-
8/20/2019 Motor Lesions
1/8
Motor lesions
Upper and Lower Motor Neurons
The performance of a voluntary act needs the integrity of 2 sets
of motor neurons, upper & lowerneurons.
Upper Motor Neurons
These consist of the motor cells of the cerebral cortex &
their axons, which relay at the motor nuclei ofthe brain stem &
spinal cord, chiefly of the opposite side.
These descending tracts include:
●The corticonuclear tract: which arises from area 8 of the
frontal cortex & terminates in the motornuclei of the , !, !
cranial nerves.
●The corticobulbar tract: which arises from the motor area
& terminates in the motor nuclei of !, !,", ", " & ".
●The corticospinal tract: #pyramidal tract$: which arises
from the motor area & terminates at theanterior horn cells of
the spinal cord.
LMN include the followi ng sets:
1.%eurons in the motor nuclei of all the above mentioned cranial
nerves & their axons to s' Musclesof the eyes & the
head
2. (nterior horn cells of spinal cord & their axons to
s' Muscles of the body .
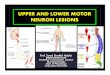
Upper Motor Neuron and Lower Motor Neuron Lesions
Manifestation of UMN lesions
(UMNL) ●)"T)%T *+ (-(./00: is wide spread because
the pyramidal fibers from a compact bundles which
occupies a small area.
●0T) *+ (-(./00: is opposite to the lesion e'g'
hemorrhage into the right internal capsule causeshemiplegia or
paralysis of the muscles of the left half of the face & the
left upper & lower limbs.
●M10.)
T*%)
: there is hypertonia & hyperreflexia due to bloc of the
extrapyramidal inhibitorydischarge on the gamma efferents &
hence the excitatory reticular formation because unopposed '
0o,spasticity is a release phenomenon from the normal inhibitory
discharge.
●- )+.)")0: superficial reflexes are absent on the
affected side as they receive their facilitatoryinfluence from the
pyramidal tracts, while the deep reflexes are exaggerated with
appearance ofclonus' 3abinsi4s sign with its center in 05 & 02
is positive.
● 6 (0T%7 *+ T) M10.): is
very slight due to exaggerated tone #spasticity$' The slight
wastingresults from the lac of voluntary movements.
-
8/20/2019 Motor Lesions
2/8
●- )0*%0) *+ M10.): to electrical
stimulation is normal, with normal excitability .
Lower Motor Neuron Lesions
●)"T)%T *+ (-(./00: is locali9ed depending on the site
of the lesion.
●0T) *+ (-(./00: is at the same side of the
lesion e'g' damage of the (s on the right side of thespinal cord
causes paralysis of the muscle supplied by these (s on the right
side.
●T*%) *+ T) M10.): there is hypotonia
because the stretch reflex arc is cut.
●- )+.)")0: both superficial and deep reflexes are
absent in the affected segments.
● 6 (0T%7 *+ T) M10.)0: is mared
due to absence of reflex tone as well as lac of
voluntarymovements.
●- )0*%0) *+ M10.)0: the response to
electrical stimulation is abnormal' The response is wea
contraction with decreased excitability, then no response when
it is transformed into fibrous tissue.
Effect of lesions of the pyramidal tracts at various
levels ●.esions of the pyramidal tract cause paralysis of the
1M%. type below the level of the lesion.
●owever, the side affected and the extent of paralysis
vary according to the site of the lesion:
○n area : this leads to restricted paralysis in the
opposite side e'g' monoplegia # paralysis of onelimb because area
is widespread so it is rarely damaged completely $.
○n corona radiate: this leads to contralateral monoplegia
or hemiplegia, depending on the extentof the lesion.
○n the internal capsule: this often leads to contralateral
hemiplegia because almost all fibers arein;ured.
○n the brain stem: this leads to contralateral hemiplegia
and ipsilateral paralysis of the cranialnerve of the .M%. type #
due to damage of their nuclei in the brain stem $.
●This condition is called
-
8/20/2019 Motor Lesions
3/8
● In the spinal cord :
(D Bi la teral lesions: in the upper cervical
region are fatal due to interruption of the respiratorypathway' n
the lower cervical region, they lead to Cuadriplegia and in the
midthoracic region lead toparaplegia.
3D Unilateral lesions: in the cervical region they lead to
ipsilateral hemiplegia while in themidthoracic region they lead to
ipsilateral monoplegia in the corresponding lower limb' n both
conditions, there is also ipsilateral paralysis of the .M%. type
of the muscles at the level of the lesiondue to damage of the
spinal motor neurons.
Note:
● (-(.)7( : paralysis of the lower limbs.
●M*%*.)7( : paralysis of one limb.
●)M.)7( : paralysis of half of the
body . ●E1(F-.)7( : paralysis of the limbs.
