Embed Size (px)
Citation preview
1
The Daily Huddle: Getting the Front Line on Board for Quality
National Health Leadership Conference Halifax, NS
June 4, 2012
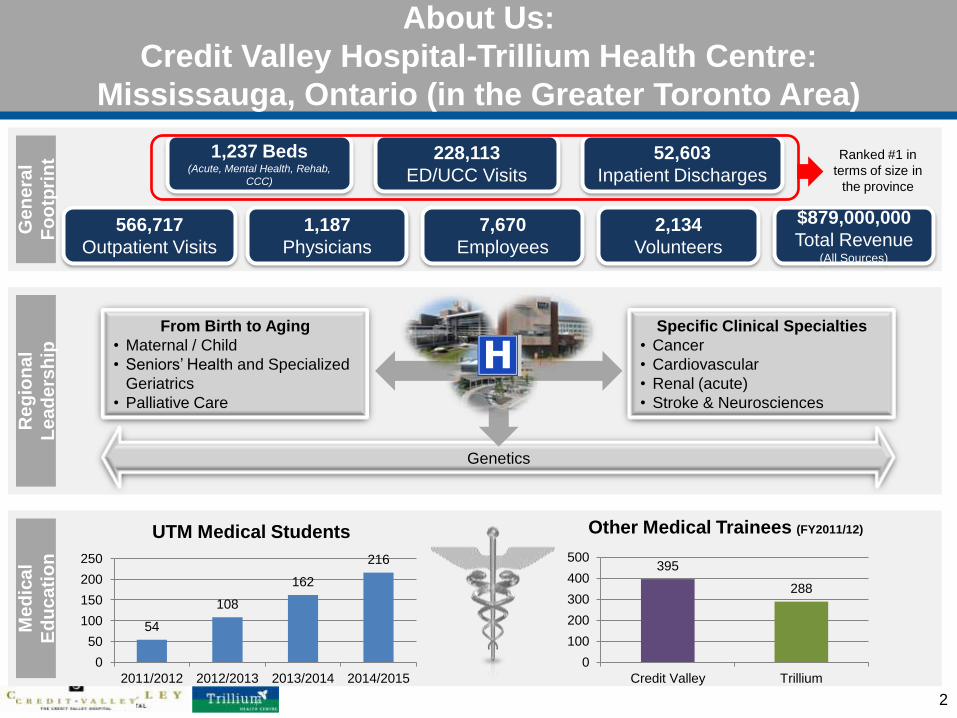
About Us:
Credit Valley Hospital-Trillium Health Centre:
Mississauga, Ontario (in the Greater Toronto Area)
2
1,237 Beds (Acute, Mental Health, Rehab,
CCC)
228,113
ED/UCC Visits
52,603
Inpatient Discharges
566,717
Outpatient Visits
1,187
Physicians
7,670
Employees
$879,000,000
Total Revenue (All Sources)
From Birth to Aging
• Maternal / Child
• Seniors’ Health and Specialized
Geriatrics
• Palliative Care
Specific Clinical Specialties
• Cancer
• Cardiovascular
• Renal (acute)
• Stroke & Neurosciences
Genetics
54
108
162
216
0
50
100
150
200
250
2011/2012 2012/2013 2013/2014 2014/2015
UTM Medical Students
395
288
0
100
200
300
400
500
Credit Valley Trillium
Other Medical Trainees (FY2011/12)
Ge
ne
ral
Fo
otp
rin
t
Re
gio
na
l
Le
ad
ers
hip
Me
dic
al
Ed
uc
ati
on
