-
8/9/2019 MRI and CT of Nasopharyngeal CA
1/8
AJR:198 , January 2012 11
and has the worst prognosis. It is analogous
to squamous cell carcinoma elsewhere in the
pharynx and is associated with cigarette and
alcohol use. Nonkeratinizing carcinoma (type
2) behaves in a fashion similar to type 3. Both
types are radiosensitive and have a much bet-
ter prognosis. Undifferentiated carcinoma
(type 3) was previously called B lymphoep-
ithelioma because of the mix of undifferen-
tiated epithelial and nonmalignant T lym-
phocytes. In North America, around 25% of
patients with NPC have type 1, 12% have type
2, and 63% have type 3. The histologic distri-
bution in southern China is 2%, 3%, and 95%,
respectively [2–6].
Imaging Techniques
MRI
The protocol for routine MRI of a naso-
pharyngeal mass includes unenhanced T1-
weighted images to detect skull base involve-
ment and fat planes (in at least an axial and
sagittal plane). A T2-weighted fast spin-echo
sequence in axial plane is used for the ad-
ditional assessment of early parapharyngealtumor spread,
paranasal sinus invasion, mid-
dle ear effusions, and detection of cervical
lymph nodes. Axial and coronal contrast-en-
hanced T1-weighted images (with and with-
out fat suppression) are used to detect tumor
extent, including perineural spread and in-
tracranial extension of the tumor. The slice
thickness is 3–5 mm [3–7].
Additional MRI sequences may be used in
evaluation of NPC but, at present, are of lim-
MRI and CT of NasopharyngealCarcinoma
Ahmed Abdel Khalek Abdel Razek1
Ann King2
Abdel Razek AAK, King A
1Department of Diagnostic Radiology, Mansoura
University Hospital, Faculty o f Medicine, ElghomheryiaSt,
Mansoura DK, Egy pt. Address correspondence to
A. A. K. Abdel Razek ([email protected]).
2Department of Diagnostic Radiology and Interventional
Radiology, Chinese University of Hong Kong, Hong Kong,
China.
Neuroradio logy/Head and Neck Imaging • Review
AJR 2012; 198 :11–18
0361–803X/12/1981–11
© American Roentgen Ray Society
Nasopharyngeal carcinoma (NPC)
is a unique disease with clinical
behavior, epidemiology, and his-
topathology that is different from
that of squamous cell carcinomas of the head
and neck. NPC accounts for 0.25% of all ma-
lignancies in the United States and 15–18% of
malignancies in southern China. It also ac-
counts for 10–20% of childhood malignan-
cies in Africa. The male to-female ratio is 3:1.
It is most common among patients 40–60
years old, and bimodal age peaks occur in the
second and sixth decades of life [1–5]. NPC is
caused by the interaction of genetic suscepti-
bility, environmental factors (e.g., exposure to
chemical carcinogens), and infection with Ep-
stein-Barr virus. High antibody titers to Ep-
stein-Barr virus antigens are useful diagnostic
markers, and there are many tests to detect
both IgG and IgA titers. In China, dietary fac-
tors for NPC include nitrosamine-rich salted
food [2–5]. Patients often present with local
symptoms, such as epistaxis and a blocked
nose, but may also present with hearing loss,
otalgia, headache, or cranial nerve (CN) in-volvement. However,
the nasopharynx is a rel-
atively clinically silent area; therefore, the
first presentation may be with cervical nodal
or distant metastasis [1–6].
Pathology
The World Health Organization classifica-
tion of NPC recognizes three histologic types.
Keratinizing squamous cell carcinoma (type
1) is found more often in nonendemic areas
Keywords: cancer, imaging, lymph node, MRI,
nasopharynx
DOI:10.2214/AJR.11.6954
Received March 25, 2011; accepted after revision
August 8, 2011.
This article was presented as educational exhibit at
RSNA 2010.
F O C U S O N :
OBJECTIVE. This article reviews the MRI and CT of
nasopharyngeal carcinoma. Ex-
tension of nasopharyngeal tumors, especially into the skull base
and the deep facial spaces,
is well illustrated on imaging. Assessment of retropharyngeal
and cervical lymphadenopa-
thy is important for treatment planning. MRI is commonly used
for monitoring patients af-
ter therapy.
CONCLUSION. Imaging can detect effect of radiation on
surrounding structures. The
imaging findings that help to differentiate nasopharyngeal
carcinoma from simulating lesionsare discussed.
