Embed Size (px)
DESCRIPTION
details about scoliosis
Citation preview

Adolescent Idiopathic Scoliosis
January 21, 2011
Meghan N Imrie, MD
Pediatric Orthopaedic Surgery
Lucile Packard Children’s Hospital

Disclosures
none

Introduction
Definition Etiology Prevalence/Natural History Screening/Evaluation Treatment
– Non-operative– Operative
On the Horizon…

Definition Scoliosis
– Derived from Greek for “crooked”
– Coronal plane deformity > 10o
• < 10o = spinal asymmetry• Measured by the Cobb method
– 3-dimensional deformity– Clinical sign, not an outright
diagnosis• Four main categories
– Congenital– Degenerative– Neuromuscular/syndromic– Idiopathic

Definition - continued “idiopathic”
– What must be ruled out?• Neurofibromatosis• Marfan syndrome• Ehlers Danlos syndrome• Intraspinal abnormalities
– Tumors– Tethered cord– Syrinx
Varies by age:– Infantile - birth to age 2 years– Juvenile - from about 2 to 8 or 9 years– Adolescent - greater than 9 or 10 years, but not an adult

Overview
Definition Etiology Prevalence/Natural History Screening/Evaluation Treatment
– Non-operative– Operative
On the Horizon…

Etiology
Numerous theories, none proven Answer is there…
– Male: female ratio1
• 1:1 for minor curves• 1:8 for treatable curves
– Family history• 27% prevalence of scoliotic curves >15 degrees in
daughters of scoliotic mothers2
– Curve type• Majority right thoracic (about 98%)
– Left thoracic is red flag for possible intraspinal abnormality1. Bunnell WP Spine 1986;11:773-6.
2. Harrington PR Clin Orthop 1977;126:17-25.

Etiology
?

Overview
Definition Etiology Prevalence/Natural History Screening/Evaluation Treatment
– Non-operative– Operative
On the Horizon…

Prevalence
Varies significantly based on degree of curvature:– >10o = 0.5-3%– >30o = 1.5-3/1000
Male to female ratio:– 1:1 for minor curves– 1:8 for those
requiring treatment1
1. Bunnell WP Spine 1986;11:773-6.

Natural History
Progression– Before skeletal
maturity– After skeletal
maturity

Natural History
Progression before skeletal maturity– Many unknowns– Some knowns
• Growth remaining• Size of curve• female
From Lonstein JE and Carlson JM JBJS Am 1984;66:1061-71.

Natural History
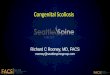
Risser sign– Radiographic
measurement based on ossification of iliac apophysis

Natural History
Clues to skeletal maturity and peak height velocity (PHV)– Radiographic measures
• Risser sign • Triradiate cartilage (TRC)• (Elbow ossification)
– Menarche in girls– Tanner staging

Natural History
From Lonstein JE and Carlson JM JBJS Am 1984;66:1061-71.

Natural History Progression after skeletal
maturity– Some variability– Weinstein and Ponseti data
most frequently used1
• Curves <30o do not progress
• Thoracic curves >500 progress average 10 per year
– 50o at 18 -> 90o curve at 58
• Lumbar curves >30o progress about 0.5o per year
1. Weinstein SL and Ponseti IV JBJS Am 1983;65:447-55.

Natural History Adults with untreated AIS:
– No increased rate of mortality (all comers with AIS)1
– Respiratory failure if curve >110 degrees2
• Increased risk of shortness of breath, especially if thoracic curve >80 degrees3
– Chronic back pain4
• Common• Not related to size or location of curve• Usually does not interfere with ability to work
1. Pehrsson K et al Spine 1992;17:1091-6.
2. Pehrsson K et al Thorax 1991;46:474.
3. Weinstein SL et al JAMA 2003;289:559-567.
4. From Tachdjian’s Pediatric Orthopaedics 269.

Natural History
Back pain in adults with untreated AIS:
Weinstein SL et al JAMA 2003;289:559-567.