Ranked #1 in
terms of size in
the province
2,134
Volunteers
3
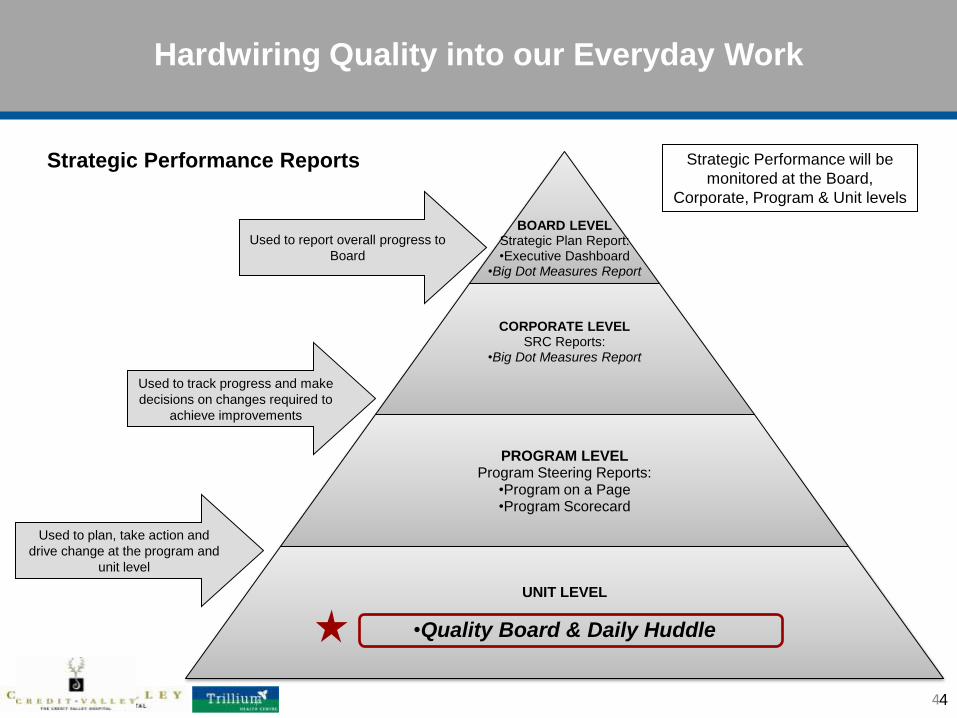
Hardwiring Quality into our Everyday Work
4 4
BOARD LEVEL Strategic Plan Report: •Executive Dashboard
•Big Dot Measures Report
CORPORATE LEVEL SRC Reports:
•Big Dot Measures Report
PROGRAM LEVEL Program Steering Reports:
•Program on a Page •Program Scorecard
UNIT LEVEL
•Quality Board & Daily Huddle
Strategic Performance Reports
Used to report overall progress to
Board
Used to track progress and make
decisions on changes required to
achieve improvements
Used to plan, take action and
drive change at the program and
unit level
Strategic Performance will be
monitored at the Board,
Corporate, Program & Unit levels
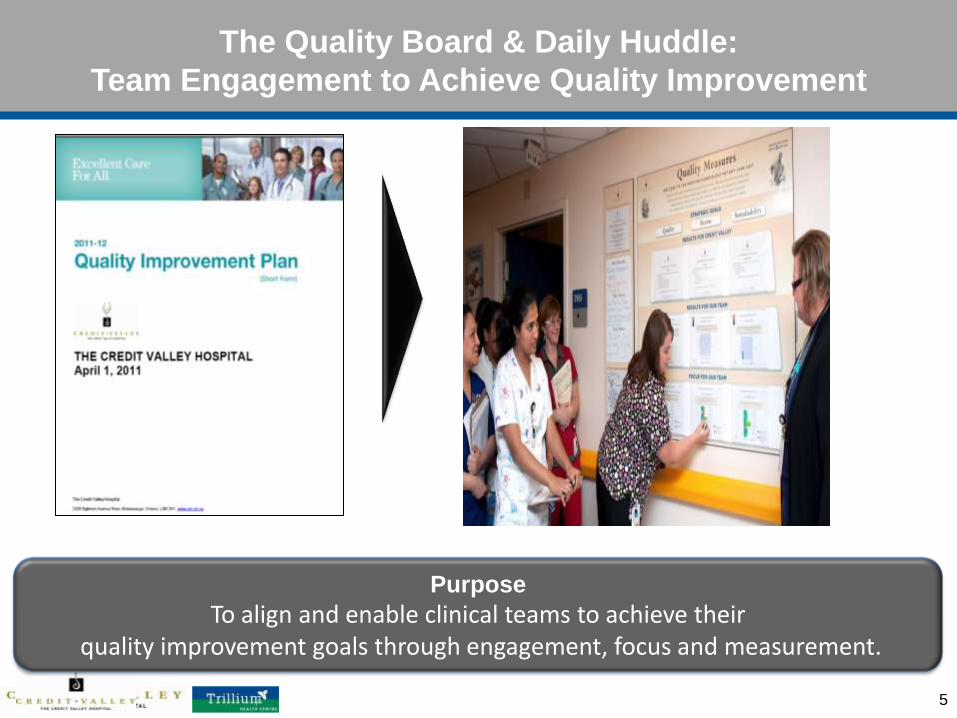
The Quality Board & Daily Huddle:
Team Engagement to Achieve Quality Improvement
5
Purpose
To align and enable clinical teams to achieve their quality improvement goals through engagement, focus and measurement.

