Embed Size (px)
Citation preview

Should We Be Doing This?
Sealing Dissections: Thoracic Stenting
Dr Peter Wilde – Consultant Cardiac RadiologistDr K Balachandran – Cardiology SpRMr A Bryan – Consultant Cardiac Surgeon
Dr A Baumbach – Consultant Cardiologist
Bristol Royal Infirmary

Should We Be Doing This?
Sealing DissectionsSealing Leaks
Closing AneurysmsRepairing Transections

P Wilde - BCIS Autumn Meeting Bristol – 30th September 2005
Stanford Type B Dissection(Intramural haematoma)

P Wilde - BCIS Autumn Meeting Bristol – 30th September 2005
Aneurysms

P Wilde - BCIS Autumn Meeting Bristol – 30th September 2005
Penetrating atherosclerotic
ulcer

P Wilde - BCIS Autumn Meeting Bristol – 30th September 2005
Transection

P Wilde - BCIS Autumn Meeting Bristol – 30th September 2005
Acute or chronic?
Acute ( <2 weeks) Recent chest painEvidence of bleedingEvidence of recent expansion
ChronicSlow increase in sizeAbsolute size of aneurysmMass effects

P Wilde - BCIS Autumn Meeting Bristol – 30th September 2005
What about surgery?

P Wilde - BCIS Autumn Meeting Bristol – 30th September 2005
Acute type B dissection
Surgical mortality 30-80%
Medical treatment mortality 10-15%
20-30% have a complication requiring intervention
No clear case for surgery in the majority

P Wilde - BCIS Autumn Meeting Bristol – 30th September 2005
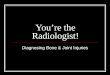
Nienaber, Zanetti et al., Am Heart J 2003
Cumulative survival of subacute type B dissection with medical therapy

P Wilde - BCIS Autumn Meeting Bristol – 30th September 2005
Thoracic aortic aneurysm resection
Elective surgical mortality at least 10%
Higher mortality in complex cases
Paraplegia rate 5-10%

P Wilde - BCIS Autumn Meeting Bristol – 30th September 2005
Acute post traumatic transection
Surgical mortality at least 15%, may be much more
Associated major trauma, especially head injury
Lower incidence of paraplegia

P Wilde - BCIS Autumn Meeting Bristol – 30th September 2005
Surgery on the Thoracic Aorta
Operations frequently last 5-7 hours
Partial cardiopulmonary bypass or circulatory arrest required
Prolonged intensive care required
Surgeons hate operating on the descending thoracic aorta

P Wilde - BCIS Autumn Meeting Bristol – 30th September 2005
Thoracic Aortic Stent Grafting (TASG)
First performed in 1994 – immediate clinical benefitsthere are no controlled trials available yet (INSTEAD)

P Wilde - BCIS Autumn Meeting Bristol – 30th September 2005

P Wilde - BCIS Autumn Meeting Bristol – 30th September 2005
Rationale for an INvestigation of STEntgrafts in Aortic Dissection (INSTEAD)-study
Hypothesis
Should the concept of stent-graft induced aortic remodeling be applied to stable dissection?
Mid-term outcomes of stent-graft placement in type B dissection?
Improvement of the natural course of type B dissection?
Design
MC, prospective, randomized
Endpoints
Outcomes at 1 & 2 years, events, remodeling of aorta

P Wilde - BCIS Autumn Meeting Bristol – 30th September 2005
Literature review of TASG (‘meta analysis’)
15 publications 1996 – 2005632 patientsSeries from 12 to 110 patientsFull range of indicationsApprox. 30% acute casesOverall early mortality 5.1%Paraplegia only 1.3% ( 0.8% recovered)

P Wilde - BCIS Autumn Meeting Bristol – 30th September 2005
Guy’s Hospital Results 1997 – 2005(Courtesy Dr J Reidy)
143 patients (66% Male)
Age 17-90 yr (mean 72)
Many non-surgical or poor surgical risk
33% for acute indications
Overall 30 day mortality 7.7%
11% acute, 6.2% chronic
Paraplegia 4.9% ( 3.5% recovered)
Late mortality 15% (mean f/u 34m)

P Wilde - BCIS Autumn Meeting Bristol – 30th September 2005
TASG Indications
Traumatic rupture Strong indication for TASG – anatomy usually favourable – long term results?
AneurysmIntervene over 5.5cm assess on a case by case basis according to anatomy
Type B dissection
Currently only indicated in ‘active’ cases (continuing pain, expansion, bleeding) but……..
Emerging evidence begins to suggest all Type B dissections
Penetrating atherosclerotic ulcerStrong indication if bleeding and anatomy is suitable

