Embed Size (px)
Citation preview

Minimally Invasive Therapy. 2009; 18:3; 1–8
ISSN 1364-5706 print/ISSN 1365-2931 online © 2009 Informa UK LtdDOI: 10.1080/13645700902921971
ORIGINAL PAPER
MR-compatible polyetheretherketone-based guide wire assisting MR-guided stenting of iliac and supraaortic arteries in swine: Feasibility study
SEBASTIAN KOS1, ROLF HUEGLI2, EUGEN HOFMANN3, HARALD H. QUICK4, HILMAR KUEHL4, STEPHANIE AKER5, GERNOT M. KAISER6, PAUL J. A. BORM7, AUGUSTINUS L. JACOB1, DENIZ BILECEN1
1Institute of Radiology, University Hospital Basel, Basel, Switzerland, 2Institute of Radiology, Kantonsspital Bruderholz Bruderholz, Switzerland, 3Biotronik, Vascular Intervention, Buelach, Switzerland, 4Department of Diagnostic and Interventional Radiology and Neuroradiology, University of Duisburg-Essen, Essen, Germany, 5Institute of Pathophysiology, University of Duisburg-Essen, Essen, Germany, 6Department of General-, Visceral-, and Transplantation Surgery, University of Duisburg-Essen, Essen, Germany, 7MagnaMedics GmbH, Aachen, Germany
AbstractThe purpose of this study was to demonstrate first magnetic resonance (MR)-guided stenting of iliac and supraaortic arteries using a polyetheretherketone-based (PEEK) MR-compatible guide wire. In vitro and animal experiments were performed in a short magnet wide-bore scanner (1.5 Tesla, Espree®, Siemens Healthcare, Erlangen, Germany). For all experiments, a 0.035″ MR-compatible guide wire prototoype was used. This wire had a compound core of PEEK with reinforcing fibres, a soft and atraumatic tip and a hydrophilic coating. For its passive visualization, paramagnetic markings were attached. All experiments were performed through a vascular introducer sheath under MR-guidance. In vitro repetitive selective over the wire catheterizations of either the right carotid artery and the left subclavian artery were performed. In vivo, selective catheterization and over-the-wire stenting of the brachiocephalic trunc and the left subclavian artery were performed. The common iliac arteries were catheterized retrogradely (left) and cross-over (right). Angioplasty and stenting were performed over-the-wire. All procedures were successful. Visibility of the PEEK-based guide-wire was rated good in vitro and acceptable in vivo. Guide wire pushability and endovascular device support were good. The PEEK-based MR-compatible guide wire is well visible and usable under MR-guidance. It supports over the wire treatment of iliac arteries and supraaortic arteries.
Key words: Guide wire, stenting, supraaortic, iliac, PEEK, MR-compatible
Introduction
Magnetic resonance imaging (MRI) provides excellent soft-tissue contrast and allows 3D image depiction of the vascular lumen, the vessel wall and the adjacent tissues and organs. MRI does not expose patients and staff to ionising radiation and may even allow some endovascular interventions without the use of con-trast media. Contrast-enhanced MR-angiography allows precise assessment of the vascular tree, but gadolinium-based contrast media must be applied with care, as they may cause nephrogenic sclerosing fibrosis (NSF). As MRI depicts both morphology and
function (e. g. temperature, oxygenation, flow, perfusion etc.) it may further help to determine the functional result of an endovascular intervention (1).
Despite these potential advantages of MR-guidance, image guided endovascular procedures are mostly exclusively performed under fluoroscopic guidance. Only few MR-guided endovascular experimental studies have been described in the literature (2–7). Interven-tional MR-systems, fast MR-sequences and some commercially available balloons, stents and catheters (though not CE-marked or FDA approved “off-label” for MR-guidance) allow MR-guided procedures, to
Correspondence: S. Kos, University Hospital Basel, Institute of Radiology, Division of Interventional Radiology, Petersgraben 4, CH-4031 Basel, Switzerland, Fax: +41-61-2655383; E-mail: [email protected]

2 S. Kos et al.
a limited extent. However the missing link was an MR-safe and visible endovascular guide wire (2,8–10).
Lacking such an MR-safe and visible wire, in vivo studies either used off-label nitinol guide wires in the magnetic field, or even interventions were per-formed without using a guide wire (11–15). Metal based electrically conductive guide wires lead to the severe risk of inductive heating and sparking in vivo, increasing the risk to dissect or perforate the vessels wall (3,11,16-18).
