Embed Size (px)
Citation preview

MOLECULAR GENETIC PATHOLOGY

MOLECULAR GENETIC
PATHOLOGY
Edited by
LIANG CHENG, MDProfessor of Pathology and Urology
Director ofMolecular Pathology Laboratory
Chief of Genitourinary Pathology Division
Department of Pathology and Laboratory Medicine
and Clarian Pathology Laboratory
Indiana University School ofMedicine, Indianapolis, IN
DAVID Y. ZHANG, MD, PhD, MPHAssociate Professor ofPathology
Director, Molecular Pathology Laboratory
Department of Pathology
Mount Sinai School ofMedicine
and the Mount Sinai Medical Center
New York, NY
,\1', H P"'1\' umana ress


Preface
We have had the opportunity to witness both the beginningand the subsequent growth of an exciting specialty thatcombines both pathology and medical genetics, a fieldcommonly referred to as molecular genetic pathology. Thebirth of this specialty took place in 1988 when Kari Mullisdeveloped a new DNA amplification technology called thepolymerase chain reaction (PCR). Within a few years, thistechnology was no longer being used exclusively in researchlaboratories. The technique had found numerous newapplications in clinical medicine as a tool for diagnosis anddiseases monitoring. The use of PCR technology has greatlyexpanded the specialties of anatomic and clinical pathologyand has increased the availability of genetic testing in theclinical setting. We expect that such advances as thecompletion of the Human Genome Project, the maturation ofpharmacogenomics, the growth of proteomics, and the rapidlygrowing field of molecular genetic pathology will lead to anew era of personalized and customized patient care.
More recently, the American Board of Pathology (ABP), inconjunction with the American Board of Medical Genetics(ABMG), established a new subspecialty, molecular geneticpathology. Fellowship training for molecular geneticpathology is approved by the Accreditation Council forGraduation Medical Education (ACGME). Many pathologistsand medical geneticists are applying for advanced trainingin this growing subspecialty. Training in molecular pathologyis also becoming a required element in pathology residencycurricula. To meet these demands, a team of more than50 leading experts has compiled this quick reference bookfor medical students, general practitioners, medicaltechnologists, pathologists, and medical geneticists . We alsohope that residents or fellows who are training in pathologyand medical genetics will find this book helpful in theirpreparation for board examinations .
Molecular Genetic Pathology contains two parts. Part Icovers general molecular genetic pathology and technology,including principles of clinical molecular biology, principles
of clinical cytogenetics, diagnostic methodology andtechnology, tissue microarrays and biomarker validation,laser capture microdissection, clinical flow cytometry,conceptual evolution in cancer biology, clinical genomics inoncology, clinical proteomics, clinical pharmacogenomics,clonality analysis in surgical pathology, fluorescencein situ hybridization (FISH), conventional cytogenetics forhematology and oncology diagnosis, instrumentation, geneticinheritance and population genetics, and genetic counseling .Part II provides disease-based information, including prenataldiagnosis, familial cancer syndromes, molecular testing forsolid tumors, molecular pathology of the central nervoussystem, molecular virology, molecular bacteriology, mycologyand parasitology, molecular testing for coagulopathies,molecular hemoglobinopathies, molecular diagnostics oflymphoid malignancies, molecular diagnostics of myeloidleukemias, HLA system and transfusion medicine (molecularapproach), molecular forensic pathology, gene therapy, ethicaland legal issues in molecular testing, and quality assurance andlaboratory inspection. Each chapter begins with a detailedTable of Contents for easy reference.
Assembling this diverse guidebook has truly been a teameffort, cutting across many traditional specialty boundaries .We are most grateful for all the contributors who made thisproject possible. Our special thanks go to Mr. Ryan P.Christy from the Multimedia Education Division of theDepartment of Pathology at Indiana University, who hasedited the illustrations for the book. We would like to thankthe staff at Humana Press/Springer, including Ms. Mary JoCasey, Mr. Paul Dolgert , Mr. Richard Hruska, and Mr. DavidCasey for their assistance in the development and editing ofthis text, and in particular Ms. Amy Thau, without whoseoutstanding work this book would have been an impossibleachievement.
Liang Cheng, MD
David Y. Zhang, MD, PhD, MPH
v

Contents
Preface v
Contributors ix
Part I General Sections
1 Principles of Clinical Molecular BiologyShaobo Zhang, DarrellD. Davidson,
David Y. Zhang, Jodi A. Parks,and Liang Cheng 1
2 Principles of Clinical CytogeneticsStuart Schwartz 33
3 Diagnostic Methodology and TechnologyJosephine Wu, Tao Feng, Ruliang Xu, Fei fe,
Bruce E. Petersen, Liang Cheng,and David Y. Zhang 65
4 Tissue Microarraysand Biomarker Validation
Martina Storz and Holger Moch 133
5 Laser Capture MicrodissectionMatthew Kuhar and Liang Cheng 141
6 Clinical Flow CytometryMagdalena Czader 155
7 Conceptual Evolution in Cancer BiologyShaobo Zhang, DarrellD. Davidson,
and Liang Cheng 185
8 Clinical Genomics in OncologyHugo M. Horlings and
Marc van de Vijver 209
9 Clinical ProteomicsDavidH. Geho, Virginia Espina,
Lance A. Liotta, Emanuel F. Petricoin,and Julia D. Wulfkuhle 231
...
10 Clinical PharmacogenomicsCatalina Lopez-Correa
and LawrenceM. Gelbert 241
11 Clonality Analysis in Modem Oncologyand Surgical Pathology
Liang Cheng, Shaobo Zhang,Timothy D. Jones,and Deborah E. Blue 261
12 Fluorescence In Situ Hybridization(FISH) and ConventionalCytogenetics for Hematologyand Oncology Diagnosis
Vesna Najfeld 303
13 InstrumentationBruce E. Petersen, Josephine Wu,
Liang Cheng, and David Y. Zhang 365
14 Genetic Inheritance and PopulationGenetics
Tatiana Foroudand Daniel L. Koller 393
15 Genetic CounselingKimberly A. Quaidand
Lisa J. Cushman 405
Part II Disease-Based Sections
16 Molecular Medical GeneticsLisa Edelmann, Stuart Scott,
and Ruth Kornreich 415
17 Prenatal DiagnosisNataline Kardon and Lisa Edelmann 441
18 Familial Cancer SyndromesMichelle P. Eliefj, Antonio Lopez-Beltran,
Rodolfo Montironi, and Liang Cheng ..... 449
vii

ContentsllIiJltEii
19 Molecular Testing for Solid TumorsNeal I. Lindeman and Paola Dal Cin 467
20 Molecular Pathology of the CentralNervous System
Eyas M. Hattab and Brent T. Harris 497
21 Molecular VirologyJosephine Wu, Mona Sharaan,
and David Y. Zhang 533
22 Molecular Bacteriology, Mycologyand Parasitology
Mona Sharaan, Josephine Wu,Bruce E. Petersen, andDavid Y. Zhang 581
23 Molecular Testing for CoagulopathiesVeshana Ramiah and Thomas L. Ortel 623
24 Molecular HemoglobinopathiesJodi A. Parks, Tina Y. Fodrie,
Shaobo Zhang, andLiang Cheng 637
25 Molecular Diagnostics of LymphoidMalignancies
Francisco Vega andDan M. Jones 655
26 Molecular Diagnostics of MyeloidLeukemias
C. Cameron Yin and Dan M. Jones 675
27 The HLA System and TransfusionMedicine: Molecular Approach
S. Yoon Choo 689
28 Molecular Forensic PathologyP. Michael Conneally and
Stephen R. Dlouhy 703
29 Gene Therapy: Vector Technologyand Clinical Applications
Kenneth Cornetta 717
30 Ethical and Legal Issuesin Molecular Testing
Kimberly A. Quaid 731
31 Quality Assurance and LaboratoryInspection
CarolL. Johns and Liang Cheng 737
AppendixLiang Cheng and Shaobo Zhang 751
Index 767
lU l U
viii21M I rr m1ttt lllTJrr_wn