Abdel Razek and KingImaging of Nasopharyngeal Carcinoma
Neuroradiology/Head and Neck ImagingReview
-
8/9/2019 MRI and CT of Nasopharyngeal CA
2/8
-
8/9/2019 MRI and CT of Nasopharyngeal CA
3/8
AJR:198 , January 2012 13
Imaging of Nasopharyngeal Carcinoma
lies above the roof of the nasopharynx. The
ethmoid and sphenoid are less commonly
involved. Sinus involvement is recognized
by the loss of contiguity of the sinus walls.
Intrasinus extension of tumor may be seen.
Tumor can be differentiated from reactive
mucosal thickening on MRI, where inflam-
matory mucosal thickening is seen as uni-form T2-weighted signal
greater than that
of tumor, also enhancing to a greater degree
than tumor [1, 10].
Category T4 NPC— Meningeal involve-
ment appears as nodular enhancement, often
along the floor of middle cranial fossa or pos-
terior to the clivus. Direct invasion of the brain
is rare. Invasion of cavernous sinus can lead to
multiple cranial palsies. NPC may spread into
the cavernous sinus from tumor surrounding
the horizontal portion of the internal carotid
artery, foramen ovale, orbital fissures, or di-
rectly through the skull base [1, 6, 10].
The frequency of diagnosed CN palsy in
NPC ranges from 8.0% to 12.4%, and the
clinical and MRI findings are not always
consistent. Nerves are resistant to tumor, and
perineural tumor spread is an insidious and
often asymptomatic process by which NPC
can invade upward and backward through
the skull base to the cavernous sinus and
middle cranial fossa and invade CN II to VI
(upper CN palsy). It may also involve the ca-
rotid space, where it may compress or invade
CN XII as it exits through the hypoglossal
canal, CN IX to XI as they emerge from the
jugular foramen (lower CN palsy), and the
cervical sympathetic nerves.
CN involvement on MRI is seen when
there is either enhancement of soft-tissue tu-
mor along the course of the ipsilateral related
nerve, replacing the normal structures of the
CN on gadolinium-enhanced T1-weighted
images; or perineural spread, with enlarge-ment or abnormal
enhancement of the nerve,
obliteration of the neural fat pads adjacent to
the neurovascular foramina, or neuroforam-
inal enlargement. Maxillary and mandibu-
lar nerve involvement is best seen on coronal
T1-weighted contrast-enhanced MRI with
fat saturation. Hypoglossal nerve involve-
ment may also occur [13, 19] (Fig. 5).
Orbital invasion is a marker of extensive dis-
ease. Direct orbital invasion is rare, but when
present it can invade via the inferior orbital fis-
sure (from tumor in the pterygopalatine fossa),
optic canal, and superior orbital fissure.
Anatomic masticator space involvement
affects the overall survival and local relapse-
free survival of patients with NPC. The fre-
quency of masticator space involvement in
NPC is 19.7%. Infiltration of the medial and
lateral pterygoid muscles, infratemporal fat,
and temporalis muscle is found when tumors
extend laterally from the parapharyngeal
space, pterygoid base, or the pterygomaxil-
lary fissure [4, 20]. Hypopharynx is the most
inferior site of tumor invasion included in the
staging classification, but it is very rarely in-
volved at diagnosis [1–3].
N Category
NPC has a propensity to spread to nodes
(Fig. 6) and, in about 75–90% of cases, is
found by imaging to have a tendency for bi-
lateral neck spread [21]. Nodal metastases
are diagnosed if the shortest nodal axial di-
ameter reaches 5 mm or greater in the lateral
retropharyngeal region, 11 mm in the jugu-lodigastric region, or
10 mm in other non-
retropharyngeal nodes of the neck; if there
is a group of three or more nodes that are
borderline in size; or if the nodes display ne-
crosis or extracapsular spread. Extracapsular
spread has also been shown to be an indepen-
dent prognostic factor [8, 22].
