Embed Size (px)
Citation preview

Nagoya J. med. Sci. 30: 59-68, 1967.
THE SIGNIFICANCE OF THE ISOLA TED POSITIVE
URINE CULTURE IN GENITOURINARY
TUBERCULOSIS
AKIO SEGAWA
Department of Urology, Nagoya University School of Medicine (Director . Prof Keizo Shimizu)
RoBERT }. REILLY AND JoHN K. LATTIMER
Department of Urology, Columbia University College of Physicians and Surgeons (Director: Prof john K. Lattimer)
ABSTRACT
In a study of 333 patients with genitourinary tuberculosis, the disease in
those who showed only a single isolated positive urine culture, as the basis for
their original diagnosis, was very easily arrested usually ( 92 per cent J only a
single course of treatment was required. On the other hand, among those whose
original diagnosis was based on a finding of multiple positive urine cultures, the
relapse rate was much higher, and the proportion who relapsed again showing
multiple positive urine cultures was much higher. Isolated positive urine cultures for tuberculosis are not always dependable
as an indication of the disease. Multiple positive urine cultures were an even
more serious indicator of susceptibility to relapse, than was the presence of large
cavitary lesions. All relapses were eventually arrested by a second, a third, or
(rarely) a fourth course of chemotherapy. There have been no failures to date.
Clinicians have long realized the hazards of establishing a diagnosis of
pulmonary tuberculosis on the basis of a single isolated positive sputum culture
or gastric washing without simultaneous clinical and laboratory evidence of
disease. Laboratory error or mislabelling of specimens might, at times, account
for an "isolated" positive. A definite clinical impression exists that patients in
whom the diagnosis of genitourinary tuberculosis is established by an isolated
positive urine culture1l have a better prognosis for the arrest of their disease
than patients having more than one positive urine culture. This study was
initiated in order to establish the significance of isolated positive urine culture
on the course and prognosis of the disease in patients with genitourinary
tuberculosis.
~IIISB7::, >n<~ r•J•7~ P ~, :?-~":/•K•77-; -:r~
Received for :publication December 22, 1966.

60 A. SEGAWA ET AL.
MATERIALS AND METHODS
Adequate follow-up was available on 333 patients with genitourinary tuberculosis who had received chemotherapy at the Combined Research Study Unit for Genitourinary Tuberculosis of Columbia University and the Kingsbridge Veterans Administration Hospital in New York City. Eighty-three of these patients were female and 250 were male. When graded according to the radio· graphic evidence2J3J of renal tuberculosis (Fig. 1), minimal lesions (no X -ray change) were noted in 143 patients, while 190 patients had advanced (cavitary) lesions. In 48 patients, renal tuberculosis was clinically unilateral. In 196 patients, the diagnosis of bilateral renal tuberculosis had been established. The remaining 89 patients had undergone previous nephrectomy and had evidence of tuberculosis in a solitary kidney.
GROUP 0 MINIMAL
No Deformity
By X.Ray
I 2 MOD. ADVANCED
One Cavity
3 4 FAR ADVANCED
2 Or More Cavities
FIG. 1. A roentgenographic classification of the lesions of the Kidney (Lattimer, J. K.).