First concepts of MR-safe polymer based guide wires were described (19,20) and in vivo usability of such MR-compatible guide wires has been shown for aortic stenting and cava filter placement in swine (21).
The goal of this feasibility study was to demonstrate the usability of the 0.035 inch MR-compatible PEEK-based guide wire to support endovascular catheterization and stenting of common iliac and supraaortic arteries in a porcine animal model.
Material and methods
MR-compatible PEEK-based guide wire and Marking Technique
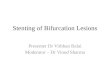
A new MR-compatible guide wire was applied, as described earlier (Biotronik Vascular Intervention, Buelach, Switzerland) (Figure 1) (21). This 0.035 inch guide wire is 160 cm long and has a central compound
A. B.
Figure 1. Pictures of the passively marked MR-compatible PEEK-based 0.035 inch guide wire (A) and the passively marked (arrowheads) non-braided 5 French Shepherd Flush catheter (B) used in the experiments.
core (0.57 mm Ø) based on PEEK, reinforced by fibres. This compound is tapered at the distal 12 cm (min. 0.15 mm Ø) of the guide wire, forming a soft and atraumatic tip. Along its axis, the guide wire has a hydrophilic coating over a polyurethane jacket. For its passive visualization, MR-markers are applied to distal portion of the guide wire. Those (0.03 mm thick, 1.5 mm broad) markers are applied by dip-coating with iron-oxide (Fe3O4) nanoparticles (“MagnaFy”; MagnaMedics GmbH, Aachen, Germany) on the polyurethane jacket, prior to hydrophilic coating. For the phantom experiments, four markers are spaced by 15 mm. For the animal experiments the four most distal markers are separated by 20 mm and two markings, further proximal, are separated by 40 mm.
The same marking technique was applied to the non-braided catheters used for the experiments (Figure 1).
MR-Imaging and MR-Suite
All experiments were conducted in a 1.5-T short magnet wide-bore scanner (Espree®, Siemens Healthcare, Erlangen, Germany) as described earlier (21). The system was equipped with a high-performance gradient system (slew rate: 100 T/m/s; gradient strength: 33 mT/m). Standard phased-array surface radiofrequency (RF) receiver coils were used. MR-images were displayed beside the MR-scanner on an 18” in-room monitor (Siemens Healthcare, Erlangen, Germany).
In vitro, a steady state free precession (True-FISP) sequence with the following sequence parameters was used: Field of view = 200 mm × 150 mm voxel size = 1.0 × 0.8 × 10.0 mm; matrix size = 256 × 200; repetition time = 5.3 ms; echo time = 5.2 ms; flip angle = 80°, bandwidth = 399 Hz/P; frame rate = 1/s.
For animal experiments, a gradient echo T1-FLASH sequence (BEAT-IRT) with the following imaging parameters was used: Repetition time = 8.12 ms; echo time = 5.24 ms; field of view = 400 × 358 mm; matrix size = 288 × 172; voxel size = 2.3 × 1.4 × 5.0 mm; flip angle = 21°; bandwidth = 299 Hz/pixel; frame rate = 2/3 per second.
Phantom experiments
Experiments were conducted at the Department of Radiology, University Hospital Basel, Switzerland. MR images were obtained along the axis of the aortic arch and the supraaortic arteries of an aortic silicon phantom.
The aortic silicon phantom is a replica of a human aorta and consists of an abdominal and thoracic

MR-guided stenting: PEEK base guide wire 3
segment (T-R-N-002 and A-S-A-004, Elastrat, Geneva, Switzerland). A right-sided femoral vascular introducer sheath (Ultimum, 6 French Hemostasis; St. Jude Medical, Minnetonka, MN, USA) was used for access. The phantom was filled with Gadoterate meglumine doped water (Gd-DOTA) (Dotarem®, Guerbet, Roissy CDG Cedex, France). Gd-DOTA concentration was 0.5 ml per liter.
The procedures described were performed ten times. The PEEK-based guide wire was first advanced into the ascending aorta. A 5 French vertebral catheter was then advanced into the ascending aorta over-the-wire and the guide wire was retracted. The vertebral catheter was pulled back, engaging the brachiocephalic trunc or the left sub-clavian artery, respectively. The guide wire was then again advanced into the right common carotid artery or the left subclavian artery, respectively, followed by over-the-wire positioning of the vertebral catheter.
In vivo experiments
Animal experiments were conducted at the Department of Radiology, University Hospital Essen (Germany). The procedures were approved by the regional and institutional animal care and use committee and were performed according to the policies for human care and the use of animals.
