat.
Retching consists of spasmodic and abortive respiratory
movements with the glottis closed.
When part of the emetic sequence, retching is associated with
intense nausea and usually,
but not invariably, culminates in the act of vomiting.
Vomiting is a partially voluntary act of forcefully expelling
gastric or intestinal content
through the mouth. Vomiting must be differentiated from
regurgitation, an effortless reflux
of gastric contents into the esophagus that sometimes reaches
the mouth but is not usually
associated with the forceful ejection typical of vomiting (see
Chapter 12).
PATHOPHYSIOLOGY
-
8/13/2019 Nausea and Vomitting
15/24
The mechanism of vomiting has been well characterized in
experimental animals and
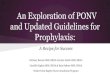
humans (Fig. 14-1).[3] Neurologic coordination of the various
components of vomiting is
provided by the emetic center (or vomiting center) located in
the medulla, specifically in the
dorsal portion of the lateral reticular formation in the
vicinity of the fasciculus solitarius. The
afferent neural pathways that carry activating signals to the
emetic center arise from manylocations in the body. Afferent neural
pathways arise from various sites along the digestive
tractthe pharynx, stomach, and small intestine. Afferent
impulses from these organs are
relayed at the solitary nucleus (nucleus tractus solitarius) to
the emetic center. Afferent
pathways also arise from nondigestive organs such as the heart
and testicles. Pathways from
the chemoreceptor trigger zone (CTZ) located in the area
postrema on the floor of the
fourth ventricle activate the emetic center. Despite its central
location, the CTZ is outside, at
least in part, the blood-brain barrier and serves primarily as a
sensitive detection apparatus
for circulating endogenous and exogenous molecules that may
activate emesis. Finally,
pathways arise from other central nervous system structures,
including the cortex,
brainstem, and vestibular system, via the cerebellum.
Figure 14-1. Schematic of the proposed neural pathways that
mediate vomiting. GI,gastrointestinal; 5-HT,
5-hydroxytryptamine.
-
8/13/2019 Nausea and Vomitting
16/24
The circuitry of the emetic reflex involves multiple
receptors.[4] The following elements are
the most relevant to clinical issues:
1. Stimulation of the 5-hydroxytryptamine3 (5-HT3) serotonin
receptor
provokes release of dopamine, which in turn stimulates dopamine
D2 receptors in the
emetic center, thereby activating the emetic sequence. This
sequence is the basis for the
pharmacodynamic action of antiemetic agents, such as
ondansetron, a 5-HT3 receptor
inhibitor that is effective in the treatment of
chemotherapy-induced vomiting,[5] and
metoclopramide, a dopamine D2 receptor antagonist.[6]
2. Histamine H1 and muscarinic M1 receptors, which are abundant
in the
vestibular center and solitary nucleus, constitute the preferred
pharmacologic targets for
inhibiting motion sickness, vestibular nausea, and
pregnancy-related emesis.[7]
3. Cannabinoid CB1 receptors in the dorsal vagal complex inhibit
the emeticreflex.[8,9] Cannabinoid agonists also modulate 5-HT3 ion
channels. Thus, the CB and 5-HT3
receptor systems colocalize and interact in the
brainstem.[10]
4. Neurokinin-1 (NK-1) receptors located in the area postrema
and the solitary
nucleus bind to substance P and are part of the terminal emetic
pathways. NK-1 antagonists
reduce emesis induced by peripherally and centrally acting
emetogens. 5-HT3 receptors
appear to be involved to a greater extent in centrally induced
emesis than in peripherally
induced emesis. Therefore, NK-1 receptor antagonists appear to
be more efficacious than
5HT3 receptor inhibitors and other known antiemetic drugs in
reducing vomiting induced by
a variety of causes. Conversely, they may have less potent
antinausea effects.[87]
When activated, the emetic center sets into motion, through
neural efferents, the various
components of the emetic sequence.[11] First, nausea develops as
a result of activation of
the cerebral cortex; the stomach relaxes concomitantly, and
antral and intestinal peristalsis
are inhibited. Second, retching occurs as a result of activation
of spasmodic contractions of
the diaphragm and intercostal muscles combined with closure of
the glottis. Third, the act of
vomiting occurs when somatic and visceral components are
activated simultaneously. Thecomponents include brisk contraction
of the diaphragm and abdominal muscles, relaxation
of the lower esophageal sphincter, and a forceful retrograde
peristaltic contraction in the
jejunum that pushes enteric content into the stomach and from
there toward the
mouth.[12] Simultaneously, protective reflexes are activated.
