-
8/9/2019 Carotid Artery Stenting Virtual Stenting 215
1/13
2014 Wichtig Publishing - ISSN 0391-3988
Int J Artif Organs ( 2014; :12) 928-93937
928
Feasibility ofa priorinumerical assessment ofplaque scaffolding
after carotid artery stentingin clinical routine: proof of
concept
Francesco Iannaccone1, Sander De Bock1, Matthieu De Beule1,2,
Frank Vermassen3, Isabelle Van Herzeele3,Pascal Verdonck1, Patrick
Segers1, Benedict Verhegghe1,2
1 IBiTech-bioMMeda, Ghent University, Ghent - Belgium2 FEops
bvba, Ghent - Belgium3 Department of Thoracic and Vascular Surgery,
Ghent University Hospital, Ghent - Belgium
ORIGINAL ARTICLE -Focus on: Modeling approaches for endovascular
devices
DOI: 10.5301/ijao.5000379
INTRODUCTION
Carotid artery stenting (CAS) is an alternative procedure
for the treatment of severely stenosed symptomatic or
asymptomatic carotid artery lesions (70%) in high-risk
patients. The procedure has a similar stroke, death, and
myocardial infarction rate as carotid endarterectomy (CEA)
(1, 2), although lower event rates have been reported for
CAS in younger patients (
-
8/9/2019 Carotid Artery Stenting Virtual Stenting 215
2/13
2014 Wichtig Publishing - ISSN 0391-3988 929
Iannaccone et al
thereby shifting the major events to post-procedural com-
plications (4) in well-selected patients.It has been suggested
that stroke after CAS may be caused
by embolization when the stent mesh is unable to ade-
quately confine the plaque (5). In 75% of all procedures,
stents are likely to obtain similar results. However,
accurate
screening and carotid stent choice is influenced mainly by
arterial anatomy and lesion morphology (7-9), suggesting
that the plaque scaffolding provided by the stent is one of
the key parameters to procedural success.
One of the requirements for carotid stent design is good
apposition to the vessel wall (10, 11) as the protruding
stent struts may induce (micro) thrombus formation by the
decreasing blood flow velocity (12, 13). The effect of in-
complete stent apposition (ISA) has been studied in coro-
nary arteries and appears to be a potential factor of late
stent thrombosis (14). Limited data is available about the
consequences of ISA on the clinical outcome of CAS (12),
leaving the associated risk of restenosis yet to be
clarified.
This post-procedural risk is, at present, not trivial to
assess
by imaging.
Mono and biplane angiography, currently the gold stan-
dard to assess CAS (15), is not an optimal technique for the
detection of stent apposition. Optical coherence tomog-
raphy (OCT) (16) or Intra-vascular ultrasound (IVUS) (17)have
been proven to be safe and effective in quantifying
stent malapposition and plaque prolapse (associated with
major adverse events) but they are not yet routinely used
in CAS.
The influence of stent design on the peri- and early post-
procedural neurological outcome is still an unsolved top-
ic, mostly due to the lack of data relating stent design to
the clinical outcome (5, 18-21). A retrospective analysis of
patients treated with various carotid stents in symptomatic
and asymptomatic carotid artery disease demonstrated
increased post-procedural event rates for the four open
cell stents and for one of the three closed cell stents (5),
confirming the findings of other studies (18, 22). When the
stents were sub-grouped according to the free cell area
(FCA), higher post-procedural event rates were correlated
with an increase of FCA especially in symptomatic patients,
who are known to have an increased risk for stroke peri-
operatively (23). However, criticism has been raised due to
possible bias and confounders (24-26), specifically because
no objective measurement of silent brain infarction (such as
diffusion-weighted magnetic resonance imaging, DW-MRI)
was performed. At the same time, however, other studies
have failed to demonstrate statistically significant
differenc-
es in stroke and death risk between patients treated
withopen/closed stent designs or grouped by FCA (19, 25, 26).
Still, questions remain, especially since the occurrence of
any stroke is uncertain (27, 28) and may have an impact
on the interpretation of the results (25). Moreover, open
cell stent design has also been associated with fewer new
DW-MRI lesions (26), although in this particular study,
unlike
the others (21), no embolic protection was used during the
procedure.
More recently a meta-analysis by Tadros et al (29) noted
that
symptomatic patients with favorable anatomy treated with a
closed cell design have fewer major adverse events, reopen-
ing the debate. We feel it is safe to state that geometrical
features of the device may play a role in CAS outcomes and
newer devices are effectively focusing on improved scaf-
folding capabilities (28). Scaffolding parameters have been
previously proposed on the free expanded configuration
(11), although the same device can have a different behavior
in situdepending on the anatomical site (7-9).
Technical tools able to predict stent apposition and its
mechanical behavior in the treated vessel are appealing,
and may be beneficial for procedural planning. Numerical
simulations can be helpful to optimize carotid stent design,
and have proven to be a valid predictive tool when testedin
vitro(30), and useful in studying the behavior of different
stent designs implanted in a single carotid model (31-34).
Nevertheless, to the authors knowledge, no in vivoCAS
validations have been previously reported.
The present work introduces a novel virtual,
patient-specific,
pre-operative environment to evaluate the feasibility of nu-
merical prediction for clinical outcomes after CAS, focusing
on plaque scaffolding. Mechanical simulations have been
coupled with novel analysis tools to quantify scaffolding
parametersin situ. Two real patient cases treated with the
Acculink stent (Abbott Vascular, Santa Clara, CA, USA) were
studied to proof the concept. Routine pre- and post-stenting
imaging were compared with the computer simulations to
validate the virtual operative procedure.
