Embed Size (px)
Citation preview
Motor System II: Brainstem and spinal cord LMN in CNS lesions
Objectives
Motor System II: Brainstem and spinal cord LMN in CNS lesions
I. Functional Organization of Motor Neurons.
II. Symptoms Following Lesions of Spinal Lower Motor Neurons.
III. The Oculomotor System.
IV. The Trigeminal Motor Nucleus.
V. The Facial Motor Nucleus.
VI. The Nucleus Ambiguus.
VII. The Spinal Accessory (XI) Nucleus.
VIII. The Hypoglossal Motor Nucleus
I. Functional Organization of Motor Neurons
Two types of motor neurons: and . are large, multipolar neurons with prominent Nissl
bodies and an axon innervating extrafusal motor fibers. are small, multipolar neurons with fine Nissl bodies
and axon innervating the polar regions of the muscle spindle.
Functionally there are two subtypes: phasic (larger cell, less easily excited, higher firing rate, faster conducting axon) and tonic (smaller cell, more easily excited, lower firing rate, slower conducting axon).
Before a muscle contracts a “pool” of motor neurons is temporally recruited as follow: tonic phasic
II. Symptoms Following Lesions of Spinal LMN
Destruction of LMN from injury (e.g., trauma) or disease (e.g., poliomyelitis) causes the “LMN syndrome” characterized by:
1) Flaccid paralysis.
2) Hypotonia or atonia depending on severity of lesion.
3) Hyporeflexia (e.g., decreased DTRs) or areflexia (absence of reflexes).
4) Muscle atrophy and reduction of muscle mass.
5) Fasciculations (random contractions of single motor units prior to muscle degeneration).
4
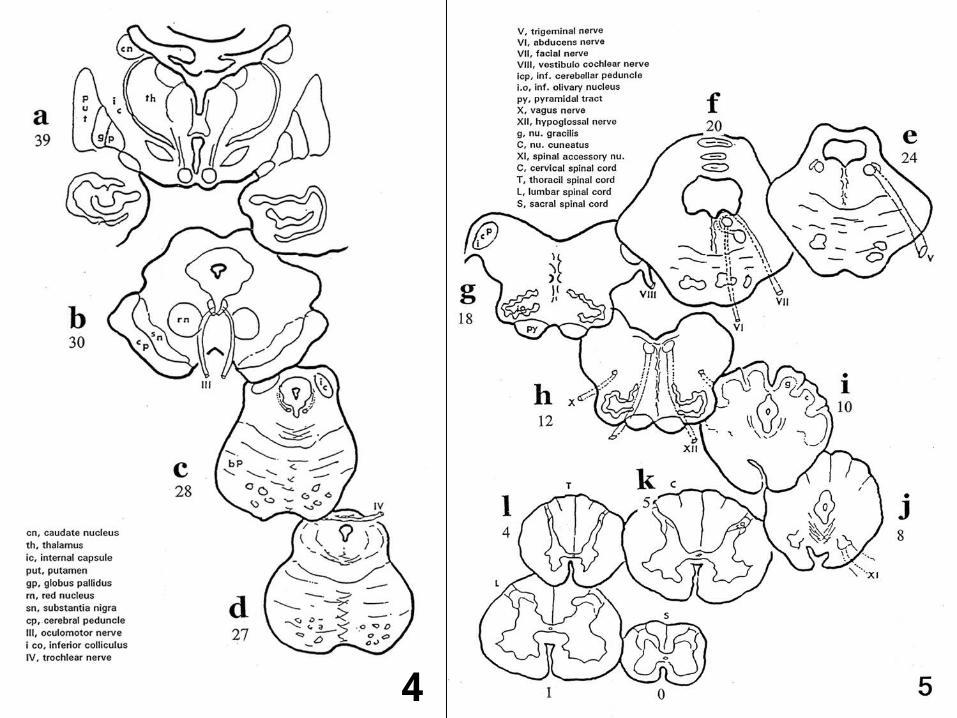
III. The Oculomotor System (Figs 4 and 5)
Includes motor III, IV and VI
Motor III. Both nuclei make V-shaped structure next to midline of rostral midbrain. Capping rostral pole is the Edinger-Westphal nucleus. Axons course through midbrain tegmentum and exit at interpeduncular fossa.
Unilateral III lesion: ipsilateral ptosis, lat strabismus (diplopia), dilated pupil (myadrisis), loss of direct light reflex and ipsilateral accomodation.
Unilateral III + PT at rostral midbrain: All of the above + PT syndrome. This combo is called the superior alternating hemiplegia (aka Weber’s syndrome).
III. The Oculomotor System (Continuation)
Motor IV (trochlear nucleus) Small, round nucleus ventral to periaquaductal gray at level of caudal midbrain.
Axons course dorsally, cross the midline, exit at midbrain/pons transition and ultimately innervate the sup oblique muscle which intorts the eye.
Unilateral 4th nerve lesion: causes ipsilateral extortion (eyeball slightly up and out) and diplopia. Patient compensates by tilting head to the non paralyzed side (which rotates the nonparalyzed eye).
