-
7/29/2019 MKG Broschuere E.pdf En
1/401
Therapy Concepts orOral & Maxilloacial Surgery
LEADING REGENERATION
-
7/29/2019 MKG Broschuere E.pdf En
2/40
-
7/29/2019 MKG Broschuere E.pdf En
3/403
Geistlich a Company with Tradition
The history o the company Geistlich began in 1851 with the
manuacturing o glues rom
bones. Later, bones and other animal tissues were processed to
yield ower ertiliser and
highquality gelatine or oodstus. In the ollowing years, the
company expanded into
the eld o pharmaceuticals and established a second plant in
Wolhusen near Lucerne.
In 1983, a new business idea was stimulated by a report rom
Proessor Philip Boyne
on the successul reconstruction o crushed jaws with cattle bone.
This led to the birth
o Geistlich BioOss: a highly puried anorganic bone material with
a high similarity to
human bone or eective bone regeneration.Thereater, a
manuacturing process to ree the bone o organic constituents,
while
maintaining its natural microstructure and anorganic
composition, was developed and
patented. Already during the initial discovery and development
phases there was close
cooperation with various experts and leading clinics. This laid
the oundation or todays
sound scientic evidence base which presently consists o more
than 600 publications.
In 1996, another undamental innovation rom Geistlich changed the
market o bone and
tissue regeneration substantially through the introduction o
Geistlich BioGide: the rst
natural and ully resorbable collagen membrane now replacing the
nonresorbable ePTFE
membrane in a majority o indications. The natural composition o
this membrane, which
is very similar to human collagen, proved to be a key parameter
or its positive eect on
bone and sot tissue healing processes.
Nowadays, Geistlich BioOss
and Geistlich BioGide
have become a benchmark in dentalbone regeneration, conrmed by
more than 20 years o clinical experience and an ever
increasing number o scientic publications. In addition, the
range o applications are
continuously being expanded within the dental, maxilloacial, and
orthopaedic elds.
With the brochure at hand we would like to oer you an overview
on current treatment
methods or complex cases o bone regeneration in the oral and
maxilloacial areas.
Your Geistlich Biomaterials Team
-
7/29/2019 MKG Broschuere E.pdf En
4/404
Acknowledgments:
Geistlich Biomaterials wishes to thank Dr. Z. Krol, Pro. Dr. Dr.
R. Sader and Pro. Dr. Dr. H.F. Zeilhoer Hightech
Research Center o CranioMaxilloacial Surgery, University
Hospital Basel or kindly delivering the oblique view o the
cranioacial CT, visualized by volume rendering method, which
appears on the cover and in the outlook.
We acknowledge all the authors o the Clinical Cases or their
valuable contribution and eorts. Geistlich Biomaterials
thanks Blackwell Publishing Wiley InterScience, RC Libri,
Quintessence Publishing, and Quintessenz Verlag or the
copyright permissions.
-
7/29/2019 MKG Broschuere E.pdf En
5/405
Index
Scientic Background06 Bone and Bone Substitutes
06 Clinical Facts
07 Quality o Lie
08 High Therapy Saety with a Membrane
Clinical Cases10 Cawood Classication
12 Cawood Class IV
12 Dr. J.J. Aranda
13 Dr. K.H. Bormann, Pro. Dr. Dr. N.C. Gellrich
14 Pro. Dr. D. Buser, PD Dr. T. von Arx
15 Pro. Dr. C. Hmmerle
16 Dr. G. Iglhaut
17 Pro. Dr. C. Maiorana
18 Pro. Dr. I. Urban
19 Cawood Class V
19 Pro. Dr. M. Chiapasco
20 Dr. P. Felice MD/DDS, Pro. L. Checchi MD/DDS, Pro. M.
Marchetti MD/DDS21 Dr. U. Grunder
22 Dr. M. Merli
23 Pro. Dr. A.R. Paranque
24 PD Dr. Dr. K.A. Schlegel
25 Pro. Dr. Dr. R. Schmelzeisen, Pro. Dr. Dr. R. Gutwald,
Dr. Dr. A. Stricker, Dr. M. Vogeler, Dr. S. Sauerbier
26 Pro. Dr. M. Simion, Dr. I. Rocchietta
27 Dr. M. Steigmann
28 Dr. S. Stbinger, Pro. Dr. Dr. R. Sader
29 Dr. T. Testori
30 Cawood Class VI30 Dr. Dr. C. Glatzer, Dr. O. Schwerdtner
31 Pro. Dr. Dr. T. Iizuka
32 PD Dr. Dr. C. Jaquiry, Dr. N. Gabutti, Pro. Dr. Dr. H.F.
Zeilhoer
33 Univ.Pro. Dr. C. Krenkel, Dr. Dr. S. Enzinger
34 Pro. Dr. Dr. H. Terheyden
35 Dr. A. Triaca, Dr. Dr. R. Minoretti, Dr. D. Kraus
Product Range36 Geistlich BioGide / Geistlich BioOss
Outlook
-
7/29/2019 MKG Broschuere E.pdf En
6/406
Bone and Bone SubstitutesBone is made up o several types o
tissues. The primary part being the mineralized tissue that is
composed mostly o
calcium hydroxylapatite and collagen I which gives it rigidity
and a threedimensional trabecular structure. Other types o
tissue ound in bones include marrow, endosteum and periosteum,
nerves, blood vessels and cartilage. Additionally, bone
tissue consists o living cells and various proteins embedded in
the mineralised matrix that makes up the osseous tissue.
Bone grating procedures are oten needed to replace missing bone
at one site with material rom another site. The bone
material may stem rom the patients own body autograt, rom human
cadavers allograt, rom animal origin xenograt,
or rom synthetic material. Allograts and xenograts are
principally unprocessed bone substitute mostly obtained rom
bone banks.
Geistlich BioOss, dierent rom all the above mentioned materials,
is a highly puried xenogeneic bone substitute
completely void o organic tissue and solely made up o the
mineral component o bovine bone.
Clinical FactsVolume Preservation:Presently, autogenous bone is
irreplaceable in the treatment o large bony deects and is regarded
as
the gold standard or bone augmentations. However, it has been
scientically proven that autogenous bone grats show a
stronger resorption than a mixture o a slow resorbable bone
substitute with autogenous bone.
Schlegel and coworkers claim that the augmented bone volume is
preserved in the sinus cavity lled with a mixture o
Geistlich BioOss, while the height o a purely autogenous bone
grat diminishes markedly.
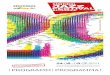
Comparison o horizontal augmentation techniques shows lower
resorption rates, i the autogenous block grat is covered
with Geistlich BioOss and Geistlich BioGide Fig. 1.36
Alternatively, using only these biomaterials or horizontal
augmentations is an eective treatment and avoids completely the
harvest o autogenous bone.
Scientic Background
Resorption(%)
autog. block+
Geistlich Bio-Oss
peripherically 4
autog. block+
autog. chipsperipherically
+
Geistlich Bio-Gide 5
autog. block+
Geistlich Bio-Oss
cover 3
autog. block+
Geistlich Bio-Oss
cover
+
Geistlich Bio-Gide 6
autog. block+
autog. chipsperipherically 3
Fig. 1: Resorption rate o the autogenous blockgrat in dierent
augmentation techniques.
Garg AK. Knochen / Biologie, Gewinnung, Transplantation in der
zahnrztlichen Implantologie. Berlin: Quintessenz 2006. Schlegel KA
et al. Histologic ndings in sinus augmentation with autogenous bone
chips versus a bovine bone substitute.
Int J Oral Maxilloac Implants 2003 JanFeb;18(1):53-8. Maiorana C
et al. Reduction o autogenous bone grat resorption by means o
biooss coverage: a prospective study.
Int J Periodontics Restorative Dent 2005;25(1):19-25. Proussaes
P et al. The use o ramus autogenous block grats or vertical
alveolar ridge augmentation and implant placement: a pilot
study.
Int J Oral Maxilloac Implants 2002 MarApr;17(2):238-48.