MATERIALS AND METHODS
Patient data
Two patient datasets (obtained after patients provided in-
formed consent for the processing of their datasets) were
-
8/9/2019 Carotid Artery Stenting Virtual Stenting 215
3/13
2014 Wichtig Publishing - ISSN 0391-3988930
Evaluation of plaque scaffolding after CAS
available for the study, referred to as patient A (male,
75 years old, 82% degree of stenosis in the internal
carotidartery, ICA) and patient B (female, 61 years, 79% degree
of stenosis in the ICA). Both asymptomatic patients were
treated via the transfemoral route using an embolic pro-
tection device (Emboshield NAV 6; Abbott Vascular, Santa
Clara, CA, USA). An Acculink stent was implanted by an
experienced team: tapered 7 10 40 mm for patient A
and tapered 7 10 30 mm for patient B. Pre-operative
computer tomography angiography (CTA) images were ac-
quired with a Siemens Somatom Sensation Cardiac scan-
ner with resolution of 0.37 0.37 1 mm for patient A and
Siemens Somatom Definition Flash scanner with resolution
of 0.54 0.54 3 mm for patient B (Siemens Healthcare,
Erlangen, Germany). Post-operative monoplane angiogra-
phy was acquired using a Philips AlluraXPer FD10 (Philips
Healthcare Imaging Systems, Andover, MA, USA).
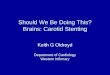
Vessel models
From the pre-operative CTA, geometries of the vessel lu-
men and of the calcified plaques were segmented (Fig. 1A)
using 3D Slicer software (35). Other tissues (such as soft
plaques and vessel wall) were not visible on CTA. To create
an approximate model of the vessel wall the following stepswere
taken:
1. the geometry of the calcified plaque and the vessel lu-
men were combined and manually corrected to create
an approximated shape of the healthy lumen before le-
sion development (Fig. 1B);
2. the actual lumen and calcified plaque were subtracted
from the geometry of the healthy lumen in order to ob-
tain the non calcified plaque geometries (Fig. 1B);
3. subsequently, the 3D triangulated models were gener-
ated for the diseased lumen, the plaques components,
and the healthy lumen;
4. the healthy lumen geometry was expanded to create
the outer vessel wall geometry; the radius of the ves-
sel, computed per node as distance of the healthy lu-
men to the centerline of the vessel (computed in vmtk
(36)), was increased by 30% in the normal direction to
the surface, a realistic value of the carotid artery wall
thickness (37).
Starting from the geometry of the real lumen and the re-
constructed outer wall, the 3D hexahedral mesh of the
vessel (Fig. 2) for the numerical solver was created using
IA_FEMesh (Finite Element Meshing Module), a meshing
tool embedded in 3D Slicer (38). The vessel was consid-
ered to be single-layered. The finite element analysis was
performed using brick elements with reduced integra-
tion (C3D8R in the Abaqus nomenclature) for both stent
devices and vessel geometries. The final meshes con-
sisted of 79 092 nodes and 35 256 elements for the stent
and of 12 848 nodes and 9477 elements for the vessel for
patient A, while the models of patient B counted 57 534
nodes and 25 680 elements for the stent and 11 000
nodes and 8038 elements for the vessel. The density of
the meshes was increased at critical locations (crowns
and regions with higher curvature of the stent struts and
the stent landing zone of the vessels). The sections of the
Fig. 1 -Work-flow of the vessel model reconstruction:
segmentation
of the vessel lumen and calcified plaque (A); manual adjustment
ofthe lumen shape to create the assumed healthy lumen and
retrieve
the subtracted non-calcified lesion depicted in blue(B);
expansion
of the healthy lumen to create the outer vessel wall (C).
Fig. 2 -Reconstructed vessel geometries of the 2 patients.
Calcifi-
cations are depicted in whiteand the assumed hypo cellular
plaque
in yellow.
-
8/9/2019 Carotid Artery Stenting Virtual Stenting 215
4/13
2014 Wichtig Publishing - ISSN 0391-3988 931
Iannaccone et al
stents counted 2 2 elements and we used 3 elements
along the thickness of the vessel wall. Displacement val-ues
were used to check convergence of the results. Since
doubling the number of elements along strut thickness
and width and the vessel wall resulted in similar displace-
ment values, the coarser meshes were used to reduce
the computational cost. Note that an accurate stress
analysis which was not the goal of this work would re-
quire denser meshes to ensure reliability of the real stress
state, especially along the width of the device. Similar
mesh densities for the carotid arteries were previously
reported to have sufficient detail to describe stresses in
the wall (33).
The vessel geometry was used as reconstructed from the
scans, without including pre-stress and pre-stretch condi-
tions. No physiological pressure was applied to the model.
To compensate for these limitations, we created an en-
gineering equivalent of the vessel material to describe the
in vivodisplacements which includes the effects of thein
vivo
boundary conditions of the vessel (pre-pressurization, pre-
stretch, interactions with the surrounding tissues, etc).
This
approach neglects the real stress state of the material but
simplifies the simulation by allowing the implantation in an
unloaded vessel configuration.
We used a stress-strain curve for the arterial wall publishedin
a previous study (39). Then we scaled the curve to cali-
brate the actual deformations induced by the stent, and
coefficients of several hyperelastic constitutive models
were fit to the material response curve using the Evaluate
tool of the Abaqus software (Simulia Corp, Providence, RI,
USA) material menu.
Mainly due to stability concerns, we opted for a third
order Ogden hyperelastic material model formulation,
whose general strain energy potential Uas a function of
the deviatoric principal stretches 1, 2 and 3 is given by:
( )= 2 + + 3=1
2 1 2 3
Ui
N
i
i
i ii
where N,iand
iare material parameters.
The original stress-strain curve was scaled along the
stretch axis to obtain a stiffer material at the beginning
of
the curve (to faster reach higher stresses in the model) in
order to consider the effects of the pressurizedin vivocon-
dition. The scaling also provides stiffer behavior at higher
stretches to account for the interaction with the surround-
ing structures. The scaled curve does not describe the
real behavior of the vessel but only an equivalent material
that can mimic the combined effects of the in vivopres-
surization, pre-stretch, and the stiffening provided by
thesurrounding tissue. A scaling factor of 0.40 was found to
describe the correct displacements.