Quality Board & Daily Huddle: A joint Strategy Management Office and
Quality, Performance and Risk Management Department Initiative
6
PROJECT TEAM
• Cheryl Hoare
Coordinator,
Strategy Management Office
• David Girard and Narinder Mundi
Analysts,
Strategy Management Office
• Barb Young
Quality, Safety and Risk Consultant,
Medicine/Cardiology
• Chris Zettler
Patient Care Manager,
Medicine/Cardiology
• Samantha D’Amico
Clinical Educator,
Medicine/Cardiology
• James Yuan
Decision Support
Consultant,
Medicine/Cardiology
• Louise Van Zeller
Communications
• Sandra Taveras
Designer
With sincere thanks to the Medicine/Cardiology (3B)
pilot project team and staff for their help designing and trialing the Quality Board &
Daily Huddle
Overview of Quality Board & Daily Huddle
• Daily measurement and monthly trending together with focused actions in
3 areas at once, help front-line staff improve
OBJECTIVE: To achieve our quality, access and sustainability performance targets
by creating a clear line of sight between our strategic goals and the work that
individuals do each day.
IMPLEMENTATION STRATEGY
• Pilot area - Medicine/Cardiology Unit:
• July-Oct. 2010: Planning and development
• Oct. 2010 – April 2011: Implementation and evaluation
• April – July 2011: 3 wave roll-out to all inpatient and out-patient clinical
areas