P Wilde - BCIS Autumn Meeting Bristol – 30th September 2005
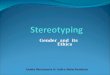
Nienaber, Zanetti et al., Am Heart J 2003
Medical therapy Elective stent graft
Cumulative survival of subacute type B dissection: Stent graft v. historical group with medical therapy

P Wilde - BCIS Autumn Meeting Bristol – 30th September 2005
Complications of TASG
Paraplegia
Stroke
Vascular complication (femoral/iliac)
Device migration
EndoleakType 1 – marginal leakType 2 – external collateral fillingType 3 - Device leak/failure

P Wilde - BCIS Autumn Meeting Bristol – 30th September 2005
Technical aspects of TASG (Bristol)
High quality imaging is essential for planning
Preliminary high resolution CT angio
3D reconstruction for assessment of anatomy and measurements
Evaluate vascular access
Aortograms during procedure in chosen projection

P Wilde - BCIS Autumn Meeting Bristol – 30th September 2005
Technical aspects of TASG (Bristol)
Catheter laboratory environment
General anaesthesia (blood pressure and heart rate control)
25F devices - surgical access (combined surgery/interventional team approach) Y-graft approach
Additional right radial catheter for check angios
Have CSF drainage as an available option

P Wilde - BCIS Autumn Meeting Bristol – 30th September 2005

P Wilde - BCIS Autumn Meeting Bristol – 30th September 2005

P Wilde - BCIS Autumn Meeting Bristol – 30th September 2005

P Wilde - BCIS Autumn Meeting Bristol – 30th September 2005

P Wilde - BCIS Autumn Meeting Bristol – 30th September 2005

P Wilde - BCIS Autumn Meeting Bristol – 30th September 2005

P Wilde - BCIS Autumn Meeting Bristol – 30th September 2005

P Wilde - BCIS Autumn Meeting Bristol – 30th September 2005
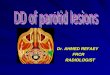
Case 1
BK
27 y Female
RTA
Severe injuries including multiple pelvic fractures in external fixation

P Wilde - BCIS Autumn Meeting Bristol – 30th September 2005

P Wilde - BCIS Autumn Meeting Bristol – 30th September 2005

P Wilde - BCIS Autumn Meeting Bristol – 30th September 2005

P Wilde - BCIS Autumn Meeting Bristol – 30th September 2005

P Wilde - BCIS Autumn Meeting Bristol – 30th September 2005

P Wilde - BCIS Autumn Meeting Bristol – 30th September 2005
BK follow up
Well and leading a normal life 1 year
later

P Wilde - BCIS Autumn Meeting Bristol – 30th September 2005
Case 2
AE
81 y Male
Mycotic aneurysm (salmonella) of descending thoracic aorta with haemoptysis and dysphagia
Previous CABG

P Wilde - BCIS Autumn Meeting Bristol – 30th September 2005

P Wilde - BCIS Autumn Meeting Bristol – 30th September 2005

P Wilde - BCIS Autumn Meeting Bristol – 30th September 2005

P Wilde - BCIS Autumn Meeting Bristol – 30th September 2005

P Wilde - BCIS Autumn Meeting Bristol – 30th September 2005

P Wilde - BCIS Autumn Meeting Bristol – 30th September 2005
AE follow up
Well and leading a normal life 2 years later (oral antibiotic
prophylaxis)

P Wilde - BCIS Autumn Meeting Bristol – 30th September 2005
Bristol Experience 2002-2005
11 patients (7 male)
Age 27-81 yr (mean 63)4 chronic aneurysm
3 type B dissection (2 Marfan)
2 traumatic rupture
1 haemorrhagic ulcer
1 mycotic aneurysm
1 failed deployment (vascular access)
No early mortality, 1 late mortality (9 mths ? cause)
CT follow up so far in 8, no endoleaks
1 transient paraplegia (treated CSF drainage)
1 transient renal failure (trash embolisation)

P Wilde - BCIS Autumn Meeting Bristol – 30th September 2005
What do we need to do this?
Most importantly a committed team who are prepared to work togetherRadiology and/or cardiology, cardiac surgery and/or vascular surgery, anaesthesia, cath lab team, operating theatre team
High quality imaging
Institutional commitmentFinancial support, clinical governance support (new techniques)
TimeTo learn the technique (visits etc.) To organise each case (small numbers, high complexity)
FacilitiesCath lab/ vascular angio lab (of operating theatre standard) or operating theatre (very high quality image intensifier)

P Wilde - BCIS Autumn Meeting Bristol – 30th September 2005
Should we be doing this?
Yes definitely
but…..
A lot of planning is required Protocols for indications and technique requiredGood access to high quality imagingFunding issues are substantial

P Wilde - BCIS Autumn Meeting Bristol – 30th September 2005
Call yourselves interventionists?This is a REAL stent!