Contributors
DEBORAH E . BLUE, MDAssistant Professor of PathologyAssociate Director, Molecular Pathology LaboratoryDepartment of Pathology and Laboratory Medicineand Clarian Pathology LaboratoryIndiana University School ofMedicineIndianapolis, IN
LIANG CHENG, MDProfessor ofPathology and UrologyDirector ofMolecular Pathology LaboratoryChief, Genitourinary Pathology DivisionDepartment ofPathology and Laboratory Medicineand Clarian Pathology LaboratoryIndiana University School ofMedicineIndianapolis, IN
S. YoON CHOO, MDAssociate Professor of Pathology and MedicineDirector of HLA Laboratory, Associate Medical DirectorofBlood BankDepartments ofPathology and MedicineMount Sinai School ofMedicine and the Mount SinaiMedical CenterNew York, NY
P. MICHAEL CONNEALLY, PhDDistinguished Professor Emeritus, Medical andMolecular Genetics and NeurologyDepartment ofMedical and Molecular GeneticsIndiana University School ofMedicineIndianapolis, IN
KENNETH CORNETIA, MDJoe C. Christian Professor and ChairmanDepartment ofMedical and Molecular GeneticsIndiana University School ofMedicineIndianapolis, IN
LISA 1. CUSHMAN, PhDCertified Genetic CounselorDepartment ofMedical and Molecular GeneticsIndiana University School ofMedicineIndianapolis, IN
-
MAGDALENA CZADER, MD, PhDAssistant Professor ofPathologyDirector of Clinical Flow Cytometry LaboratoryDepartment ofPathology and Laboratory MedicineIndiana University School ofMedicineIndianapolis, IN
PAOLA DAL ON, PhDAssociate Professor ofPathologyCytogenetics LaboratoryDepartment ofPathologyBrigham and Women's Hospitaland Harvard Medical SchoolBoston, MA
DARRELL D . DAVIDSON, MD, PhDAssistant Professor ofPathologyDepartment of Pathology and Laboratory MedicineIndiana University School ofMedicineIndianapolis, IN
STEPHEN R. DLOUHY, PhDAssociate Research ProfessorDepartment ofMedical and Molecular GeneticsIndiana University School ofMedicineIndianapolis, IN
LISA EDELMANN, PhDAssistant ProfessorDepartment ofGenetics and Genomic SciencesDirector, Molecular CytogeneticsCo-Director, Genetic Testing LaboratoryMount Sinai School ofMedicine and the Mount SinaiMedical CenterNew York, NY
MICHELLE P. EUEFF, MDStaff PathologistDiagnostic Pathology Services, Inc.Nampa, ID
JltW
ix

ContributorsmUI
VIRGINIA ESPINA, MSResearch ProfessorThe Center for Applied Proteomicsand Molecular MedicineGeorge Mason UniversityManassas, VA
HUGO M. HORLINGS, MDDepartment of PathologyThe Netherlands Cancer Institute/Antoni vanLeeuwenhoek HospitalAmsterdam, The Netherlands
TAO FENG, MS, MP (ASCP)Research AssistantDepartment of PathologyMount Sinai School ofMedicineand the Mount Sinai Medical CenterNew York, NY
TINA Y. FODRIE, BS, MT, MP (ASCP)Supervisor, Department ofMolecular PathologyIndiana University School ofMedicineand VA Medical CenterIndianapolis, IN
CAROL L. JOHNS, PhDSupervisor and Technical CoordinatorClarian Molecular Pathology LaboratoryIndiana University School ofMedicineIndianapolis, IN
DAN M . JONES, MD, PhDProfessor of PathologyDepartment ofHematopathologyMedical Director, Molecular Diagnostics LaboratoryThe University of Texas M. D. Anderson Cancer CenterHouston, TX
TATIANA FOROUD, PhDProfessor ofMedical and Molecular GeneticsDepartment ofMedical and Molecular GeneticsIndiana University School ofMedicineIndianapolis, IN
TIMOTHY D . JONES, MDStaff PathologistDepartment of PathologyFloyd Memorial Hospital and Health ServicesNew Albany, IN
DAVID H. GEHO, MD, PhDAssociate Director of ImagingMerck and Company, Inc.West Point, PA
LAWRENCE M. GELBERT, PhDResearch AdvisorEli Lilly and CompanyIndianapolis, IN
BRENT T. HARRIS, MD, PhDAssistant Professor ofPathologyDepartment of PathologyDartmouth Medical SchoolLebanon, NH
EYAS M. HATIAB, MDAssociate Professor of PathologyDepartment ofPathology and Laboratory Medicineand Clarian Pathology LaboratoryIndiana University School ofMedicineIndianapolis, IN
NATALINE KARDON, MDAssociate ProfessorDirector ofPrenatal Cytogenetics LaboratoryDepartment of Genetics and Genomic Science sMount Sinai School of Medicine and the Mount SinaiMedical CenterNew York, NY
DANIEL L. KOLLER, PhDResearch Assistant ProfessorDepartment ofMedical and Molecular GeneticsIndiana University School ofMedicineIndianapolis, IN
RUTH KORNREICH, PhDResearch Assistant Professor ofHuman GeneticsCo-Director Genetic Testing LaboratoryDepartment ofHuman GeneticsMount Sinai School ofMedicine and the Mount SinaiMedical CenterNew York, NY
MATIHEW KUHAR, MDResidentDepartment of Pathology and Laboratory Medicine andClarian Pathology LaboratoryIndiana University School ofMedicineIndianapolis, IN
IU!
_____..... ...Jjl...J'M"iG.~~ll!il"'_1f:Jrn!1~ • If'l!!W1!¥_M'''RW''''.ttti''''·~...··. ·.,.f _
x

Contributors
NEAL I. LINDEMAN, MDAssociate Pathologist, Clinical ChemistryAssociate Pathologist, Molecular DiagnosticsBrigham and Women 's HospitalAssistant Professor of PathologyHarvard Medical SchoolBoston , MA
LANCE A. LIOTIA, MD, PhDDirector, The Center for Applied Proteomicsand Molecular MedicineProfessor of Life SciencesGeorge Mason UniversityManassas, VA
ANTONIO LOPEZ-BELTRAN, MD, PhDProfessor ofPathologyDepartment ofPathology and SurgeryCordoba University Medical SchoolCordoba, Spain
CATALINA LOPEZ-CORREA, MD, PhDPrincipal Research ScientistEli Lilly and CompanyIndianapolis, IN
HOLGER MOCH, MDProfessor and ChairmanInstitute ofSurgical PathologyDepartment of PathologyUniversity Hospital ZurichZurich, Switzerland
RODOLFO MONTIRONI, MD, FRCPathProfessor ofPathologyInstitute of Pathological Anatomy and HistopathologyPolytechnic University of the Marche Region (Ancona)School ofMedicineUnited HospitalsAncona, Italy
VESNA NAJFELD, PhDProfessor of Pathology and MedicineDirector, Tumor Cytogenetics, and Oncology, Molecularand Cellular Tumor MarkersMount Sinai School ofMedicine and the Mount SinaiMedical CenterNew York, NY
THOMAS L. ORTEL, MD, PhDAssociate Professor ofMedicine and PathologyHemostasis and Thrombosis CenterDuke University Medical CenterDurham, NC
JODI A. PARKS, MDVisiting Lecturer, Clinical ChemistryDepartment of Pathology and Laboratory Medicineand Clarian Pathology LaboratoryIndiana University School ofMedicineIndianapolis, IN
BRUCE E. PETERSEN, MDMolecular Genetic Pathology FellowDepartment of PathologyMount Sinai School ofMedicine and the Mount SinaiMedical CenterNew York, NY
EMANUEL F. PETRICOIN, PhDProfessor ofLife SciencesDirector, The Center for Applied Proteomicsand Molecular MedicineChair, Department of Molecular and MicrobiologyGeorge Mason UniversityManassas, VA
KIMBERLY A. QUAID, PhDProfessor ofMedical and Molecular GeneticsDepartment ofMedical and Molecular GeneticsIndiana University School ofMedicineIndianapolis, IN
VESHANA RAMIAH, MD
Hematology/Oncology FellowDuke University Medical CenterDurham, NC
STUART SCHWARTZ, PhD, FACMGProfessor of Human GeneticsDepartment of Human GeneticsUniversity of ChicagoChicago,IL
STUART SCOTT, PhDClinical Molecular Genetics FellowDepartment of Human GeneticsMount Sinai School ofMedicine and the Mount SinaiMedical CenterNew York, NY
MONA SHARAAN, MDMolecular Genetic Pathology FellowDepartment ofPathologyMount Sinai School ofMedicine and the Mount SinaiMedical CenterNew York, NY
""' AU
XI

