-
8/7/2019 my lecture scoliosis
1/32
SPINAL DEFORMITIES
BY ,
NEHA GAGGAR (MPT)
-
8/7/2019 my lecture scoliosis
2/32
SPINAL DEFORMITY
DEFINTION :
any abnormality of the formation , alignment , or shape of
the
vertebral column .
TYPES :
1. Frontal plane
scoliosis2. Sagital plane
forward head
kyphosis
exaggerated lordosis
flat back
However SCOLIOSIS have multiplanar component : frontal
sagital
torsional
-
8/7/2019 my lecture scoliosis
3/32
SCOLIOSIS
DEFINITION :
Appreciable lateral deviation (>10 degrees) in the normally
straight
vertical line of spine.
ETIOLOGY :
Genetic
Disorders of bone , muscle, disc
Developmental growth abnormalities
Central nervous system causes
-
8/7/2019 my lecture scoliosis
4/32
CLASSIFICATION
SCOLIOSIS
C
STRUCTURAL NONSTRUCTURAL
A.Idiopathic A.Postural
Infantile(0-3yrs) B.Compensatory
juvenile (4-9yrs) C.Sciatic Adolescent (10-20 yrs)
B.Congenital
C.Neuromuscular
-
8/7/2019 my lecture scoliosis
5/32
GRADES OF SCOLIOSIS
Grade I mild postural scoliosis
Grade II structural scoliosis with curve < 40 degrees
Grade III structural scoliosis with curve > 40 degrees
-
8/7/2019 my lecture scoliosis
6/32
CURVE PATTERNS
1.Cervical curve : apex between C1 C6
2.Cervicothoracic curve : apex is at C7, T1
3.Single major thoracic curve : Apex is between T2 T11
4.Single major high thoracic curve : Apex from T3 with the
curve
extending from C7 or T1 to T4 or T55.Single major lumbar curve:
Apex between L1-L2 and L4
6.Single major thoracolumbar curve : Apex is at T12 or L1
7.Combined thoracic & lumbar curves (double major curves)
:
Symmetrical double major curves
8.Double major thoracic curve :Upper thoracic from T1 to T5 or
T6 and convex to the left
-
8/7/2019 my lecture scoliosis
7/32
-
8/7/2019 my lecture scoliosis
8/32
SCOLIOTIC CURVES
1. Compensatory curve due to primary curve
2. Compensatory curve due to deformities in
other parts of the body3. Rotational element
-
8/7/2019 my lecture scoliosis
9/32
EVALUATION
I. INSPECTION
A.OBSERVATION
1.level of ear & contour of neck
2. shoulder level
3. scapular level
4. position of the arms and the waist line
5. back
6. thorax
concave : ribs crowded & flattened
convex : ribs apart & buldge backwards
7. hips & PSIS8. pelvis : concave : forward rotation
9.knee
10.feet
-
8/7/2019 my lecture scoliosis
10/32
-
8/7/2019 my lecture scoliosis
11/32
-
8/7/2019 my lecture scoliosis
12/32
EVALUATION CNTD...
B. ADAMS TEST
II. EXAMINATION
1. Range of motion
2.scoliometer
-
8/7/2019 my lecture scoliosis
13/32
EVALUATION CNTD...
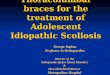
3.Cobb angle measurement
: The Cobb method is used to measure the degree of scoliosison
the posteroanterior radiograph .
STEP 1 : the apical vertebra is first identified; this is
the most likely displaced and rotated vertebra with
the least tilted end plate.
STEP 2 : The end/transitional vertebra are then
identified through the curve above and below.
The end vertebra are the most superior and inferior
vertebra which are least displaced and rotated and
have the maximally tilted end plate.
STEP 3 : A line is drawn along the superior end plate
of the superior end vertebra and a second line drawn
along the inferior end plate of the inferior end vertebra.
The angle between these two lines (or lines drawn
perpendicular to them) is measured as the Cobb angle.
-
8/7/2019 my lecture scoliosis
14/32
EVALUATION CNTD...
4. To check vertebral rotation :
Nash and moe method,
Look at the pedicles
If they are equidistant from the sides of the vertebral bodies
,
no vertebral rotation (0 rotation)
Grade 4 is in which the pedicle is past the center of
thevertebral body.
5. Skin marker
-
8/7/2019 my lecture scoliosis
15/32
EVALUATION CNTD...
6.Rib Mehtas angle
(Difference at the apical rib) is of prognostic value.
The RVA difference (RVAD) is the difference between the values
of the RVAs on the
concave and convex sides of the curve [apical vertebra].
If the convex apical rib head does not overlap the apical
vertebral body, a curve with an
initial RVAD of 20 or more is considered progressive.One line
perpendicular to the apical vertebral endplate and another from the
mid neck to
the mid head of the corresponding rib.