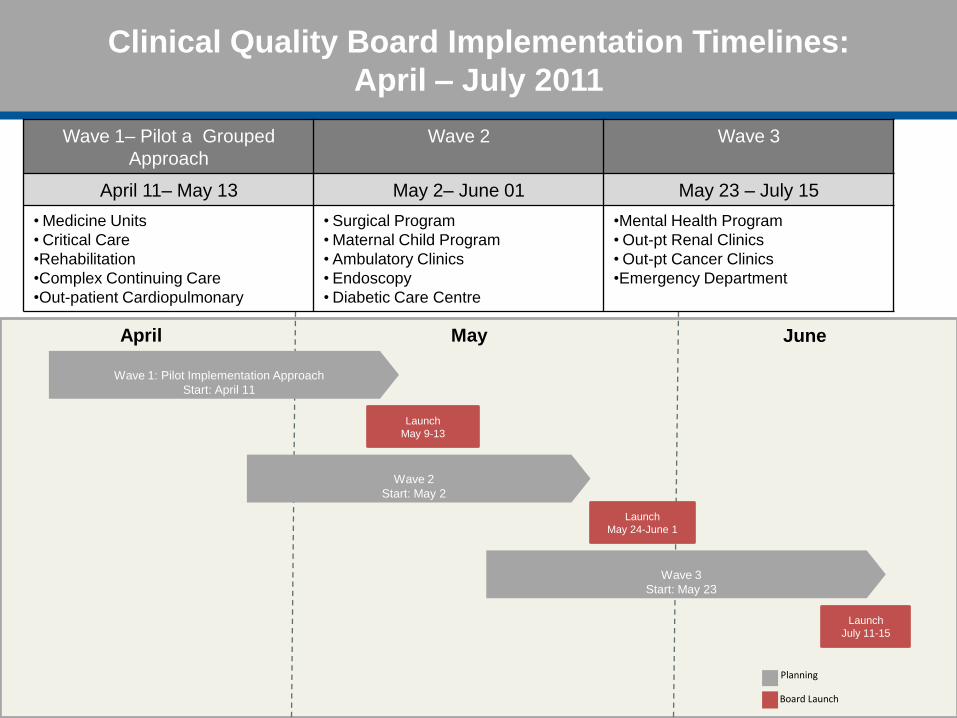
Clinical Quality Board Implementation Timelines:
April – July 2011
8
April May
Planning
Board Launch
Launch
May 9-13
Wave 1: Pilot Implementation Approach
Start: April 11
June
Wave 2
Start: May 2
Launch
May 24-June 1
Wave 3
Start: May 23
Launch
July 11-15
Wave 1– Pilot a Grouped
Approach
Wave 2 Wave 3
April 11– May 13 May 2– June 01 May 23 – July 15
• Medicine Units
• Critical Care
•Rehabilitation
•Complex Continuing Care
•Out-patient Cardiopulmonary
• Surgical Program
• Maternal Child Program
• Ambulatory Clinics
• Endoscopy
• Diabetic Care Centre
•Mental Health Program
• Out-pt Renal Clinics
• Out-pt Cancer Clinics
•Emergency Department
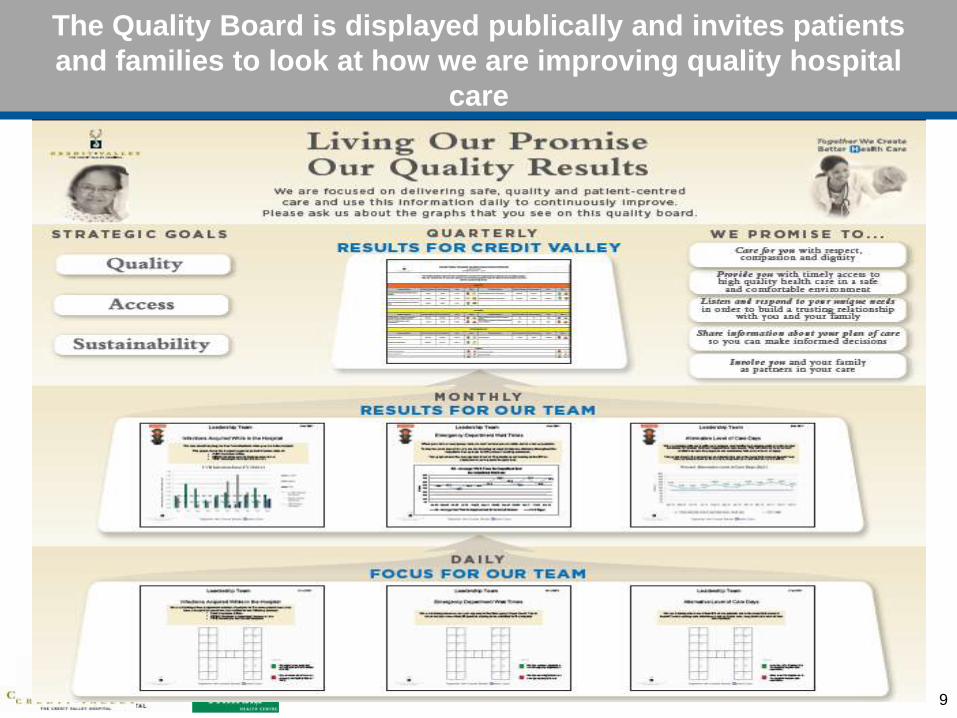
The Quality Board is displayed publically and invites patients
and families to look at how we are improving quality hospital
care
9
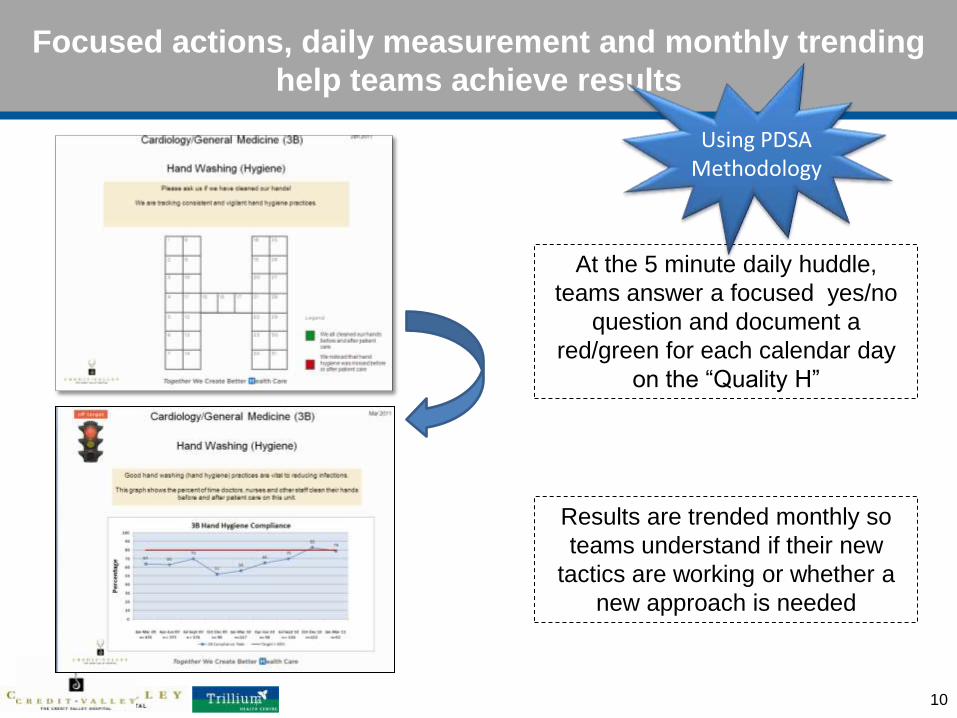
Focused actions, daily measurement and monthly trending
help teams achieve results
10
At the 5 minute daily huddle,
teams answer a focused yes/no
question and document a
red/green for each calendar day
on the “Quality H”
Results are trended monthly so
teams understand if their new
tactics are working or whether a
new approach is needed
Using PDSA Methodology
Quality Board Huddle in Action
11
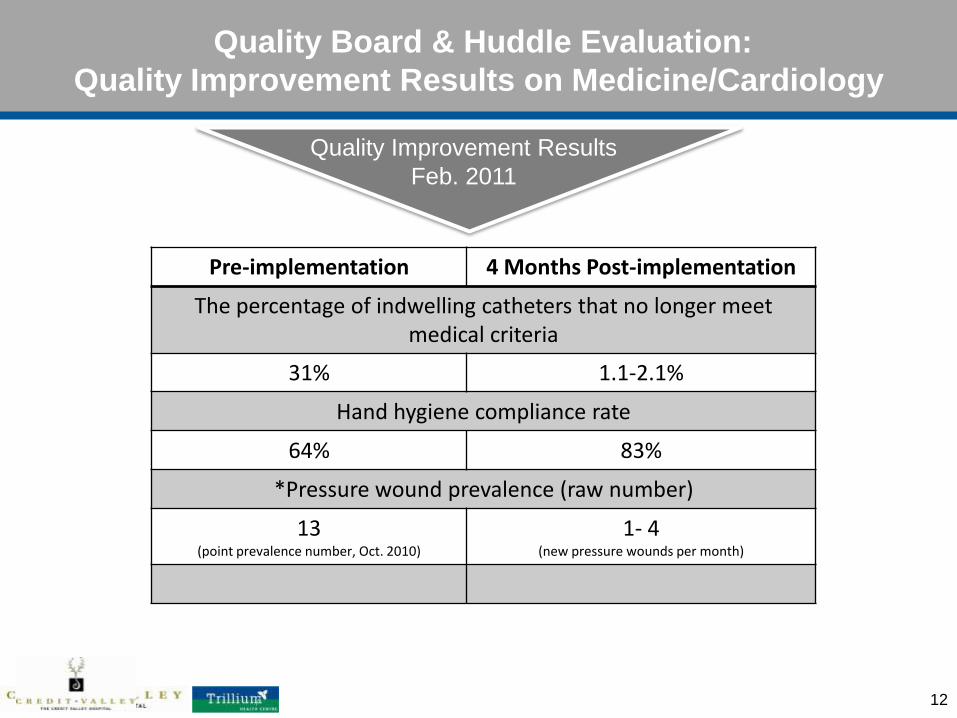