Contributors
MARTINA STORZ, BS
Directorof TMA Core FacilityInstitute ofSurgicalPathologyDepartmentofPathologyUniversity Hospital ZurichZurich, Switzerland
MARC VAN DE VIJVER, MD, PhDProfessor of PathologyDepartment ofPathologyThe Netherlands Cancer Institute/Antoni vanLeeuwenhoek HospitalAmsterdam, The Netherlands
FRANCISCO VEGA, MD, PhDAssistant Professor of PathologyDepartmentof HematopathologyThe University of Texas M. D. Anderson CancerCenterHouston, TX
JOSEPHINE WU, DDS, CLSp(MB), CLDirAssistant ProfessorDepartmentof PathologyMount Sinai School ofMedicineand the Mount SinaiMedical CenterNew York, NY
JULIA D. WULFKUHLE, PhDResearch ProfessorThe Centerfor Applied Proteomics and MolecularMedicineGeorge Mason UniversityManassas, VA
RULIANG XU, MD, PhDAssociate Professor of PathologyDepartmentof PathologyNew York University School ofMedicineNew York, NY
FEI YE, PhDAssistant ProfessorDepartmentof PathologyMount Sinai School ofMedicine and the Mount SinaiMedical CenterNew York, NY
C. CAMERON YIN, MD, PhDAssistant Professor of PathologyDepartmentof HematopathologyThe University of Texas M. D. Anderson Cancer CenterHouston, TX
DAVID Y. ZHANG, MD, PhD, MPHAssociate ProfessorofPathologyDirector, MolecularPathology LaboratoryDepartmentofPathologyMount Sinai School ofMedicine and the Mount SinaiMedical CenterNew York, NY
SHAOBO ZHANG, MDAssociate ResearchProfessorDepartmentofPathology and LaboratoryMedicineIndiana University School ofMedicineIndianapolis, IN
RID
xiisr. - we w I.

Part I
General Sections

1
Principles of Clinical Molecular BiologyShaobo Zhang, MD, Darrell D. Davidson, MD, PhD, David Y. Zhang, MD, PhD, MPH,
Jodi A. Parks, MD, and Liang Cheng, MD
CONTENTS
I. Deoxyribonucleic Acid (DNA) 1-4Overv iew 1-4Types of DNAs 1-5DNA Replication 1-7DNA Mutation 1-8
DNA Mutation and Disease 1-9Factors Related to DNA Aberrations 1-9
DNA Repair Mechanisms 1-12
II . Genes 1-13Overview 1-13Gene Components 1-13Functional Categories of Genes 1-13Cancer- Related Genes 1-14Regulation of Gene Expression 1-14Signal Transduction 1-19
III. Chromosomes 1-19Overview 1-19Chromatin 1-19
Chromosomes 1-19
IV. RNA and Proteins 1-22Overview 1-22Types of RNA 1-23Ribosome and Ribozyme 1-23mRNA Processing 1-24Protein Translation 1-27
V. Mitochondrial DNA 1-28Overview 1-28mtDNA Inheritance 1-28Characteristics of mtDNA 1-28Mitochondrial Genes and Gene Expression 1-28mtDNA Replication 1-29mtDNA Damage, Mutations,
and Repair 1-30Mitochondrial Disease 1-31
VI. Suggested Reading 1-32
3

1-4
DEOXYRIBONUCLEIC ACID (DNA)
Molecular Genetic Pathology
Overview• Definition
- DNA is a large nucleic acid polymer arranged inchromosomes for storage, expression and transmissionof genetic information
- The genetic information is encoded by a sequence ofnucleotides
• Components of DNA
- Bases are molecules containing carbon-nitrogen ringsin DNA
• Purines: adenine (A) and guanine (G) have twojoined carbon-nitrogen rings
• Pyrimidines: thymine (T) and cytosine (C) have onecarbon-nitrogen ring
- Nucleoside is made up of a five-carbon sugar(deoxyribose) and a base
- Deoxyribose is the same sugar found in RNA, but withoxygen removed from the 2' carbon position
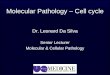
- Nucleotide is made up of a phosphate group, apentose sugar (deoxyribose), and a nitrogenous base(Figure 1)
• The phosphodiester bond
• The phosphate group is bond to the nucleosideat the hydroxyl group of the 5' carbon atom ofdeoxyribose
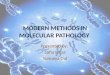
• Phosphodiester bonds are strong covalent bondsbetween phosphate groups connecting the 5'carbon of one deoxyribose to the 3' carbon ofthe next deoxyribose of the adjacent nucleotidenucleotide (Figure 2)
• The phosphodiester bond determines DNAchain polarity (ends designated as either 5'or 3')
• DNA sequence refers to the order of the nucleotidesin a DNA strand, which code for unique sets ofgenetic information, both proteins and regulatorysegments
Adenine Guanine Cytosine Thymine
2-Deoxyribose
HOf>°""I~HHO HCytidine
I
NH2Ij'N=CN
'\ ~)N N
HOf> 0",,1~H
HO H
Adenosine
Nucleoside
Fig. 1. There are four bases in DNA: Adenine (A), guanine (G), thymine (T), and cytosine (C). Adenine and guanine are purinesand thymine and cytosine are pyrimidines. Deoxyribose is the sugar in DNA. The carbon atoms are numbered as indicated. Notethere is no oxygen on site 2 of deoxyribose. A nucleoside molecule is composed of a base and deoxyribose. When a phosphategroup is added to nucleoside, the complex becomes a nucleotide . Nucleotides are the basic building blocks of DNA.
4

Principles of Clinical Molecular Biology
5 CH2 Base
l /o~ 14C C
I\H HI'H I I H
3'--1 2
o H
IO=p-O-
IoI
5 CH2
o Base
c/~l'\ H HI'H \1 1 H
C--C
I Io H
1-5
Fig . 2. 3'5' Phosphodiester bonds joint by the unit of the repetitive sugar-phosphate chain. Each nucleotide is linked by the3' carbon atom of upstream ribose to the 5' carbon of the downstream ribose. Phosphodiester bonds are central to all life onearth, as they make up the backbone of DNA and RNA strands in every organism.
- The deoxyribonucleotides in DNA differ only in thebases they carry, so the DNA sequence is denoted by abase sequence (e.g., -ATTGCAT-)
- Base sequence is presented from 5' to 3'
- DNA strands are pairs of complementary molecules,which entwine each other in an antiparallel direction
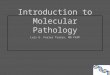
- Two strands of DNA wind around each other to form adouble helix (Figure 3)
• Deoxyribose-phosphate backbone is on the exteriorof the DNA double helix
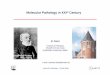
• The interior of the DNA is formed by paired basesattached to each other by hydrogen bounds.G (Guanine) pairs with C (Cytosine) via threehydrogen bonds, and A (Adenine) pairs withT (Thymine) via two hydrogen bonds inside thedouble helix. Note that the three hydrogen bondsjoining G to C (GC bond) are stronger than the twohydrogen bonds joining A to T (AT bond) (Figure 4)
- DNA has two DNA chains; one is oriented 5'~3' whilethe other strand is oriented 3'~5' direction (antiparallel)
• Sense is a DNA strand that could be transcribed.Sense strand has a sequence similar to its RNAtranscript
• Antisense is the complimentary strand of sense.Antisense works as template for the RNA transcript
• A DNA fragment appears to have a uniquefunction, either structural , regulatory, or coding
Types of DNAs• Single copy DNA is a specific DNA sequence that is
present only once in the genome
• Repetitive DNA is a DNA segment with a specificDNA sequence that is repeated multiple times in thegenome
• Moderately repetitive DNA refers to 10-105 copies of thesequence per genome
- Moderate repeated DNA is found primarily in noncoding sequences
• Highly repetitive DNA describes DNA sequence presentin greater than 105 copies per genome
- Highly repeated DNA is found primarily incentromere and telomere regions as tandem repeats
• Tandem repeat DNA contains a variable number of shortDNA sequences repeated many times in series . Thenumber of repeats is unique to each individual , and canbe used for relationship testing
- The tandem repeat pattern may vary from one baserepeats (mononucleotide repeat) to several IOOO-bprepeat sequences
5