Retropharyngeal Lymph Nodes
The diagnosis of enlarged retropharyngeal
lymph nodes in patients with NPC can only
be made by imaging, and MRI has an ad-
vantage over CT in being better able to sep-
arate the lateral retropharyngeal nodes from
the primary tumor in the adjacent postero-
lateral nasopharynx. Lateral retropharyngeal
nodes are among the most common sites of
nodal spread from NPC and have been con-
sidered the first echelon of metastatic spread
[21] (Fig. 7). However, nodal spread may by-
pass these nodes and spread to other nodes of
the upper neck. Metastatic lateral retropha-
ryngeal nodes can be identified from the skull
base to the level of C3. Retropharyngeal node
involvement is now classified as category N1,
whether unilateral or bilateral [1, 23]. PET/CT
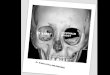
Fig. 1—49-year-old woman with nasopharyngealcarcinoma (NPC)
localized to nasopharynx (T1). Axialcontrast-enhanced T1-weighted
image shows smallNPC (short arrows ) centered in
left Rosenmüllerfossa (long arrow ), which is the most common
sitefor this cancer, and involving posterior wall. Tumoris confined
to nasopharynx, and there is smallmetastatic left retropharyngeal
node (curved arrow ).
Fig. 2—50-year-old man with nasopharyngealcarcinoma (NPC) with
parapharyngeal extension(T2). Axial contrast T1-weighted image
shows NPC(white arrows ) with left parapharyngeal
extensionand involvement of parapharyngeal fat space. Notenormal
levator palatini muscle (red arrow ),
tensorpalatini muscle (blue arrow ),
pharyngobasilar fascia(black arrow ), and fat space
(yellow arrow ) on normalright side
Fig. 3—58-year-old man with nasopharyngealcarcinoma with
prevertebral extension (T2). AxialT1-weighted contrast-enhanced
image showsnasopharyngeal carcinoma (straight arrows )
withextensive spread predominantly posteriorly intolongus muscles
(arrowheads ) and clivus (curvedarrows ).
-
8/9/2019 MRI and CT of Nasopharyngeal CA
4/8
14 AJR:19 8, January 2012
Abdel Razek and King
reveals increased FDG uptake in metastatic
cervical lymph nodes, but MRI appears to be
superior to PET/CT for the assessment of ret-
ropharyngeal nodal metastasis because of the
better discrimination of nodes from the adja-
cent primary tumor [24].
Other Cervical Lymph Nodes
Metastatic nodes posterior to the jugu-
lar vein in the upper neck are the most com-
mon sites for nonretropharyngeal nodes [22]
and are designated as high internal jugular
nodes, although at this site, the internal jug-
ular and spinal accessory nodal chains con-verge. Nodes then
usually spread in an or-
derly sequence down the neck. Nodes in the
submandibular and parotid or periparotid re-
gion are far less common at diagnosis. Nodal
metastases at supraclavicular fossa increase
the incidence of distant metastases [1].
M Category
NPC shows a high frequency of distant me-tastases (5–41%). The
most common sites of
metastases include bone (20%), lung (13%),
and liver (9%). Patients with supraclavicu-
lar lymphadenopathy or tumors extension
into the parapharyngeal and retropharyngeal
space have a significantly higher risk of dis-
tant metastases. PET/CT is sensitive to detect
bony and soft-tissue metastatic deposits [8].
Whole-body MRI shows a diagnostic capac-
ity similar to that of FDG PET/CT in assess-
ing distant-site status in patients with untreat-
ed NPC; in one reported study, the combined
interpretation of whole-body MRI and FDG
PET/CT showed no significant benefit over ei-
ther technique alone [24].
Tumor Volume
Tumor volume is a significant prognostic
factor in the treatment of malignant tumors.
However, it is not used presently in staging
because technical considerations have pre-
vented tumor volume measurement from be-
ing routinely used in a clinical setting and be-
cause methods for volume measurement are
not standardized. The measurement of tumor
volume has always been tedious and often in-
volves tracing the tumor outline. The resultsare often affected
by both intra- and interop-
erator performance. To overcome this prob-
lem, several investigators have developed
semiautomated systems to reduce inter- and
intraoperator variability. Errors encountered
by computer-based techniques are thus likely
to be classified as systematic errors and not as
resulting from the experience of the operator.
Semiautomated tumor volume measurementis now possible for NPC
[25, 26].
Pediatric NPC
Pediatric NPC is rare and usually poorly dif-
ferentiated. It has a predilection for adolescents
and teenagers. Unfortunately, these tumors
tend to be locally advanced by the time they
are diagnosed, mainly because the clinical pre-
sentation is nonspecific. Gross parapharyngeal
space invasion is common, and tumor can also
extend to the pterygopalatine fossa. Metastasis
to liver and spleen in NPC commonly presents
as solitary or multiple solid masses. Lymphoid
hyperplasia, which is more common in the
younger population, can be differentiated from
pediatric NPC by the symmetric configuration
and a striped pattern on both T2-weighted and
contrast-enhanced images. Also, rhabdomyo-
sarcoma can be differentiated from pediatric
NPC by lower peak incidence (3–10 years) and
inhomogeneous enhancement with necrotic in-
tratumoral foci [27].