Quality Board & Huddle Evaluation:
Quality Improvement Results on Medicine/Cardiology
12
Quality Improvement Results
Feb. 2011
Pre-implementation 4 Months Post-implementation
The percentage of indwelling catheters that no longer meet medical criteria
31% 1.1-2.1%
Hand hygiene compliance rate
64% 83%
*Pressure wound prevalence (raw number)
13 (point prevalence number, Oct. 2010)
1- 4 (new pressure wounds per month)
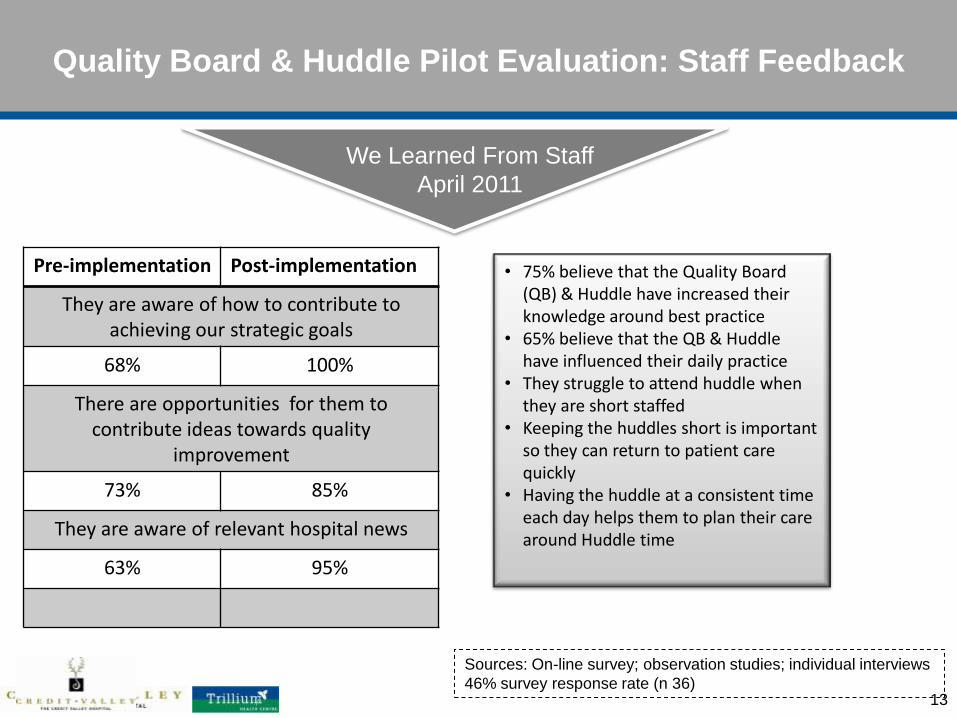
Quality Board & Huddle Pilot Evaluation: Staff Feedback
13
Pre-implementation Post-implementation
They are aware of how to contribute to achieving our strategic goals
68% 100%
There are opportunities for them to contribute ideas towards quality
improvement
73% 85%
They are aware of relevant hospital news
63% 95%
We Learned From Staff
April 2011
• 75% believe that the Quality Board (QB) & Huddle have increased their knowledge around best practice
• 65% believe that the QB & Huddle have influenced their daily practice
• They struggle to attend huddle when they are short staffed
• Keeping the huddles short is important so they can return to patient care quickly
• Having the huddle at a consistent time each day helps them to plan their care around Huddle time
Sources: On-line survey; observation studies; individual interviews
46% survey response rate (n 36)