1-6 Molecular Genetic Pathology
3' end
3'end
5'end
5'
3'
3'
5'
Fig. 3. Human genomic DNA contains two polynucleotide chains wound around each other to form a double-stranded helix . Thetwo chains are "antiparallel,' one running 5'-3' and the other running 3'-5' direction . The DNA strands are synthesized and readout by RNA polymerase in the 5'-3' direction . The purine or pyrimidine attached to each deoxyribose projects into the center ofthe helix. Base A pairs with T and a G pairs with C through hydrogen bonds in the central axis.
6
- These segments of DNA are satellite DNA because ofthe experimental observation that they often forma minor satellite band near the major centrifugationfraction when DNA is separated by density gradient
- Clusters of such repeats are scattered on manychromosomes. Each variant is an allele that isinherited co-dominantly
- Megasatellite DNAs are tandem repeat DNA segmentswith a length greater than 1000 bp (1 kbp) repeated50-400 times
- Satellite DNAs comprise about 15% of human DNA.The repeated sequence ranges from 5 to 170 bp andthe complex is about 100 kbp in length
- Minisatellite DNAs are repeated sequence s rangingfrom 14 to 500 bp in length . The repeat complex is0.1-20 kbp in length. Minisatellite DNA is present intelomere region
- Microsatellite DNAs are sequences <15 bp in lengththat repeat 10-100 times without interruption. Thereare approx 200,000 microsatellite loci in the humangenome (Table 1)
• Loss of heterozygosity (LOH) in a cell representsthe loss of one parent's contribution of DNA to acell 's genome, often in microsatellite regions
• It often indicates the presence of tumor-suppressorgene loss around the microsatellite locus
• LOH can arise through deletion, nonreciprocalDNA transfer, mitotic recombination, orchromosome loss
• LOH is often used to analyze the clonal originof cancer-associated loci
• Microsatellite DNA loci are useful markers forthe detection of LOH

Principles of Clinical Molecular Biology
HI
C N-:? ......... / .....H----OHC C III II /C<, __NN", N---H- N C \.
Su~ r I II ;CH.....C~ ...... C__
O----H- N ""N...... NI \H Sugar
Fig. 4. The double helical structure of DNA is largely due tohydrogen bonding between the base pairs linking onecomplementary strand to the other. Hydrogen bonds are noncovalent, weak bonds between electron donors and recipients.There are two hydrogen bonds between A and T and threehydrogen bonds between G and C, thus the bonds between Gand C are stronger than between A and T.
Table 1. Major Characteristics of RepetitiveDNA
Number ofForm of DNA Length (bpJ repeats
Singlecopy Vary Singlecopy
Moderately repetitive Vary 10-105
Highly repetitive Vary >105
Tandem repeat
Megasatellite >1000 50-400
Satellite 5-170 500-2000
Minisatellite 14-500 7-40
Microsatellite <15 10-100
1-7
• When parents' contributions of certainmicrosatellite loci are of different size, thesemicrosatellite loci are informative
- Microsatellite instability at critical loci is a marker formalignancy or premalignant genetic change(see details in Chapter 7)
• Mitochondrial DNA (mtDNA) (seeMitochondrial DNA)
DNA Replication• Double-stranded DNA (dsDNA) is exactly duplicated
prior to cell division so that each daughter cell isendowed with an exact replica of the parent cell DNA
• DNA replication occurs during S (synthesis) phase of thecell cycle
- Cell cycle refers to a cycle of events in a eukaryoticcell from one cell division to the next; it consists ofGo' G I' S, G2, and M phases (Figure 5)
- Semiconservative replication means that each DNAmolecule consists of one original and one newlysynthesized chain (Figure 6)
• DNA Polymerases
- DNA polymerases are enzymes involved in DNAreplication. Eukaryotic cells have five different DNApolymerases
• DNA polymerase a and 8 replicate nuclear DNA
• DNA polymerase ~ and E are involved in DNArepair
• DNA polymerase yreplicates mitochondria DNA(mtDNA)
• Multiple replications means that replication begins atmultiple sites within a DNA strand and proceedsbidirectionally from each origin (Figure 7)
- The replication apparatus at each origin forms abubble and extends toward both ends of the DNAmolecule until it meets another bubble
- The leading strand is the DNA chain that issynthesized continuously in the 5'-3' direction
• Synthesis of the leading strand is catalyzed byDNA polymerase 8
- The lagging strand is the DNA chain that issynthesized as a series of short fragments, known asOkazaki fragments, polymerized in the 5'~3'direction also (Figure 8)
• The newly synthesized DNA fragments willeventually meet and ligate to create an intactstrand
• The lagging strand is synthesized by DNApolymerase a
• The lagging strand polymerizes from 5' to 3'at the nucleotide level but overall growth byligation of Okazaki fragments is in the 3'~5'direction
7

1-8
S PHASE(DNA replication)
mitosis(nucleardivision)
Molecular Genetic Pathology
M PHASE
Fig. 5. The cell cycle, or cell-divi sion cycle, is the series of events in a eukaryotic cell between one cell division and the next. Thecell cycle consists of four phases , GI' S, Go' and M phase. Go is a period in which cells exist in a quiescent state. Go'Gl' G2, andS phase are collectively known as interphase. Cells in Go phase are resting cells unable to divide without a signal to re-enter thecell cycle. DNA synthesis occurs during S phase, which is followed by a short G2 phase. Mitosis and cytokinesis together aredefined as the M (mitotic) phase, during which the mother cell divides into two daughter cells .
DNA Mutation
• DNA mutation is a permanent change in the geneticmaterial sequence
• Most mutations are found in noncoding sequences
• Single base pair substitution (point mutation) involves asingle nucleotide, which is replaced with another nucleotide
- Point mutation is the most common form of mutation
- It happens most commonly in non-coding sequences
- It is also the most frequent type of mutation associatedwith tumor suppressor gene mutation
• Transitions are the mutations that substitute a differentpurine for a purine or a pyrimidine for a pyrimidine
• Transversions are mutations that substitute a differentpurine for a pyrimidine or a pyrimidine for a purine
• Synonymous (silent) mutation is a single base pairsubstitution yielding a different codon that stillcodes for the same amino acid
• Missense mutation is a single base pair substitutionthat results in a different codon and a differentamino acid
• Nonsense mutation is a single base pair substitutionthat converts a codon specifying an amino acid intoa stop codon
8
- Deletion is an irreversible mutation in which one ormore nucleotides are removed from the DNAsequence
• The deletion will cause a shift of the reading frame• A one base deletion, for example, will shift all
codons left, altering the amino acids for whichthey code
• Insertion is a mutation that adds one or more nucleotidesto the DNA sequence
- An insertion in the coding region of a gene may causea shift in the reading frame
- An insertion alters splicing of messenger RNA(mRNA) (splice site mutation)
• Amplification increases the dosage of genes locatedwithin a locus by inserting multiple copies of thechromosomal region or by promulgating fragments ofDNA containing the locus outside the chromo somes.Proteins produced from amplified genes are generallyincreased
• Loss of heterozygosity (LOH) is a DNA alteration inwhich one allele from one parent's contribution is lost,either by deletion or a recombination event
• The most frequently observed gene associated with LOHin sporadic cancer is p53