Three female domestic pigs (60–70 kg BW) were prepared as described in earlier published protocols (21,22). Using a 6.5 mm endotracheal tube, ventilation was performed throughout the intervention by a res-pirator (Oxylog, Draeger, Luebeck, Germany) and anesthesia was continuously applied by i. v. infusion of fentanyl, propofol and midazolam.
A standard 11 French/10 cm catheter sheath (Radiofocus® Introducer II, Terumo, Leuwen, Belgium) was surgically positioned into the left external iliac artery. Initially an intravenous heparin bolus (5000 U) was given, followed by 1000 U heparin every hour. The swine was positioned head-first supine within the MR-scanner.
To allow better vessel depiction throughout endovascular procedures, a single intravenous bolus injection (dosage: 0.03 mmol gadolinium / kg body weight) of blood-pool contrast media gado-fosveset (Vasovist®, BayerSchering Pharma, Berlin, Germany) was administered before the in vivo experi-ments. No further contrast media was given throughout the endovascular procedures described below.
In this study all balloons and stents were applied as commercially available, without additional MR-markings. These devices had standard x-ray absorbing device markings (platinum (90%) iridium (10%) alloy) attached to the delivery catheter. The
use of balloons and stents was performed “off-label” as these instruments are not CE-marked for delivery and usage in MR-guided interventions.
Subclavian artery stenting
Through the introducer sheath, the guide wire was advanced twice into the thoracic segment of the descending aorta. The left subclavian artery was directly probed twice. Over the positioned guide wire, a 6/38 mm (diameter / length) 316L stent (Peiron, Biotronik, Buelach, Switzerland) was posi-tioned in the postostial segment of the left subclavian artery and deployed.
Stenting brachiocephalic trunc
The guide wire was advanced into the thoracic segment of the descending aorta. The marked non-braided 4 French vertebral catheter (SOFTouch®, Merit Medical, Galway, Ireland) was advanced into the aortic arch. The catheter engaged the ostium of the brachio-cephalic trunc. The guide wire was consecutively advanced in the distal vessel parts. The vertebral catheter was removed and a 9/30 mm self-expandable nitinol stent (Astron, Biotronik, Buelach, Switzerland) positioned and deployed in the postostial portion of the brachiocephalic trunc.
Iliac artery stenting
Owing to the small diameter (10 mm) of the abdominal aorta in our swine, configuration of the 5 French non-braided Shepherd Flush catheter (Merit Medical, Galway, Ireland) used for cross-over maneuver could not be performed in the abdominal aorta. Therefore the guide wire was advanced into the ascending aorta, followed by the catheter. The guide wire was retracted back and the catheter was configured. The non-braided catheter was then pulled back into the abdominal segment of the descending aorta. Through the catheter, the guide wire was advanced into the contralateral (right) iliac artery and the catheter was then positioned on the bifurcation.
With the guide wire in the external iliac artery, the catheter was removed and a non-marked 5/40 mm balloon-catheter (Pheron, Biotronik, Buelach, Switzerland) was inserted over-the-wire. Angioplasty was performed in the common iliac artery twice, adjacent to the bifurcation. The balloon-catheter was removed and a balloon-expandable 5/30 mm stent (Peiron, Biotronik, Buelach, Switzerland) was positioned and deployed.
Finally the guide wire was pulled back into the abdominal aorta and ipsilateral 5/30 mm stenting

4 S. Kos et al.
(Peiron, Biotronik, Buelach, Switzerland) was performed over-the-wire.
For all procedures, procedure time was documented and procedure success (2 grades: +/-) was rated. The guide wire’s visibility, pushability and its support (3 grades: poor (+); acceptable (++); good (+++)) for the endovascular devices (balloon, stent, catheter) were assessed in consensus by the interventional radi-ologists. Animals were sacrificed by intravenous injection of a phenobarbital (80 mg/kg) bolus.
Results
Supraaortic arteries
Under exclusive MR-guidance, all procedures performed were successful in vitro and in vivo. Guide wire positioning in the ascending aorta descending thoracic aorta was feasible, as were selective catheterization of the brachiocephalic trunc and the left subclavian artery (Figure 2). Over-the-wire stent deployments were successful in vivo (Figure 3).
Iliac arteries
Over-the-wire positioning in the ascending aorta and configuration of the omni-flush catheter was
feasible (Figure 4). The cross-over manoeuvre was successful, as were consecutive cross-over balloon angioplasty and stenting of the right common iliac artery (Figure 5). After pull-back of the guide wire, stenting of the ipsilateral common iliac artery was feasible (Figure 5).