Proussaes P. Clinical and histologic evaluation o the use o
mandibular tori as donor site or mandibular block autograts: report
o three cases.Int J Periodontics Restorative Dent 2006
Feb;26(1):43-51. von Arx T & Buser D. Horizontal ridge
augmentation using autogenous block grats and the guided bone
regeneration technique with collagen membranes:
a clinical study with 42 patients. Clin Oral Implants Res
2006;17(4):359-66. Hmmerle CHF et al. Ridge augmentation by
applying bioresorbable membranes and deproteinized bovine bone
mineral: a report o twelve consecutive cases.
Clin Oral Implants Res 2008;19(1):19-25.
-
7/29/2019 MKG Broschuere E.pdf En
7/407
Implant survival rates:In the past years, several clinical
studies and metaanalysis have evaluated the implant survival
rate
depending on the urnishing bony support in sinus lit procedures.
The survival rate increases ater augmentation with
bone substitutes alone or in a mixture with autogenous
particulate grats, as compared to sites augmented with
autogenous
bone only Fig. 2a,b.810 Generally it has been shown that the
implant survival in augmented bone is similar to the survival
rate in sites where an augmentation was not needed.
Therapeutic Flexibility:Autogenous bone resorption narrows the
therapeutic time window or implant placement.
The slowresorbing matrix structure o Geistlich BioOss increases
the stability o the grat and prevents premature
resorption o the newly ormed bone. The augmented volume is
preserved over a prolonged period and so extends
the therapeutic window.
Quality o LieNumerous clinical studies report rom 18% up to 50%
o patients with diminished sensitivity
ater bone harvesting rom the chin. Joshi et al. state 20% and
25% o donor site morbidity
ater bone harvesting rom the ramus and the iliac crest,
respectively.
The addition o a bone substitute may render the access o a
second surgical site unnecessary,
which, in turn, increases the quality o lie.
Wallace SS & Froum SJ. Eect o maxillary sinus augmentation
on the survival o endosseous dental implants.
A systematic review. Ann Periodontol 2003;(1):328-43. Aghaloo TL
& Moy PK. Which hard tissue augmentation techniques are the
most successul in urnishing bony support or implant placement?
Int J Oral Maxilloac Implants 2007;22Suppl:49-70.
Del Fabbro M et al. Systematic review o survival rates or
implants placed in the grated maxillary sinus.Int J Periodontics
Restorative Dent 2004 Dec;24(6):565-77. von Arx T et al.
Neurosensory disturbances ollowing bone harvesting in the
symphysis: a prospective clinical study. Clin Oral Implants Res
2005;16(4):432-9. Raghoebar GM et al. Morbidity o chin bone
harvesting. Clin Oral Implants Res 2001 Oct;12(5):503-7. Misch CE.
Implant dentistry. Dent Today 2002 Nov;21(11):62.Joshi A &
Kostakis GC. An investigation o postoperative morbidity ollowing
iliac crest grat harvesting. Br Dent J 2004 Feb 14;196(3):167-71;
discussion 155.
Fig. 2b: The implant survival rate is signicantly higher
inaugmentations with biomaterials compared to those withautogenous
bone only.
. . .
bone substituteautogenous bone autogenous bone+ bone
substitute
Implantsurvivalrate(%)
Fig. 2a: Implant survival rates in external sinus oor
elevationdier with augmentation materials 5128 implants,
ollowup12102 months.
*Note: the 22 reerenced studies with xenogeneic materialswere
conducted with Geistlich BioOss.
100
95
90
85
80
75
70
65
Implantsurvivalrate(%)
88.0 92.0 93.3 95.6
synthetic iliac crest autogenous allogeneic xenogeneic* n=190)
(n=1845) (n=2904) (n=189) (n=443)
0
81.0
-
7/29/2019 MKG Broschuere E.pdf En
8/408
High Therapy Saety with a MembraneThe use o a membrane or the
regeneration o bone and sot tissue is the essential component o the
Guided Bone
Regeneration GBR and Guided Tissue Regeneration GTR concept. The
membrane perorms several important unctions
and orms a basis or predictable clinical results. An optimal
barrier unction, stabilisation o the augmentate, and supportive
properties or excellent wound healing are all crucial
prerequisites or high therapy saety and an optimal outcome in
the
aesthetic zones.
More bone:Recent animal experiments and clinical studies have
analysed the new bone ormation with and without
the use o a membrane. Gielkens et al. conclude that bone
ormation is signicantly higher in the presence o Geistlich
BioGide, than in its absence, a nding also reected in the
clinical trial results o Wallace and coauthors.
Higher bone density: Kim et al. show in the dog model that the
combination o Geistlich BioOss and Geistlich BioGide
leads to signicantly higher bone density in GBR procedures than
Geistlich BioOss alone compare Figure 3.
Less Resorption:In horizontal augmentations, scientic evidence
demonstrates that the autogenous block undergoes
less resorption, when combining Geistlich BioOss with Geistlich
BioGide compared to the same treatment without
Geistlich BioGide von Arx 2006, Maiorana 2005.
Enhanced Wound Healing: Vascularization is critically important
in the early phases o successul wound healing. Thereore,
the requirements proposed or an adequate barrier in GBR/GTR are,
among others, tissue integration, nutrient transer
and biocompatibility.,
Clinical studies comparing dierent membranes conclude that the
resorbable collagen membrane Geistlich BioGide
shows a lower incidence o wound dehiscencies., In case o a
dehiscence the wound heals uneventully.
Bonedensity()
weeks weeks
Control
Geistlich Bio-Oss
Geistlich Bio-Oss and Geistlich Bio-Gide
.
.
.
.
Fig. 3: Bone density measured by dental CT postoperatively 100%
is intact adjacent alveolar bone.The extraction socket sites were
treated with i Geistlich BioOss, ii Geistlich BioOss andGeistlich
BioGide, or iii neither Geistlich BioOss nor Geistlich BioGide
control.
Gielkens PF et al. Vivosorb, BioGide, and GoreTex as barrier
membranes in rat mandibular deects: an evaluation by
microradiography and microCT.
Clin Oral Implants Res 2008;19(5):516-21. Wallace SS et al.
Sinus augmentation utilizing anorganic bovine bone BioOss with
absorbable and nonabsorbable membranes placed over the lateral
window:
histomorphometric and clinical analyses. Int J Periodontics
Restorative Dent 2005;25(6):551-9. Kim M et al. Eect o bone mineral
with or without collagen membrane in ridge dehiscence deects
ollowing premolar extraction. In Vivo 2008 MarApr;22(2):231-6.
Lakey LA et al. Angiogenesis: Implications or tissue repair. In:
Davies JE, ed. Bone Engineering. Toronto: Em Squared Incorporated
2000;137-142.
Hardwick R et al. Membrane design criteria or guided bone
regeneration o the alveolar ridge. In: Buser D, et al. Guided bone
regeneration in implant dentistry.Hong Kong: Quintessence
1994;101-136. Tal H et al. Longterm biodegradation o crosslinked
and noncrosslinked collagen barriers in human guided bone
regeneration.
Clin Oral Implants Res 2008;19(3):295-302. Zitzmann NU et al.
Resorbable versus nonresorbable membranes in combination with
BioOss or guided bone regeneration.
Int J Oral Maxilloac Implants 1997;12(6):844-52.
-
7/29/2019 MKG Broschuere E.pdf En
9/409
Reliable Barrier Function and Biocompatibility: Alteration o
natural collagen structures by crosslinking reduces the
enzymatic degradation rate at the cost o decreased
biocompatibility, as seen in Figure 5 adapted rom Rothamel
2005.
The literature does not report a dierence in bone ormation in
relation to the duration o the barrier unction. Due to
the natural bilayer structure and its similarity to human
collagen, Geistlich BioGide leads to optimal bone ormation
as well as excellent wound healing. Native collagen is resorbed
enzymatically through an irritationree process and
consequently shows signicant less dehiscences than crosslinked
collagen.