In order to account for the different plaque components,
the elements of the vessel mesh located inside the seg-
mented plaque surfaces were selected. The material prop-
erties of the plaques were taken from Loree et al (40) and
fit using a first-order, hyperelastic Ogden model using the
previously mentioned Abaqus tool. To roughly emulate the
rupture of the plaque, we assumed a constant plastic be-
havior at the reported values of plaque rupture. All
material
parameters are summarized in Table I.
Stent models
To retrieve the basic cell geometry, the stent models were
built starting from a micro-CT scan of a 8 20 mm Acculink
straight design. After segmentation of the stent geometry
(in 3D Slicer), a parametric hexahedral stent model was
built
in pyFormex (41) using the approach described in De Bock
et al (42). The parametric model was adapted to create the
tapered stents (7 10 30 mm and 7 10 40 mm) shown
in Figure 3. Stent thickness and width were assumed equal
to the ones of the available sample, measured in 3D Slicer(0.17
mm and 0.16 mm, respectively).
The stress-strain relationship of the nitinol alloy (Ti55.8
wt% Ni) was retrieved from the literature (43) and defined
using an embedded user subroutine in Abaqus based on
the model of Auricchio et al (44). Symmetry in compres-
sion was assumed (Tab. I). All phases of the device ma-
nipulation were assumed to occur at body temperature
of 37C.
Virtual stent deployment procedure
The numerical simulation involved non-linearity due to
the material properties, large deformations, and complex
contact problems of a real stent implantation; a
quasi-static
analysis was performed using the commercial finite element
solver Abaqus/Explicit. The general contact algorithm was
used to handle the interactions, assuming a friction value
of
0.05 for all the contact surfaces (34).
The stent placement was emulated imposing analytical
displacements to a cylindrical catheter (4-node surface el-
ements with reduced integration - SFM3D4R) by a VDISP
subroutine to drive crimping, smooth bending along the
-
8/9/2019 Carotid Artery Stenting Virtual Stenting 215
5/13
2014 Wichtig Publishing - ISSN 0391-3988932
Evaluation of plaque scaffolding after CAS
centerline of the vessel and deployment of the stent at the
arterial lesion, as previously described (42). A similar
cylin-
drical geometry was used to enlarge the vessels, to emu-
late balloon pre-dilation of the vessel to ensure the device
insertion in the vascular cavity.
Validation
To validate the numerical results we compared the post-
procedural monoplane angiographic images and the virtual
implantation both qualitatively (visual assessment) and
quantitatively measuring the relative errors %
between the
diameters of the stented location Dsimulationwith respect tothe
clinical data D
in vivomeasured as :
=
D D
D100%
simulation in vivo
in vivo
The monoplane angiograms were previously calibrated
from the catheter size used during CAS. The numerical
results were imported in pyFormex to extract the ves-
sel lumen. The angle of view of the deformed model was
manually adjusted in the viewer to match the position of
thein vivodataset. In vivoand simulated implantation im-
ages were then calibrated to match the diameter of the
non-stented vessel portions.
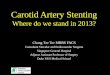
Post-processing for evaluation of scaffolding
Three different parameters were measured to evaluate the
scaffolding of the stent, i.e. the support given by the
stent
to the arterial lesion, as schematically depicted in Figure
4:
1. Incomplete strut apposition (ISA) to the vessel wall,
computed as the distance from the external stent sur-
face nodes to the closest vessel surface element. As
a descriptive parameter of ISA, the percentage area of
TABLE I -MATERIAL PARAMETERS FOR THE CALIBRATED VESSEL WALL, THE
FIT PLAQUE COMPONENTS, AND THENITINOL STENT
Arter ial material parameters Source
1
(kPa)
1
2
(kPa)
2
3
(kPa)
3
Calibrated
healthy wall
III order Ogden
(Hyperelastic)
-14790 -2.14 10122 0.51 507 -7.79
(kPa) Plasticity
threshold
(kPa)
Hypocellular
plaque
I order Ogden
(Hyperelastic)
21.8 24.72 400 Loree et al,
1994 (40)
Calcifiedplaque
I order Ogden(Hyperelastic)
72.34 25.00 400 Loree et al,1994 (40)
Device material parameters
Ea(kPa) v
aE
m
(kPa)
vm
L
LS
(kPa)
LE
(kPa)
TO
US
(kPa)
UE
(kPa)
CLS
(kPa)
LV
Nitinol 41000 0.3 23333 0.3 0.0437 450 520 37 210 130 450 0.0437
Gong et al,
2004 (43)
Fig. 3 -Implanted tapered Acculink stent model (7 10 40 mm
and
7 10 30 mm).
-
8/9/2019 Carotid Artery Stenting Virtual Stenting 215
6/13
2014 Wichtig Publishing - ISSN 0391-3988 933
Iannaccone et al
stent struts within a threshold distance of the vessel
wall relative to the total stent area was computed. The
threshold of 0.2 mm was chosen to identify most critical
areas undergoing ISA (16).
2. Stent cells areas of the implanted stent. The cell area
was computed from the minimal surfaces that could fill
the FCAs. The surface was created on the undeformed
stent, triangulating the cell nodes and keeping trace of
the connectivity of each triangle. Using the connectivitytable,
the surface was then deformed according to the
new position of the cell nodes after the implant.
3. Largest fitting sphere (LFS) going through the FCA. The
surface fitting the FCA was seeded with an adequate
number of points (determined after convergence es-
timation). The minimum distance of each point to the
free edges of the cell was computed. The point (center
of the sphere) with the largest distance (radius of the
sphere) was then selected.