The soft palate is raised to
prevent gastric content from entering the nasopharynx,
respiration is inhibited
momentarily, and the glottis is closed to prevent pulmonary
aspiration, which is a
potentially serious complication of vomiting. Other reflex
phenomena that may accompany
this picture include hypersalivation, cardiac arrhythmias, and
passage of gas and stool
rectally.
-
8/13/2019 Nausea and Vomitting
17/24
Current_Pediatric_Diagnosis_Treatment
Vomiting
Vomiting is an extremely complex, poorly understood activity.
The centers controlling andcoordinating vomiting are in the
paraventricular nuclei of the brain. These nuclei receive
afferent input from many sources: drugs and neurotransmitters in
cerebrospinal fluid, the
chemoreceptor trigger zone (CTZ) near the distal fourth
ventricle, the vestibular apparatus of
the ear, the GI tract and other abdominal organs, and even from
higher cortical areas. Vagal
afferents from gut to brain are stimulated by ingested drugs and
toxins, mechanical stretch,
inflammation, and local neurotransmitters. Additionally, local
feedback loops in the gut also
appear capable of initiating vomiting.
Vomiting is the presenting symptom of many pediatric conditions.
It is the pediatrician's
difficult job to find the underlying cause. The most common
cause of vomiting in childhood
is probably acute viral gastroenteritis. However, obstruction
and acute or chronicinflammation of the GI tract and associated
structures are also major causes. Central nervous
system inflammation, pressure, or tumor may cause vomiting.
Metabolic derangements
associated with inborn errors of metabolism, sepsis, and drug
intoxication can stimulate either
the CTZ or the brain directly to promote vomiting.
Regurgitation associated with GE reflux of infants should be
distinguished from vomiting. In
this instance, spontaneous relaxation of the lower esophageal
sphincter creates a common
cavity between the stomach and esophagus. Because the resting
pressure of the thorax is
negative, the mildly positive pressure of the abdominal cavity
(~ 6 mm Hg) pushes gastric
contents into the esophagus, causing an effortless flow into the
mouth. Occasionally,
regurgitated fluid stimulates the pharyngeal afferents and
provokes gagging or even acomplete vomiting complex.
Control of vomiting with medication is rarely needed in acute
gastroenteritis and should not
be attempted in other patients until the source is clear.
Antihistamines and anticholinergics
are appropriate for motion sickness because of their
labyrinthine effects. 5-HT3receptor
antagonists (ondansetron, granisetron) are useful for vomiting
associated with surgery and
chemotherapy. Benzodiazepines, corticosteroids, and substituted
benzamides are also used in
chemotherapy-induced vomiting. Butyrophenones (droperidol,
haloperidone) are powerful
drugs that block the D2 receptor in the CTZ and are used for
intractable vomiting in acute
gastritis, chemotherapy, and after surgery. Phenothiazines are
helpful in chemotherapy, cyclicvomiting, and acute GI infection but
are not recommended for outpatient use because of
extrapyramidal side effects.
Cyclic Vomiting Syndrome
Clinical Findings
Cyclic vomiting syndrome (CVS) is characterized by recurrent
episodes of stereotypical
vomiting in children usually older than 1 year of age. The
emesis is forceful and frequent,
occurring up to six times per hour for up to 72 hours or more.
Episode frequency ranges from
two to three per month to less than one per year. Nausea,
retching, and small-volume biliousemesis continue even after the
stomach is emptied. Hematemesis secondary to forceful
-
8/13/2019 Nausea and Vomitting
18/24
vomiting may occur. Patients experience abdominal pain,
anorexia, and rarely, diarrhea.
Autonomic symptoms, such as pallor, sweating, temperature
instability, and lethargy are
common and give the patient a very ill appearance. The episodes
end suddenly, often after a
period of sleep. In some children, dehydration, electrolyte
imbalance, and shock may occur.
Between episodes, the child is completely healthy.
The cause of CVS is unknown; however, a similarity to migraine
has long been recognized.
Family history is positive for migraine in 5070% of cases and
many patients developmigraine headaches as adults. Research
suggests that abnormalities of neurotransmitters and
hormones provoke CVS. About one quarter of patients have typical
migraine symptoms
during episodes: premonitory sensation, headache, photophobia,
and phonophobia.
Identifiable triggers include infection, positive or negative
emotional stress, diet (chocolate,
cheese, monosodium glutamate), menses, or motion sickness.