Duration oBiodegra
dation
Biocompatibility, tissueintegration,
vascularization
Geistlich BioGide
Crosslinked membranes
Nonresorbable membranesFig. 5: Geistlich BioGide oers the
optimalbarrier unction while providing the highest
level o biocompatibility based on Rothamel2005.
AT EL ML IL AT EL ML IL AT EL ML IL
Fig. 4: Immunohistochemical stainings 2 weeks ater implant.
Complete transmembraneous vascularization with Geistlich Bio
Gide
a. Angiogenesis merely reached the external layer o the
respective membrane bodies o b BioMend Extend and cTutoDent
original magnication 20x. AT: adjacent tissue; EL: external layer;
ML: middle layer; IL: internal layer. Arrows indicatethe ormation o
blood vessels in the respective layers.
a b c
Schwarz F et al. Angiogenesis pattern o native and crosslinked
collagen membranes: an immunohistochemical study in the rat.Clin
Oral Implants Res 2006;17(4):403-9. Schwarz F et al.
Immunohistochemical characterization o guided bone regeneration at
a dehiscencetype deect using dierent barrier membranes:
an experimental study in dogs. Clin Oral Implants Res 2008
Apr;19(4):402-15. Rothamel D et al. Biodegradation o dierently
crosslinked collagen membranes: an experimental study in the rat.
Clin Oral Implants Res 2005 Jun;16(3):369-78. Becker J. Interview:
Is a long barrier unction necessary?. Geistlich News
2007;2:28-29.
Predictable Outcome:The use o a membrane to cover the lateral
window in sinus lit has been correlated with a higher
implant survival rate in a systematic review and metaanalysis.
Thus, a more predictable outcome can be expected due to
consistently better bone ormation obtained using a membrane.
As seen rom the below immunohistochemical evaluations in a rat
model, Geistlich BioGide shows a homogeneous angi
ogenesis pattern and transmembraneous vascularisation ater two
weeks Fig. 4. Other collagen membranes tested do
not vascularise until 4 to weeks, some not even ater 24
weeks.,
-
7/29/2019 MKG Broschuere E.pdf En
10/4010
Clinical Cases
Cawood ClassicationIn 1988, Cawood and Howell established a
classication o edentulous jaws that has been generally accepted
over the
years. Such a classication serves to simpliy description o the
residual ridge and thereby aid selection o the appropriate
surgical and prosthodontic technique.
Arising rom their morphological studies o edentulous jaws,
Cawood and Howell concluded that i basal bone does not
change shape signicantly unless subjected to harmul local eects
and ii alveolar bone changes shape signicantly
ollowing a predictable pattern.
The most commonly observed changes in shape o the alveolar
process are summarised or the mandible Fig. a,b
and or the maxilla Figure 7a,b.
Cawood JI & Howell RA. A classication o the edentulous jaws.
Int J Oral Maxilloac Surg 1988 Aug;17(4):232-6.
Posterior Mandible
Fig. b: Classication o posterior mandible. Basal bone and
alveolar bone in blue and white, respectively.
Anterior Mandible
Fig. a: Classication o anterior mandible. Basal bone and
alveolar bone in blue and white, respectively.
-
7/29/2019 MKG Broschuere E.pdf En
11/4011
Descriptive classications o the alveolar bone changes derived
rom the composite diagrams:
Class I dentate
Class II immediately postextraction
Class III wellrounded ridge orm, adequate in height and
width
Class IV knieedge ridge orm, adequate in height and inadequate
in width
Class V at ridge orm, inadequate in height and width
Class VI depressed ridge orm, with some basalar loss evident
Although this classication was originally based on the
observations o edentulous jaws, it can also be used to describe
deects in partially edentulous jaws, taking into account that
the transitions between classes are gradual.
The clinical cases presented subsequently show dierent therapy
concepts in partially or ully edentulous jaws or oral and
maxilloacial deects belonging to Cawood Class IV, V, or VI.
Anterior Maxilla
Posterior Maxilla
Fig. 7a: Classication o anterior maxilla. Basal bone and
alveolar bone in blue and white, respectively.
Fig. 7b: Classication o posterior maxilla. Alveolar bone in
blue.
-
7/29/2019 MKG Broschuere E.pdf En
12/4012
1 CT-scan images o the recipi
ent area.
2 Intrasurgical view o the reci
pient area. Note the severehorizontal ridge resorption.
6 Two layers o Geistlich BioGide, xed with tacks, coverthe
recipient area. This provides protection against a potential sot
tissue enestration and also rom an eventualresorption o the
grats.
3 Intrasurgical view o the do
nor site lled with GeistlichBioOss. A single ap waselevated
including receptorand donor areas.
4 Autogenous bone grat placed
and xed in its correct position at the recipient area.
5 Geistlich BioOss covers theblock in order to achieve asot
contour o the gratedarea. This avoids potentialcomplications during
thehealing process and the collapse o the membrane.
7 Reentry surgery ater months, demonstrating optimal bone
regeneration.
8 Panoramic Xray ater imimplant placement.
Cawood Class IV
ConclusionWithin the available treatment modalities or the
regeneration o posterior mandibular areas, autogenous bone block
grats
rom the mandibular symphysis remain as one o most popular
procedures perormed by the dental community as this
surgical technique oers an easy access and enough grat material
or adequate augmentation. The biomaterials, Geistlich
BioOss
and Geistlich BioGide
may help the surgeon to obtain optimal regeneration results,
avoiding potential sot andhard tissue complications during the
healing process in both donor and receptor areas.
GBR with Block GratingDr. Juan Jos Aranda; Madrid
Therapy Concept
Jaw Dentition Region Augmentation
Upper Jaw Partially Edentulous Anterior Horizontal
Lower Jaw Fully Edentulous Posterior Vertical
Material
> Autogenous bone block chin
> Geistlich BioOss
> Geistlich BioGide xed with tacks
Aim
> Horizontal ridge augmentation: a GBR procedure is perormed
with an autogenous bone block grat
harvested rom the chin area utilizing Geistlich BioOss and
Geistlich BioGide.
-
7/29/2019 MKG Broschuere E.pdf En
13/4013
Cawood Class IV
ConclusionThe combination o autogenous bone grats harvested rom
the alveolar zygomatic buttress with autogenous bone chips
is suited or reconstruction o bony alveolar crest deects in the
anterior maxillary region. Bone harvesting was perormed
with the piezoelectric device Mectron Medical Technology, which
avoids trauma to the mucosal membrane o the
maxillary sinus.
Besides a minimal morbidity, the zygomatic buttress donor site
supplies good quality bone with a natural convex shape
ideally suited or the anterior alveolar process region. The
combination o cortical bone external layer covering the
autogenous bone chips internal lling provides an excellent basis
or successul osseointegration o dental implants.
This avoids the need or later secondary corrective sot tissue
augmentation with brous tissue grats to reconstitute thevestibular
projection. Geistlich BioGide protects the bone grat, avours wound
healing, and adds additional saety to
a predictable outcome.
Combining Cortical and Particulate BoneDr. KaiHendrik Bormann,
Pro. Dr. Dr. NilsClaudius Gellrich; Hannover
1 Bony deect in the anterior
region.
2 A cortical bone transplant is
gained rom the alveolar zygomatic buttress region.
3 The bone grat is harvested
without harming the Schneiderian membrane.
4 The thin cortical bone grat
in place with transosseousscrew xation.
5 Ater lling the gap under thealveolar zygomatic buttesswith
autogenous bone chips,Geistlich BioGide is placed
over the augmented deect.
6 Sot tissue situation ater 4weeks.
7 Situation at reopening beore implant insertion, 12weeks ater
augmentation.
8 Fixation screws are removedand the dental implant is
inserted.