After Treatment
The primary treatment for NPC is radia-
tion therapy, but induction chemotherapy
with 5-fluorouracil cisplatin is sometimescombined with
radiation therapy. NPC is
Fig. 4—Patient with nasopharyngeal carcinoma(NPC) with skull
base invasion and pterygoid sclerosis(T3). A xial CT bone window
shows large NPC fillingnasopharynx and nasal cavity with bony
destructionof sphenoid bone, including right pterygoid base,which
also shows sclerosis (arrow ). Right middle eareffusion is
present.
A
Fig. 5—68-year-old man with nasopharyngeal carcinoma (NPC) with
skull base foraminal invasion . A, Coronal T1-weighted
contrast-enhanced MRI shows NPC (straight arrows ) with skull
base invasion at foramen ovale (arrowhead ) with invasion into
cavernous sinus(curved arrow ).B, Coronal T1-weighted
contrast-enhanced MRI shows invasion of NPC (straight arrows )
into foramen lacerum (arrowheads ), where it encases carotid
artery andextends into cavernous sinus (curved
arrow ).C, Axial T1-weighted contrast-enhanced MRI shows
NPC invading pterygopalatine fossa (circle ), pterygomaxillary
fissure (arrow ), and vidian canal (arrowhead ).
CB
-
8/9/2019 MRI and CT of Nasopharyngeal CA
5/8
AJR:198 , January 2012 15
Imaging of Nasopharyngeal Carcinoma
treated primarily by a high radiation dose (>
60 Gy), and in conventional (2D) radiothera-
py, the nasopharynx and adjacent region are
treated by radiation beams from the left and
right sides and sometimes also with an an-
terior radiation beam. The neck lymphatics
are usually irradiated by a separate anterior
radiation beam. Intensity-modulated radio-
therapy offers the opportunity of dose es-
calation to the tumor without increasing the
dose to other organs at risk. These treatmentsrequire very
accurate delineation of the gross
tumor volume [3, 28].
Tumor Recurrence
It is advantageous to obtain a scan 3–6
months after radiation therapy to provide a
baseline study against which any future im-
aging can be compared. Regular surveil-
lance imaging is also desirable, but its value
has not been proven, especially for patients
with early-stage disease in whom the radio-
therapy response rates are high. Therefore,
follow-up scans are often guided by clini-
cal factors, such as suspicion of tumor recur-rence or
development of a radiation-induced
complication. Any enlarging posttreatment
soft-tissue mass or any new deep lesion or
intracranial enhancement is concerning for
recurrent disease [1, 3].
Differentiating fibrosis from tumor re-
currence is difficult on routine CT. PET/
CT often provides an easier method for dif-
ferentiating tumor recurrence from fibrosis.
Typically, recurrent tumors show uptake of
radionuclide tracer, but fibrosis does not.
MRI can differentiate mature scar tissue,
which shows retraction, low T2 signal, and
no contrast enhancement from tumor, which
is expansile and of intermediate T2 signal
with moderate contrast enhancement on non-
fat-saturated images (Fig. 8). However, there
may be an overlap between partially treated
tumor and immature scar tissue. MRI shows
a trend toward higher accuracy in detecting
disease at the primary site than does PET/
CT, although the latter shows a trend toward
higher accuracy in detecting nodal disease
[28–30].
Nonmalignant Pharyngeal MassNonmalignant pharyngeal masses
are
seen in less than 1% of MRI examinations
performed 2–14 years (mean, 8 years) after
radiation therapy. It has two patterns. The
first is a nasopharyngeal polyp (1–5 cm) that
shows mixed heterogeneous T2 signal inten-
sity and marked contrast enhancement (Fig.
9), with the larger polyps having stellate ar-
eas of reduced enhancement. The second is
a sphenoid sinus mass, which consists of a
nonenhancing mass filling a nonexpanded
sinus and a heterogeneous-enhancing mass
expanding the sinus or nonenhancing rhino-
liths in the sphenoid sinus. This appearance
in sphenoid sinus, as well as the larger polyps
with a stellate appearance, can be similar to
that of radiation-induced sarcomas [31].