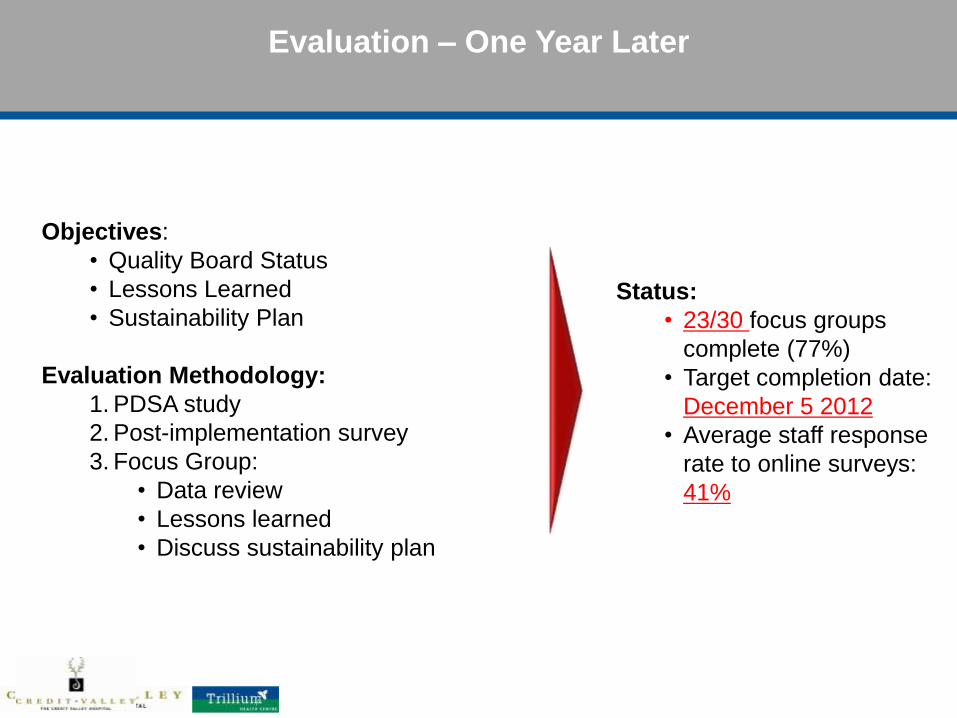
Evaluation – One Year Later
Objectives:
• Quality Board Status
• Lessons Learned
• Sustainability Plan
Evaluation Methodology:
1. PDSA study
2. Post-implementation survey
3. Focus Group:
• Data review
• Lessons learned
• Discuss sustainability plan
Status:
• 23/30 focus groups
complete (77%)
• Target completion date:
December 5 2012
• Average staff response
rate to online surveys:
41%
Preliminary Key Findings: The Benefits
What the benefits are:
• Staff collaboration and recognition
• Issue resolution (manager present)
• Information and best practices shared
Huddle
What the benefits are:
• Provide a structured way to implement change
• Create awareness and increase knowledge
• Peer accountability
• Positive feedback from patients
Indicators
Preliminary Key Findings: The Challenges
• Long huddles due to increased scope as huddles
have become a forum for sharing organizational
messages
• Lack of staff engagement/attendance both at
huddles (can be due to patient care priorities) and
in the indicator development process
• May not be meaningful for staff who already
perform well, for clinicians whose practice is not
impacted by the selected metrics or when the
selected indicators are subjective/not truly
measureable
• If the people huddling do not have actual control
over the indicator, changes to practice may not