Differential Diagnosis
Conditions that mimic CVS include drug toxicity, increased
intracranial pressure, seizures,brain tumor, Chiari malformation,
recurrent sinusitis, choledochal cyst, gallstones, recurrent
small bowel obstruction, inflammatory bowel disease, familial
pancreatitis, obstructive
uropathy, recurrent urinary infection, diabetes, mitochondrial
diseases, disorders of fatty and
organic acid metabolism, adrenal insufficiency, and Mnchausen
syndrome by proxy.
Although tests for GE reflux are often positive in these
patients, it is unlikely that GE reflux
and CVS are related.
Treatment
Avoidance of triggers prevents spells in some patients. Sleep
can also end a spell although
some children awaken and resume vomiting. Diphenhydramine or
lorazepam are used at the
onset of spells in some children to reduce nausea and induce
sleep. Early use of antimigraine
medications (sumatriptan), antiemetics (ondansetron), or
antihistamines can abort spells in
some patients. Once a spell is well established, intravenous
fluids are often required to end it.
With careful supervision, some children with predictable spells
can receive intravenous fluids
at home. Several approaches usually are tried before an
effective therapy is found. Preventing
spells with prophylactic propranolol, amitriptyline, or
antihistamines is effective in some
patients with frequent or disabling spells. Some patients have
been successfully treated with
anticonvulsants.
Nelson_Textbook_of_Pediatrics__18th_Edition
VOMITING.
Vomiting is a highly coordinated reflex process that may be
preceded by increased salivationand begins with involuntary
retching. Violent descent of the diaphragm and constriction of
the abdominal muscles with relaxation of the gastric cardia
actively force gastric contents
back up the esophagus. This process is coordinated in the
medullary vomiting center, which
is influenced directly by afferent innervation and indirectly by
the chemoreceptor trigger zone
-
8/13/2019 Nausea and Vomitting
19/24
and higher central nervous system (CNS) centers. Many acute or
chronic processes can cause
vomiting ( Table 303-1 and Table 303-3 ).
TABLE 303-3 -- Causes of Gastrointestinal Obstruction
ESOPHAGUS
Congenital
Esophageal atresia
Vascular rings
Schatzki ring
Tracheobronchial remnant
Acquired
Esophageal stricture
Foreign bodyAchalasia
Chagas disease
Collagen vascular disease
STOMACH
Congenital
Antral webs
Pyloric stenosis
Acquired
Bezoars/foreign body
Pyloric stricture (ulcer)
Chronic granulomatous disease of childhood
Eosinophilic gastroenteritis
Crohn disease
Epidermolysis bullosa
SMALL INTESTINE
CongenitalDuodenal atresia
Annular pancreas
Malrotation/volvulus
Malrotation/Ladd bands
Ileal atresia
Meconium ileus
Meckel diverticulum with volvulus or intussusception
Inguinal hernia
Intestinal duplication
-
8/13/2019 Nausea and Vomitting
20/24
Acquired
Postsurgical adhesions
Crohn disease
Intussusception
Distal ileal obstruction syndrome (cystic fibrosis)
Duodenal hematoma
Superior mesenteric artery syndrome
COLON
Congenital
Meconium plug
Hirschsprung disease
Colonic atresia, stenosis
Imperforate anusRectal stenosis
Pseudo-obstruction
Volvulus
Colonic duplication
Acquired
Ulcerative colitis (toxic megacolon)
Chagas disease
Crohn disease
Fibrosing colonopathy (cystic fibrosis)
Vomiting caused by obstruction of the gastrointestinal tract is
probably mediated by intestinal
visceral afferent nerves stimulating the vomiting center (see
Table 303-1 ). If obstruction
occurs below the 2nd part of the duodenum, vomitus is usually
bile stained. Emesis may also
become bile stained with repeated vomiting in the absence of
obstruction when duodenal
contents are refluxed into the stomach. Nonobstructive lesions
of the digestive tract can also
cause vomiting; this includes diseases of the upper bowel,
pancreas, liver, or biliary tree.
CNS or metabolic derangements may lead to severe, persistent
emesis.
Cyclic vomitingis a syndrome with numerous episodes of vomiting
interspersed with well
intervals. The onset is usually between 2 and 5 yr of age; the
frequency of vomiting episodes
is variable (average of 12 episodes per yr) with each episode
typically lasting 23 days, withfour or more emesis episodes per
hour. Patients may have a prodrome of pallor, intolerance
of noise or light, nausea, lethargy, and headache or fever.
