Embed Size (px)
Citation preview

MRD in myeloma
UKMF Spring Day
Assessment of disease response, CR and beyond.
Roger Owen
St James’s Institute of OncologyLeeds, UK

Myeloma trials: the challenges
Complex multicomponent
therapy
Increasing survivalM protein issues

What do we need?
Applicability
Consensus on methodology
Predicts PFS and OS including CR pts
Cytogenetic risk groups
Transplant eligible and ineligible
Upfront and relapse
Independent of treatment
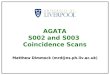
Flow cytometry in MM.
Minimum four colour method Gating using CD38, CD138 and CD45 MRD+ defined by a minimum of 100 events (106 total events
acquired for a sensitivity of 0.01%) Clonality assessment suboptimal for MRD due to the presence of
normal cells in post treatment samples Aberrant phenotype defined by CD19 and CD56
Leeds - CD138/CD38/CD45/CD19/CD56/CD27
Applicability ~97%

Value of flow cytometry in the routine setting
• Confirmation of a diagnosis of myeloma- good practice c.f. acute leukaemia- immunohistochemistry on trephine sections only
needed in limited situations - saves time and money• Differential diagnosis of MGUS and MM• Outcome prediction – MGUS, smouldering MM and
plasmacytoma• Amyloidosis• Rare / difficult cases • Response assessment

Flow cytometry in AL amyloidosis. 97% of patients have aberrant phenotype PCs
Paiva B et al. Blood 2011;117:3613-3616
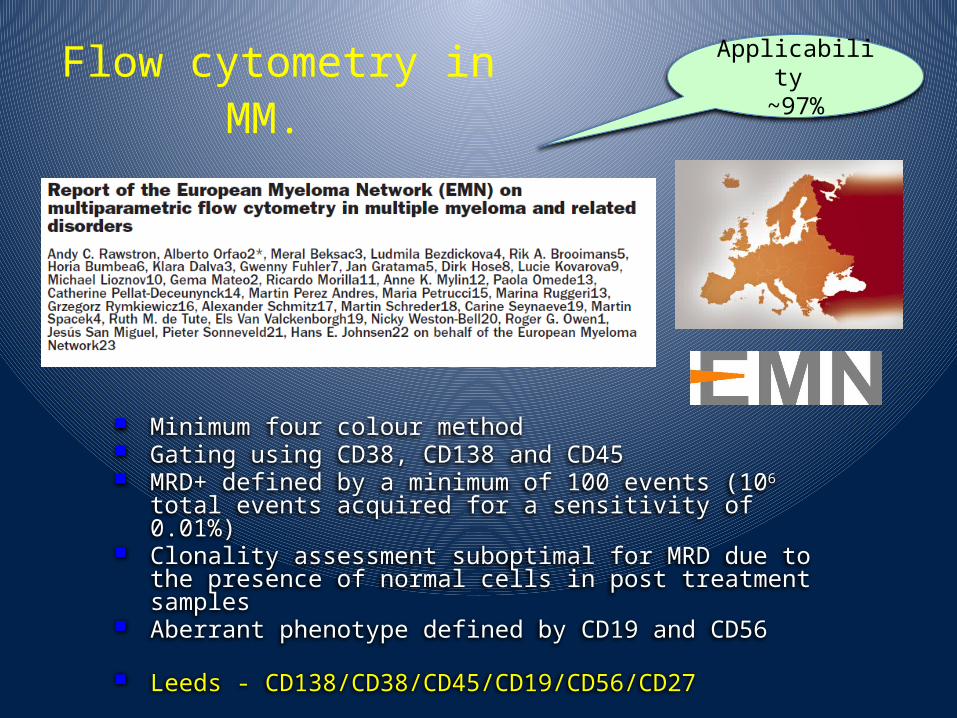
Perez-Persona, E. et al. Blood 2007;110:2586-2592Updated BJ Haem epub October 2009
Progression in MGUS (A) and SMM (B) – Salamanca data
Adverse risk defined by >95% aberrant phenotype plasma cells.

2002!


MRC Myeloma IX— Trial Design
Intensive
ClodronateCVAD
Zoledronic acidCVAD
ClodronateCTD
Zoledronic acidCTD
MEL-200ASCT
–Thal +Thal
Non-intensive
ClodronateMP
Zoledronic acidMP
ClodronateCTDa
Zoledronic acidCTDa
MaximalResponse
–Thal +Thal
N = 1,960
RANDOMISATION RANDOMISATION
RANDOMISATION RANDOMISATION