Therapy Concept
Jaw Dentition Region Augmentation
Upper Jaw Partially Edentulous Anterior Horizontal
Lower Jaw Fully Edentulous Posterior Vertical
Material> Autogenous bone transplant and chips alveolar
zygomatic buttress
> Geistlich BioGide
Aim> Horizontal ridge augmentation: to achieve an excellent
aesthetical outcome with an alveolar zygomatic buttress bone
transplant in combination with autogenous bone chips covered
with Geistlich BioGide.
-
7/29/2019 MKG Broschuere E.pdf En
14/4014
ConclusionThe technique is appropriate or patients with severe
horizontal bone atrophy and provides a successul ridge
augmentation
with high predictability.
Covering the autogenous block grat with Geistlich BioOss and
Geistlich BioGide signicantly reduces autogenous
bone block resorption.
The resorbable membrane, Geistlich BioGide, shows an easy
handling and simplies the surgical method. The stability o
the membrane can be urther improved using the doublelayer
technique.
Cawood Class IV
GBR with Block GratingPro. Dr. Daniel Buser, PD Dr. Thomas von
Arx; Bern*
1 Thin ridge situation in the
posterior mandible.
2 The bone cortex is perorated
with a small round bur to induce bleeding rom the marrow
cavity.
3 Bone grat rom the retromo
lar area xed with a titaniumscrew.
4 Coverage with Geistlich Bio
Oss.
5 The collagen membrane,Geistlich BioGide , is applied using the
doublelayertechnique.
6 Primary wound closure is accomplished with single interrupted
sutures.
7 Optimal bony support or implant placement ater approx.
months.
8 Stable periimplant bone level18 months postoperatively.
Therapy Concept
Jaw Dentition Region Augmentation
Upper Jaw Partially Edentulous Anterior Horizontal
Lower Jaw Fully Edentulous Posterior Vertical
Material
> Autogenous bone block retromolar area posterior to the
augmentation
> Geistlich BioOss
> Geistlich BioGide doublelayer technique
Aim> Horizontal ridge augmentation: using Geistlich BioOss
and Geistlich BioGide to cover the
autogenous bone block or minimizing resorption o the bone
grat.
* von Arx T & Buser D. Horizontal ridge augmentation using
autogenous block grats and the guided bone regeneration technique
with collagen membranes:
a clinical study with 42 patients. Clin Oral Implants Res
2006;17(4):359-66.
-
7/29/2019 MKG Broschuere E.pdf En
15/4015
Cawood Class IV
ConclusionThis method appears suitable or successul horizontal
ridge augmentation, prior to implant placement, in the
indications
o single tooth gaps, multiple tooth gaps, and edentulous distal
extension situations. The combination o Geistlich
BioOss and Geistlich BioGide appears to be an eective treatment
option or horizontal ridge augmentation and
avoids harvesting o autogenous bone.
The barrier unction o the resorbable collagen membrane Geistlich
BioGide seems to be adequate or the desired bone
regeneration in these indications.
GBR with BiomaterialsPro. Dr. Christoph Hmmerle; Zurich*
1 Buccal view o the deect
sites.
2 Augmentation with Geistlich
BioOss granules and Geistlich BioOss SpongiosaBlocks.
3 The resorbable Geistlich Bio
Gide membrane coveringthe right side o the augmented area.
4 The entire area covered with
Geistlich BioGide.
5 Suitable bone support or implant insertion 9-10
monthspostoperatively.
6 Ater placement o the implants, no remaining bonedeects were
present.
7 Occlusal view o the deectclosure.
8 Final outcome ater insertiono the xed partial denture.
Therapy Concept
Jaw Dentition Region Augmentation
Upper Jaw Partially Edentulous Anterior Horizontal
Lower Jaw Fully Edentulous Posterior Vertical
Material
> Geistlich BioOss Spongiosa Block
> Geistlich BioOss
> Geistlich BioGide
Aim> Horizontal ridge augmentation: GBR using biomaterials as
sole substitute or alveolar bone augmentation
to avoid autogenous bone grat harvesting.
* Hmmerle CHF, Jung RE, Yaman D, Lang NP. Ridge augmentation by
applying bioresorbable membranes and deproteinized bovine bone
mineral:
a report o twelve consecutive cases. Clin Oral Implants Res
2008;19(1):9-25.
-
7/29/2019 MKG Broschuere E.pdf En
16/4016
ConclusionThe crest splitting technique allows the placement o
implants in anatomic situations with insufcient ridge thickness,
by
moving the external cortical plate o the maxilla in a labial
direction. This technique allows immediate implant placement,
despite a large ridge augmentation.
The gap resulting rom the crest splitting is lled with
autogenous particulate boneand Geistlich BioOss ratio 1:1,
which
allows a predictable bone volume preservation. Due to the good
adhesion o Geistlich BioGide to the deect, the
particulate bone grat is kept in situ during the regeneration
process.
Cawood Class IV
Crest SplittingDr. Gerhard Iglhaut; Memmingen
1 Occlusal view o the ridge a
ter ap elevation.
2 Longitudinal split o the alve
olar crest.
3 Two implants are placed in
the expanded crest.
4 The split around the implants
is lled with a mixture oautogenous bone chips andGeistlich
BioOss.
5 The augmented ridge is covered with a Geistlich
BioGidemembrane beore closure othe sot tissue.
6 Lingual view o the nal situation.
7 Occlusal view o the prosthetic outcome.
8 Xray ndings 6 months aterimplant placement.
Therapy Concept
Jaw Dentition Region Augmentation
Upper Jaw Partially Edentulous Anterior Horizontal
Lower Jaw Fully Edentulous Posterior Vertical
Material
> Autogenous bone chips retromolar
> Geistlich BioOss
> Geistlich BioGide
Aim
> Horizontal ridge augmentation: the crest splitting
procedure in combination with Geistlich BioOss and
Geistlich BioGide is used to increase ridge width.
-
7/29/2019 MKG Broschuere E.pdf En
17/4017
Cawood Class IV
1 Preoperative panoramic ra
diograph showing partiallyedentulous ridge at teeth 32,31,
41.
2 Bone resorption and ridge
width reduction can be seenin the edentulous area.
3 Bone harvesting rom chin. 4 Onlay grat xation and
Geistlich BioOss contouringand covering.
5 Sot tissue healing monthsater surgery.
6 Occlusal view showing complete preservation o thegrat volume
ater months.
7 Dental implants in place. 8 Postoperative panoramic
radiograph.
ConclusionOptimal horizontal augmentation can be achieved in
partially edentulous areas by contouring the autogenous bone
block
with Geistlich BioOss.
Geistlich BioOss can be placed over grated areas, taking
advantage o its osteocondutive properties and compensating
or the natural bone resorption that always occurs. Geistlich
BioOss provided a spacemaking eect that allowed better
healing with osteogenic cell colonization and adequate volume o
the grated area. Further, it appeared to avour good
blood supply and resulted in relatively dense bone within
months.
Block ContouringPro. Dr. Carlo Maiorana; Milan*
Therapy Concept
Jaw Dentition Region Augmentation
Upper Jaw Partially Edentulous Anterior Horizontal
Lower Jaw Fully Edentulous Posterior Vertical
Material> Autogenous bone blocks chin
> Geistlich BioOss
* Maiorana C & Simion M. Advanced Techniques or Bone
Regeneration with BioOss and BioGide. RC libri 2005;34-37.
Aim
> Horizontal ridge augmentation: smoothing the surace o the
autogenous bone block with Geistlich BioOss
to avoid sot tissue ingrowth and bone resorption.
-
7/29/2019 MKG Broschuere E.pdf En
18/4018
ConclusionThe combination o particulate autogenous bone and
Geistlich BioOss allows a minimal invasive horizontal ridge
augmentation. This procedure avoids harvesting o an autogenous
bone block and its related morbidity o the donor site.
The grat is urther protected with Geistlich BioGide. The barrier
unction o the bioresorbable collagen membrane gives
the needed protection or optimal GBR and sot tissue healing. The
xation o the membrane is mandatory in this case,
as it is vital to prevent micromovements o the grat.