Trismus With Masticator Space Abnormalities
Trismus is most commonly due to abnor-
mality of masticator muscles as a result of
the effects of radiation and rarely is second-
ary to damage of the mandibular nerve. It
may be due to osteoradionecrosis of the man-
dibular ramus and temporomandibular joint
Fig. 6—Patient with metastatic cervical lymphnode (N2). Axial
T1-weighted contrast-enhancedMRI shows metastatic node
(arrow ) posterior to leftupper internal jugular vein, which
is common site formetastatic node with or without
retropharyngealnodal involvement.
Fig. 7—Patient with retropharyngeal metastaticcervical lymph
node (N1). Axial T1-weighted contrast-enhanced MRI shows metastatic
node (arrow ) inleft retropharyngeal region, which is
frequently firstechelon for nodal spread.
A
Fig. 8—Patient with nasopharyngeal carcinoma (NPC)
recurrence.A, Image obtained before treatment shows NPC
involving nasopharyngeal mucosa, centered in rightRosenmüller fossa
(straight arrow ) with deep posterior extension
into longus muscles (curved arrow ).B, Image obtained 3
months af ter treatment shows that mucosal component of tumor has
resolved (straightarrow ) leaving behind mild symmetric post
treatment mucosal thickening in nasopharynx. Deep component issmall
residual mass (curved arrow ), which is nonspecific and could
represent early scar tissue or residual cancer.
B
-
8/9/2019 MRI and CT of Nasopharyngeal CA
6/8
16 AJR:19 8, January 2012
Abdel Razek and King
or abnormality in the perimasticator tissues
as a result of radiation fibrosis or inflamma-tion spreading
from sinusitis. One half of
patients have no significant abnormality on
MRI [4, 32] (Fig. 10).
Temporal Lobe Injury
Temporal lobe injury occurs in 3% of pa-
tients of NPC with a latent period of 1.5–13
years. Depending on the radiation field, it may
be bilateral or unilateral. It can involve the gray
and white matter simultaneously or the gray
matter alone; however, isolated white matter
lesions are rare. Temporal lobe injury result-
ing from radiation is not always an irrevers-
ible and progressive process but is one that canregress or
resolve at MRI. In the evolution of
radiation injury, white matter lesions are seen
first and are followed by contrast-enhanced le-
sions, which have an increasing tendency to be-
come necrotic with increasing size. Cysts are
the least frequent manifestation and arise in the
late stages (Fig. 11). MRI spectroscopy in early
delayed phase of injury shows reduced N-ace-
tyl aspartate and creatine levels and increasedcholine levels as
a result of demyelination. The
late delayed phase of radiation injury shows the
decrease of N-acetyl aspartate, choline, and
creatine levels [33].
Osteoradionecrosis
Osteoradionecrosis may occur 1 year after
irradiation. It is believed to be secondary to os-
teoblastic destruction with subsequent vascu-
lar damage. The skull base, cervical spine, and
the mandible are commonly affected. Imaging
findings include areas of osteolysis and mixed
sclerosis (Fig. 12) within the irradiation por-
tal. Fragmentation and sloughing of necroticbone may also be
found. There is surrounding
inflammatory soft-tissue mass that may mimic
tumor recurrence or osteomyelitis [34].
Radiation-Induced Tumors
Radiation-induced tumors ar ise 5–10 years
after irradiation of NPC in 0.4–0.7% of cas-
es. Sarcomas and squamous cell carcinomas
arise in the high-dose field zone and involvesites around the
maxillary region, such as the
palate, maxillary sinus, alveolar process, and
nasal cavity. Squamous cell carcinomas also
arise in the low-dose field, may occur many
years after radiotherapy, and may involve pe-
ripheral sites such as the temporal bone. The
presence of a heterogeneous tumor or rapidly
growing large destructive mass that displays
different signal intensity from NPC should
suggest the possibility of a radiation-induced
sarcoma. The presence of calcification or os-
sification points strongly to a diagnosis of ra-
diation-induced sarcoma [2, 35].
Differentiation of NPC From
Simulating Lesions
Lymphoma
The nasopharynx is one of the most com-
mon sites of extranodal non-Hodgkin lympho-
ma in the head and neck region. It usually oc-
curs in the sixth decade of life and is associated
A
Fig. 12—61-year-old man with osteoradionecrosis.A, Axial CT
scan bone window showsosteoradionecrosis in skull base with
sclerosis andosteolysis.B, Sagittal CT scan bone window
showsosteoradionecrosis in anterior arch of C1 (long
arrow )and tip of dens (short arrow ).