RESULTS AND DISCUSSION
Validation
The numerical simulations were able to emulate the over-
all shape of the implanted stents retrieved from the clini-
cal monoplane angiographic images (Figs. 5 and 6). Table II
summarizes the relative error of the lumen diameters for the
indicated sections. Mean relative errors of the lumen diam-
eters were 5.31 8.05% for patient A and 4.12 9.84% for
patient B.
Both the qualitative and quantitative comparison between
post-procedural angiography and the projected image of
the virtually implanted stent showed overall good agree-
ment, capturing the main features of the deformed stent
shape. Patient A showed a somewhat better visual match
Fig. 4 - Schematic description of the evaluated scaffolding
pa-
rameters.
Fig. 5 -Qualitative comparison of the implanted stent
configura-
tion for patient A, showing the clinical and numerical results.
From
left to right:angiography of stented lumen, numerical results,
and
X-ray of the implanted stent.Red arrowsindicate the location of
the
measured diameters.
Fig. 6 -Qualitative comparison of the implanted stent
configuration
for patient B, showing the clinical and numerical results. From
left
to right: angiography of stented lumen, numerical results, and
X-
ray of the implanted stent. Red arrows indicate the location of
the
measured diameters.
-
8/9/2019 Carotid Artery Stenting Virtual Stenting 215
7/13
2014 Wichtig Publishing - ISSN 0391-3988934
Evaluation of plaque scaffolding after CAS
of the stent shape compared to patient B, even though
average diameter errors were similar in both cases.
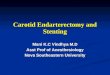
Scaffolding
The results of the scaffolding evaluation are summarized in
Table III and Figures 7, 8, and 9.
As it can be observed in Figure 7, the open-cell design
showed ISA to the vessel wall in the most tortuous and ana-
tomically complex regions. The percentage of stent struts
area with ISA was markedly higher for patient A (8.8% vs.
2.4%). Note, however, that results can be misleading due to
the fact that patient B had a completely occluded external
carotid artery and patient A had a larger part of the stent
deployed at the bifurcation region where there was a higher
mismatch between stent and vessel diameter, consequently
leading to a higher area of ISA. Both cases showed good
apposition to the ICA. For patient B the sections at the
bifur-
cation and at the ICA were similar, giving better apposition
to the vessel wall, also due to a smaller curvature of the
ves-
sel. At the inner curvature of the vessel wall, ISA was
noted
TABLE II -ABSOLUTE VALUES OF THE DIAMETERS OF THE STENTED VESSEL
AND THE RELATIVE ERROR BETWEEN THENUMERICAL SIMULATION AND THE
CLINICAL DATA, COMPUTED AT 9 DIFFERENT SECTIONS
Diameters Section Average
S1 S2 S3 S4 S5 S6 S7 S8 S9
Patient A Numerical (mm) 7.38 8.59 4.82 4.20 4.59 3.71 4.14 4.42
4.30
Clinical (mm) 7.44 8.12 3.99 3.78 4.17 3.94 3.94 4.30 4.37
% -0.85 5.82 21.06 11.01 10.15 -5.73 5.20 2.79 -1.61 5.31
8.05
Patient B Numerical (mm) 6.45 5.71 5.80 5.97 6.37 5.62 5.63 6.29
5.76
Clinical (mm) 6.45 6.18 6.54 5.89 5.30 4.96 5.21 5.96 5.37
% 0.00 -7.62 -11.25 1.26 20.28 13.33 8.10 5.55 7.40 4.12
9.27
TABLE III - AVERAGE RESULTS OF INCOMPLETE STRUTAPPOSITION, FREE
CELL AREAS, AND THERADIUS OF THE LARGEST FITTING SPHERE
Global scaffolding parameters
Model Stent area
with ISA (%)
FCAs (mm2) Radius of
LFSs (mm)
Patient A 8.8% 7.69 3.05 0.45 0.11
Patient B 2.4% 7.59 2.80 0.46 0.11
Fig. 7 - Incomplete strut apposition (struts colored in red) of
the
implanted stents. Threshold was set at 0.2 mm. The
arrowsindicate
the regions where the fish scaling effect occurs.
Fig. 8 -Free cell areas of the implanted stents (in mm2).
-
8/9/2019 Carotid Artery Stenting Virtual Stenting 215
8/13
2014 Wichtig Publishing - ISSN 0391-3988 935
Iannaccone et al
in both cases, also showing the fish scaling effect that is
typical for stents with an open-cell design. This effect was
very apparent in patient A at the bifurcation (Fig. 7).
Distal
ISA, which was reported previously (12), occurred in patient
B, while proximal ISA occurred in both patients.
The analysis of the deformed free cell area (FCA) showed
that the target diameter of the vessel highly influences
scaf-folding provided by the device. In fact, patient A, with a
smaller ICA diameter resulted in smaller FCAs compared to
patient B with a larger ICA diameter (Fig. 8). Also, in
patient
B, the cross-sectional change of the vessel was less pro-
nounced, leading to a more uniform cell shape deformation.
The largest fitting spheres (LFSs, Fig. 9) did not pace the
FCAs distribution. Maximum values of FCAs do not neces-
sarily correspond to higher values of the LFSs. For patient
B,
the FCAs were similar at the bifurcation and at the mid part
of the stent, while the LFSs were more inhomogeneous,
ranging from 0.36 mm to 0.7 mm. High values of LFSs
were found at the ICA, mainly concerning the cells appos-
ing at the concave region of the vessel. Similar consider-
ations can be made for patient A. The chosen stent, which
corresponds to the diameter requirements of the distal
ICA, was undersized for the bifurcation diameter result-
ing in an under-expansion of the stent, leading to a free
expanded-like configuration with higher FCAs and LFSs.
It can be noticed that high values of LFCs were also found
at the distal location of the ICA, again at a concave part
of
the vessel although the FCA is small. This seems reason-
able when thinking of a bending bar: at the inner curvature,
stent struts get closer, while at outer curvatures they wid-
en. The values were also influenced by ISA. In fact, if thecell
opens in the radial directions, due to fish scaling,
this resulted in higher LFSs compared to a more planar
configuration, as indicated by the green arrow in Figure 9.