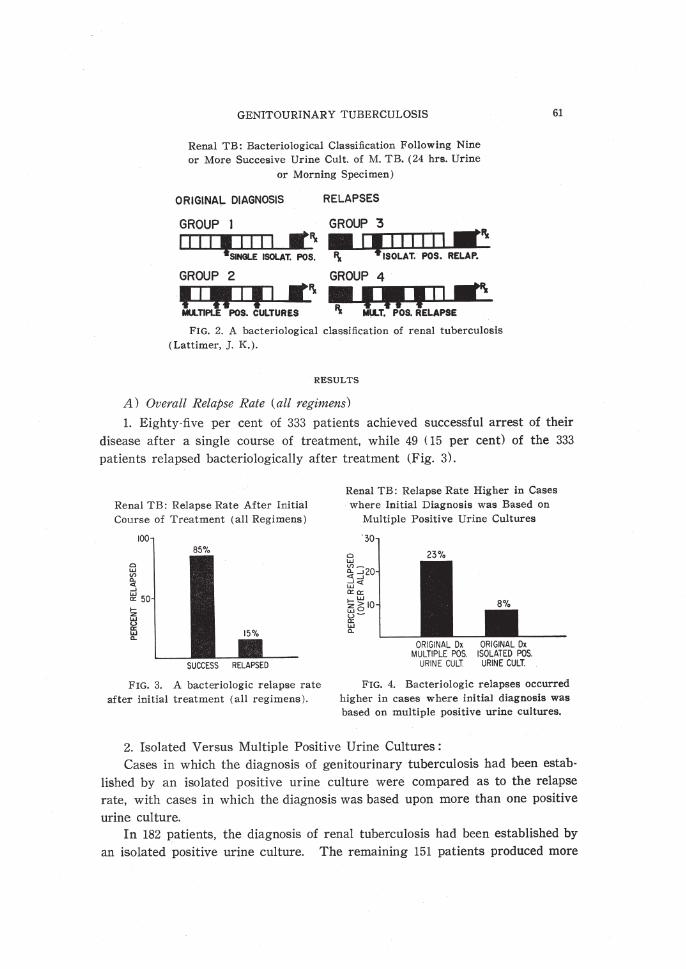
The diagnosis of genitourinary tuberculosis was established by the isolation of the pathogenic acid fast bacilli by culture and guinea pig inoculation from one or more of three, sometimes nine or more, 24-hour urine collections1J3J. The patients were divided into 4 groups for the purpose of this study (Fig. 2). The first group consisted of those patients who had a single isolated positive urine culture prior to the initiation of treatment. The second group was made up of those patients in whom the original diagnosis of genitourinary tuberculosis was established by the finding of more than one positive urine culture. The patients who relapsed after treatment were, in turn, divided into groups 3 and 4. In group 3, evidence of relapse was based on an isolated positive urine culture, while in group 4, relapse was established bacteriolbgically by more than one positive urine culture.
GENITOURINARY TUBERCULOSIS
Renal TB: Bacteriological Classification Following Nine
or More Succesive Urine Cult. of M. TB. (24 hrs. Urine
or Morning Specimen)
ORIGINAL DIAGNOSIS RELAPSES
GROUP I GROUP 3
1111,1111 ·1\~ SINGLE ISOLAT. POS. 1\ ISOLAT. POS. RELAP.
GROUP 2 GROUP 4
·fiWill-Lf\ Mtl..TIPLE POS. CULTURES
FIG. 2. A bacteriological classification of renal tuberculosis
(Lattimer, ]. K.).
RESULTS
A) Overall Relapse Rate (all regimens)
61
1. Eighty-five per cent of 333 patients achieved successful arrest of their
disease after a single course of treatment, while 49 ( 15 per cent) of the 333
patients relapsed bacteriologically after treatment (Fig. 3).
Renal TB: Relapse Rate After Initial Course of Treatment (all Regimens)
0 w <f) c..
"" ...1 w a:: ... z w
ffi c..
SUCCESS RELAPSED
Renal TB: Relapse Rate Higher in Cases where Initial Diagnosis was Based on
Multiple Positive Urine Cultures
23%
ORIGINAL Dx ORIGINAL Dx MULTIPLE POS. ISOLATED POS.
URINE CULT URINE CULT.
FIG. 3. A bacteriologic relapse rate FIG. 4. Bacteriologic relapses occurred
after initial treatment (all regimens). higher in cases where initial diagnosis was based on multiple positive urine cultures.
2. Isolated Versus Multiple Positive Urine Cultures:
Cases in which the diagnosis of genitourinary tuberculosis had been estab
lished by an isolated positive urine culture were compared as to the relapse
rate, with cases in which the diagnosis was based upon more than one positive
urine cui ture. In 182 patients, the diagnosis of renal tuberculosis had been established by