B
Fig. 9—54-year-old man with nonmalignantpharyngeal mass. Axial
T1-weighted contrast-enhanced MRI shows small markedly
enhancinginflammatory polyp (arrow ) arising from
posteriorwall of nasopharynx.
Fig. 10—Patient with changes to pterygoid muscleafter radiation
therapy. Axial T2-weighted MRIshows increased T2 signal in
pterygoid muscles(arrows ) mainly involving left side.
Fig. 11—50-year-old man with radiation-inducedinjury to temporal
lobe. Coronal T2-weighted MRIshows bilateral radiation-induced
injury to whitematter in temporal lobes (arrows ).
-
8/9/2019 MRI and CT of Nasopharyngeal CA
7/8
AJR:198 , January 2012 17
Imaging of Nasopharyngeal Carcinoma
with gastrointestinal tract lymphoma in up to
10% of patients at either the time of diagno-
sis or relapse. Lymphoma is frequently located
in the midline, unlike NPC, which often arises
laterally. Bone invasion is not common even in
large tumors, and as with NPC, nodes are fre-
quent but these may involve sites such as the
submandibular and parotid nodes, which areless frequently
involved at presentation in pa-
tients with NPC. Also, lymphoma has a lower
apparent diffusion coefficient value than does
NPC because of its higher cellularity [6–8].
Adenoid Cystic Carcinoma
Adenoid cystic carcinoma usually affects
patients during middle age and there is no re-
ported sex predilection. Unlike patients with
NPC, patients with adenoid cystic carcino-
mas rarely present with cervical lymphade-
nopathy. This tumor has a greater propensity
for perineural spread than does NPC. The tu-
mor exhibits higher apparent diffusion coef-
ficient value on diffusion-weighted MRI be-
cause of its cystic component [6, 7].
Extramedullary Plasmacytoma
Extramedullary plasmacytoma is a rare ma-
lignant soft-tissue tumor, but 80% of these tu-
mors occur in the head and neck with the na-
sopharynx being a common site. It is most
commonly seen in the sixth and seventh decades
and has an 80% male preponderance. The tu-
mor transgresses into a multiple myeloma in 20–
30% of cases. The lesion may present as a sub-
mucosal homogeneous and enhancing polypoidnasopharyngeal mass
several centimeters in di-
ameter, with or without bone destruction [6].
Pleomorphic Adenoma
Pleomorphic adenoma occurs in the pha-
ryngeal mucosal space, arising from minor
salivary gland tissue. When associated bone
changes are present, benign-appearing bone
remodelling is the typical pattern. However,
slowly progressive bone destruction with an
aggressive appearance can be observed [36].
Tuberculosis
Nasopharyngeal tuberculosis is rare andis thought to result from
direct infection of
the upper respiratory tract. It mimics NPC,
especially in Asian patients. It has two pat-
terns. The first pattern is a discrete polypoid
mass in the adenoids, and the second pattern
is a more diffuse soft-tissue thickening of
one or two of the walls of the nasopharynx.
Extension outside the confines of the naso-
pharynx is not usually a major feature [37].
Pseudotumor
Fibrosing inflammatory pseudotumor is
a nonspecific inflammatory process of un-
certain cause that rarely involves the naso-
pharynx. MRI findings that help to differen-
tiate pseudotumors from NPC are ill-defined
less likely contour bulging features, with lo-
cal infiltration, hypointensity on T2-weight-ed images,
relatively weak enhancement, no
significant regional lymphadenopathy, and
good response to steroid therapy [38].
Amyloidosis
On CT, amyloidosis appears as a well-de-
fined submucosal homogeneous calcified
mass without bone destruction with or with-
out lymphadenopathy. The lesion exhibits
minimal enhancement. On MRI, the submu-
cosal location, distinctive hypointensity on
T2-weighted imaging, and early enhancement
on dynamic contrast-enhanced MRI helps to
differentiate amyloidosis from NPC [39].
Conclusion
In conclusion, MRI is essential for detec-
tion of early NPC, staging of the primary tu-
mor, and evaluation of associated retropha-
ryngeal and cervical lymphadenopathy. It has
been used for monitoring patients after thera-
py to detect tumor recurrence and radiation-
associated changes in the soft tissue and bone.
Imaging is valuable for the differentiation of
NPC from other simulating lesions.