As highlighted in our study, the fish scaling effect is
present
even with moderate tortuosity at the convex lumen regions,
which will clearly be more accentuated with a more com-
plex lumen shape. It has been speculated that fish scaling
may contribute to restenosis and stent fracture (10). The
price for the absence of shortening, optimal conformability
and flexibility of the open-cell design leads to plaque
scaf-
folding with lower plaque coverage, possibly promoting
plaque protrusion through the interstices of the stent
struts,
allowing plaque material to embolize after implantation
(45).
Nevertheless, in the analyzed patients due to a straight,
post-stented vessel geometry and adequate sizing, the
stent seems to offer a good scaffolding of the lesion.
Another variable to take into account may be device over-
sizing. Even though manufacturers provide guidelines, the
choice for a certain degree of oversizing still depends on
operators preference and experience and on the high vari-
ability of the carotid anatomy. In patient A the stent had a
larger degree of oversizing, resulting in a higher closure
of
the stent cells at the ICA, offering more lesion protectionand
increasing surface covering. Oversizing may, however,
lead to increased tension on the vessel wall, consequently
causing neointimal hyperplasia and restenosis (46).
In a previous finite element study, Conti et al (31) con-
structed a single atherosclerotic carotid model which was
virtually treated with four different types of stents
(includ-
ing Acculink); they then analyzed the FCAs. Likewise, the
authors found a higher reduction of the cell area at the
mid-
dle location as in patient A. Further comparisons are not
possible due to the different anatomy, the lower degree of
stenosis, and different stent positioning.
In the same study, it was highlighted that LFSs in the free
expanded configuration (as previously described (11)) can-
not capture differences in stent designs. Nevertheless, it
is
our opinion that LFSs in the deformed configuration can
be relevant for measuring the maximum plaque particles
potentially protruding through the stent struts, especially
when similar devices are compared under different condi-
tions. LFSs may improve and refine the FCA analysis. In
fact, cells with similar FCAs may result in various deformed
shapes that influence the LFSs (see the ICA segment
in Figs. 8 and 9 for both patients), suggesting that both
Fig. 9 -Radius of the largest fitting spheres of the implanted
stents(in mm).Red arrows show the concave regions of the vessel,
which
are associated with relatively large spheres compared to the
convex
regions. Thegreen arrowshows how the fish scaling can
influence
the dimensions of the spheres.
-
8/9/2019 Carotid Artery Stenting Virtual Stenting 215
9/13
2014 Wichtig Publishing - ISSN 0391-3988936
Evaluation of plaque scaffolding after CAS
measures are complementary scaffolding parameters.
LFSs may be regarded as a measure of how opposite strutsof a
single cell are tied, i.e. how the cell is assembled.
An obvious observation from our results is that the speci-
ficity of the lesion influences stent behavior and its scaf-
folding capability. CAS success has been often thought to
be influenced by stent design, i.e. open versus closed stent
design, but this may be too basic, as previously suggested
(44). To refine the discrimination, other studies refer to
FCA
in the free expanded configuration (more than open versus
closed design) to be an important parameter in CAS failure
(5). However, other stent characteristics, such as conform-
ability in angulated arteries and low radial force, play a
role
in selecting the appropriate stent (11, 24, 45, 47).
Measurements of the maximum free cell area and the cell
pore diameter of the free expanded stent previously pro-
posed (11) can be misleading, as the deformed configura-
tion of the deployed stent in a tortuous vessel is
neglected.
Our approach may be more suitable to analyze cell support
at the lesion. Our results also suggest that global values
may not be adequate because they can mask zones at
higher risk for embolization (i.e., at the lipid plaque
loca-
tion). According to Table III, the mean values of FCAs and
LFSs do not show any difference between the two pa-
tients, even though the two stents behaved very differently.On
the other hand, a visual evaluation of the scaffolding
parameters of the virtual implantation allows a direct as-
sessment of the possible CAS outcome scenarios.
A recent study, using a strategy that is similar to ours,
com-
pared vessel changes after virtual balloon expanded coro-
nary stenting with clinical images from two patients (48).
They were able to reproduce the general geometrical fea-
tures of the stented vessel and performed both a qualitative
validation (comparing the stented vessel lumen of conven-
tional angiographic images and the numerical results) and
a quantitative analysis, measuring the straightening of the
vessel in one patient for whom CTA data were available. Al-
though their results suggest the feasibility of their
numerical
approach, the differences in the interventional procedure
along with the vascular district and parameters used for the
validation make a direct comparison with the results of our
work difficult.
Limitations
The main limitations of our study are related to the imaging
techniques used to retrieve pre- and post-operative data.
The routine pre-operative CTA scans do not provide ac-
curate information about the vessel wall and, more impor-tantly,
about soft plaques. Validation of the results should
ideally be based on imaging techniques that allow a direct
comparison with the post-operative 3D stent configura-
tion and/or are able to quantify the ISA, which cannot be
measured by conventional angiography. Inadequate CTA
resolutions can mask abrupt changes of the lesion, thereby
introducing inaccuracies into the pre-stented vessel geom-
etry, which may be amplified by the smoothing algorithms
to clean the surface for model meshing. Also, the artery
is acquired by CTA at a certain phase of the cardiac cycle,
which may be different during post-procedural imaging
due to a different pressure load. The position of the neck
also changes the carotid configuration (11, 49) potentially
raising additional mismatches between the numerical and
the angiographic configurations.