Precipitants include infection,
stress, and excitement. Idiopathic cyclic vomiting may be a
migraine equivalent (abdominal
migraine),or it may result from altered intestinal motility or
mutations in mitochondrial
DNA. The differential diagnosisincludes gastrointestinal
anomalies (malrotation,
duplication cysts, choledochal cysts), CNS disorders (neoplasm,
epilepsy, vestibular
pathology), nephrolithiasis, cholelithiasis, hydronephrosis,
metabolic-endocrine disorders(urea cycle, fatty acid metabolism,
Addison disease, porphyria, hereditary angioedema,
-
8/13/2019 Nausea and Vomitting
21/24
familial Mediterranean fever), chronic appendicitis, and
inflammatory bowel disease.
Laboratory evaluationis based on a careful history and physical
examination and may
include, if indicated, endoscopy, contrast gastrointestinal
radiography, brain MRI, and
metabolic studies (lactate, organic acids, ammonia). Treatment
includes hydration and
ondansetron. Prevention may be possible with the antimigraine
agent amitriptyline or
cyproheptadine.
Potential complications of emesis are noted in Table 303-4 .
Broad management strategies for
vomiting in general and specific causes of emesis are noted in
Table 303-5 and Table 303-6 .
TABLE 303-4 -- Complications of Vomiting
COMPLICATION PATHOPHYSIOLOGY
HISTORY, PHYSICAL
EXAMINATION, AND
LABORATORY STUDIES
Metabolic Fluid loss in emesis DehydrationHCl loss in emesis
Alkalosis;hypochloremia
Na, K loss in emesis Hyponatremia;hypokalemia
Alkalosis
Na into cells
HCO3loss in urine Urine pH 78
Na and K loss in urine Urine Na , K
HypochloremiaCl conserved
by kidneys
Urine Cl
Nutritional Emesis of calories and nutrients
Malnutrition;failure to thrive
Anorexia for calories and
nutrients
Mallory-Weiss tear Retchingtear at lesser curve
of gastroesophageal junction
Forceful emesishematemesis
Esophagitis Chronic vomitingesophageal
acid exposure
Heartburn;hemoccult + stool
Aspiration Aspiration of vomitus,
especially in context ofobtundation
Pneumonia;neurologic dysfunction
Shock Severe fluid loss in emesis or in
accompanying diarrhea
Dehydration (accompanying diarrhea
can explain acidosis?)
Severe blood loss in
hematemesis
Blood volume depletion
From Kliegman RM, Greenbaum LA, Lye PS (eds): Practical
Strategies in Pediatric
Diagnosis and Therapy, 2nd ed. Philadelphia, Elsevier, 2004, p
318.
Cl, chloride; HCl, hydrogen chloride; HCO3, bicarbonate; K,
potassium; Na, sodium.
-
8/13/2019 Nausea and Vomitting
22/24
TABLE 303-5 -- Pharmacologic Therapies for Vomiting Episodes
DISEASE/CONDITION
THERAPY-DRUG CLASS: SPECIFIC AGENT/TRADE
NAME (DOSE)
Reflux Dopamine antagonist: metoclopramide (Reglan) (0.10.2
mg/kgqid PO/IV)
Peripheral dopamine antagonist: domperidone (Motilium) (0.20.6
mg/kg tidqid PO)
Gastroparesis Metoclopramide, domperidone; see above
Motilin agonist: erythromycin (24 mg/kg tidqid PO/IV)
Intestinal
pseudoobstruction
Stimulation of intestinal migratory myoelectric complexes:
Octreotide (Sandostatin) (1 g/kg bidtid SC)
Chemotherapy Metoclopramide;see above (0.51.0 mg/kg qid IV,
withantihistamine prophylaxis of extrapyramidal side effects)
Serotoninergic 5-HT3antagonist: ondansetron (Zofran) (0.150.3
mg/kg tid IV/PO)
Phenothiazines:(extrapyramidal, hematologic side effects)
Prochlorperazine (Compazine) (0.3 mg/kg bidtid PO)
Chlorpromazine (Thorazine) (>6 mo of age: 0.5 mg/kg
tidqidPO/IV)
Steroids:dexamethasone (Decadron) (0.1 mg/kg tid PO)
Cannabinoids:nabilone (tetrahydrocannabinol) (0.050.1