Natural History Adults with untreated AIS:
– Demographics similar to control group• Education level
• Marriage
• Children– Lower C section rate
– Rate of depression similar– Body satisfaction
• AIS slightly dissatisfied to slightly satisfied
• Control slightly satisfied to satisfied
– Perception of limitation due to scoliosis• 32% reported such issues as difficulty in
purchasing clothes, decreased physical capacity, and self-consciousness
Weinstein SL et al JAMA 2003;289:559-567.

Natural History
In summary:– Trying to prevent curves from
reaching at skeletal maturity:• >50 degree thoracic• >40 or 45 degree lumbar
– Because these curves continue to progress in adulthood
– Adults with untreated, more mild scoliosis do well in adulthood (at least in Iowa…)

Overview
Definition Etiology Prevalence/Natural History Screening/Evaluation Treatment
– Non-operative– Operative
On the Horizon…

Screening Somewhat controversial
– AAOS, SRS, POSNA and AAP currently recommend1:
• Females screened twice at ages 10 and 12
• Males screened once, at age 13 or 14
– British Orthopaedic Association and British Scoliosis Society advise against screening
– United States Preventive Services Task Force (USPSTF) in 2004 recommended against screening
• AAOS, SRS, POSNA, AAP responded with 2008 information statement1
1. Richards BS and Vitale MG JBJS Am 2008;90:195-8.

Screening - controversy In summary:
– Screening is fairly reliable to detect curves (though not terribly accurate)
– Early detection could result in improved health outcomes (by potentially avoiding surgery)
– Brace therapy is likely effective in altering natural history for many patients (but not all)
Most organizations continue to recommend screening

Evaluation History
– Reason for presentation (in patient or parent’s own words
– Pain• Red flag warnings: positive finger test, night pain, non-activity
related pain
– Age– Family history– Pubertal status– Rate of progression– Any neurologic complaints
• Radicular symptoms• Bowl/bladder incontinence

Evaluation Back pain and AIS
– 23% have pain at presentation1
• Only 9% of these had underlying pathological condition
– 9% have pain during course of observation1
– Significant association if1:• > 15 years• Risser 2 or more• Post-menarchal status• History of injury
– Painful left thoracic curve or abnormal neuro exam more likely to have neuro-axis problem
1. Ramirez et al JBJS Am 1997;79:364-8.

Evaluation - radiographs
Cobb Angle - inter/intra observer error 5o

Evaluation Indications for MRI
– Atypical, specific pain– Neuro abnormality
• Abnormal reflexes• Ataxia• weakness• Progressive foot deformity
(cavus feet)
– Left thoracic curve– Rapidly progressive curve– ?males
• Routinely recommended, but minimal data to support1
1. Nakahara D et al Spine 2010 (epub ahead of print)

Evaluation
Classification systems– King-Moe– Lenke

Evaluation
Classification systems– King-Moe– Lenke

Overview
Definition Etiology Prevalence/Natural History Screening/Evaluation Treatment
– Non-operative– Operative
On the Horizon…

Treatment
A lot of information on the internet
Three main treatments:– Observation– Bracing
• Daytime• Nighttime• Spine-Cor
– Surgery

Treatment
11-25o 25-45o >40-50o
Skeletal maturity?* Skeletal maturity?
yes yesno no
F/u as needed
F/u every 4-6 mos until skeletal maturity
F/u q5 yrs to assess progression
Consider bracing, f/u q 4-6 mos
Consider surgical intervention
*skeletal maturity = Risser 3 or greater

Natural History
From Lonstein JE and Carlson JM JBJS Am 1984;66:1061-71.