Mean procedure time for the in vitro procedures was four minutes. Procedure time for brachiocephalic, subclavian and iliac stenting was eight minutes, five minutes and seven minutes, respectively.
During the described experiments, the PEEK-based guide wire and also the passive markings applied to the wire and catheters remained intact. There was no macroscopic evidence of device fracture and/or kinking.
In consensus, guide wire visibility was rated good (+++) in the phantom experiments and acceptable (++) in vivo. Guide wire pushability and its support for catheters, stents and balloons were rated good (+++).
Discussion
This is the first study to demonstrate that MR-guided stenting using a MR-compatible PEEK-based guide wire is feasible, not only in straight, non-branching vessels, but also in the branches of the aortic arch.
Furthermore, this is the first study to demonstrate feasibility of an MR-guided cross-over manoeuvre even in acute-angled iliac arteries.
A. B. C. D.
E. F. G. H.
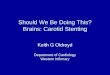
Figure 2. Synopsis of in vitro experiments. The PEEK-based guide wire is advanced into the ascending aorta (arrows in A and B). 4 French vertebral catheter is positioned in the ascending aorta over-the-wire (arrows in C and D). After guide wire retraction, the catheter is pulled back and engaged the brachiocephalic trunc (arrow in E). The guide wire is advanced through the catheter and positioned in the right common carotid artery (arrows in F and G). The catheter is advanced over-the-wire into the common carotid artery (arrow in H) and the guide wire is removed.

MR-guided stenting: PEEK base guide wire 5
Earlier studies have shown that MR-guided stenting of either supraaortic arteries or retrograde stenting of iliac arteries is feasible, but such studies have to be considered unsafe in vivo, as they applied standard metal based guide wires, bearing relevant risks of heating, as discussed above (23–25). This limitation has been overcome by the usage of the new PEEK-based guide wire.
Regarding the mechanical properties of the PEEK-based guide wire, its good pushability and good support for the over-the-wire devices used are mandatory for any endovascular procedure.
This first proof of concept study also demonstrates that this PEEK-based guide wire offers good to acceptable visibility through its applied passive markers. This passive marking technique allowed
A. B. C.
D. E. F.
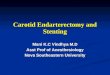
Figure 3. Maximum intensity projection (MIP) of the aortic arch in the swine (A). Note, that in the swine the left subclavian artery (arrow in A) branches from the aortic arch, whereas the right subclavian artery and both carotid arteries derive from the brachiocephalic trunc (arrowhead in A). For stenting of the brachiocephalic trunc, the guide wire was positioned in the descending aorta and a passively marked non-braided vertebral catheter was used to engage the ostium of the trunc (arrowheads in B). The guide wire was positioned in the trunc through the catheter (arrow in C). After catheter removal, the stent was advanced (arrow in D), positioned, and partially released (arrow in E). Fully deployed stent (arrow in F) is documented after removal of catheter and wire.
A. B. C.
Figure 4. To allow safe configuration of the 5 French Shepherd Flush catheter (arrowhead in A), the guide wire was positioned in the ascending aorta (arrow in A). The guide wire was retracted (arrow in B) and the catheter configured in the ascending aorta (arrowhead in B). After the catheter was pulled back into the ascending aorta (arrowhead in C), the guide wire was advanced pointing towards the abdominal aorta (arrow in C).

6 S. Kos et al.
easy usage of the wire and catheters, resulting in a short procedure time. Other studies using active tracking techniques (e.g. electrified wire loops, self-resonant radio-frequency circuits, or receiver coils) require a technically more complex setup and lead to longer procedure times consecutively (2,3,26–28). Passive self-resonant radio-frequency circuits are technically challenging but do not require complex setup and longer procedure time.
In this study we manually adjusted the scan plane according to direction of the targeted artery. As automated tracking techniques for passively marked interventional devices have been proposed, procedure control may be even further facilitated and also allow dynamic device tracking in branching vessels (29).
As described above, balloons and stents were applied in this study as commercially available, without additional MR-markings. This has lead to suboptimal visibility of these over-the-wire devices through a rather weak artifact, caused by x-ray absorbing markers. Passive markings may also be applied to these devices,
thus increasing visibility and the precision of positioning (e.g. balloons) and deployment (e.g. stents and cava filters) during MR-guided interventions. However, as such passive markers of different endovascular devices may overlap and thereby decrease their individual visibility and differentiation, even a combination of actively visualized devices with the passively marked PEEK-based guide wire should be considered a conceivable combination.