mg/kgbidtid PO)
Postoperative Ondansetron, phenothiazines: see above
Motion sickness; vestibular
disorders
Antihistamine:dimenhydrinate (Dramamine) (1 mg/kg tidqidPO)
Anticholinergic:scopolamine (Transderm Scp) (adults: 1patch/3
days)
Adrenal crisis Steroids:cortisol (2 mg/kg bolus IV followed by
0.20.4mg/kg/hr IV [ 1 mg/kg IM])
Cyclic vomiting syndrome(CVS)
Supportive:
Analgesic:meperidine (Demerol) (12 mg/kg q46h IV/IM)
Anxiolytic, sedative: Lorazepam (Ativan) (0.050.1 mg/kg
q6hIV)
Antihistamine, sedative: diphenhydramine (Benadryl) (1.25
mg/kg q6h IV)
Abortive:
Serotoninergic 5-HT3antagonist:
Ondansetron:see above
-
8/13/2019 Nausea and Vomitting
23/24
DISEASE/CONDITION
THERAPY-DRUG CLASS: SPECIFIC AGENT/TRADE
NAME (DOSE)
Granisetron (Kytril) (10 g/kg q46h IV)
Nonsteroidal antiinflammatory agent (GI ulceration side
effect):
Ketorolac (Toradol) (0.51.0 mg/kg q68h IV)Serotoninergic 5-HT1D
agonist: sumatriptan (Imitres) (>40 kg;
20 mg intranasally/25 mg PO, one time only)
Prophylactic:(if >1 CVS bout/month;taken daily)
Antimigraine, -adrenergic blocker: propranolol (Inderal) (0.52.0
mg/kg bid PO)
Antimigraine, antihistamine: cyproheptadine (Periactin) (0.250.5
mg/kg/day bidtid PO)
Antimigraine, tricyclic antidepressant: amitriptyline
(Elavil)
(0.330.5 mg/kg tid PO, and titrate to maximum of 3.0mg/kg/day as
needed; obtain baseline ECG at start of therapy,
and consider monitoring drug levels)
Antimigraine antiepileptic: Phenobarbital (Luminal) (23mg/kg
qhs)
Erythromycin:see above
Low estrogen oral contraceptives: consider for catamenial
CVS
episodes
From Kliegman RM, Greenbaum LA, Lye PS (eds): Practical
Strategies in Pediatric
Diagnosis and Therapy, 2nd ed. Philadelphia, Elsevier, 2004, p
317.
bid, twice daily; ECG, electrocardiogram; GI, gastrointestinal;
IM, intramuscularly; IV,
intravenously, PO, orally; q46h, every 4 to 6 hours; q6h, every
6 hours; q68h, every 6 to 8hour; qhs, each bedtime; SC,
subcutaneously; tid, three times daily; qid, four times daily.
TABLE 303-6 -- Supportive and Nonpharmacologic Therapies for
Vomiting Episodes
DISEASE THERAPY
All Treat cause: obstructionoperate; allergychange diet
(steroids);
metabolic error
Rx defect; acid peptic disease
H2RAs, PPIs, etc.Complications
Dehydration IV fluids, electrolytes
Hematemesis Transfuse, correct coagulopathy
Esophagitis 2 s, s
Malnutrition NG or NJ drip feeding useful for many chronic
conditions
Mecomium ileus Gastrografin enema
DIOS Gastrografin enema; balanced colonic lavage solution (e.g.,
GoLytely)
Intussusception Barium enema; air reduction enemaHematemesis
Endoscopic:injection sclerotherapy or banding of esophageal
varices;
-
8/13/2019 Nausea and Vomitting
24/24
DISEASE THERAPY
injection therapy, fibrin sealant application, or heater probe
electrocautery
for selected upper GI tract lesions
Sigmoid volvulus Colonoscopic decompression
Reflux Positioning;dietary measures (infants:rice cereal, 1
tbs/oz of formula)
Psychogenic
components
Psychotherapy;tricyclic antidepressants; anxiolytics (e.g.,
diazepam: 0.1
mg/kg/tidqid PO)
From Kliegman RM, Greenbaum LA, Lye PS (eds): Practical
Strategies in Pediatric
Diagnosis and Therapy, 2nd ed. Philadelphia, Elsevier, 2004, p
319.
DIOS, distal intestinal obstruction syndrome; GI,
gastrointestinal; H2RAs, histamine2-
receptor antagonists; IV, intravenous; NG, nasogastric; NJ,
nasojejunal; PO, orally; PPIs,
proton pump inhibitors; qid, four times a day; tbs, tablespoon;
tid, three times a day.