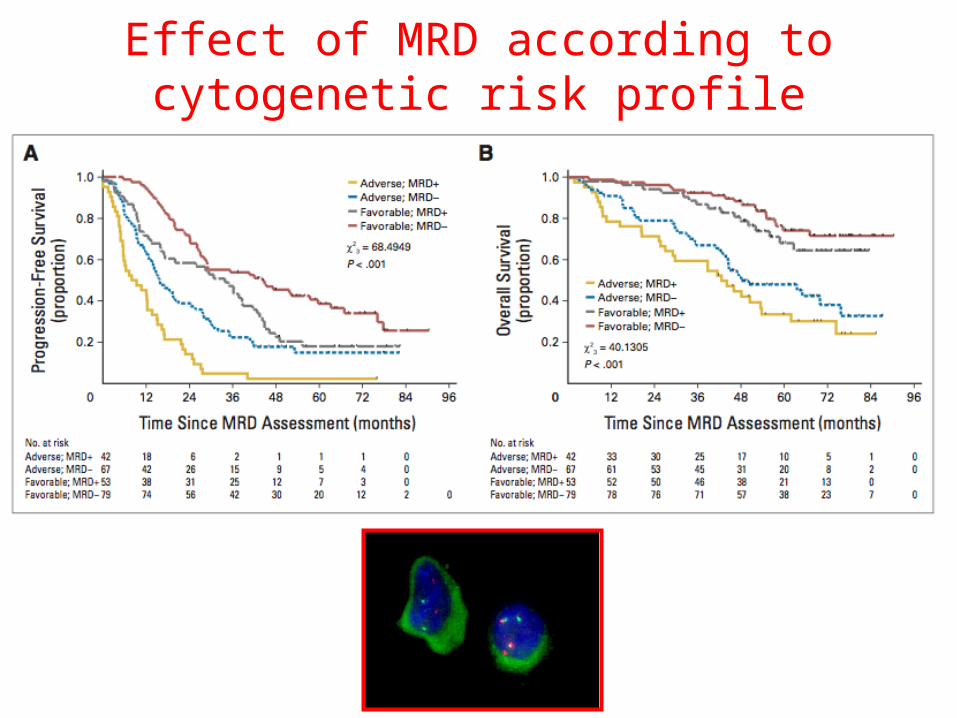
Effect of MRD according to cytogenetic risk profile

Paiva B et al. Blood 2012;119:687-691


What about salvage Rx?
Ashcroft et al, ASH 2013Paiva et al, Haematologica. 2015;100(2):e53-5.

Impact of therapy received
1 2 3 4 5 6 7 8
20
40
60
80
100
TIME (YEARS)
% P
FS
MRD- CVAD n = 113 MRD+ CVAD n = 95 MRD- CTD n = 134 MRD+ CTD n = 55
2
3= 24.30
P < .00001
de Tute et al, submitted
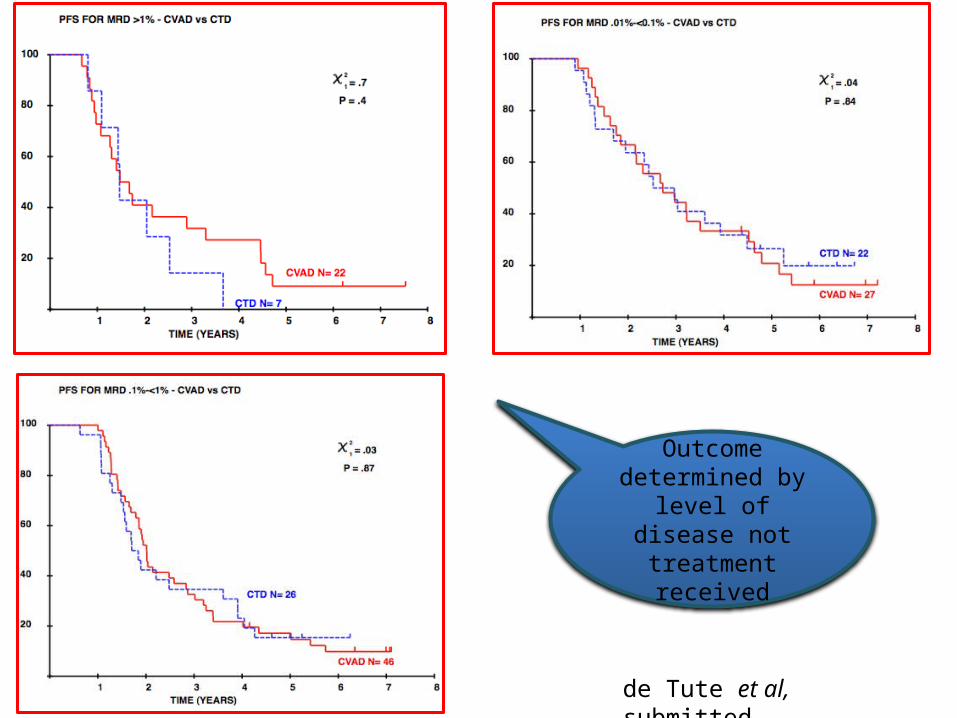
de Tute et al, submitted
Outcome determined by level
of disease not treatment received


CR patients only?