an isolated positive urine culture. The remaining 151 patients produced more
62 A. SEGAWA ET AL.
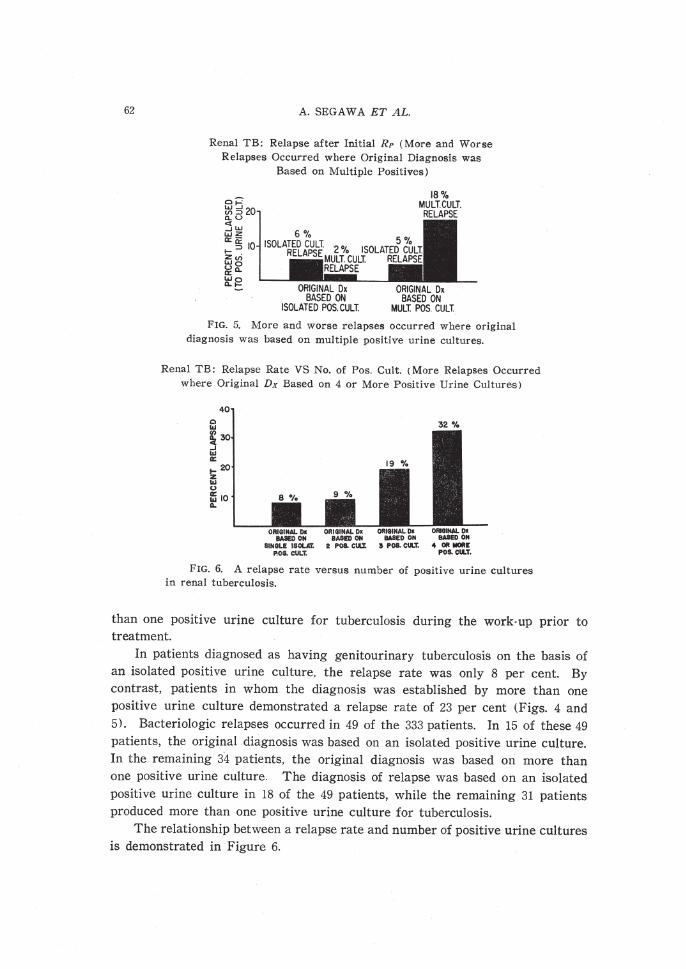
Renal TB: Relapse after Initial RP (More and Worse Relapses Occurred where Original Diagnosis was
Based on Multiple Positives)
FIG. 5. More and worse relapses occurred where original diagnosis was based on multiple positive urine cultures.
Renal TB: Relapse Rate VS No. of Pos. Cult. (More Relapses Occurred where Original Dx Based on 4 or More Positive Urine Cultures)
0 ... ~ ..J ... a:
40
1-20 z ... (,)
ffi1o a.. .
32%
FIG. 6. A relapse rate versus number of positive urine cultures in renal tuberculosis.
than one positive urine culture for tuberculosis during the work-up prior to treatment.
In patients diagnosed as having genitourinary tuberculosis on the basis of an isolated positive urine culture, the relapse rate was only 8 per cent. By contrast, patients in whom the diagnosis was established by more than one positive urine culture demonstrated a relapse rate of 23 per cent (Figs. 4 and 5). Bacteriologic relapses occurred in 49 of the 333 patients. In 15 of these 49 patients, the original diagnosis was based on an isolated positive urine culture. In the remaining 34 patients, the original diagnosis was based on more than one positive urine culture. The diagnosis of relapse was based on an isolated positive urine culture in 18 of the 49 patients, while the remaining 31 patients produced more than one positive urine culture for tuberculosis.
The relationship between a relapse rate and number of positive urine cultures is demonstrated in Figure 6.
GENITOURINARY TUBERCULOSIS 63
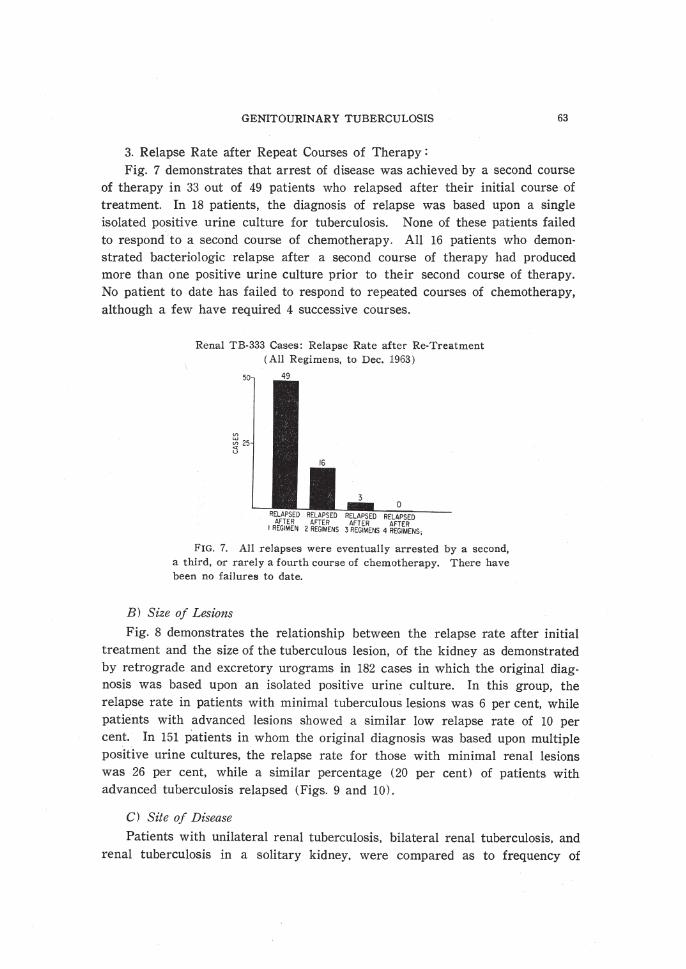