The difficulties that may be encountered in linking pre- and
post-treatment imaging data in this hybrid angio suite can
be shown by some of the pre-operative sequences of pa-
tient B, who exhibited less accurate validation. Figure 10A
shows how displacements of the artery (due either to patient
movements, heart rate or blood pressure changes) during
the injection of the contrast agent modify the curvature and
configuration of the pre-stented vessel. Rigorous validationthus
requires strict protocols. Ideally, an identical position of
the patient should be used during the procedure with stable
hemodynamics. We believe that these factors contribute to
the initial mismatch between pre- and post-operative data
as displayed in Figure 10. Moreover, the angiographic pic-
tures show irregularities and ulceration of the plaque
anato-
my that could not be detected by the CTA scans due to the
low resolution in the axial direction (arrows in Fig. 10).
Although the level of complexity in the simulations is high,
there are still important simplifications in thein
vivoloading
(ignoring blood pressure, pre-stretching and pre-stresses)
and on the lesion morphology due to routine CTA inability to
recognize different tissues (lack of ulceration, thrombus or
fibrous cap, assumptions of vessel thickness, single-layered
vessel). A multi-detector scanner and specific reconstruc-
tion algorithms may improve the lesion imaging (50).
These factors, together with the high variability of the
biolog-
ical materials, complicate a correct per-patient calibration
of
anisotropic material models. An isotropic material model was
used in this study, which might not adequately describe the
real biomechanics of the vascular tissue (51). We needed to
stiffen the artery by scaling the original arterial
stress-strain
-
8/9/2019 Carotid Artery Stenting Virtual Stenting 215
10/13
2014 Wichtig Publishing - ISSN 0391-3988 937
Iannaccone et al
Registry first 2,001 patients. Catheter Cardiovasc Interv.
2009;73(2):129-136.
2. Brott TG, Hobson RW II, Howard G, et al; CREST Investiga-
tors. Stenting versus endarterectomy for treatment of carot-
id-artery stenosis. N Engl J Med. 2010;363(1):11-23.
curve in order to achieve better matching with the in vivo
data. This is in line with the results of Auricchio et al (51)
who
found larger vessel deformation with the mentioned model
when compared with other literature data. One might specu-
late that when dealing within vivostructures even accurate
ex vivoexperimental material description may underestimatethe
real stiffness of the treated vessel if the in vivo loading
conditions and the interaction with surrounding structures
are neglected. To overcome the latter problem, alternatively
to our approach, spring elements might be considered to
describe these interactions as previously suggested (52).
CONCLUSIONS
In the present study we used finite element computer mod-
el simulations to imitate CAS procedures, and applied au-
tomatic tools to quantify vessel scaffolding in two
patients.
Results showed the feasibility of the proposed method
with an overestimation of the predicted stented lumen di-
ameter of 5.31 8.05% and 4.12 9.84% for the two pa-
tients compared to the clinical outcome. The quantitative
measurements of the incomplete stent apposition, free cellareas,
and largest fitting spheres highlighted the variability
of device behavior in relation to the target lesion. In gen-
eral, the free cell area depended on the target diameter and
oversizing, while the largest fitting spheres and apposition
values were influenced by the local concavity and convex-
ity of the vessel region.
The proposed method, pending a more accurate 3Din vivo
validation with a larger number of datasets, may be an ad-
ditional tool for cardiovascular interventionists for a
proper
selection of stent design and more accurate positioning
in complex anatomies. This would help to reduce post-
procedural strokes by better assessinga priorithe poten-
tial risk of embolization.
ACKNOWLEDGEMENTS
The authors gratefully acknowledge P. Mortier, PhD, and G.
De Santis, PhD, for their valuable support in the modeling
pro-
cess and results evaluation, and B. Vandeghinste for sharing
his expertise in medical imaging.
Financial Support: This study was financially supported by
the
Research Foundation Flanders (FWO grant 3G06591) and by
GhentUniversity (grant BOF10/GOA/005).
Conflict of Interest:The authors have no financial disclosures.
M. De
Beule and B. Verhegghe are shareholders of FEops, an
engineering
consultancy spin-off from Ghent University, and have served as
con-
sultants for several medical device companies.
Meeting Presentations:Part of this work was presented at the
11th
International Symposium on Computer Methods in Biomechanics
and
Biomedical Engineering held in Salt Lake City, Utah, USA, in an
oral
presentation given on April 6, 2013. A poster presentation was
given
on June 12, 2013 at the Multidisciplinary European
Endovascular
Therapy conference in Rome, Italy.
Address for correspondence:
Francesco Iannaccone
Universiteit Gent IbiTech
De Pintelaan 185, blok B/5
B-9000 Gent, Belgium
[email protected]
Fig. 10 -Mismatch of the pre-operative condition between
conven-
tional angiography and the reconstructed model. Arterial
configuration
changes during contrast agent injection (A). The border (in
red)of thevessel from angiography at a certain instant is overlaid
on the angiogra-
phy at a subsequent instant clearly showing the modification of
the lu-
men shape due to loading factors. At the bottom the arterial
geometry
from the CTA is depicted (B). Thered arrowsindicate the
irregularities
not detected in the CTA (B), which are visible in the
angiography (A).
REFERENCES
1. Massop D, Dave R, Metzger C, et al; SAPPHIRE Worldwide
Investigators. Stenting and angioplasty with protection in
pa-
tients at high-risk for endarterectomy: SAPPHIRE Worldwide
-
8/9/2019 Carotid Artery Stenting Virtual Stenting 215
11/13
2014 Wichtig Publishing - ISSN 0391-3988938
Evaluation of plaque scaffolding after CAS
3. White CJ. Carotid artery stent placement. JACC Cardiovasc
Interv. 2010;3(5):467-474.
4. Cremonesi A, Setacci C, Manetti R, et al. Carotid
angioplas-
ty and stenting: lesion related treatment strategies.
EuroIn-
tervention. 2005;1(3):289-295.
5. Bosiers M, de Donato G, Deloose K, et al. Does free cell
area
influence the outcome in carotid artery stenting? Eur J Vasc
Endovasc Surg. 2007;33(2):135-141.