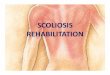
Treatment - bracing
Types– Full-time bracing
• Boston• Milwaukee (if apex
higher than T7)
– Night-time bending brace
• Charleston• Providence
– Others• Spine-Cor

Treatment - bracing
TLSO (Boston-type)– Worn as much as
possible• Can take off for
sports, sleepovers etc
– Want at least 50% correction in brace

Treatment - bracing
Milwaukee brace– For refractory curves– Apex >T7– Not really tolerated in
our patient population

Treatment - bracing
Night-time bending braces:– Overcorrects the curve– Only worn at night– Probably not as efficacious
• Price et al1 - 66% success, only 17% requiring surgery
• Randomized study - Charleston vs Boston brace2
– 41% vs 61% success (<5 degrees progression)
– 31% vs 19% required surgery
1. Price CT et al JPO 1997;17:703-707
2. Katz DE Spine 1997;22:1302-12.

Treatment - bracing
SpineCor– Well advertised– Soft straps, so more
easily worn under clothers/during physical activity
– Originators report only 40% progressed, only 23% needed surgery1
• Other authors have found no better results with SpineCor2
1. Christine C et al. Stud Health Technol Inform 2008;135:341-55.
2. Wong MS et al Spine 2008;33:1360-5.

Treatment - bracing Brace efficacy -
– Data all over the place, both for and against– Meta-analysis by Rowe et al1
• 1910 patients in 22 studies on non-operative treatments– Weighted mean proportion of success
» 0.93 for bracing» 0.49 for observation» 0.39 for electrical stimulation
– Prospective international study2
• Boston brace in girls with 25-35 degree curves– 74% success vs 34% with observation alone
– Prospective study of Boston brace with heat sensor (compliance)• >12 hours/day: 82% success• <7 hours/day: 31% success• Patients who went on to surgery: 24% compliance• Patients who did not progress to surgery: 42% compliance
1. Rowe DE et al JBJS Am 1997;79:664-74.
2. Nachemson AL et al JBJS Am 1995;77:815-22.
3. Katz DE et al JBJS Am 2010;92:1343-52.

Treatment - bracing Best for:
– Girls1
• Boys only 38% compliant with brace wear
• 30 degree curve 50% chance of surgery
– Lower BMI2
• BMI >85th %ile --> 2.5x risk of failure, double surgical rate
– More flexible curves– Younger patients
• Many studies• Higher rate of progression by
natural history
1. Karol LA Spine 2001;26:2001-5.
2. O’Neill PJ et al. JBJS Am 2005;87:1069-74.

Treatment - bracing Summary:
– Probably alters natural history in some but not all
• Especially if patient young, thin, and compliant
• Curve can definitely still progress
– Only tool we have to prevent progression
– Success = prevent progression• Never corrects the curve!
– Prospective, blinded, randomized controlled study needed
• BRAiST underway• Enrollment has been difficult

Treatment - surgery Indications for surgery:
– Thoracic curve >40-45 degrees in skeletally immature patient
– Thoracic curve >50 degrees in skeletally mature patient
– Lumbar numbers: usually around >40 degrees
– Double curves more well tolerated
Goals of surgery:– Achieve solid fusion SAFELY!– (improve cosmesis, body
image)

Treatment - surgery

Treatment - surgery No long-term, prospective controlled
studies to support hypothesis that surgery for AIS is superior to natural history– Reliably prevents progression– Achieves permanent correction– Improves appearance
Not a small undertaking– 4-7 day hospital stay– 6 months out of contact sports– Complications:1
• Infection 0-6%• Pseudarthrosis 2-7%• Reoperation rate 5-7%• Possibility of permanent neurologic
injury
– Expensive to health care system1. Westrick ER and Ward T JPO 2011;31:S61-8.