3. Relapse Rate after Repeat Courses of Therapy : Fig. 7 demonstrates that arrest of disease was achieved by a second course
of therapy in 33 out of 49 patients who relapsed after their initial course of treatment. In 18 patients, the diagnosis of relapse was based upon a single isolated positive urine culture for tuberculosis. None of these patients failed to respond to a second course of chemotherapy. All 16 patients who demonstrated bacteriologic relapse after a second course of therapy had produced more than one positive urine culture prior to their second course of therapy. No patient to date has failed to respond to repeated courses of chemotherapy, although a few have required 4 successive courses.
Renal TB-333 Cases: Relapse Ra te after Re-Treatment (All Regimens, to Dec. 1963)
0 RELAPSED
AFTER 4 REGIMENS;
F IG. 7. All relapses were eventually arrested by a second, a third , or rarely a fourth course of chemotherapy. There have been no failures to date.
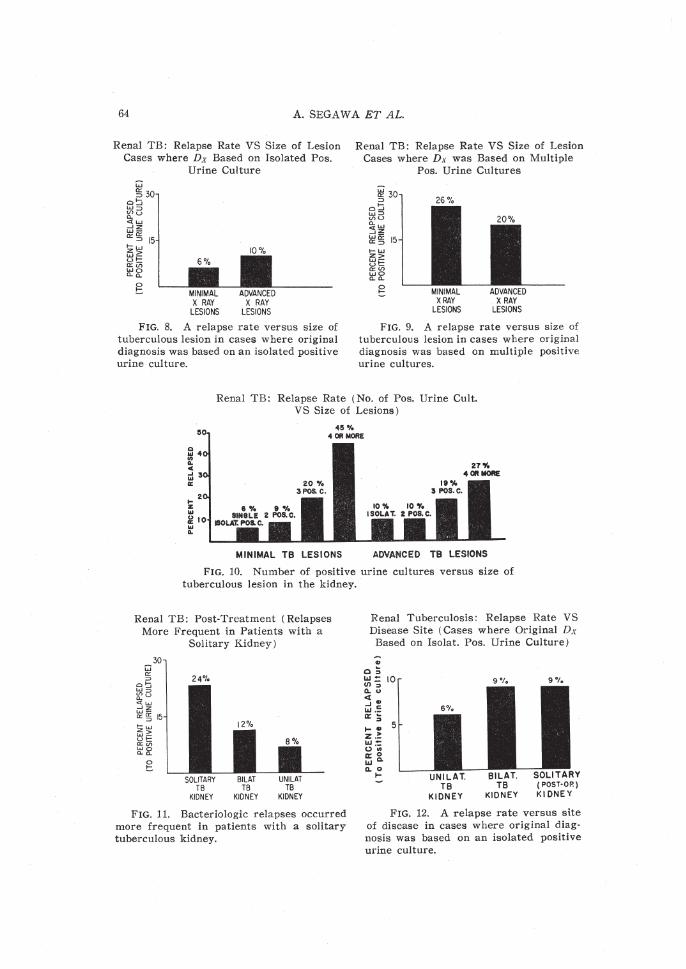
B) Size of Lesions
Fig. 8 demonstrates the relationship between the relapse rate after initial treatment and the size of the tuberculous lesion, of the kidney as demonstrated by retrograde and excretory urograms in 182 cases in which the original diagnosis was based upon an isolated positive urine culture. In this group, the relapse rate in patients with minimal tuberculous lesions was 6 per cent, while patients with advanced lesions showed a similar low relapse rate of 10 per cent. In 151 patients in whom the original diagnosis was based upon multiple positive urine cultures, the relapse rate for those with minimal renal lesions was 26 per cent, while a similar percentage (20 per cent) of patients with advanced tuberculosis relapsed (Figs. 9 and 10).