Principles of Clinical Molecular Biology 1-9
Fig. 6. Semiconservative DNA duplication occurs when DNA replicates, each parental chain is used as template for synthesis of acomplimentary daughter chain. Newly formed duplex strands contain one parental and one daughter chain as indicated by color scheme.
DNA Mutation and Disease• DNA mutations cause errors in protein sequences,
creating partially or completely non-functional proteins
• DNA mutations give rise to offspring that carry themutation in all their cells
- Human beings with a single allele mutation willtransmit the mutation to half of the progeny
- If both alleles are mutated, all progeny will inherit themutation
Factors Relatedto DNA Aberrations• Spontaneous chemical reactions
- Spontaneous chemical reactions cause single base pairsubstitutions or single base pair deletion through thefollowing processes
• Tautomerism-base change by repositioning ahydrogen atom
• Depurination-loss of a purine base (A or G)
• Deamination-changes a normal base to an atypicalbase
• Change from C~U
• Spontaneous deamination of 5-methycytosine(irreparable)
• Change from A~HX (hypoxanthine)
• Transition-a purine changes to another purine, ora pyrimidine to a pyrimidine
• Transversion-a purine becomes a pyrimidine, or apyrimidine becomes a purine
• Induced mutations- Chemical mutagenesis can modify bases and cause
either interstrand or intrastrand cross-linking.Common chemical mutagens include:
• Nitrosoguanidine (N-methyl-N'-nitrosoguanidine)
• Hydroxylamine (NHPH)
9

1-10 Molecular Genetic Pathology
t Multiple DNA replication sites
....---..... ....---..... ....---.....-- -- --t DNA fragment extension
:..-----------~:..---------------'::::---..---: :::---..---:
t New strands synthesised
+
Fig. 7. Multiple replications are an efficient way to synthesize chromosomal DNA. DNA synthesis begins at many locations andproceeds bidirectionally from each location . Eventually the replication bubbles merge and the DNA fragments are ligated to formtwo daughter DNA strands. Each of the newly synthesized double strands consists of one parental and one newly synthesizedchain (semiconservative).
•" ~ ~ s
5' 3'
5' 3'
Leading strand
5' 3'
•"sf ~\, s,
Lagging strand
3' 5'
5' 3'
•'\'\\' 5
Fig. 8. The DNA double helix is unwound by the enzyme helicase before synthesis of a new DNA chain begins. A DNApolymerase (shown in green) binds to the strand and moves along the strand assembling the leading strand (fragment inside theleft fork). The lagging strand is synthesized in discontinuous polynucleotide segments called Okazaki fragments . A series ofOkazaki fragments are linked by DNA ligase to form the lagging strand. In eukaryotic cells the leading and lagging strands aresynthesized by DNA polymerase 0 and a, respectively.
10
• Base analogs (e.g., bromodeoxyuridine) onlymutate DNA when the analog is incorporatedduring S phase in replicating DNA
• Alkylating agents (e.g., cyclophosphamide) mutateboth replicating and non-replicating DNA. Thealkylating agent transfers an alkyl group, often tothe N7 position of guanine
• Polycyclic hydrocarbons are converted within cellsto highly reactive epoxy compounds that react withDNA (e.g., benzpyrenes found in internalcombustion engine exhaust and cigarette smoke)
• DNA intercalating agents insert themselvesbetween the stacked bases at the center of the DNAstrand (e.g., ethidium bromide)

Principles of Clinical Molecular Biology 1-11
3'
_ x
I I i I I 3 'A G T C CT C A G GI I I I I 5 '
5' I
TTCTG AGTCC
3' ~ ~ f ~ W y ~ f f 5'
+Gf-Diester:?
5' I I ,.::;:: ( "'i~ I I 3 'TTCTG AGTCC
3,11 f 1 W y 1 f Y5'DNA polymerase ~
5' and ligase
f+6+~+AAGACA
3' I I I I I I
5 ' I I I I If1 I I I I 3'TTCTG AGTCCA AGAC TCAGG
3" I !! W I I I 1 5'
+
5' 3'TT CTG AG T C CAA G A C TCAGG
3' " " W ' I I ' 5'
+
- Mismatch repair removes nucleotides, which aremispaired with the corresponding base on thecomplementary chain, usually by DNA polymeraseerrors. This repair process can also remove up to 30base insertions (Figure 10)Translation synthesis temporarily replaces theconventional polymerase at a DNA lesion by one of agroup of specialized polymerases that can replicatedamaged DNA. It is better for the daughter cell toinherit a point mutation than to have a significant partof a chromosome deleted, causing framshift
Fig. 9. A single base in DNA may be chemically mutated, forexample, by deamination or alkylation , causing incorrect basepairing (X), and consequently, incorrect codons in the DNA.BER is initiated by DNA glycosylases linking particular typesof chemically altered bases to the desoxyribose-phosphatebackbone. This mutated base is excised as a free base ,generating sites of base loss called apurinic or apyrimidinic(AP) sites. The AP sites are substrates for AP endonucleases.The ribose-phosphate backbone is then removed from theDNA by an exonuclease called deoxyribophosphodiesterase(dp-diesterase). Then the DNA polymerase and a ligasecatalyze incorporation of a specific deoxyribonucleotide intothe repaired site, enabling correct base pairing.
DNA Repair Mechanisms
• DNA repair include s a collection of processes throughwhich a cell identifies and corrects damage to its DNA
• DNA repair is essential to cell survival
• If DNA damage is irreparable then programmed celldeath (apoptosis) should ensue
• Failure to correct molecular lesions in gamete-formingcells leads to progeny with congenital mutations
• Single-strand damage repair
- Direct repair is an enzyme-catalyzed reaction thatdirectly reverses DNA damage. No template is neededto correct an altered base back to its natural state
- Base excision repair (BER) removes a damaged baseand replaces it with a normal base (Figure 9)
• DNA cross-linkers cause both interchain covalentbonds and stable bonds between the DNA strandsand nuclear proteins (e.g., platinum)
• Oxidative damage caused by oxygen radicalsaccelerating hydroxylation of guanine to8-hydroxyguanine, causing a G:C to A:T transversion
- Radiation
• Ionizing radiation can cause individual base lesions,cross-linking, or strand breakage, sometimesmediated by oxygen radicals
• Ultra violet radiation causes covalent bondingbetween adjacent cytosine and thymine basescreating pyrimidine dimers
- Viral mutagenesis involves a DNA virus, RNA orretrovirus integrating all or part of its sequence intothe human genome
• An episome is a DNA molecule separate from thechromosomal DNA and capable of autonomousreplication. It is the common status of viralparticles during viral infection
• Integration means that DNA fragments of viralorigin have become inserted into chromosomal DNA
• Epstein-Barr virus has been associated withlymphoproliferative disorder in immunocomprornisedpatients (such as post-transplantation)
• Human herpesvirus 8 has been associated withKaposi's sarcoma, Castleman's disease, body cavitylymphoma (primary effusion lymphoma), andmultiple myeloma
• Human papillomavirus has been associated withpremalignant and malignant transformation of theuterine cervix
• Inborn errors of metaboli sm
- Inborn errors comprise a large class of geneticdiseases involving metabolic disorders
- The majority of inborn errors are due to single genedefects that code for enzymes to convert intermediarymetabolites
11