7.MRI8.CT Myelography
-
8/7/2019 my lecture scoliosis
16/32
MANAGEMENT
OBSERVATION
SURGERY
BRACING
-
8/7/2019 my lecture scoliosis
17/32
PREVENTIVE ROLE
early detection
screening programme for all school children of
age between 10-14 yrs
education of parents and teaching them simple
observational technique
-
8/7/2019 my lecture scoliosis
18/32
BASIC PRINCIPLES OF CORRECTION
1. ACTIVE CORRECTION :
self corrective postural activities
2. PASSIVE CORRECTION :Unequal hanging
Axial traction given by 2 therapists
3. MAINTENANCE OF CORRECTION :
Education of patient
Spinal bracing
-
8/7/2019 my lecture scoliosis
19/32
MANAGEMENT FOR GRADE I
Re-education of bad posture
monitoring after every 6 months
regimen includes:
general body relaxation
re-education of correct posture
passive correction
repeated session of maintenance of corrected posture
general free mobility exercises
strengthening spinal extensors, abdominals
deep breathing ex
balance ex stretching of concave side
avoiding activities prone to produce the deformity
-
8/7/2019 my lecture scoliosis
20/32
MANAGEMENT FOR GRADE II
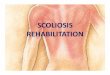
MILWAUKEE BRACE
Aka Cervicothoraciclumbosacral orthotic (CTLSO brace)
Adjustable ht, can grow with the patientWorn 23 hrs/day
Contains pelvic attachment, thoracic pads,
and chin support
Primary goal = stop progression of
scoliosis
Very effective if treatment plan is followed
-
8/7/2019 my lecture scoliosis
21/32
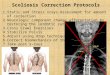
BOSTON BRACE
Aka Low Profile Thoracolumbarsacral orthotic (TLSO)
Primarily used for lower thoracic,
thoracolumbar , & lumbar curves
Still widely used, due to better
patient acceptance than Milwaukee
Brace
-
8/7/2019 my lecture scoliosis
22/32
-
8/7/2019 my lecture scoliosis
23/32
EXERCISE THERAPY
Goals = Improve ROMEspecially in direction of convexity
Reduce contractural change of soft tissues on
concave side
Done through:Improve strength, endurance, & postural
control of muscles on convex side
Identify & correct vestibular and/or
proprioceptive imbalance/deficiency
Improve balance & coordinationNormalize weight bearing in
lower
extremities & spine
-
8/7/2019 my lecture scoliosis
24/32
Specific Exercises:
Stretch concave side = balance ball, hanging from
bar, leaning against wall
Strengthen convex side = active exercise
Strengthen trunk muscles
Rotary torso exercises to left (right thoracic curve)
Proprioceptive training
Heel lift (up to 5 mm) goal is to balance weight
bearing for CNS re-education, re-evaluate every 6
weeks
-
8/7/2019 my lecture scoliosis
25/32
Exercises to restore cervical lordosis
Work with Exercise Ball proprioceptive control
Sleep posture lying on side with pillow under
ribs
To correct pelvic unleveling (ex. elevated Rt.
Ilium)
Strengthen: Lt. QL, Lt. hip adductors, Rt. G
Med
Stretch: Rt. QL, Rt. hip adductors, Lt. G Med
Breathing exercises maximize & normalize
chest expansion
-
8/7/2019 my lecture scoliosis
26/32
MANAGEMENT FOR GRADE III
Surgery is the treatment of choice
TRACTION
NONSKELETAL SKELETAL
1.Combination of
intermittent and
continuous
2. Superimposition of
both
3. Traction of
gravitational
1.Halopelvic
2. halofemoral
-
8/7/2019 my lecture scoliosis
27/32
INDICATIONS FOR SURGERY
1. Cord compression
2. Rapid progressive curve
3. Severe pain
4. Respiratory impairment
5. Cosmetic
-
8/7/2019 my lecture scoliosis
28/32
AIMS OF SURGERY
1. Restore the symmetry of trunk as much as possible
2. Straighten the thoracic curve to stop decrease in
pulmonary function
-
8/7/2019 my lecture scoliosis
29/32
PRINCIPLES OF SURGERY
I . CORRECTION OF CURVE :
1. turnbuckle cast techniques
2. distraction technique
3. lessening of the curve
II. MAINTENANCE OF CORRECTION ACHIEVED1. spinal fusion
2. spinal instrumentation
harringtons instrumentation
segmental spinal instrumentation
Dwyers instrumentation
Zieko instrumentation
-
8/7/2019 my lecture scoliosis
30/32
PREOPERATIVE PHYSIOTHERAPY
measurements
assessment of pulmonary function
muscle charting
detailed neurological examination gait analysis and functional
status
postural guidance
spinal stretching and mobility
-
8/7/2019 my lecture scoliosis
31/32
POSTOPERATIVE PHYSIOTHERAPY
FIRST 2 DAYS
Respiratory status
Ankle toe movements
upper extremity mobility
Passive movts to lower limb
turning every 2 hrly
3 RD & 4 TH DAY
Active movts for lower limb
measurement of curve
AFTER 5 DAYS
Guidance in rolling , sitting , standing
sitting
chair sitting
standing and walking
-
8/7/2019 my lecture scoliosis
32/32