The internal capsule
● The internal capsule is the only subcortical pathway through
which nerve fibers ascend to anddescend from the cerebral
cortex'
● t is a ! shaped consisting of anterior and posterior limbs and
a genu #nee$'
● t is surrounded by the putamen and globus pallidus laterally
and the caudate nucleus and thethalamus medially'
The anterior limb
t contains descending fibers from the cerebral cortex to the red
nucleus, pons to cerebellum,thalamus, =rd , th , &
?th cranial nerves'
The genu
t contains corticobulbular tract'
The posterior limb
#what is underlined is what we need to memori9e' The anatomy is
not important$ contains:
● T) F)0)%F%7 /-(MF(. &
)"T-(/-(MF(. +3)-0 in the anterior 2G='
-
8/20/2019 Motor Lesions
4/8
● T) 0*M(T*0)%0*-/ -(F(T*% that ascends
behind the pyramidal fibers from the thalamic nucleito the cortical
sensory area'
● T) *T -(F(T*% that ascends behind the
somatosensory radiation from the lateral geniculate body to
visual areas in the occipital lobe'
● T) (1FT*-/ -(F(T*% that ascends
most posteriorly from the medial geniculate body of theauditory
areas in the temporal lobe'
Effect of a unilateral lesion in the posterior limb of the
internal capsule:
0uch lesion commonly called cerebral stroe is usually caused by
thrombosis or hemorrhage oflenticuloDstriate artery #a branch of
the middle cerebral artery$' atients pass into an acute thenchronic
stage'
cute stage
This lasts a few days up to 2D= wees' t is a stage of acute 1M%.
, showing the following
manifestations in the opposite side:
! +.(F (-(./00: including the upper & lower limbs, the
lower parts of the face & 5G2 of thetongue'
! )M(%()0T)0( : loss of all sensations
! .*00 *+ T) 01)-+(. -)+.)")0'
!
M (/ 3) ( *0T!) 3 (3%0H40 07%'
Notes:
The manifestations of this stage are similar to those of LMNL.
Howeer! the" can be differentiated from the LMNL b" the
following:
a' The extent of paralysis is much more widespread than in
.M%.' b' There is associated hemianaesthesiac' There may be a
Ive 3abinisi4s sign'd' 0light absence of muscle atrophy'
"hronic (permanent or spastic) stage
The main manifestations of this stage include the
following:
► Contralateral hemiplegia: of the 1M%. type, which is
characteri9ed by hypertonia, musclespasticiy of clasp nife type,
exaggerated tendon ;ers & clonus, loss of superficial reflexes
& apparentIve 3abinisi4s sign'
-
8/20/2019 Motor Lesions
5/8
Notes
● artial recovery occurs after a variable period by the effect
of the ipsilateral corticospinal tract, theextrapyramidal tracts as
the corticorubral spinal pathway, so, the patient can stand &
even wal, butthe fine silled movements of the fingers & hands
are permanently lost'
● ermanent loss of fine sensations in the opposite side, but the
crude sensations recover gradually'
● *%T-(.(T)-(. *M*%/M*10 )M(%*( : .oss of vision
in the opposite half of the 2 visual fieldsdue to interruption of
signals from the temporal part of ipsilateral retina of nasal part
of contralateralretina'
● FM%0)F )(-%7 *6)- : n both ears #by about
>BJ $, because of damage of auditory radiation
Complete SC transaction
● This result usually from accidents'
● mmediate & everDlasting loss of sensation of voluntary
movements occur due to cut of all sensorymotor tracts below the
transaction'
● Transaction in the upper cervical regions #above the =rd
cervical segment $ result in immediate deathdue to respiratory
arrest as in hinging'
● owever, at lower levels, patients pass = stages: spinal shoc,
recovery of spinal reflex activity, thenits failure &
death'
The following stage follow cord transaction:
■ 0T(7) *+ 0%(. 0*H # wees to
months in men$: all cord function are depressed'
● The manifestation of this stage are the following:
- aralysis of all muscle below the lesion #Cuadriplegia or
paraplegia $ due to cut of 1M%'
- omplete loss of all sensation below the level of
transaction'
- .oss of cord reflexes, as the stretch reflex, hence the
paralysed muscle are flaccid & the deepreflexes are absent' The
other reflexes are also absent such as the withdrawal flexor
reflex'
- (3 #arterial blood pressure $ drops maredly if the
transaction is at the level of the 5st
thoracic segment, but slight drop occurs if the lesion is below
the 2ed lumber segment' Thisdrop of (3 as well as the vascular
!F are due to sympathetic activity bloc' owever, thepressure return
to normal within few days'
- .oss of control micturition & defecation reflexes because
facilitatory pathway from thehigher centers, responsible for
bladder & rectum evacuation are interrupted by thetransaction
leading to retention with over flow with dribbling of urine by a
full bladder' Thisreturns bac after the 5st few wees'
-
8/20/2019 Motor Lesions
6/8
- .oss of erection'
● #ause of spinal shoc$:
○ t is due to sudden withdrawal of supraspinal facilitation
on spinal alpha motor neurons,namely: the continual tonic discharge
transmitted along the excitatory
reticalocpinal, vestibulospinal & corticospinal
tracts'
● %uration of spinal shoc$:
○ The Furation of spinal shoc differs in different animals
according to the degree ofdevelopment of cerebral cortex'
○ t is only a few minutes in rats'
○ n human, the duration last 2D? wees'
● #omplication of spinal shoc$:
○ hypotrension specially in highDlevel spinal cord
lesion'
○ ncrease protein catabolism due to lac of movement causing
muscle wasting & bonedissolution'
○ schemia of the compresed against bed # upper bac, gluteal
region and heels $ which healpoorly due to protein depletion'
○ 1rinary tract infection due to urine stasis'
○ +all of body temp' due to reduction of the metabolic rate
after loss of muscle tone'
Management of the Spinal Cord Lesions
● This is aimed at rapid recoer" of the spinal refle&
actiit" which can be achieed b" the following:
○ ( huge dose of 7lucocorticoids #5BgGday$ though their
antiDinflammatory action couldreduce the death rate from 8BJ to
8J'
○ (ntibiotics & good nursing care prevents infections
& reduces the mortality too'
○ 0timulants to the spinal centers as (mphetamines &
%eurotrophins'
○ 3ladder catheteri9ation to prevent urine retention &
rectal enema #to evacuate the rectum$'
○ revention of bed sore by cleaning sin with an antiseptic
& freCuent changing of thepatient4s position in bed'
○ (deCuate nutrition #malnutrition delays recovery$'
-
8/20/2019 Motor Lesions
7/8
#tages of $ecovery of the #pinal $efle% ctivity
● (fter the stage of spinal shoc, the spinal centers below the
level of the lesion recover gradually #butthe sensations &
voluntary movements never recover because the tracts in the spinal
cord cannotregenerate due to lac of neurolema'
● 'pinal recoer" occurs as the following:
• The static stretch #muscle tone$ recovers spastic
paralysis
• t appears first in the flexor muscles #causing paraplegia in
flexion$'
• Then a few months later, the extension muscle tone
predominates resulting inparaplegia in extension'
• This is followed by other extensor responses e'g' positive
supporting reaction so thepatient can stand without support'
• (s a result of recovery of muscle tone the metabolic
rate increases, the body temperature
rises towards normal level'
• The activity of the spinal vasomotor centers #lateral horn
cells$ is restored, leading to vasoconstriction so the (3
rises #but it remains labile because its precise controlmechanism
by the baroreceptors is absent$'
• -eflex micturation and defecation return but are autonomic #as
in infants$ due toabsence to voluntary control'
• 0exual reflexes recover #stimulation of the external genitalia
in males leading toerection$'
• (ppearances of the mass reflex'
Mass $efle% ● This is a hyperactive spinal reflex response
that appears after a few months'
● Mild noxious stimuli applied to the sin below the level of the
lesion results in a wide range spreadeffects due to irradiation of
signals in spinal cord to involve multiple somatic & autonomic
centers'
● 'uch effects includes:
5' )xaggerated withdrawal of the stimulated part2' 1rination
& defecation=' 0in pallor & profuse sweating' +luctuation
of the (3 #usually rise$
Notes
-
8/20/2019 Motor Lesions
8/8
● atient can be trained to induce urination or defecation
through producing intentional mass reflex#by striing or pinching
the thigh sin$'
● The flexor withdrawal reflex & 3abinisi signs are usually
the 5st to appear followed by extensorreflex e'g' nee ;er'
Possible mechanisms of The Reappearance of Spinal
Reflexes
● Fevelopment of denervation hypersensitivity, the 0pinal neuron
becomes hypersensitive tomediators released by remaining excitatory
endings'
● 7rowth of new collaterals from preexisting neurons &
formation of additional excitatory endings oninterneuron and motor
neurons #spinal neurons$'
● -eplace of spinal centers from the normal inhibitory control
of the highest centers'
Stage of ailure of Reflex !cti"it#
●This is a terminal #premortal$stage that results from bad
management during the recovery stage.
●1rinary tract infection and bed sores infection result in
failure of reflex activity and the patient diesfrom renal
failure
●The spinal centers below the leel of the lesion are
depressed once more leading to:
○.oss of the muscle tone and tendon ;ers then mass
reflex,withdrawl reflex and babinisi4s sign
○.oss of the defecation and micturtion reflexes resulting
in constipation and urineretention with over flow
○ypotension due to depression of spinal ! center 'T)
=-F stage doesn4t now days occur because of perfect
nursing and administration of antibiotics, both lines of treatment
'guard against bed source and renal infection