1-12 Molecular Genetic Pathology
Human mismatch repair
3'- - - - - - ...JA '-- - - - - -5'S ~V
____x~ __.=x- - - -
3'--- - - ---.JA '-- - - - - - 5'5'- - 3'V
1
Excision 1 Fig. II . Homologous recombination repairs a double-strandedbreak. It allows the precise replacement of a sequence fromone allele with a sequence from the homologous allele. Thebreaks in dsDNA use a homologous dsDNA molecule as atemplate . Homologous recombination requires a homologoussequence to guide the repair.
Nonhomologous end joining
3" ---.JA '- 5'
5'- - 3'
-----3'
~---;.____--------5'/Fig. 12. NHEJ can also repair double-strand breaks in DNA.NHEJ directly ligates the breaks without a homologous template.NHEJ typically utilizes short homologous DNA sequences,termed microhomologous, to guide the repair but still results insome DNA sequence information being lost or "spliced out."
1DNA synthes is
3'-- - - - - - - - - - - - - - -5'5' 3'
Fig. 10. Mismatch repair is a cellular procedure forrecognizing and repairing insertion, deletion or misincorporation. The DNA damage is repaired by excising themis-incorporated base or segment and synthesizing a newstretch of DNA is synthesized to replace the excised segment.This process involves more than just the mismatchednucleotide itself and can lead to the removal and synthesis ofa significant piece of DNA. Also there are multiple excisionrepair systems in a single cell type .
• Double-strand break repair
- Homologous recombination uses an intact homologsequence as a template for repair of a broken DNAstrand (Figure 11)
- Non-homologous end joining (NHEJ) links the ends oftwo double-strands without needing for a homologoustemplate and regardless of sequence similarity. Just assome information is lost when splicing a movie film orcassette tape, NHEJ introduces mutations that areminimized by various failsafe mechanisms (Figure 12)
GENES
Overview
• Genes are DNA sequences that encode heritable biologiccharacteristics
- The human genome is divided into two categories,nuclear and mitochondrial genome
• DNA in the human nuclear genome encodes about30,000-40,000 different genes, much lower than previousestimates of around 100,000 genes before completion ofthe genome map
• DNA in the human mitochondrial genome encodes 37 genes
Gene Components (Figure 13)
• Promoter is a DNA fragment to which RNA polymerasebinds to initiate transcription
- Core promoter directs the basal transcription complexto initiate the transcription of the gene
• TATA box is a short sequence located within thepromoter of most genes
- TATA box has a core 5'-TATAAA-3' sequence
- The TATA box is usually found as the binding site ofRNA polymerase II
12

Principles of Clinical Molecular Biology
IEnhancer I
Polyadenation signal
IStop codon I~
1-13
Fig. 13. A gene consists of both coding and non-coding sequences. The coding sequence (open reading frame, ORF) extends froma start codon to a stop codon. Introns are non-coding sequences that will be spliced out after transcription. 5' untranslated region(UTR) is a part of mRNA located between cap site and start codon. 3' untranslated region is also a part of mRNA following codingsequence. A promoter and different regulatory motifs are located up stream of a gene. Enhancer or silencer may be locatedupstream or downstream of the gene it regulates .
• CCAAT Box (CAT box) is located at -75 and serves as amodulator for the basal transcription
- CCAAT box has a core 5'-CCAATC-3' sequence
- CCAAT box is the binding site of nuclear factor I(NF-I) and CCAAT box binding factor (CBF)
• GC box is also called Sp I box. It has consensussequences GGGCGG and is found within 100 bp fromthe transcription initiation site
- GC boxes serve as a modulators to the basaltranscription of the core promoter
• CpG sites are region s of DNA with a high frequency ofphosphodiester-linked cytosine-guanine pairs . The "r"in CpG indicates that a normal phosphodiester bondbetween nucleosides gives the the CG sequencedirection
- CpG islands are located near or within 40% ofmammalian gene promoters
- The genes with CpG islands are expressed if the CpGislands are not methylated
• Enhancers are DNA sequences that when bound bycertain factors increase transcription levels of genes
- Unlike promoters, enhancers do not have to be withinor near the genes they act on, or even located on thesame chromosome
• Silencer is a DNA sequence that can bind regulators oftranscription called repressors. The binding of repressorprevents RNA polymerase from initiating transcription
- When repressor is bound to target DNA, RNAsynthesis is decrea sed or fully suppressed
• An exon is any region of DNA within a gene that encodesa protein. Exons of many eukaryotic genes interleavewith segments of non-coding DNA (introns). MaturemRNA contains only sequentially linked exons
• Introns are sections of non-coding DNA located betweenexons, which are transcribed into RNA but are spliced outto form mRNA
• Open reading frame (ORF) is the sequence of DNA ormRNA molecule from the start codon (ATG) to a stopcodon (TAA, TAG, or TGA). An open reading frame codesfor amino acid codons that can be translated into a protein
• Boundary elements (insulator elements) are regions ofDNA that mark the 5' and 3' ends of a gene
• Gene expression is the process by which a gene 's DNAsequence is converted into the structures and funct ions ofa cell
- Protein-coding genes are translated into proteins
- Non-protein coding genes code for RNAs, (e.g.,ribosomal RNA [rRNA] genes, and transfer RNA[tRNA] genes), which usually have a structural ,regulatory or catalytic role
Functional Categories of Genes• Housekeeping genes are genes that are transcribed at a
relatively constant level and remain unaffected byenvironmental conditions
- Housekeeping gene products are necessary for cellmaintenance
• Since their expression is typically unaffected byexperimental conditions, they may be used fornormalization of other gene expression levels in thecell
• Housekeep ing genes often lack the CCAAT andTATA boxes
- Actin and glyceraldehyde 3-phosphate dehydrogenaseare example s of housekeeping genes commonly usedas control s for mRNA quantitation
13

1-14
• Facultative genes are transcribed only when needed
• Inducible gene expression is either responsive toenvironmental changes or dependent on the stage of thecell cycle
• Pseudogenes are multiple copy genes characterized bydefective copies , mostly truncated, of a functional gene
- Pseudogenes arise from gene duplication orretrotransposition
• RNA genes transcribe mRNA as their end productswithout protein translation
Cancer-Related Genes (Table 2)
• Tumor-suppressor genes prevent cell overgrowth(neoplasia)
- They are involved in cell cycle control, celldifferentiation, and apoptosis
- Tumor-suppressor gene products generally promotegenomic stability
- Tumor-suppressor gene inactivation mechanismsinclude point mutation, deletion, and epigeneticinactivation of the gene
• Proto-oncogenes are normal genes that cause a malignantphenotype either because of mutation or increasedexpression . Proto-oncogenes code for proteins to regulatecell growth and differentiation
- A proto-oncogene becomes an oncogene whenmutated, inappropriately expressed or over expressed,transforming the cell by unregulated growth anddifferentiation
• Oncogene- Oncogene products include
• Growth factors bind receptors on the cell surfaceto stimulate cell proliferation or to controldifferentiation
• Receptors are proteins on the cell surface, withinthe cytoplasm or in the cell nucleus for bindingspecific molecules (ligands) to initiate a cellularresponse
• Protein kinases chemically add phosphate groups tospecific amino acids of substrate proteins. Thisprocess usually results in a functional change of thetarget protein resulting in changed enzyme activity,altered cellular location, or modified associationwith other proteins
• Receptor tyrosine kinases are membrane-boundenzymes to transfer a phosphate group from ATP toa tyrosine residue in a protein. The tyrosine kinasebinding hormones and growth factors are generallygrowth-promoting and mitogenic agents, such asepidermal growth factor receptor (EGFR)
• Cytoplasmic tyrosine kinases are non-receptortyrosine kinases (TK) to regulate many cellularprocesses, such as inducing gene of Rouse sarcoma
14
Molecular Genetic Pathology
virus (Src-family), SYK-Zeta-chain associatedprotein kinase 70 (Syk-ZAP-70 family), andBruton's tyrosine kinase (BTK family) oncogenesbelongs to the cytoplasmic tyrosine kinases group.The bcr-abl transcript (fusion gene of thePhiladelphia chromosome in chronic myelocyticleukemia (CML) is also a tyrosine kinase . Thebcr-abl fusion gene kinase activates mediators ofthe cell cycle regulation system, leading to a clonalmyeloproliferative disorder
• Regulatory GTPases are a large family of enzymesthat bind and hydrolyze GTP (guanosinetriphosphate) existing in GTP-bound and -unboundstates. They play important roles in the followingcellular processes:
• Signal transduction at the intracellular domain oftransmembrane receptors
• Protein biosynthesis at the ribosome
• Control of differentiation during cell division
• Translocation of proteins through membranes
• Transport of vesicles within the cell
• Ras oncogene produces a small regulatoryGTPase important as a molecular switch for avariety of signal pathways. Ras controls suchprocesses as cytoskeletal integrity, cellproliferation, adhesion, apoptosis, and migration
• Cytoplasmic serine/threonine kinase phosphorylatesthe hydroxyl group of serine or threonine . The Rajkinase, and cyclin-dependent kinases belong to theserinelthreonine kinase family
• Adaptor proteins are small accessory proteins,which lack intrinsic enzymatic activity but bindsignal transduction pathway components, drivingthe formation of active protein complexes
• Transcription factors mediate the binding of RNApolymerase to DNA and initiation of transcription.A transcription factor may work to either stimulateor repress transcription of a gene
Regulation of Gene Expression
• Regulation of gene expression controls the amount andappearance agenda of a gene's functional product
- All steps of gene expression can be modulated
- Regulation of gene expression is the basis for celldifferentiation, diversity, and adaptation
• Cis-action factors are short regulatory sequences locatedwithin the promoter or in the vicinity of a gene'sstructural portion. Cis-sequences facilitate thetranscription of adjacent polypeptide-encoding sequences
• Trans-action factors bind to the cis-acting sequences tocontrol gene expression
• Enhancer is a short region of DNA that upregulatestranscription levels of genes. Enhancer sequences areactive when bound to trans-action factors