References 1. King A, Bhatia KS. Magnetic resonance
imaging
staging of nasopharyngeal carcinoma in the head
and neck. World J Radiol 2010; 2:159–165
2. Chong VF, Ong CK. Nasopharyngeal carcinoma.
Eur J Radiol 2008; 66:437–447
3. Glastonbury C. Nasopharyngeal carcinoma: the
role of magnetic resonance imaging in diagnosis,
staging, treatment, and follow-up. Top Magn Re-
son Imaging 2007; 18:225–235
4. Dubrulle F, Souillard R, Hermans R. Extension
patterns of nasopharyngeal carcinoma. Eur Radi-
ol 2007; 17:2622–2630
5. Chin S, Fatterpekar G, Chen C, Som P. MR imag-
ing of diverse manifestations of nasopharyngeal
carcinomas. AJR 2003; 180:1715–1722
6. Weber AL, al-Arayedh S, Rashid A. Nasophar-
ynx: clinical, pathologic, and radiologic assess-
ment. Neuroimaging Clin N Am 2003; 13:465–483
7. Goh J, Lim K. Imaging of nasopharyngeal carcino-
ma. Ann Acad Med Singapore 2009; 38:809–816
8. Ng S, Chan S, Yen T, et al. Pretreatment evalua-
tion of distant-site status in patients with nasopha-
ryngeal carcinoma: accuracy of whole-body MRI
at 3-Tesla and FDG-PET-CT. Eur Radiol 2009;
19:2965–2976
9. Fong D, Bhatia KS, Yeung D, King AD. Diagnos-
tic accuracy of diffusion-weighted MR imaging
for nasopharyngeal carcinoma, head and neck
lymphoma and squamous cell carcinoma at the
primary site. Oral Oncol 2010; 46:603–606
10. King A, Yeung D, Ahuja A, Leung S, Tse G, van
Hasselt A. In vivo proton MR spectroscopy of pri-
mary and nodal nasopharyngeal carcinoma.
AJNR 2004; 25:484–490
11. King AD, Vlantis AC, Bhatia KS, et al. Primary
nasopharyngeal carcinoma: diagnostic accuracy
of MR imaging versus that of endoscopy and en-
doscopic biopsy. Radiology 2011; 258:531–537
12. Edge SB, Byrd DR, Compton CC, Fr itz AG,
Greene FL, Trotti A. American Joint Committee
on Cancer Staging Manual, 7th ed. New York:
Springer-Verlag, 2010:41–49
13. Hyare H, Wisco J, Alusi G, et al. The anatomy of
nasopharyngeal carcinoma spread through the
pharyngobasilar fascia to the trigeminal mandib-
ular nerve on 1.5 T MRI. Surg Radiol Anat 2010;
32:937–944
14. King AD, Lam WW, Leung SF, Chan YL, Teo P,
Metreweli C. MRI of local disease in nasopharyn-
geal carcinoma: tumour extent vs tumour stage.
Br J Radiol 1999; 72:734–741
15. Ng WT, Chan SH, Lee AW, et al. Parapharyngeal
extension of nasopharyngeal carcinoma: still a
significant factor in era of modern radiotherapy?
Int J Radiat Oncol Biol Phys 2008; 72:1082–1089
16. Lee CC, Chu ST, Chou P, Lee CC, Chen LF. The
prognostic influence of prevertebral space in-
volvement in nasopharyngeal carcinoma.
ClinOtolaryngol 2008; 33:442–449
17. Chen L, Liu LZ, Mao YP, et al. Grading of MRI-
detected skull-base invasion in nasopharyngeal
carcinoma and its prognostic value. Head
Neck
2011; 33:1309–1314
18. Shatzkes D, Meltzer D, Lee J, Babb J, Sanfilippo
N, Holliday R. Sclerosis of the pterygoid process
in untreated patients with nasopharyngeal carci-
noma. Radiology 2006; 239:181–186
19. Liu L, Liang S, Li L, et al. Prognostic impact of
magnetic resonance imaging detected cranial
nerve involvement in nasopharyngeal carcinoma.