C) Site of Disease
Patients with unilateral renal tuberculosis, bilateral renal tuberculosis, and renal tuberculosis in a solitary kidney. were compared as to frequency of
64 A. SEGAWA ET AL.
Renal TB: Relapse Rate VS Size of Lesion Cases where Dx Based on Isolated Pos.
Urine Culture
MINIMAL X RAY
LESIONS
ADVANCED X RAY
LESIONS
FIG. 8. A relapse rate versus size of tuberculous lesion in cases where original diagnosis was based on an isolated positive urine culture.
Renal TB: Relapse Rate VS Size of Lesion Cases where Dx was Based on Multiple
Pos. Urine Cultures
26%
MINIMAL XRAY
LESIONS
ADVANCED X RAY
LESIONS
FIG. 9. A relapse rate versus size of tuberculous lesion in cases where original diagnosis was based on multiple positive urine cultures.
Renal TB: Relapse Rate (No. of Pos. Urine Cult. VS Size of Lesions)
MINIMAL TB LESIONS ADVANCED TB LESIONS
FIG. 10. Number of positive urine cultures versus size of tuberculous lesion in the kidney.
Renal TB: Post-Treatment (Relapses More Frequent in Patients with a
Solitary Kidney)
24'/o
SOLITARY TB
KIDNEY
BILAT TB
KIDNEY
UNILAT TB
KIDNEY
FIG. 11. Bacteriologic relapses occurred more frequent in patients with a solitary tuberculous kidney.
Renal Tuberculosis: Relapse Rate VS Disease Site (Cases where Original Dx
Based on Isolat. Pos. Urine Culture)
.. 0~ *~ 10 o..u
:3~ UJ.-a: ~ ...... z.:: l&J;t= o .. ~g_ 0..0 .... UNILAT.
TB KIDNEY
9%
BILAT . TB
KIDNEY
9%
FIG. 12. A relapse rate versus site of disease in cases where original diag· nosis was based on an isolated positive urine culture.
GENITOURINARY TUBERCULOSIS
Renal Tuberculosis: Relapse Rate VS Disease Site (Case Where Original Dx Based on Mult. Pos. Urine Culture)
40
0 ~ "' ~ ~ ~ 30 .. u ..J ..
"' c 0::: ·::: ~ 20
1- .. z > UJ:;:: 0 ·;;
ffi g_ 10 Q.
0
!:
UNILAT. BILAT. SOLITARY T 8 TB (POST·OP)
KIDNEY KIDNEY KIDNEY
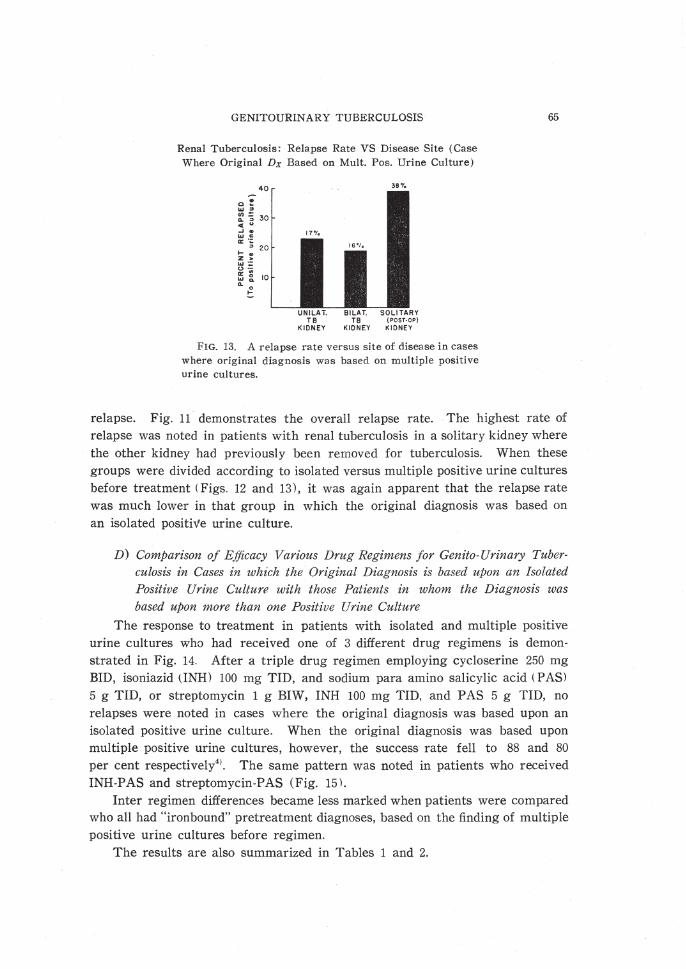
FIG. 13. A relapse rate versus site of disease in cases where original diagnosis was based on multiple positive urine cultures.