6. Gray WA, Rosenfield KA, Jaff MR, Chaturvedi S, Peng L,
Verta
P; CAPTURE 2 Investigators and Executive Committee. In-
fluence of site and operator characteristics on carotid
artery
stent outcomes: analysis of the CAPTURE 2 (Carotid ACCU-
LINK/ACCUNET Post Approval Trial to Uncover Rare Events)
clinical study. JACC Cardiovasc Interv. 2011;4(2):235-246.
7. Maleux G, Nevelsteen A. Carotid artery stenting: which
stent
for which lesion? Acta Chir Belg. 2002;102(6):430-434.8.
Mller-Hlsbeck S, Preuss H, Elhft H. CAS: which stent
for which lesion. J Cardiovasc Surg (Torino). 2009;50(6):
767-772.
9. Bosiers M, Deloose K, Verbist J, Peeters P. Carotid
artery
stenting: which stent for which lesion? Vascular.
2005;13(4):
205-210.
10. Siewiorek GM, Finol EA, Wholey MH. Clinical significance
and technical assessment of stent cell geometry in carotid
artery stenting. J Endovasc Ther. 2009;16(2):178-188.
11. Mller-Hlsbeck S, Schfer PJ, Charalambous N, Schaffner
SR, Heller M, Jahnke T. Comparison of carotid stents: an
in-vitro experiment focusing on stent design. J Endovasc
Ther. 2009;16(2):168-177.12. Onizuka M, Kazekawa K, Nagata S, et
al. The significance of
incomplete stent apposition in patients undergoing stenting
of internal carotid artery stenosis. AJNR Am J Neuroradiol.
2006;27(7):1505-1507.
13. Ohyama M, Mizushige K, Ohyama H, et al. Carotid turbu-
lent flow observed by convergent color Doppler flowmetry
in silent cerebral infarction. Int J Cardiovasc Imaging.
2002;
18(2):119-124.
14. Ozaki Y, Okumura M, Ismail TF, et al. The fate of
incomplete
stent apposition with drug-eluting stents: an optical coher-
ence tomography-based natural history study. Eur Heart J.
2010;31(12):1470-1476.
15. North American Symptomatic Carotid Endarterectomy
TrialCollaborators. Beneficial effect of carotid endarterectomy
in
symptomatic patients with high-grade carotid stenosis. N
Engl J Med. 1991;325(7):445-453.
16. de Donato G, Setacci F, Sirignano P, Galzerano G,
Cappelli
A, Setacci C. Optical coherence tomography after carotid
stenting: rate of stent malapposition, plaque prolapse and
fibrous cap rupture according to stent design. Eur J Vasc
Endovasc Surg. 2013;45(6):579-587.
17. Clark DJ, Lessio S, ODonoghue M, Schainfeld R,
Rosenfield
K. Safety and utility of intravascular ultrasound-guided ca-
rotid artery stenting. Catheter Cardiovasc Interv.
2004;63(3):
355-362.
18. Jansen O, Fiehler J, Hartmann M, Brckmann H. Protec-
tion or nonprotection in carotid stent angioplasty: the
influ-
ence of interventional techniques on outcome data from the
SPACE Trial. Stroke. 2009;40(3):841-846.
19. Schillinger M, Gschwendtner M, Reimers B, et al. Does
ca-
rotid stent cell design matter? Stroke. 2008;39(3):905-909.
20. Tadros RO, Spyris CT, Vouyouka AG, et al. Comparing the
embolic potential of open and closed cell stents during
carotid angioplasty and stenting. J Vasc Surg. 2012;56(1):
89-95.
21. Park KY, Kim DI, Kim BM, et al. Incidence of embolism
asso-
ciated with carotid artery stenting: open-cell versus
closed-
cell stents. J Neurosurg. 2013;119(3):642-647.
22. Hart JP, Peeters P, Verbist J, Deloose K, Bosiers M. Do
de-
vice characteristics impact outcome in carotid artery stent-
ing? J Vasc Surg. 2006;44(4):725-730.23. Biasi GM, Froio A,
Diethrich EB, et al. Carotid plaque echo-
lucency increases the risk of stroke in carotid stenting:
the
Imaging in Carotid Angioplasty and Risk of Stroke (ICAROS)
study. Circulation. 2004;110(6):756-762.
24. de Vries JP. Comments regarding Comparison of stent free
cell area and cerebral lesions after unprotected carotid
artery
stent placement. Eur J Vasc Endovasc Surg. 2012;43(1):15.
25. Jim J, Rubin BG, Landis GS, Kenwood CT, Siami FS, Sicard
GA; SVS Outcomes Committee. Society for Vascular Surgery
Vascular Registry evaluation of stent cell design on carotid
artery stenting outcomes. J Vasc Surg. 2011;54(1):71-79.
26. Grunwald IQ, Reith W, Karp K, et al. Comparison of stent
free cell area and cerebral lesions after unprotected ca-rotid
artery stent placement. Eur J Vasc Endovasc Surg.
2012;43(1):10-14.
27. Cremonesi A, Setacci C, Castriota F, Valgimigli M.
Carotid
stent cell design: lack of benefit or lack of evidence?
Stroke.
2008;39(8):e130-e130.
28. Setacci C, de Donato G, Bosiers M; Belgium-Italian
Carotid
Registry. Two different studies on carotid stent cell design
importance, or are we just saying the same thing? Stroke.
2008;39(8):e129-e129.
29. Tadros RO, Malik RK, Vouyouka AG, Ellozy SH, Marin ML,
Faries PL. A systematic review of carotid stent design and
selection: strategies to optimize procedural outcomes.
Inter-
ventional Cardiology. 2013;5(2):203-211.30. Conti M, Van Loo D,
Auricchio F, et al. Impact of carotid stent
cell design on vessel scaffolding: a case study comparing
experimental investigation and numerical simulations. J En-
dovasc Ther. 2011;18(3):397-406.