Cawood Class IV
GBR with Particulate GratingPro. Dr. Istvan Urban; Budapest
1 Preclinical situation. 2 Knieedge ridge in the poste
rior mandible.
3 Mixture o autogenous parti
culate bone and GeistlichBioOss is placed onto theresidual
ridge.
4 The grat is urther protected
with Geistlich BioGide.
5 Titanium pins are used to xthe collagen membrane.
6 Clinical situation ater twoweeks o healing.
7 Excellent incorporation o thegrat at reentry 7 monthsater rst
surgery. The ridgewidth is approximately 10 mm
and thereore sufcient orimplant placement.
8 Implant insertion.
Therapy Concept
Jaw Dentition Region Augmentation
Upper Jaw Partially Edentulous Anterior Horizontal
Lower Jaw Fully Edentulous Posterior Vertical
Material
> Autogenous bone chips oblique ridge o the retromolar
area
> Geistlich BioOss
> Geistlich BioGide xed with titanium pins
Aim
> Horizontal ridge augmentation: minimal invasive
augmentation procedure to obtain sufcient bone with a mixture o
autogenous bone and Geistlich BioOss covered with a Geistlich
BioGide membrane.
-
7/29/2019 MKG Broschuere E.pdf En
19/4019
Cawood Class V
ConclusionBoth edentulous upper jaw sites are vertically
augmented with a sinuslit procedure. On the let site an autogenous
block
grat compensates additionally the severe vertical atrophy.
To prevent bone resorption and to preserve the augmented volume,
Geistlich BioOss is used in the sinus lit in combination
with autogenous bone and to cover the lateral window in the
sinus lit. Furthermore, beore sot tissue closure the
collagen membrane, Geistlich BioGide, is placed on the entire
deect to protect it and to avour an optimal aesthetic
outcome.
Sinus Lit and Block GratingPro. Dr. Matteo Chiapasco; Milan
1 Preoperative radiograph sho
wing a partially edentulousmaxilla on both sides with
anassociated vertical atrophy,more severe on the let side.
2 Sinus grating with a mixture
o Geistlich BioOss and autogenous bone associatedwith vertical
onlay grating othe atrophic let maxilla.
3 Coverage and contouring o
the grat and the autogenousbone in the lateral enestration with
Geistlich BioOss.
4 The lateral window and the
autogenous bone block arecovered with Geistlich BioGide.
5 Radiographic control atersurgery sinus grating
withsimultaneous implant placement on the right side hasbeen
perormed during thesame session.
6 Clinical situation ater sottissue closure.
7 Prosthetic rehabilitation outcome right side.
8 Clinical situation ater completion o prosthetic rehabilitation
let side.
Therapy Concept
Jaw Dentition Region Augmentation
Upper Jaw Partially Edentulous Anterior Horizontal
Lower Jaw Fully Edentulous Posterior Vertical
Material
> Autogenous bone block and chips let ramus
> Geistlich BioOss
> Geistlich BioGide
Aim
> Vertical ridge augmentation: reduction o autogenous bone
grat resorption by covering the augmented site with
Geistlich BioOss and Geistlich BioGide.
-
7/29/2019 MKG Broschuere E.pdf En
20/4020
Cawood Class V
ConclusionThe sandwich osteotomy procedure in the posterior
mandible yields an optimal vertical gain, which allows adequate
bone
or implant placement, in patients with a minimum o 5 mm o bone
above the mandibular canal.
Filling the recipient site with Geistlich BioOss Spongiosa Block
avoids a second intervention or collection o autogenous
bone. Thus, the use o an inorganic cancellous bone block
simplies the inlay surgery or both, dentist and patient.
Geistlich BioGide covers the distracted segment and the
substitute bone grat and enhances wound healing without
complications.
Interpositional Bone GratingDr. Pietro Felice* MD/DDS, Pro.
Luigi Checchi MD/DDS,Pro. Claudio Marchetti MD/DDS; Bologna
1 Exposure o the alveolar ridge
and buccal bone.
2 Horizontal and vertical oste
otomies o the distractedsegment.
3 The upward lit o the trans
ported segment, obtaining aheight dimension gain o 7mm.
4 Geistlich BioOss Spongiosa
Block is trimmed to the adequate dimension and shapeto be
completely tted in therecipient site.
5 The distracted segment andthe biomaterial block arexed with
miniplates and miniscrews.
6 A resorbable bilayer collagenmembrane Geistlich BioGide is
used to cover the gratmaterial.
7 Intraoperative situation ollowing implants insertion, 4months
ater the reconstruction.
8 Periapical xray evaluationimmediately ater implant
insertion.
Therapy Concept
Jaw Dentition Region Augmentation
Upper Jaw Partially Edentulous Anterior Horizontal
Lower Jaw Fully Edentulous Posterior Vertical
Material
> Osteosynthesis plates
> Geistlich BioOss Spongiosa Block
> Geistlich BioGide
* Felice P et al. Vertical ridge augmentation o the atrophic
posterior mandible with interpositional block grats: bone rom the
iliac crest versus bovine
anorganic bone. Eur J Oral Implant 2008 Sept (in press).
Aim
> Vertical ridge augmentation: gain o sufcient ridge height
with a sandwich osteotomy lled with Geistlich BioOss
Spongiosa Block and covered with Geistlich BioGide.
-
7/29/2019 MKG Broschuere E.pdf En
21/4021
Cawood Class V
1 The vertical bony deect is vi
sible ater ap elevation.
2 The autogenous bone grat is
used or stabilising the heighto the membrane.
3 The 3dimensional volume is
created by using GeistlichBioOss Collagen, and covered by a
titaniumreinorcedePTFE membrane.
4 Geistlich BioGide is placed
over the nonresorbable ePTFE membrane or betterwound
healing.
5 The ePTFE membrane is
removed and the implant isinserted months postoperatively.
6 Closure o the sot tissue a
ter implant placement.
7 months ater implant place
ment the sot tissue healsuneventully and the verticaland
horizontal ridge dimension is regained.
8 Optimal outcome in the aes
thetic relevant zone.
ConclusionThis method is appropriate or augmentations in the
anterior region to allow implant placement and to ensure a good
aesthetic result. The autogenous bone grat is used or supporting
the titaniumreinorced ePTFE membrane, which
denes the appropriate ridge height. The horizontal and vertical
volume is created by using Geistlich BioOss Collagen.
The use o Geistlich BioGide over the nonresorbable membrane
avours the healing o the sot tissue and minimises the
incidence o wound dehiscence.
Horizontal/Vertical AugmentationDr. Ueli Grunder;
ZurichZollikon
Therapy Concept
Jaw Dentition Region Augmentation
Upper Jaw Partially Edentulous Anterior Horizontal
Lower Jaw Fully Edentulous Posterior Vertical
Material
> Autogenous bone block spina nasalis
> Geistlich BioOss Collagen
> Titaniumreinorced ePTFE membrane> Geistlich BioGide
Aim
> Horizontal and vertical ridge augmentation: adequate bone
volume as a support or sot tissue
to obtain an optimal aesthetic result.
-
7/29/2019 MKG Broschuere E.pdf En
22/4022
ConclusionThis technique is relatively simple and can provide
excellent GBR results in partially endentulous patients. The
osteosyn
thesis plates can be rapidly shaped and customized to any
possible situation providing a rigid scaold to protect the bone
grat. The resorbable Geistlich BioGide is preerred over
nonresorbable membranes in order to minimize postoperative
complications.
Cawood Class V
Vertical AugmentationDr. Mauro Merli; Rimini
1 Radiological ndings showing
the deect prior to the intervention.
2 Immediate implant insertion
beore vertical ridge augmentation.
3 Titanium osteosynthesis
plates are opportunely bentand xed with screws on thedeect.
4 The resorbable barrier Geist
lich BioGide is placed overosteosynthesis plates lledwith the
particulate autogenous bone grat.
5 Xray displaying the situationimmediately ater
augmentation.
6 Tissues during the healingphase o the grat just beoreimplant
exposure.