65
relapse. Fig. 11 demonstrates the overall relapse rate. The highest rate of relapse was noted in patients with renal tuberculosis in a solitary kidney where the other kidney had previously been removed for tuberculosis. When these groups were divided according to isolated versus multiple positive urine cultures before treatment (Figs. 12 and 13), it was again apparent that the relapse rate was much lower in that group in which the original diagnosis was based on an isolated positive urine culture.
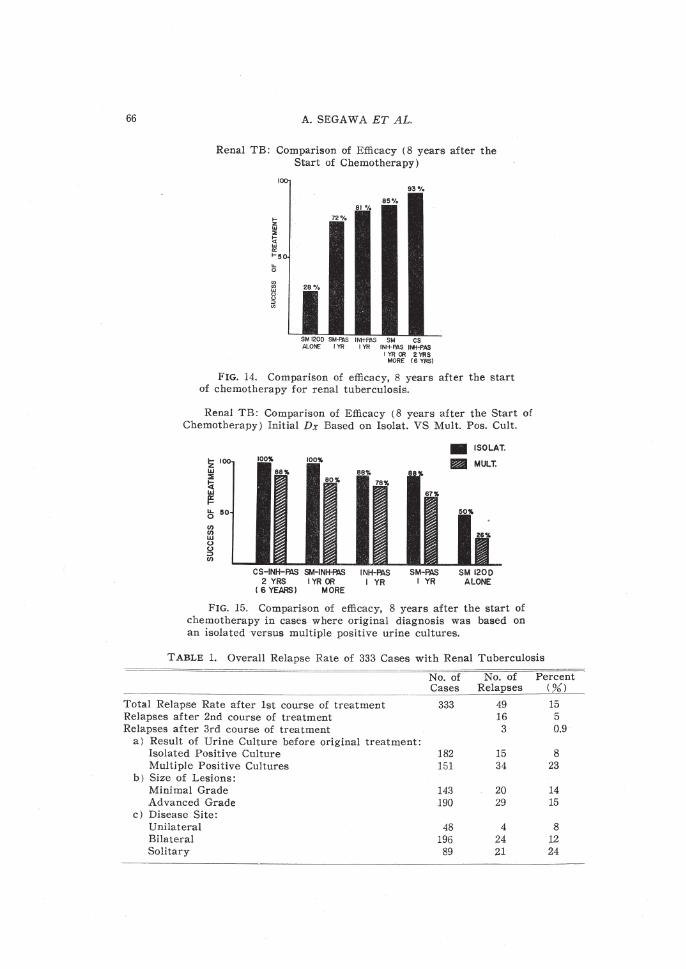
D) Comparison of Efficacy Various Drug Regimens for Genito-Urinary Tuberculosis in Cases in which the Original Diagnosis is based upon an Isolated Positive Urine Culture with those Patients in whom the Diagnosis was based upon more than one Positive Urine Culture
The response to treatment in patients with isolated and multiple positive urine cultures who had received one of 3 different drug regimens is demonstrated in Fig. 14. After a triple drug regimen employing cycloserine 250 mg BID, isoniazid (INH) 100 mg TID, and sodium para amino salicylic acid (PASl 5 g TID, or streptomycin 1 g BIW, INH 100 mg TID, and PAS 5 g TID, no relapses were noted in cases where the original diagnosis was based upon an isolated positive urine culture. When the original diagnosis was based upon multiple positive urine cultures, however, the success rate fell to 88 and 80 per cent respectively41 • The same pattern was noted in patients who received INH-PAS and streptomycin-PAS (Fig. 15\.
Inter regimen differences became less marked when patients were compared who all had "ironbound" pretreatment diagnoses, based on the finding of multiple positive urine cultures before regimen.
The results are also summarized in Tables 1 and 2.