In the future, size and thickness of passive markings equivalent to the imaging behaviour may also be adapted to the individual diameter of the targeted vessel, to allow precise tracking and positioning, without obscuring the whole vessel lumen by the induced artifact of the devices. This would require frequent exchange of the guide wire and raise the cost per procedure. Different markers would also increase the cost of production, as different types of guide wires would have to be produced.
High-quality MR-angiography requires the usage of Gadolinium-based contrast agents. The additional i. v. administration of blood-pool contrast media provided
A. B. C.
D. E. F.
G. H. I.
Figure 5. For cross-over manoeuvre, the configured 5 French Shepherd Flush catheter was pulled back into the abdominal aorta (arrow in A). The guide wire was stepwise advanced into the contralateral common iliac artery (arrows in B and C) and the catheter was positioned on the bifurcation (arrow in D). After positioning of the guide wire in the external iliac artery, a balloon was placed in the common iliac artery over-the-wire and angioplasty was performed (arrow in E). After balloon removal, the balloon-expandable stent was positioned and deployed (arrow in F). The good positioning of the deployed stent (arrowhead in G) in the right common liliac artery is seen after guide wire pull back into the abdominal aorta (arrow in G). The stent was retrogradely advanced into left common liac artery and distal abdominal aorta over-the-wire (H). After its repositioning the stent was deployed at the same level as the contralateral stent (arrowheads in I).

MR-guided stenting: PEEK base guide wire 7
good vascular contrast and vessel-device contrast, which is attributed to its 4–6 fold higher relaxivity, when compared with extracellular MR contrast medium (30). Furthermore, by its longer blood half-life (average: 0.48 hours), the whole endovascular procedure may be performed using only a single injection of contrast media (31).
Usage of gadolinium-based contrast media may cause nephrogenic sclerosing fibrosis (NSF). However, to our knowledge, there were no NSF cases reported, related to the usage of gadofoseveset, as applied in this study.
This study was designed as a first proof of concept in a porcine animal model. Further investigations are necessary to determine the potential of this new PEEK-based guide wire for MR-guided interventions, especially in stenosed and/or occluded arteries and to acquire CE Mark and FDA approval.
Grant information
The research work presented herein was supported by a research grant (Swiss Confederation’s innovation promotion agency: Grant 7893.1 LSPP-LS).
Acknowledgements:
We thank Tanja Haas, RT and Verena Koch (University Hospital Basel, Switzerland) and Lena Schäfer (University Hospital Essen, Germany) for their support in MR imaging and figure illustration. We thank Viurel Rusu for application of paramagnetic markers on devices.
References
Rhee TK, Larson AC, Prasad PV, et al. Feasibility of blood 1. oxygenation level-dependent MR imaging to monitor hepatic transcatheter arterial embolization in rabbits. J Vasc Interv Radiol. 2005;16:1523–8.Kos S, Huegli R, Bongartz G, et al. MR-guided endovascular 2. interventions: a comprehensive review on techniques and applications. Eur Radiol. 2008;18:645–57.Bock M, Wacker F. MR-guided intravascular interventions: 3. techniques and applications. J Magn Reson Imaging 2008;27:326–38.Ozturk C, Guttman M, McVeigh ER, Lederman RJ. 4. Magnetic resonance imaging-guided vascular interventions. Top Magn Reson Imaging 2005;16:369–81.Wacker FK. [Interventionel MRT: current inventory and 5. preview]. Rofo. 2004;176: 941–3.Wacker FK, Hillenbrand CM, Duerk JL, Lewin JS. MR-guided 6. endovascular interventions: device visualization, tracking, navigation, clinical applications, and safety aspects. Magn Reson Imaging Clin N Am. 2005;13:431–9.