7 Exposure o the regeneratedarea with the plates still insitu 9
months ater implantinsertion.
8 The implants are completelysurrounded by bone.
Therapy Concept
Jaw Dentition Region Augmentation
Upper Jaw Partially Edentulous Anterior Horizontal
Lower Jaw Fully Edentulous Posterior Vertical
Material
> Autogenous bone chips ramus
> Osteosynthesis plates
> Geistlich BioGide
Aim> Vertical ridge augmentation: grat stability is achieved
using osteosynthesis microplates.
GBR is perormed with autogenous bone grat and a resorbable
barrier membrane, Geistlich BioGide.
-
7/29/2019 MKG Broschuere E.pdf En
23/4023
Cawood Class V
1 Computed Tomography beore
augmentation.
2 The drawing shows the stron
gly resorbed alveolar bone.Autogenous bone blocks inbuccal and
palatal sides createa 3 wall cavity, which is lledwith a mixture o
GeistlichBioOss and autogenousbone chips ratio 3:1.
5 CT showing the situation months ater bony augmentation.
4 3dimentional CT showing the
augmented deect rom thelet prole.
3 CT showing the augmented
deect.
6 Geistlich BioOss lls thesinus cavity and the gaps between the
autogenous boneblock grats.
7 months postbone grating,implants are inserted.
8 Xray ndings ater implantplacement.
ConclusionMaxillary sinus augmentation with Geistlich BioOss,
combined with autogenous bone block grats is a possible method
or creating adequate bone height and width beore implant
insertion. In cases o severe atrophy autogenous block grats
in the buccal and in the palatal sides create a 3wall cavity or
reconstruction o the alveolar crest. The created cavity can
be easily lled with Geistlich BioOss and autogenous bone
chips.
The Geistlich BioOss material not only serves as a scaold or
blood clot ormation, but also preserves the augmented
volume due to its slow rate o conversion to autogenous bone
remodeling.
Alveolar Reconstruction and Sinus LitPro. Dr. Armand R.
Paranque; Paris
Therapy Concept
Jaw Dentition Region Augmentation
Upper Jaw Partially Edentulous Anterior Horizontal
Lower Jaw Fully Edentulous Posterior Vertical
Material> Autogenous bone blocks and chips ramus and chin
> Geistlich BioOss
Aim
> Horizontal and vertical ridge augmentation: alveolar crest
reconstruction associated with maxillary sinus lit.
-
7/29/2019 MKG Broschuere E.pdf En
24/4024
Cawood Class V
1 Preoperative panoramic radio
graph.
2 Clinical situation in the right
maxilla ater implant placement.
3 The site augmentated with
Geistlich BioOss is stabilised with a titanium mesh.
4 Geistlich BioOss lls the
lateral enestration o the sinus.
5 Situation in the let upper jawater lateral window
preparation.
6 Geistlich BioOss lls thesinus cavity and covers thedeect
around the implants.A titanium mesh stabilises the
retromolar augmentation.
7 Radiographic ndings months ater augmentation.
8 Final outcome months atersurgery right side.
ConclusionThe combination o sinus lit with horizontal and
vertical augmentation using particulate bone substitute allows
implant
insertion in a onestage procedure.
Geistlich BioOss is used to ll the sinus cavity and or
augmentation o the ridge deect. The use o particulate bone
substitute, which is stabilised with a titanium mesh, avoids
completely the harvesting o autogenous bone and the risk o
morbidity o the donor site.
Sinus Lit and Bone Substitute GratingPD Dr. Dr. Karl Andreas
Schlegel; Erlangen
Therapy Concept
Jaw Dentition Region Augmentation
Upper Jaw Partially Edentulous Anterior Horizontal
Lower Jaw Fully Edentulous Posterior Vertical
Material > Geistlich BioOss stabilised with a titanium
mesh
Aim
> Horizontal and vertical ridge augmentation: Geistlich
BioOss used in sinus elevation and in
horizontal augmentation, supported by a titanium mesh.
-
7/29/2019 MKG Broschuere E.pdf En
25/4025
Cawood Class V
1 Panoramic Xray o the initial
situation.
2 Bone marrow approx. 60 ml
is harvested with a needlerom the pelvis dorsal orventral. The
bone marrowaspirate is concentrated in acentriuge to 37 ml in
approx. 15 minutes.
3 Geistlich BioOss is mixed
with the bone marrow concentrate and with
autologousthrombin.
4 The mixture is lled into the
sinus oor deect throughthe lateral enestration andinto the
extraction socket.
5 The lateral enestration and
augmentation sites are covered by a Geistlich BioGide.
6 Implant placement at reentry
only 3 months ater sinus lit.
7 Final situation with the pro
sthetic supply on both sites.
8 Panoramic Xray ater implant
insertion.
ConclusionThe sinus model demonstrates that the combination o
Harvest BMAC Bone Marrow Aspirate Concentrate with
Geistlich BioOss and Geistlich BioGide accelerates the tissue
regeneration. Histological analysis conrms the presence
o mature bone with a high percentage o lamellar bone, already
ater 3 months.
The concentrated bone marrow aspirate delivers growth actors and
mononuclear cells including mesenchymal stem cells
specically targeted to the deect. This allows the immediate
presence o the complex physiological system needed or
tissue regeneration. Thereore, the addition o Harvest BMAC to
Geistlich BioOss may be a successul technique or a
broad range o clinical indications.
The Harvest BMAC in combination with Geistlich BioOss
and Geistlich BioGide
is currently being tested in a prospectivemulticenter study.
Sinus Lit with Harvest BMACTM
Pro. Dr. Dr. Rainer Schmelzeisen*, Pro. Dr. Dr. Ral Gutwald,Dr.
Dr. Andris Stricker, Dr. Michael Vogeler, Dr. Sebastian Sauerbier;
Freiburg*FRCS London
Therapy Concept
Jaw Dentition Region Augmentation
Upper Jaw Partially Edentulous Anterior Horizontal
Lower Jaw Fully Edentulous Posterior Vertical
Material
> Harvest BMACTM Bone Marrow Aspirate Concentrate
> Geistlich BioOss
> Geistlich BioGide
Aim
> Vertical ridge augmentation: acceleration o the tissue
regeneration process to obtain mature bone in a short
period o time ater augmentation.
-
7/29/2019 MKG Broschuere E.pdf En
26/4026
ConclusionSuccessul vertical ridge augmentation can be achieved
in partially edentulous lower jaws by covering a mixture o
particulate Geistlich BioOss and autogenous bone chips with a
titaniumreinorced ePTFE membrane.
Histologic observations conrm a positive osteoconductivity o
Geistlich BioOss in close contact with the newly ormed
bone.*
Geistlich BioOss undergoes very slow resorption and substitution
with new bone remodelling, which is expected to be
advantageous or the longterm stability o regenerated bone.
Cawood Class V
Vertical AugmentationPro. Dr. Massimo Simion, Dr. Isabella
Rocchietta; Milan
1 Intraoral view o the deect in
the posterior right mandible.
2 Two tenting screws are in
serted to support the overlying membrane and the particulated
grat.
3 Augmentation with Geistlich
BioOss and autogenousbone 1:1 and covering with atitanium
reinorced ePTFEmembrane.
4 The ePTFE membrane is
shaped to adapt to the deect. The membrane is secured bucally by
two xationscrews.
5 Primary wound closure. 6 Panoramic X-ray o the augmented
sites.
7 Ater months o uneventulhealing, the screws and themembrane are
removed.
8 Three titanium implants areplaced.
Therapy Concept
Jaw Dentition Region Augmentation
Upper Jaw Partially Edentulous Anterior Horizontal
Lower Jaw Fully Edentulous Posterior Vertical
Material
> Autogenous bone chips maxillary tuberosity
> Geistlich BioOss
> Titaniumreinorced ePTFE membrane xed with screws
* Simion M et al. Vertical ridge augmentation by
expandedpolytetrauoroethylene membrane and a combination o
intraoral autogenous bone grat and
deproteinized anorganic bovine bone Bio Oss. Clin Oral Implants
Res 2007 Oct;18(5):620-9.