31. Auricchio F, Conti M, Ferraro M., Reali A. Evaluation of
ca-
rotid stent scaffolding through patient-specific finite
element
analysis. Int J Numer Method Biomed Eng. 2012:28(10):
1043-1055.
32. De Santis G, Conti M, Trachet B, et al. Haemodynamic im-
pact of stent-vessel (mal)apposition following carotid
artery
stenting: mind the gaps! Comput Methods Biomech Biomed
Engin. 2013;16(6):648-659.
-
8/9/2019 Carotid Artery Stenting Virtual Stenting 215
12/13
2014 Wichtig Publishing - ISSN 0391-3988 939
Iannaccone et al
33. Auricchio F, Conti M, De Beule M, De Santis G, Verhegghe
B. Carotid artery stenting simulation: from patient-specific
images to finite element analysis. Med Eng Phys. 2011;33(3):
281-289.
34. Wu W, Qi M, Liu X-P, Yang D-Z, Wang W-Q. Delivery and
re-
lease of nitinol stent in carotid artery and their interactions:
a
finite element analysis. J Biomech. 2007;40(13):3034-3040.
35. Fedorov A, Beichel R, Kalpathy-Cramer J, et al. 3D
Slicer
as an Image Computing Platform for the Quantitative Imag-
ing Network. Magn Reson Imaging. 2012;30(9):1323-1341.
http://www.slicer.org. Accessed December 22, 2014.
36. vmtk - the Vascular Modeling Toolkit.
http://www.vmtk.org.
Accessed December 22, 2014.
37. Sommer G, Regitnig P, Kltringer L, Holzapfel GA. Biaxial
mechanical properties of intact and layer-dissected human
ca-
rotid arteries at physiological and supraphysiological
loadings.Am J Physiol Heart Circ Physiol.
2010;298(3):H898-H912.
38. Grosland NM, Shivanna KH, Magnotta VA, et al. IA-FEMesh:
an open-source, interactive, multiblock approach to ana-
tomic finite element model development. Comput Methods
Programs Biomed. 2009;94(1):96-107.
39. Creane A, Maher E, Sultan S, Hynes N, Kelly DJ, Lally C.
Fi-
nite element modelling of diseased carotid bifurcations gen-
erated fromin vivocomputerised tomographic angiography.
Comput Biol Med. 2010;40(4):419-429.
40. Loree HM, Grodzinsky AJ, Park SY, Gibson LJ, Lee RT.
Static
circumferential tangential modulus of human atherosclerotic
tissue. J Biomech. 1994;27(2):195-204.
41. pyFormex. http://www.nongnu.org/pyformex/. AccessedDecember
22, 2014.
42. De Bock S, Iannaccone F, De Santis G, et al. Our
capricious
vessels: The influence of stent design and vessel geometry
on the mechanics of intracranial aneurysm stent deploy-
ment. J Biomech. 2012;45(8):1353-1359.
43. Gong P, Pelton AR. Finite element analysis on nitinol
medi-
cal applications. International Mechanical Engineering Con-
gress and Exposition. 2002;53:1-2.
44. Auricchio F, Taylor RL, Lubliner J. Shape-memory alloys:
mac-
romodelling and numerical simulations of the superelastic
behavior. Comput Methods Appl Mech Eng. 1997;146(3-4):
281-312.
45. Castriota F, Liso A, Biamino G, Cremonesi A. Technical
Evo-
lution of Carotid Stents. Interventional Cardiology.
2008;3(1):
74-78.
46. Timmins LH, Miller MW, Clubb FJ Jr, Moore JE Jr.
Increased
artery wall stress post-stenting leads to greater intimal
thick-
ening. Lab Invest. 2011;91(6):955-967.
47. Siewiorek GM, Finol EA, Wholey MH. Clinical significance
and technical assessment of stent cell geometry in carotid
artery stenting. J Endovasc Ther. 2009;16(2):178-188.48.
Morlacchi S, Colleoni SG, Crdenes R, et al. Patient-specific
simulations of stenting procedures in coronary bifurcations:
two clinical cases. Med Eng Phys. 2013;35(9):1272-1281.
49. Riedel C, Mller-Hlsbeck S, Heller M. Quantitative
Analyse
physiologischer Deformationen der Karotiden auf der Basis
von 3D-TOF-MRA -Daten [in German]. Fortschr Rntgenstr.
2006;1:178-VO_308_5.
50. Vukadinovic D, van Walsum T, Manniesing R, et al.
Segmen-
tation of the outer vessel wall of the common carotid artery
in CTA. IEEE Trans Med Imaging. 2010;29(1):65-76.
51. Auricchio F, Conti M, Ferrara A, Morganti S, Reali A.
Patient-
specific finite element analysis of carotid artery stenting:
a
focus on vessel modeling. Int J Numer Method Biomed
Eng.2013;29(6):645-664.
52. Pericevic I, Lally C, Toner D, Kelly DJ. The influence
of
plaque composition on underlying arterial wall stress dur-
ing stent expansion: the case for lesion-specific stents.
Med
Eng Phys. 2009;31(4):428-433.
-
8/9/2019 Carotid Artery Stenting Virtual Stenting 215
13/13
C o p y r i g h t o f I n t e r n a t i o n a l J o u r n a l o
f A r t i f i c i a l O r g a n s i s t h e p r o p e r t y o f W i
c h t i g I n t e r n a t i o n a l
L i m i t e d a n d i t s c o n t e n t m a y n o t b e c o p i
e d o r e m a i l e d t o m u l t i p l e s i t e s o r p o s t e d
t o a l i s t s e r v
w i t h o u t t h e c o p y r i g h t h o l d e r ' s e x p r e
s s w r i t t e n p e r m i s s i o n . H o w e v e r , u s e r s m
a y p r i n t ,
d o w n l o a d , o r e m a i l a r t i c l e s f o r i n d i v
i d u a l u s e .