Schulz T, Puccini S, Schneider JP, Kahn T. Interventional and 7. intraoperative MR: review and update of techniques and clinical experience. Eur Radiol. 2004;14:2212–27.Immel E, Melzer A. Improvement of the MR imaging behavior 8. of vascular implants. Min Invas Ther & Allied. Technol. 2006;15:85–92.Schaefers G, Melzer A. Testing methods for MR safety and 9. compatibility of medical devices. Min Invas Ther & Allied. Technol. 2006;15:71–5.Shellock FG. Reference Manual for Magnetic Resonance 10. Safety, Implants and Devices: 2008 Edition. Biomedical Research Publishing Group. Los Angeles CA, 2008.Bucker A, Neuerburg JM, Adam GB, et al. Real-time MR 11. Guidance for inferior vena cava filter placement in an animal model. J Vasc Interv Radiol. 2001;12:753–6.Eggebrecht H, Kuhl H, Kaiser GM, et al. Feasibility of 12. real-time magnetic resonance-guided stent-graft placement in a swine model of descending aortic dissection. Eur Heart J. 2006;27:613–20.Omary R, Gehl J, Schirf B, et al. MR imaging- versus 13. conventional X-ray fluoroscopy-guided renal angioplasty in swine: prospective randomized comparison. Radiology 2006;238:489–96.Omary RA, Frayne R, Unal O, et al. MR-guided angioplasty 14. of renal artery stenosis in a pig model: a feasibility study. J Vasc Interv Radiol. 2000;11:373–81.Shih MC, Rogers WJ, Hagspiel KD. Real-time magnetic 15. resonance-guided placement of retrievable inferior vena cava filters: comparison with fluoroscopic guidance with use of in vitro and animal models. J Vasc Interv Radiol. 2006;17:327–33.Manke C, Nitz W, Lenhart M, et al. [Stent angioplasty of 16. pelvic artery stenosis with MRI control: initial clinical results]. Rofo. 2000;172:92–7.Nitz WR, Oppelt A, Renz W, et al. On the heating of 17. linear conductive structures as guide wires and catheters in interventional MRI. J Magn Reson Imaging 2001;13:105–14.Wildermuth S, Dumoulin CL, Pfammatter T, et al. MR-guided 18. percutaneous angioplasty: assessment of tracking safety, catheter handling and functionality. Cardiovasc Intervent Radiol. 1998;21:404–10.Krueger S, Schmitz S, Weiss S, et al. An MR guidewire based 19. on micropultruded fiber-reinforced material. Magn Reson Med. 2008;60:1190–6.Mekle R, Hofmann E, Scheffler K, Bilecen D. A polymer-based 20. MR-compatible guidewire: a study to explore new prospects for interventional peripheral magnetic resonance angiography (ipMRA). J Magn Reson Imaging 2006;23:145–55.Kos S, Huegli R, Hofmann, E, etal. First Magnetic Resonance 21. Imaging-Guided Aortic Stenting and Cava Filter Placement Using a Polyetheretherketone-Based Magnetic Resonance Imaging-Compatible Guidewire in Swine: Proof of Concept. Cardiovasc Intervent Radiol. 2008 [e-published ahead of print].Kaiser G, Breuckmann F, Aker S, et al. Anesthesia for 22. cardiovascular interventions and magnetic resonance imaging in pigs. J Am Assoc Lab Anim Sci. 2007;46:30–3.Feng L, Dumoulin CL, Dashnaw S, et al. Feasibility of stent 23. placement in carotid arteries with real-time MR imaging guidance in pigs. Radiology 2005;234:558–62.Krombach GA, Wehner M, Perez-bouza A, et al. Magnetic 24. resonance-guided angioplasty with delivery of contrast-media doped solutions to the vessel wall: an experimental study in swine. Invest Radiol. 2008;43:530–7.Buecker A, Adam GB, Neuerburg JM, et al. Simultaneous 25. real-time visualization of the catheter tip and vascular anatomy for MR-guided PTA of iliac arteries in an animal model. J Magn Reson Imaging 2002;16:201–8.

8 S. Kos et al.
Quick HH, Kuehl H, Kaiser G, et al. Interventional MRA 26. using actively visualized catheters, TrueFISP, and real-time image fusion. Magn Reson Med. 2003;49:129–37.Quick HH, Zenge MO, Kuehl H, et al. Interventional magnetic 27. resonance angiography with no strings attached: wireless active catheter visualization. Magn Reson Med. 2005;53:446–55.Ocali O, Atalar E. Intravascular magnetic resonance imaging using 28. a loopless catheter antenna. Magn Reson Med. 1997;37:112–8.
Rauschenberg J, de Oliveira A, Muller S, et al. [An algorithm 29. for passive marker localization in interventional MRI]. Z Med Phys. 2007;17:180–9.Meaney J, Goyen M. Recent advances in contrast-enhanced 30. magnetic resonance angiography. Eur Radiol. 2007;17 Suppl 2: B2–6.Bremerich J, Bilecen D, Reimer P. MR angiography with 31. blood pool contrast agents. Eur Radiol. 2007;17:3017–24.