Treatment - surgery
A brief history of correction:– All methods at core the same:
• Expose the spine (facet joints)• Get correction
– Coronal plane (Cobb angle)
– Axial plane (rotation)
– Sagittal plane (maintain normal kyphosis/lordosis relationship)
• Wait for the fusion

Treatment - history of surgery
(Brief) history of correction– 1958, Moe
• Risser cast, bed rest, no instrumentation
• Ave correction 43%

Treatment - history of surgery
(Brief) history of correction– 1958, Moe
• Risser cast, bed rest, no instrumentation
• Ave correction 43%
– 1964, Moe• Harrington rods, Risser
cast
• Ave correction 55% --> 41%

Treatment - history of surgery
(Brief) history of correction– 1958, Moe
• Risser cast, bed rest, no instrumentation
• Ave correction 43%
– 1964, Moe• Harrington rods, Risser cast
• Ave correction 55% --> 41%
– 1992, Lenke• CDI - Cotrel Dubousset
instrumentation
• Ave correction 48%

Treatment - history of surgery
(Brief) history of correction– 2004, Luk et al
• Comparative studies of 4 different systems (CD Horizon, Moss-Miami, TSRH, Isola)
• Ave correction: 63% for CD Horizon, Moss-Miami vs 58% for TSRH, Isola
• Equal when matched against bending films

Treatment - history of surgery
(Brief) history of correction– 2004, Luk et al
• Comparative studies of 4 different systems (CD Horizon, Moss-Miami, TSRH, Isola)
• Ave correction: 63% for CD Horizon, Moss-Miami vs 58% for TSRH, Isola
• Equal when matched against bending films
– 2005, Suk• Introduction of pedicle screw• Ave correction 62%
– Other pedicle screw correction rate: 62-76%

Treatment - current techniques
Approach:– Posterior vs– Anterior
• Open vs• Thoracoscopic
– Combined approach• For very big, stiff curves• Younger patients
– To prevent crankshaft

Treatment - current techniques
Standard posterior approach– Positioning
• Prone• neuromonitoring
– Approach• Posterior exposure• Careful at most cephalad and caudal ends to
avoid unnecessary exposure• +/- Use of C-arm

Treatment - current techniques
Preparing the spine for fusion– Facetectomies
“loosening up the spine”– Ponte osteotomies– Allow for better Cobb
correction and kyphosis creation

Treatment - current techniques
Screw placement– Free-hand– With C-arm– With O-arm– Definitely dealer’s choice
Correction– In 3 planes
• Coronal (straight rods)• Axial (derotation)• Sagital (rod contour)

Treatment - current technique
Screw types– Monoaxial– Uniplanar– Polyaxial
Ways to reduce the screws to the rods– Reduction screws– Reduction tools
• Each company has their specific types

Treatment - current techniques
Preparation for fusion– Facetectomies– Decortication
• Various techniques
– Addition of bone graft• Autograft (iliac crest)• Allograft
– Many options!
Closure!– +/- drain– +/- brace

Treatment - current techniques
“MIS” scoliosis surgery– Applying some adult
techniques to pediatric scoli
– At cephalad levels mostly
– ? Fusion rates?

Overview
Definition Etiology Prevalence/Natural History Screening/Evaluation Treatment
– Non-operative– Operative
On the Horizon…

On the Horizon Scoli score = developed by Axial Biotech/Jim Ogilvie and
crew– Saliva test– Predictive of progression– For Caucasian girls, age 9-13, with curves between 10 and 25
degrees• Likelihood will progress to surgical curve
– Based on 53 genetic markers– Log scale from 0 to 200– Very high and very low scores helpful, middle score unclear– Not widely used or accepted– Expensive– May be more helpful in research
• Ie are curves with high scores those that progress despite a brace?

On the Horizon “Fusionless”
techniques:– Compressing anterior
overgrowth• Vertebral stapling• Spinal tethering
– Newton et al» Encouraging
results in animal model
» Human trials just starting
“Fusionless” techniques:– Compressing anterior
overgrowth• Vertebral stapling• Spinal tethering
– Newton et al» Encouraging
results in animal model
» Human trials just starting

Summary AIS
– 3-dimensional deformity– Defined as 10 degrees of curve on PA xray– Exact cause unknown; watch for red flags– Screening controversial but still recommended by
most• Girls at 10 and 12 years (younger better)• Boys at 13 or 14 years
– > 7 degrees on Adams forward bend, consider xray vs referral to orthopaedist
– Treatment• Based on age and size of curve• Includes observation, bracing, and surgery

Thank you