Motor VI (abducens motor nucleus) Fairly large, round nucleus close to midline of caudal pons. Fibers of internal
genu of VII wrap around this nucleus. Axons from motor VI course ventrally in the tegmentum and exit at the junction of pons and medulla (inf pontine sulcus).
Unilateral nerve VI lesion. Results in ipsilateral medial strabismus with diplopia.
Unilateral abducens motor nucleus lesion. Produces the “lateral gaze syndrome”. In this syndrome neither eye can be turned towards the lesion side and both eyes tend to be conjugately deviated to the side opposite the lesion.
Unilateral nerve VI + PT lesion. This can occur at the basilar portion of the caudal pons. Signs and symptoms are those of unilateral VI lesion together with the PT syndrome. Facial paralysis does not occur because corticobulbar fibers to motor VII do not travel with PT at this level.
IV. The Trigeminal Motor Nucleus (Fig 4)
Large, round nucleus located just medial to the chief sensory nuclus of V at mid pontine levels. Axons from motor V leave the pons with the Vth nerve and then its mandibular (V3) division. Innervate the ipsilateral muscles of mastication, tensor tympani and tensor veli palatini.
Unilateral nerve V lesion. Results in paralysis of ipsilateral muscles of mastication with jaw deviating to paralyzed side upon protusion. Hyperacusis may occur from paralysis of the tensor tympani. Sensory loses to the ipsilateral face are prominent but discussed elsewhere.
Unilateral nerve V + PT. This results in the above signs + PT syndrome signs. It may occur from a single lesion occuring in the basilar portion of the pons at mid pontine levels. No facial paralysis occurs (see reason for VI + PT).
V. The Facial (VII) Motor Nucleus (Fig 4)
Large nucleus in the caudal pontine tegmentum at the same level as the abducens motor nucleus. Axons from motor VII first course dorsomedial, then wrap around the abducens nucleus (internal genu), then course ventrolaterally between the spinal nucleus of V and the facial motor nucleus, finally axons exit the pons at the cerebellopontine angle, just medial to nerve VIII.
Motor VII can be divided into a dorsal ½ (neurons innervate upper face muscles) and a ventral ½ (neurons innervate lower face muscles). Stapedius muscle also innervated.
Unilateral nerve VII lesion. Results in Bell’s palsy with patient unable to smile, show the teeth, close the eyelid or wrinkle the forehead on the paralyzed (ipsilateral) side. Hyperacusis may result from paralysis of the stapedius. Ipsilateral corneal reflex is also abolished.
Unilateral lesion of corticobulbar fibers innervating motor VII. Results in contralateral lower facial paralysis (patient can wrinkle forehead on both sides but cannot smile contralateral to lesion side).
Unilateral VI + VII + PT. Produces the Millard-Gubler syndrome
VI. The Nucleus Ambiguus (Fig 5)
Long narrow column of cells in the reticular formation at rostral and mid medulla levels. Although nucleus cannot be seen in Atlas images, at any given cross sectional level, it is located approximately half way between the spinal nucleus of V and the inf olivary complex. Axons from the ambiguus join cranial nerves IX and X (XIth portion ends up joining X outside of the CNS). They innervate the ipsilateral pharyngeal constrictors (for swallowing) and laryngeal muscles (for vocalization). Also innervate soft palate muscle.
Unilateral ambiguus (or nerve X) lesion. Results in isilateral paralysis of above muscles with dysphagia (difficulties in swallowing), dysarthria (difficulties in vocalizing) and deviation of uvula to nonparalyzed side when patient vocalizes.
Bilateral ambiguus (or nerve X) lesions. Results in aspiration pneumonia, asphyxia and eventual death. Note that this is similar to“pseudobulbar palsy” as described earlier.
VII. The Hypoglossal (XII) Motor Nucleus (Fig 5)
Column of cells next to the midline at mid and caudal medulla levels. Axons from nucleus course ventrally, just lateral to med lemniscus and then lat to pyramid, after which they exit medulla at the preolivary sulcus.
Unilateral XII nerve (or nucleus) lesion. Results in ipsilateral paralysis of intrinsic and extrinsic tongue muscles. When protruded tongue deviates to paralyzed side. In time fasciculations and atrophy of ½ the tongue occur.
Unilateral XII nerve and PT lesion. Basically at levels of the medullary pyramid, results in the inf alternating hemiplegia with signs of XII as above + PT syndrome. No facial paralysis accompanies this syndrome.
VIII. The Spinal Accesory (XI) Motor Nucleus (Fig 5)
This is another long, narrow column of cells found in the gray horn at the transition between medulla and spinal cord and from C1-5 spinal levels. Axons from the nucleus leave spinal cord half way between the dorsal and ventral roots, then rootlets coalesce to form the nerve which ascends and enters into the skull through the foramen magnum only to leave the skull through the jugular foramen. Axons eventually innervate the ipsilateral sternocleidomastoid and trapezius muscles.
Unilateral XI nerve lesion. Causes ipsilateral paralysis of the above muscles downward and outward rotation of ipsilateral scapula. The patient has difficulties turning the head to the side opposite the lesion and shrugging at the shoulder.