Principles of Clinical Molecular Biology
• Response element is a short sequence of DNA within thepromoter of a gene that can bind to a specific hormonereceptor complex and regulate transcription of genessubject to that hormone
SignalTransduction• A signal transduction pathway is a sequence of enzymes
and second messengers by which a receptorcommunicates with the cell nucleus
• The signal transduction pathway "translates" the receptorligand message at the surface into a cellular response inthe nucleus
- abl and ras are signal transducers
• Transcription factors
1-15
- A transcription factor is a molecule that initiatestranscription of DNA in the eukaryotic nucleus
- Transcription factors interact with promoter orenhancer sequences either by binding directly to DNAor by interacting with other DNA-bound proteins
- myc is an example of a transcription factor thatactivates expression of many genes by binding toconsensus sequences
• Programmed cell death regulators are molecules thatprevent apoptosis . Activation of these regulators leads toovergrowth of abnormal cells
- bcl-2 is an example of a programmed cell deathregulator that governs mitochondrial outer membranepermeability and suppresses apoptosis
CHROMOSOMES
Fig. 14. Structure of a typical human chromosome.
- Heterochromatin is a darkly stained and tightly packedform of DNA. Its major biologic characteristic is thatit is not transcribed
• Chromatin composition
- Histones are the major chromatin binding proteins.They act as spools around which DNA winds
• Histones playa role in gene regulation
• Histones H2A, H2B, H3, and H4 form octamers(two of each) with a cylindrical shape (Figure 15)
Overview• A chromosome is an enormous macromolecule into which
somatic DNA is packaged in eukaryotic cells. Three billionbase pairs of nucleotides (a complete set of DNA) aredivided among 46 chromosomes, each containing manygenes, regulatory elements, and intervening nucleotidesequences (Figure 14)
• Chromosomes are found only in the eukaryotic nucleusand can be seen only during nuclear division
• During most of the life cycle, the genetic materialoccupies areas of nuclei in the form of chromatin, andindividual chromosomes cannot be distinguished
• In eukaryotes, the basic function of the chromosomeis to package and compress the DNA, exposing specificgenes for transcription during certain phases of thecell life span
Chromatin• Chromatin is the form of genetic material existing during
interphase of eukaryotic cells and is made up of DNAand protein
• Chromatin can be seen with the light microscope afterstaining with nuclear stains
• Chromatin is a packaged state of DNA in a small volumeto strengthen the DNA, to allow mitosis and meiosis, andto serve as a mechanism for expression control
• Chromatin functions as a gene regulator
- The changes in chromatin structure are effectedmainly by methylation (DNA and proteins) andacetylation (proteins)
- Euchromatin is a loosely packed form of chromatinthat is involved in active transcription or regulationand is lightly stained by nuclear stains
Telomere -e:
Telomere -e:
1p
Centrome re
q
15

1-16
Fig. 15. Nucleosomes are the fundamental repeating subunitsof all eukaryotic chromatin. They package DNA intochromosomes inside the cell nucleus and control geneexpression . The DNA winding around the nucleosome coreparticle consists of about 146 bp of dsDNA wrapped in 1.65left-handed superhelical turns around complexes of the fourhistone proteins known as the histone octames. The DNAhanging between two nucleosome cores is typically 55-bp longand is known as linker DNA.
• When DNA winds 1.65 times around a histoneoctamer a nucleosome results
• Each nucleosome contains 146 bp
• The nucleosomes are stacked and further coiledinto a 30-nm fiber, which makes up thechromosome residing in the cell nucleus
• Linker DNA is the DNA hanging between twonucleosomes, typically 55-bp long
• Histone-DNA interaction regulates geneexpression. Acetylation of histone modulates geneexpression and leads to transcription activation.The extent of interaction between histone andDNA is affected by the degree of histoneacetylation
• Histone acetylation is the process in which chargedlysine side chains are acetylated, leading to reducedaffinity between histone and DNA. Afteracetylation, RNA polymerase and transcriptionfactors have better access to the promoter
Chromosomes• Chromosome structure
- Each chromosome has two short arms (p), two longarms (q), one centromere, and four telomeres
• The centromere is the constricted region of achromosome, which has a special sequence andstructure for attachment to the spindle filamentduring M-phase and for separation of chromosomesduring mitosis (Figure 14)
16
Molecular Genetic Pathology
• The centromere divides the chromosome into fourarms
• The two equal short arms are designated "p"(petite)
• The two equal long arms are designated "q"(follows p in the Latin alphabet)
• Telomere: (see Chapter 7, Telomere section)
• Chromosome grouping
- Chromosomes are numbered and grouped according totheir morphologic characteristics
- Chromosomes are numbered according to their relativesizes from largest to smallest. The position of thecentromere determines chromosome grouping
• Group A have nearly equal p and q arms whereasgroup E have the centromere almost at thetelomere
- Chromosome identification is confirmed by the bandingpattern unique to each chromosome (Figure 16)
• Chromosome number
- Human cells contain 46 chromosomes (23 from eachparent) including 22 pairs of autosomes and one pairof sex chromosomes
- The number of chromosomes doubles during celldivision
• Meiosis is a process allowing one diploid cell todivide in a special way into four haploid cells ineukaryotes
• Mitosis is the process by which a cell separates itsduplicated chromosomes into two identical sets ofchromosomes
• Ploidy is the number of homologous sets ofchromosomes in a cell
• Haploidy (monoploidy) is the number ofchromosomes in the gamete of an individual(23 in a human) . Haploid chromosomes haveonly one short and one long arm
• Diploidy is the normal state of chromosomesin a cell, with two copies of each chromosome,one from each parent. The two chromosomesin a pair are said to be homologous
• Polyploidy is the state of cells with extrachromosomes beyond the basic set of pairedchromosomes
• Aneuploidy is a condition in which the numberof chromosomes is abnormal owing either toextra or missing chromosomes. The number ofchromosomes in an aenuploide cell cannot be amultiple of the haploid set (Figure 17)
• Monosomy is a type of aneuploidy with at leastone missing parental chromosome (Figure 18)
• Trysomy is a type of aneuploidy with one extrachromosome added to a pair of homologouschromosomes

Princ iples of Clinical Molecular Biology 1-17
Human Genome and Chromosomes
Genome size:3.2x109 nucleotides
22 autosomes and 2 sexchromosomes
Diploid (2N):(1-22)x 2 + XV/XX = 46
(\J 35,000genes 2
~y
x13
150 millionnucleotide pairs
oFig. 16. Chromosomes are grouped according to their relative size, the position of their centromere, and banding patterns .
•..~ , ' I'·-- -... ~ '-
\ ,I ~ 1' ·, - >, '\.~. I . ,. ~
. ' •• , # /. \., ., '. . ..\ I. .. -
I
Fig. 17. Aneuploidy is a condition in which the number ofchromosomes is not a multiple of the haploid set due to gainingor losing chromosomes. The figure shows a fluorescent probechromosome painting of tumor cell chromosomes featuring aseries of chromosome gains and loses.
Fig. 18. Monosomy is a type of aneuploidy with loss of onechromosome from a pair in the cell 's diploid chromosome set.Fluorescence in situ hybridization shows the loss of onechromosome in these cells indicated by having only onesignal present in each nucleus.
17