Aim> Vertical ridge augmentation: combination o a mixture o
Geistlich BioOss and autogenous bone chips 1:1
with a titaniumreinorced ePTFE membrane or longterm successul
GBR.
-
7/29/2019 MKG Broschuere E.pdf En
27/40
-
7/29/2019 MKG Broschuere E.pdf En
28/40
-
7/29/2019 MKG Broschuere E.pdf En
29/4029
Cawood Class V
ConclusionThanks to the CT diagnostic, the complexity o the
sinus cavity can be revealed and an appropriate surgical procedure
can
be planned.
In sinuses with multiple septa, careul attention should be payed
in membrane elevation in order to preserve its integrity.
The Schneiderian membrane can be successully protected or
repaired in case o peroration with Geistlich BioGide.
With Geistlich BioOss, a predictable implant outcome can be
achieved even without the use o autogenous bone.
Sinus Lit AugmentationDr. Tiziano Testori; Como
1 Computed tomography show
ing the complexity o the sinus anatomy.
2 Orthopantomograph o the
initial situation.
3 Antrostomy with membrane
elevation displaying the multiple septa.
4 The Schneiderian membrane
is protected with GeistlichBioGide.
5 The antrum is lled with
large particles o GeistlichBioOss.
6 Geistlich BioOss complete
ly lls the antrum up to thevestibular cortical wall.
7 Placement o two Geistlich
BioGide membranes doublelayer technique to coverthe
antrostomy.
8 Post-op orthopantomograph
showing the sinus lift proce-dure.
Therapy Concept
Jaw Dentition Region Augmentation
Upper Jaw Partially Edentulous Anterior Horizontal
Lower Jaw Fully Edentulous Posterior Vertical
Material> Geistlich BioOss
> Geistlich BioGide
Aim> Vertical ridge augmentation: reconstructive surgery with
a sinus lit augmentation with multiple septa.
-
7/29/2019 MKG Broschuere E.pdf En
30/4030
Cawood Class VI
ConclusionLe Fort I osteotomies allow the repositioning o the
maxilla in an aesthetic as well as a unctional context. The
resulting
acial contours lead to a juvenilisation o the prole, which
cannot be achieved by using maxilliary sinus grating.
The coverage o the autogenous bone grat by Geistlich BioGide
reduces the autogenous bone resorption, and ensures
the bony bridging o the osteotomy gap.
Le Fort I OsteotomyDr. Dr. Corvin Glatzer, Dr. Oliver
Schwerdtner; Berlin
1 Preoperative situation: Typi
cal Class III malocclusion.
2 Buccal view with an extreme
ly atrophied alveolar ridge.
3 Le Fort I osteotomy and xa
tion with osteosynthesisplates.
4 Contouring with autologous
bone chips.
5 The deect is covered with aresorbable collagen membrane
Geistlich BioGide.
6 Situation months ater surgery.
7 Osteosynthesis plates areremoved at the stage o reentry.
8 Successul Le Fort I osteotomyoutcome leading to a
pleasantprole.
Therapy Concept
Jaw Dentition Region Augmentation
Upper Jaw Partially Edentulous Anterior Horizontal
Lower Jaw Fully Edentulous Posterior Vertical
Material
> Autogenous bone chips harvested intraorally
> Osteosynthesis plates
> Geistlich BioGide
Aim
> Vertical ridge augmentation: oral unctionality restored
with the Le Fort I osteotomy.
-
7/29/2019 MKG Broschuere E.pdf En
31/4031
Cawood Class VI
ConclusionThe autogenous bone grat allows ull reconstruction o a
severely atrophied alveolar ridge in both the upper and the
lower
jaw with recovery o oral unction. The bone blocks are urther
contoured with autogenous bone chips to ll the remaining
gaps and even out the labial alveolar ridge.
Due to multiple layers o Geistlich BioGide covering the deect,
the bony augmentation is strongly stabilized, which
enhances a proper GBR.
GBR with Block GratingPro. Dr. Dr. Tateyuki Iizuka; Bern
1 Preoperative xray reveals
strong resorption o the maxilla and the mandible letside.
2 Situation ater exposure o
the maxillary alveolar ridge.
3 Autogenous bone block grats
are xed and contoured withautogenous bone chips.
4 The maxillary grat is covered
completely with several layers o Geistlich BioGide.
5 Autogenous bone block inplace mandible.
6 Contouring o the mandibular grat with autogenousbone
chips.
7 Resorbable collagen membranes Geistlich BioGideare placed over
the augmented site beore suture.
8 Radiography, 3 months atersurgery.
Therapy Concept
Jaw Dentition Region Augmentation
Upper Jaw Partially Edentulous Anterior Horizontal
Lower Jaw Fully Edentulous Posterior Vertical
Material> Autogenous bone blocks and chips calvaria
> Geistlich BioGide
Aim> Horizontal and vertical ridge augmentation:
reconstruction o extremely atrophied maxilla and mandible
to restore oral unction.
-
7/29/2019 MKG Broschuere E.pdf En
32/4032
ConclusionThis method is suitable and sae or bilateral sinus
elevation and simultaneous lateral ridge augmentation in cases
where
large volumes o hard tissue > cc are required.
Bilateral sinus elevation by using biomaterial alone is possible
under the conditions o: i undamaged Schneiderian
membrane, and ii relatively low volume o hard tissue required 3
cc or successul implant installation.
In severe atrophy cases however, the combination o autologous
bone harvested rom the iliac crest and Geistlich BioOss
provides: i sufcient volume o regenerative material by
simultaneous reduction in the need or autologous bone, ii
sufcient stability by introducing a slow resorbable biomaterial,
and iii sufcient amount o potentially osteogenic cells.
Sinus Lit and Block GratingPD Dr. Dr. Claude Jaquiry, Dr.
Nicolas Gabutti,Pro. Dr. Dr. HansFlorian Zeilhoer; Basel
2 The bony window is removed
PiezoSurgery and theSchneiderian membrane issuccessully
elevated. A Geistlich BioGide is placed toprotect the mucosa and to
acilitate introduction o autologous bone and biomaterial.
3 Autologous blocks harvested
rom the iliac crest are placedin multilayer technique.
Gapsbetween the blocks are lledup using a 1:1 mixture oGeistlich
BioOss and cancellous bone.
4 The bony window is replaced
and additional blocks or lateral augmentation are xedby titanium
screws.
5 The augmented area is covered by a Geistlich BioGidemembrane
in order to prevent invasion o brous tissue.
6 CTscan sagittal section othe right upper jaw 9 monthsater
augmentation showingconsolidated hard tissuewithin the newly
createdridge.
7 The vertical dimension > 10mm allows successul implant
installation 4.2 mm diameter and 12 mm length.
8 Clinical view ater xed prosthetic rehabilitation.
Therapy Concept
Jaw Dentition Region Augmentation
Upper Jaw Partially Edentulous Anterior Horizontal
Lower Jaw Fully Edentulous Posterior Vertical
Material
> Autogenous bone blocks and chips iliac crest
> Geistlich BioOss
> Geistlich BioGide
1 Partially edentulous maxilla
showing severe atrophy oposterior ridge. Residual vertical bone
1 mm does notallow simultaneous implantinstallation.
Aim> Horizontal and vertical ridge augmentation: successul
vertical and lateral ridge augmentation in a severe atrophy
case.
Cawood Class VI
-
7/29/2019 MKG Broschuere E.pdf En
33/4033
Cawood Class VI
1a Clinical situation beore sur
gery.
2a Augmented site ater 14
weeks o distraction procedure.
3a Implant insertion and tem
porary bridge 4 months ater rst surgery.
4a Final prosthodontic rehabi
litation with xed bridge inthe lower jaw 9 months ater rst
surgery.
1b Xray corresponding to picture 1a.
2b Xray corresponding to picture 2a.