happen
Huddle
Indicators
Preliminary Key Findings: Suggestions for Improvement
• Do not use huddle time for lengthy problem
solving; if suggestions arise, engage individuals
further after huddle time
• Further explain “Big Dots” and the purpose of
the Quality Board so the value is fully
understood
• Develop a process for changing indicators at
appropriate intervals
• Implement shared indicators between units to
improve flow
Huddle
Indicators
Next Steps
Clinical Support Services In the Planning Stage
• Diagnostic Imaging
• Laboratory
• Pharmacy
Sustainability Goals:
• Analyze quality improvement results & implement improvement tactics
(PDSA cycles)
• Implement standard process for how new indicators are selected and
implemented
• Establish program level accountability for Quality Boards
19
Cheryl Hoare, RN, BScN, MN, PNC(C)
Patient Care Manager
Mother Baby Unit, High Risk Pregnancy, Breastfeeding and Women’s Health Clinics
Credit Valley Hospital/Trillium Health Centre, Credit Valley Site
2200 Eglinton Avenue West
Mississauga, ON L5M 2N1
905-813-1100 ext. 6346
Rhonda Warrian, RN, MN, CHE
Patient Care Program Director
Surgery and Ambulatory Care
Credit Valley Hospital/Trillium Health Centre, Credit Valley Site
2200 Eglinton Avenue West
Mississauga, ON L5M 2N1
905-813-2509
Contact Information
20