66 A. SEGA W A ET AL.
Renal TB: Comparison of Efficacy ( 8 years after the Start of Chemotherapy)
cs INH-PAS INH-PAS
! YR 00 2 YRS MORE (6 YRSl
FIG. 14. Comparison of efficacy, 8 years after the start of chemotherapy for renal tuberculosis.
Renal TB: Comparison of Efficacy ( 8 years after the Start of Chemotherapy) Initial Dx Based on Isolat. VS Mult. Pos. Cult .
CS-INH-~ SM-IN~ INH-A:IS 2 YRS I YR OR I YR
I 6 YEARS) MORE
SM-PAS I YR
• ISOLAT.
l!llm MULT.
SM 1200 ALONE
FIG. 15. Comparison of efficacy, 8 years after the start of chemotherapy in cases where original diagnosis was based on an isolated versus multiple positive urine cultures.
TABLE 1. Overall Relapse Rate of 333 Cases with Renal Tuberculosis
No. of No. of Percent Cases Rela_pses ___ ( %) _
·· -- -- -·""_, ____
Total Relapse Rate after 1st course of treatment 333 49 15 Relapses after 2nd course of treatment 16 5 Relapses after 3rd course of treatment 3 0.9
a) Result of Urine Culture before original treatment: Isolated Positive Culture 182 15 8 Multiple Positive Cultures 151 34 23
b) Size of Lesions: Minimal Grade 143 20 14 Advanced Grade 190 29 15
c) Disease Site: Unilateral 48 4 8 Bilateral 196 24 12 Solitary 89 21 24
GENITOUR!NARY TUBERCULOSIS
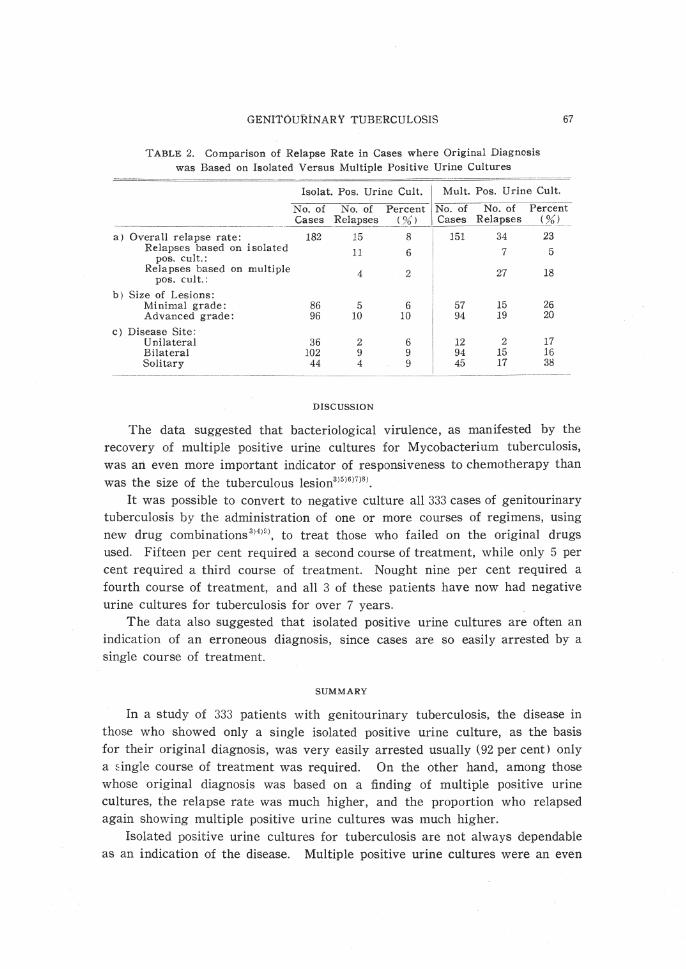
TABLE 2. Comparison of Relapse Rate in Cases where Original Diagnosis was Based on Isolated Versus Multiple Positive Urine Cultures
67
N:~o~:t. ~:: ~rm;e~:~:·t.l N~u~:· P:~. ~:inep~. : .. c.l: .. ~t.-. Cases R~laps~~ _( %L ___ Cas~5! Re~pses_(~) _
a) Overall relapse rate: Relapses based on isolated
pos. cult.: Relapses based on multiple
pos. cult.:
b) Size of Lesions: Minimal grade: Advanced grade:
c) Disease Site: Unilateral Bilateral Solitary
182 15 8 151 34 23
11 6 7 5
4 2 27 18
86 5 6 57 15 26 96 10 10 94 19 20
36 2 6 102 9 9 44 4 9
DISCUSSION
The data suggested that bacteriological virulence, as manifested by the recovery of multiple positive urine cultures for Mycobacterium tuberculosis, was an even more important indicator of responsiveness to chemotherapy than was the size of the tuberculous lesion3 )5 )6)7)8 ).