MRD predicts outcome in CR patients.
Paiva et al. Blood 2008;112:4017-4023

MRD and M protein response
Rawstron et al, 2015

Bruno Paiva et al. Blood 2008;112:4017-4023
MRD and M protein response

MRD and M protein response.
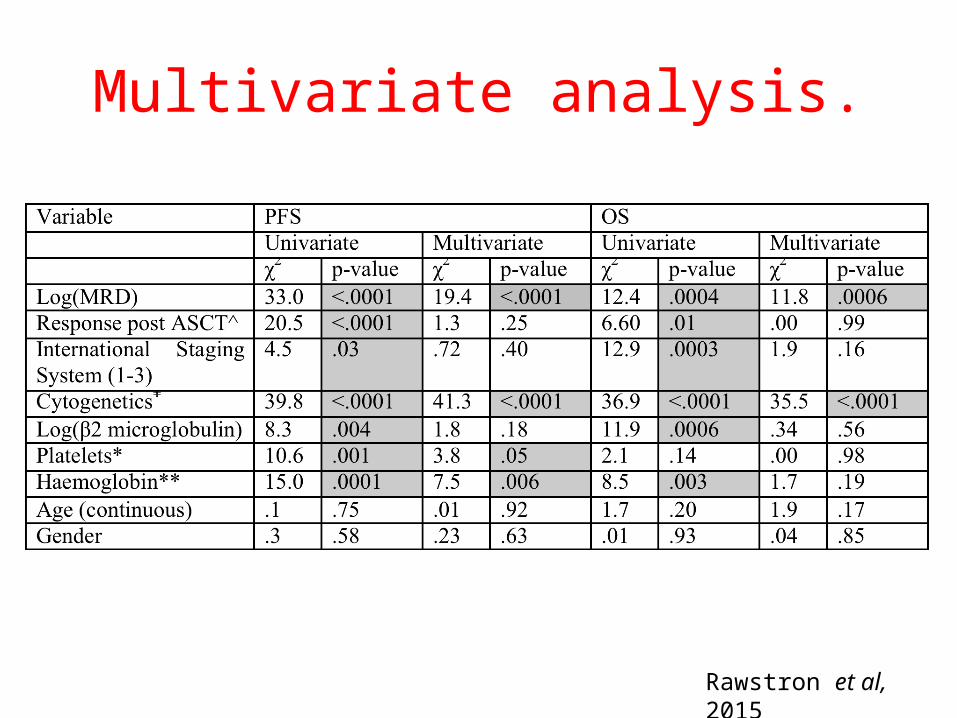
Multivariate analysis.
Rawstron et al, 2015



MRD: Comparison of induction regimens.CVAD CTD
Post induction (n=252)
13% 25% P=0.004
Day 100(n=397)
54% 71% P<0.0001

Ongoing role of ASCT?
Rawstron et al, J Clin Oncol. 2013 ;31(20):2540-7
Paiva B et al. Blood 2008;112:4017-4023

Maintenance

No change in conventional response with thalidomide maintenance but clear differences in neoplastic plasma cell levels
• “Using electrophoresis and immunofixation as a monitoring technique, there was no difference between the thalidomide maintenance and no maintenance arms in the percentage of patients that upgraded response status over time (P .19).” (1)
27.6
96
3.4
68.8
0
20
40
60
80
100
Become MRD negative Remain MRD negative
Thalidomide maintenance
No maintenance(2)
1. Morgan et al, Blood 2012, 119(1): 7-152. Rawstron, JCO 2013; 31(20):2540-7

1 2 3 4 5 6 7 8 9 100
0.2
0.4
0.6
0.8
1.0
0
Years from Diagnosis
Pro
por
tion
free
fro
m d
isea
se p
rogr
essi
on
P=0.003
Normal phenotype plasma cells
Neoplastic phenotype plasma cells
Outcome prediction in SPB
Hill et al, Blood 2014
IMWG – “solitary plasmacytoma with minimal marrow involvement”
IDRIS study of Len-Dex in high-risk patients

Conclusions.
MRD assessment is highly predictive of outcome
CR patientsStandard and adverse risk cytogeneticsPresentation and relapseASCT and non-ASCT
Assessment of individual components of multicomponent treatment schedules and maintenance strategies
Thalidomide / Bortezomib eradicates MRD in a proportion of patients

University of BirminghamMT DraysonK WalkerA AdkinsN Newnham
Wessex Regional Genetics Laboratory, SalisburyF RossL Chieccio
LTHT, LeedsG CookS FeylerD Bowen
HMDS, LeedsRG OwenAC RawstronR de TuteM DewarS Denman
ICR, LondonFE DaviesM JennerB WalkerD JohnsonD GonzalezN DickensK BoydP LeoneL BritoA Avridromou
MRC Leukaemia Trial Steering Committee
MRC Leukaemia Data Monitoring and Ethics Committee
NCRI Haematological Oncology Clinical Studies Group
NIHR, through the National Cancer Research Network
UK Myeloma Forum Clinical Trials Committee
Myeloma UK
FundingMedical Research CouncilPharmion Novartis Chugai Pharma Bayer Schering PharmaOrthoBiotech CelgeneKay Kendall Leukaemia Fund
Chief InvestigatorsJA ChildGJ MorganGH Jackson
CTRU, LeedsK CocksW GregoryA SzubertS BellN Navarro CoyF HeatleyP BestJ CarderM MatoukD EmsellA DaviesD PhillipsA GillmanL FlanaganC Tyas and others
Acknowledgements