3b Xray corresponding to picture 3a.
4b Xray corresponding to picture 4a.
ConclusionThe endodistraction device, looking like a dental
implant, is positioned in the centre o the bone and, when
escalated,
creates a distraction chamber, which lls up with callus ormation
and later original bone.
Compared to conventional devices with plates, the main
advantages are: no tilting tendency to the lingual side and no
second operation or device removal.
Using the endodistraction technique bone, gums, and the
rehabilitation o the aesthetics o ace and lips are gained
within
one operation.
DistractionUniv.Pro. Dr. Christian Krenkel, Dr. Dr. Simon
Enzinger; Salzburg
Therapy Concept
Jaw Dentition Region Augmentation
Upper Jaw Partially Edentulous Anterior Horizontal
Lower Jaw Fully Edentulous Posterior Vertical
Material > EndoDistractor Krenkel
Aim
> Vertical ridge augmentation: ull reconstruction o the
alveolar bone and recovery o oral unctionality.
-
7/29/2019 MKG Broschuere E.pdf En
34/4034
Cawood Class VI
ConclusionInterpositional bone grat procedures i.e., Le Fort I
osteotomy in the maxilla and sandwich osteotomy in the mandible
provide several advantages to edentulous patients with moderate
to severe bone loss ater periodontitis: i sagittal and
vertical movement o the ridges with compensation o the bone
loss, ii conservation o the xed gingival tissues on top
o the ridge, iii less resorption than with onlay grats, iv good
wound healing o the bony deect.
The good biological prerequisites or regeneration in the
osteotomy gaps interpositional grating allow clinical use o
bone substitute materials such as Geistlich BioOss.
Le Fort I and Sandwich OsteotomiesPro. Dr. Dr. Hendrik
Terheyden; Kassel*
1 Preoperative radiologic n
dings showing strong boneresorption in mandible andmaxilla.
2 The gap let ater osteotomy
was lled with iliac crest andGeistlich BioOss 1:3.
3 The deect in the maxilla was
covered with Geistlich BioGide.
4 Filling o the mandibular
sandwich osteotomy witha mixture o particulate iliaccrest and
Geistlich BioOss1:3.
5 Ater 4 months implants wereplaced.
6 Situation in the maxilla aterimplant insertion.
7 Optimal outcome with xedprosthetic supply.
8 Panoramic Xray ater implant placement.
Therapy Concept
Jaw Dentition Region Augmentation
Upper Jaw Partially Edentulous Anterior Horizontal
Lower Jaw Fully Edentulous Posterior Vertical
Material
> Autogenous bone blocks and chips iliac crest
> Geistlich BioOss
> Geistlich BioGide
* Terheyden H et al. Interpositionsosteoplastik des zahnlosen
Ober und Unterkieers Eine therapeutische Alternative bei
Knochenverlust durch aggres
sive Parodontitis. Implantologie 2007;15(3):297-304.
Aim> Horizontal and vertical ridge augmentation: use o
Geistlich BioOss and Geistlich BioGide or reconstruction
o extremely atrophied ridges in edentulous patients.
-
7/29/2019 MKG Broschuere E.pdf En
35/4035
Cawood Class VI
ConclusionOne therapy concept or vertical ridge augmentation o a
partially endentulous ridge in an aesthetically relevant region
is
the combination o distraction osteogenesis ollowed by an
autogenous bone grating.
The prerequisite or using distraction osteogenesis is a minimum
o 6 to 7 mm o bone height above the vital structures.
In the distraction phase, the two pieces o bone undergo gradual
incremental separation and new bone lls in the deect.
Due to the additional bone grating ater distraction, a good
aesthetic outcome is ensured. Implant placement is carried
out in a third stage.
Distraction and Block GratingDr.Albino Triaca, Dr. Dr. Roger
Minoretti; Zurich & Dr. Dan Kraus; Lugano
1 Preoperative clinical situation. 2 Raising the
mucoperiosteal
ap, ater a vestibular incision, and perorming the osteotomy.
3 Fixation o the crane distrac
tor MDOC, Orthognathicswith screws.
4 Situation at the end o the
distraction procedure 0.250.5 mm per day.
5 The distractor is removed atthe end o the distraction
retention period, which lasts 3months.
6 Autogenous bone blocks andchips are use or urther augmentation
and xed withscrews and a titanium mesh.
7 Ater months, the titaniummesh and screws are removed.
Additionally the attachedgingiva is broadened with apalatal sot
tissue grat.
8 Situation ater implant placement and healing.
Therapy Concept
Jaw Dentition Region Augmentation
Upper Jaw Partially Edentulous Anterior Horizontal
Lower Jaw Fully Edentulous Posterior Vertical
Material
> Distractor MDOC, Orthognathics
> Autogenous bone blocks and chips iliac crest, stabilised
with a titanium mesh
> Osteosynthesis screws
Aim> Vertical ridge augmentation: the distraction procedure
and an iliac crest bone grat used or excellent
outcome in the aesthetically relevant zone.
-
7/29/2019 MKG Broschuere E.pdf En
36/4036
Product Range
Resorption(%)
Less
resorption!
autog. block+
Geistlich Bio-Oss
peripherically 4
autog. block+
autog. chipsperipherically
+Geistlich Bio-Gide 5
autog. block+
Geistlich Bio-Oss
cover 3
autog. block+
Geistlich Bio-Oss
cover+
Geistlich Bio-Gide 6
autog. block+
autog. chipsperipherically 3
Comparison o horizontalaugmentation techniquesshows lower
resorption
rates, i the autogenousblock grat is coveredwith Geistlich
BioOssand Geistlich BioGide.
Geistlich BioGide PerioSystem CombiPack
Geistlich BioOss Geistlich BioOss Collagen
Geistlich BioGide and Geistlich BioOss:
your successul regeneration team
-
7/29/2019 MKG Broschuere E.pdf En
37/4037
Geistlich BioGide Geistlich BioOss
Geistlich Bio-Gide
resorbable, bilayer membrane25 x 25 mm
Geistlich Bio-Oss
spongiosa granules0.251 mm; 0.25 g, 0.5 g, 2 g
Geistlich Bio-Gide
resorbable, bilayer membrane30 x 40 mm
Geistlich Bio-Oss
spongiosa granules12 mm; 0.5 g, 2 g
Geistlich Bio-Gide Perioresorbable, bilayer membrane16 x 22 mm,
sterile templates
Geistlich Bio-Oss Collagenspongiosa granules + 10% collagen100
mg approx. 0.20.3 cm
250 mg approx. 0.50.6 cm
Perio-System Combi-Pack
Geistlich BioOss
Collagen 100 mg+ Geistlich BioGide Perio 16 x 22 mm,sterile
templates
Geistlich Bio-Oss Spongiosa Block
1 block1 x 1 x 2 cm approx. 2 cm
-
7/29/2019 MKG Broschuere E.pdf En
38/4038
Oral and maxilloacial surgery oers a plurality o therapy
concepts or regeneration o sot and hard tissues. A broad
variety o surgical approaches within the alveolar ridge
augmentation therapies has been presented in this brochure.
As a pioneer in bone and sot tissue regenerative processes,
Geistlich Biomaterials is committed to scientic research in
better solutions and new areas o regeneration. With this goal,
Geistlich Biomaterials together with leading international
surgeons conduct several clinical studies, ocusing on a broad
spectrum o oral and maxilloacial indications, namely:
cranial deects, orbital oor, rhinoplasty, palatal and alveolar
clet, orthognathics, genioplasty.
We are looking orward to presenting you our results and
discussing with you new indications or using biomaterials in
cranial and maxilloacial surgery.
Outlook
Cranial Defects
Orbital Floor
Rhinoplasty
Palatal Cleft
Orthognathics
Genioplasty
Alveolar Cleft
-
7/29/2019 MKG Broschuere E.pdf En
39/40
-
7/29/2019 MKG Broschuere E.pdf En
40/40
31290.1
/0808/e