It was possible to convert to negative culture all 333 cases of genitourinary tuberculosis by the administration of one or more courses of regimens, using new drug combinations 3H)'), to treat those who failed on the original drugs used. Fifteen per cent required a second course of treatment, while only 5 per cent required a third course of treatment. Nought nine per cent required a fourth course of treatment, and all 3 of these patients have now had negative urine cultures for tuberculosis for over 7 years.
The data also suggested that isolated positive urine cultures are often an indication of an erroneous diagnosis, since cases are so easily arrested by a single course of treatment.
SUMMARY
In a study of 333 patients with genitourinary tuberculosis, the disease in those who showed only a single isolated positive urine culture, as the basis for their original diagnosis, was very easily arrested usually (92 per cent) only a !:ingle course of treatment was required. On the other hand, among those whose original diagnosis was based on a finding of multiple positive urine cultures, the relapse rate was much higher, and the proportion who relapsed again showing multiple positive urine cultures was much higher.
Isolated positive urine cultures for tuberculosis are not always dependable as an indication of the disease. Multiple positive urine cultures were an even
68 A. SEGAWA ET AL.
more serious indicator of susceptibility to relapse, than was the presence of large cavitary lesions. All relapses were eventually arrested by a second, a third, or (rarely) a fourth course of chemotherapy. There have been no failures to date
REFERENCES
1) Lattimer, ]. K., Common errors in the diagnosis and management of genitourinary tuberculosis, Med. Clin. North Amer., 43, 1623, 1959.
2) Lattimer, J. K .. A roentgenographic classification of the lesions of the kidney, Amer. Rev. Tuberc., 67, 604, 1953.
3) Lattimer, ]. K., Modern treatment of renal tuberculosis. Seminar Report, 4, 2, 1959. (Merck Sharp and Doh me ) .
4) Lattimer, ]. K., Reilly, R. ]., Segawa, A ., Wechseler, H., Siegel, J., Girgis, A . and Gieason, D., Injections are no longer necessary in treatment of renal tuberculosis, ]. Urol., 93, 735, 1965.
5) Halkier, E. and Meyer, J., Treatment of tuberculosis of the kidney, Urol. Int., 3, 96, 1956.
6) Ljunggren, E., Indications for nephrectomy, nephroureterectomy and partial nephrectomy in renal tuberculosis, ]. Urol., 78, 499, 1957.
7) T empel, F., Present status of specific drug treatment of tuberculosis. ].A.MA., 150, 1165, 1952.
8) Ljunggren, E., Specific inflamations (Urogenital tuberculosis) . Encyclopedia of Urol., lX/2, p 72 and pp 154- 155, Spring-Verlag, Berlin, Gottingen, Heidelberg, Germay, 1959.
9) Lattimer, ]. K., Vasquez. G. and Wechseler, H., New drugs for the treatment of genitourinary tuberculosis; a comparison of efficacy, J Urol., 83, 493, 1960.



![Nagoya ]. med. Sci. 30: 365-372, 1967. …...PULMONARY AIR EMBOLISM 371 the pulmonary artery, arrhythmia appeared in each case. Therefore, it was considered that the pulmonary air](https://img.pdfslide.us/doc/110x75/5f024c037e708231d40390f2/nagoya-med-sci-30-365-372-1967-pulmonary-air-embolism-371-the-pulmonary.jpg)




![Nagoya STUDIES ON BLOOD VISCOSITY DURING ......Nagoya ]. med. Sci. 31: 25-50, 1967. STUDIES ON BLOOD VISCOSITY DURING EXTRACORPOREAL CIRCULATION HrsASHI NAGASHIMA 1st Department of](https://img.pdfslide.us/doc/110x75/5f78d449f10fab1fd17dc2fe/nagoya-studies-on-blood-viscosity-during-nagoya-med-sci-31-25-50.jpg)