1-18
• Structural alterations of chromosomes (see details inChapter 2)
- Inversion occurs when a chromosome segment is flippedend to end. Inversion is designated by the symbol inv
Reciprocal translocation is a chromosomalrearrangement caused by the interchange of chromosomesegments between non-homologous chromosomes .Reciprocal translocations are denoted by the symbol tfollowed by parentheses showing the exchangedchromosome breakpoints separated by a semicolon
Isochromosome is a chromosome which has lost oneset of its arms, either p or q, and replaced them withan exact copy of the other arms. Isochromosomes thushave four identical arms , either p or q. Isochromosomeis denoted by the symbol i
Molecular Genetic Pathology
- Ring chromosome is a chromosome that is formedwhen the telomeres have been lost, and the ends ofarms fuse together to form a ring. A ring chromosomeis denoted by the symbol r
• Fragile sites are chromosome regions that are poorlyconnected to the rest of the chromosome
- Fragile sites are often rich in CGG or CGC repeats andare inherited like a gene and break away frequently
- Double chain breaks in fragile sites lead to the loss ofgenetic material
- Fragile sites are especially prone to breakage whencells are cultured under conditions that inhibit DNAreplication or repair
Selected tumors with chromosomal anomalies (Table 2)
Table 2. Selected Tumors with Commonly Found Chromosomal Anomalies
Tumor Common chromosome anomalies Genes involved
Epithelial tumors
Basal cell carcinoma 9q22 .3 PTCH
Clear cell renal carcinoma 3p25-26 VHL
Translocation renal cell carcinoma t(X; I)(p 11.2;q21) PRCC-TFE3
t(X; 17)(p11.2-q25) ASPL-TFE3
t(X;I)(p11.2;p34) PSF-TEFJ
Papillary renal cell carcinoma Gain 7, 17, loss Y, and 4 -
Hereditary papillary renal cell cancer 7q31 c-MET
Breast cancer Iq -
17q21 BRCA1, Her-2/neu
13ql2 BRCA2
del(l6q) -
Colorectal cancer del(l7p) TP53
12p Ras
3pl4 FH1T
5q21-22 APC
18q21 DCC, SMAD4
Lung cancer del(3p) FH1T
13q RB
9p21 P16
17p TP53
(Continued)
18

Principles of Clinical Molecular Biology 1-19
Table 2. (Continued)
Tumor Common chromosome anomalies Genes involved
Prostate cancer t(21;21)(p22.2;q22.3) TMPRSS2-EGR
del(8pI2-2l) NKX3.1
lq24 HPCI
Xq27-28 HPCX
Xqll AR
del(lOq24) PTEN
Trisomy 7 -
Loss ofY -
Bladder transitional cell carcinoma gain 3,7, 17,del(9p21) P53, Pl6
(UroVysion panel)
Medullary thyroid carcinoma lOql1.2 RET
Papillary thyroid carcinoma IOqll-q13 RET
inv(1) NTRKI-TPM3 (TRK)
Mesothelioma del(3p21) CTNNBI
Ovarian papillary cystadenocarcinoma t(6;14) -
Granulosa cell tumor and Brenner tumor trisomy 12 -
i(12p) -
Testicular germ cell tumors i(12p) -
12p overrepresentation -
Wilm's tumor del(1 lpI3) WTI
Soft tissue tumors
Alveolar soft-part sarcoma t(X; 17)(p II ;q25) TFE3-ASPL
Alveolar rhabdomyosarcoma t(2; 13)(q35;q 14), PAX3-FKHR,
t(1; 13)(p36;q14) PAX7-FKHR
Clear cell sarcoma (melanoma t(12;22)(q 13;q12) EWS-ATFIof soft part)
Dermatofibrosarcoma protuberans t(17;22)(q22 ;q13) COLlAI-PDGFBand giant cell fibroblastoma
Myxoid chondrosarcoma t(9;22)(q22 ;q12) EWS-CHN
Lipoma t(3; 12)(q27;q 13) HMGIC-LPP
Lipoblastoma 8q rearrangement -
Myxoid liposarcoma t(12;16)(q13;pll) CHOP-FUS
t(12;22)(q 13;q12) EWS-CHOP
Well-differentiated liposarcoma Ring chromosome 12 -
(Continued)
19

1-20 Molecular Genetic Pathology
Table 2. (Continued)
Tumor Common chromosome anomalies Genes involved
Ewing's sarcoma/primitive t(l i ;22)(q24;q12), EWS-FLl l,
neuroectodermal tumor t(21;22)(q22;q 12) EWS-ERG
Desmoplastic small round cell tumor t(li ;22)(p13;q 12) EWS-WTl
Synovial sarcoma t(X;18)(pll ;qI I) SIT-SSXl
t(X;20) -
Infantile fibrosarcoma and t(l2; l5 )(p13;q25) ETV6-NTRK3congenital mesoblastic nephroma
Inflammatory myofibroblastic tumor t( I ;2)(q22;p23) TPM3-ALK
t(2;I9 )(p23;p13) TPM4-ALK
Gastrointestinal stromal tumor 4qll -2l c-kit exon II
Hemangiopericytoma t(l2;19) -
Uterine leiomyoma t(l 2;14)(q l3 -I5;q24.I ) HMG1C
Endometrial stromal sarcoma t(7;17)(p l5-p2I ;q 12-q2I ) JAZFl-JJAZI
Leiomyosarcoma del(l p) -
Pleomorphic adenoma t(3;8)(p I2;q 12) FGFR1-FlM
Aneurysmal bone cyst I7p rearrangement -Desmoplastic fibrobla stoma and t(2; II ) -
fibroma of tendon sheath
Melanoma del(9p21) CDKN2
I2qI4 CDK4
del(22q) -
Neural/neuroendocrine tumors
Acoustic neuroma 22qI2.2 NF2
Schwan noma deI(22qI3) NF2
Meningioma del(22q II-q 13) NF2
Monosomy 22 -
Gliobl astoma multiforme Trisomy 7 EGFR gene amplificationMonosomy 10, 22 (7pII )t(lO;19)(q24;qI3)
Medulloblastoma del(lOq) PTEN and DMBTl (l Oq)
i(l7q) -
del(17p13.2) -
Trisomy 8 -
Neuroblastoma 2p N-Myc amplificationdel( Ip31-32) (homogenous staining region
and double minutes)
(Continu ed)
20

Principles of Clinical Molecular Biology 1-21
Table 2. (Continued)
Tumor Common chromosome anomalies Genes involved
Oligodendroglioma del(lp36) TP73
del(l9q13) PEG3
Retinoblastoma del(l3qI4) RB
Pheochromocytoma del(22q13) SLCI
del(lp11-36) RIZI
Lymphomas/leukemia
Burkett's lymphoma t(8;14)(q24;q32), c-myc-IgH
t(8;22)(q24 ;qll) c-myc-IgL
t(2;8)(p 12q24) c-myc-IgK
Follicular lymphoma t(14;18)(q32;q21) IgH-BCL2
Mantle cell lymphoma t(lI;14)(qI3;q32) IgH-BCLl (cyclin 01)
llq ATM mutation or deletion
del(l3q14) -
Trisomy 12 -
del(l7p) -
Mucosa-associated lymphoid t(ll; 18)(q21;q21) API2-MALTltissue (MALT) lymphoma Trisomy 3
Diffuse large cell lymphoma t(l4;18)(q32;q2l) IgH-BCL2
t(3;14)(q27;q32) BCL6-1gH
Anaplastic large cell lymphoma t(2;5)(p23;q35) NPM-ALK
Lymphoplasmacytic lymphoma t(9;14)(p13;q32) PAX5
Myelodysplastic disorder del(5q) -
Trisomy 8 -
Monosomy 7 -
del(7q) -del(l7p) -
del(20q) -Chronic myelogenous leukemia t(9;22)(q34;q11) BCR-ABL
Acute myelogenous leukemia (AML)-M2 t(8;2l )(q22;q22) AMLl-ETO
Acute promyelocytic leukemia -M3 t(l5 ;17)(q22;q2l) PML-RARa
AML-M4eo inv(l6)(p13;p22) MYHII-CBFB
AML-M4,M5 t(l1 ;19) MLL-ENL
llq23 MLL
(Continued)
21