Cancer 2009; 115:1995–2003
20. Tang LL, Li WF, Chen L, et al. Prognostic va lue
and staging categories of anatomic masticator
space involvement in nasopharyngeal carcinoma:
a study of 924 cases with MR imaging. Radiology
2010; 257:151–157
21. King AD, Ahuja AT, Leung SF, et al. Neck node
metastases from nasopharyngeal carcinoma: MR
imaging of patterns of disease. Head
Neck 2000;
22:275–281
22. Wang XS, Hu CS, Ying HM, Zhou ZR, Ding JH,
-
8/9/2019 MRI and CT of Nasopharyngeal CA
8/8
18 AJR:19 8, January 2012
Abdel Razek and King
Feng Y. Patterns of retropharyngeal node metas-
tasis in nasopharyngeal carcinoma. Int J Radiat
Oncol Biol Phys 2009; 73:194–201
23. Tang L, Li L, Mao Y, et al. Retropharyngeal
lymph node metastasis in nasopharyngeal carci-
noma detected by magnetic resonance imaging
prognostic value and staging categories. Cancer
2008; 113:347–354
24. King AD, Yau YY, Zee B, et al. The impact of18F-FDG
PET/CT on assessment of nasopharyn-
geal carcinoma at diagnosis. Br J Radiol 2008;
81:291–298
25. Chong VH. Tumour volume measurement in head
and neck cancer. Cancer Imaging 2007; 7:S47–S49
26. Lee CC, Huang TT, Lee MS, et al. Clinical appli-
cation of tumor volume in advanced nasopharyn-
geal carcinoma to predict outcome. Radiat Oncol
2010; 5:20
27. Stambuk H, Patel S, Mosier K, Wolden S, Holod-
ny A. Nasopharyngeal carcinoma: recognizing
the radiographic features in children. AJNR 2005;
26:1575–1579
28. Ng S, Liu H, Ko S, Hao S, Chong V. Posttreatment
imaging of the nasopharynx. Eur J Radiol 2002;
44:82–95
29. King A, Ahuja A, Yeung D, et al. Delayed compli-
cations of radiotherapy treatment for nasopharyn-
geal carcinoma: imaging findings. Clin Radiol
2007; 62:195–203
30. Ng S, Chan S, Yen T, et a l. Comprehensive imag-
ing of residual/recurrent nasopharyngeal carci-
noma using whole-body MRI at 3 T compared
with FDG-PET-CT. Eur Radiol 2010; 20:2229–
2240
31. King A, Ahuja A, Leung S, et al. MR imaging of
nonmalignant polyps and masses of the nasophar-
ynx and sphenoid sinus after radiotherapy for naso-
pharyngeal carcinoma. AJNR 2008; 29:1209–1214
32. Bhatia K, King A, Paunipagar B, et al. MRI find-
ings in patients with severe trismus following ra-
diotherapy for nasopharyngeal carcinoma. Eur
Radiol 2009; 19:2586–2593
33. Wang YX, King AD, Zhou H, et al. Evolution of
radiation-induced brain injury: MR imaging-
based study. Radiology 2010; 254:210–218
34. King AD, Griffith JF, Abrigo JM, et a l. Osteora-
dionecrosis of the upper cervical spine: MR imag-
ing following radiotherapy for nasopharyngeal
carcinoma. Eur J Radiol 2010; 73:629–635
35. Makimoto Y, Yamamoto S, Takano H, et al. Im-
aging findings of radiation-induced sarcoma of
the head and neck. Br J Radiol 2007; 80:790–797
36. Downer J, Fryer E, Capper J, Woo E. Pleomorphic
adenoma of the nasopharyngeal mucosal space
with locally aggressive appearance. Eur Radiol
2011; 21:443–446
37. King A, Ahuja A, Tse G, van Hasselt A, Chan A.
MR imaging features of nasopharyngeal tubercu-
losis: report of three cases and literature review.
AJNR 2003; 24:279–282
38. Lu CH, Yang CY, Wang CP, Yang CC, Liu HM,
Chen YF. Imaging of nasopharyngeal inflamma-
tory pseudotumours: differential from nasopha-
ryngeal carcinoma. Br J Radiol 2010; 83:8–16
39. Motosugi U, Ichikawa T, Araki T, Endo S, Ma-
suyama K, Nakazawa T. Localized nasopharyn-
geal amyloidosis with remarkable early enhance-
ment on dynamic contrast-enhanced MR imaging.
Eur Radiol 2007; 17:852–853
F O R Y O U R I N F O R M A T I O N
Unique customized medical search engine service from ARRS!
ARRS GoldMiner ® is a keyword- and
concept-driven search engine that provides instant access to
radiologic images published in peer-reviewed
journal s. For more infor mat ion, visit htt
p://goldminer. arrs. org.