Embed Size (px)
Citation preview

Minimal/Measurable residual disease in AMLEuropean LeukemiaNet guidelines
Arjan A. van de Loosdrecht
Department of HematologyAmsterdam UMC
VU University Medical CenterCancer Center Amsterdam (CCA)
Amsterdam, The Netherlands
London8-9 November 2018
CDDF Multi-stakeholder workshop on MRD in AML and CLL

• The persistence of leukemic cells after chemotherapy and which numbers are below the sensitivity detection level of routine morphology
• Represents the sum of the effect of all relevant cellular resistance mechanisms, pharmacokinetic resistance and other unknown factors affecting the effectiveness of the treatment
Measurable Residual Disease (MRD) in AML
Hourigan CS, et al., Leukemia 2017;31:1482Schuurhuis GJ, et al., Blood 2018;131:1275

2016 European LeukemiaNet Response criteria in AML
Diagnosis and Management of Acute Myeloid Leukemia in Adults: 2016 Recommendations from an International Expert Panel
On behalf of the ELN. H. Dohner, et al. Blood 2017;129:424-447

MRD Why?
• To provide objective methodology to establish remission status
• To refine outcome prediction and inform post remission treatment
• To identify impending relapse to enable early intervention
• To allow more robust post-transplant surveillance
• To Use as surrogate endpoint to fasten drug approval
Hourigan CS, et al., Leukemia 2017;31:1482Schuurhuis GJ, et al., Blood 2018;131:1275

MRD How?
• Leukemia specific features at diagnosis distinguish residual leukemic cells from normal cells:
– Aberrant immunophenotype (FCM)– Fusion transcripts (RNA PCR)/digital PC)– Gene mutations (DNA/RNA PCR, NGS)– Gene overexpression (RNA qPCR)
Hourigan CS, et al., Leukemia 2017;31:1482Schuurhuis GJ, et al., Blood 2018;131:1275

Limitation of morphological assessment to assess remission status in AML
67%
Inaba H, et al, J Clin Oncol 2012;30:3625-32
Post-induction:No detectable AML by flow
EFS
≥5% blasts by morphology
EFS
<5% blasts by morphology
EFS

Mol-MRD status; the most powerful prognostic factor in NPM1 mutant AML
CIR OS
In multivariate analysis MRD status was only significant independent prognostic factor, considering:• Age• WBC• Mutational profile (51 gene panel including FLT3-ITD, DNMT3A, WT1)
2P<0.00001
2P<0.00001
MRD neg
MRD neg
MRD pos
MRD pos
NCRI AML17: PCR status in peripheral blood post-chemotherapy course 2
Ivey A, Hills RK et al. NEJM 2016;374:422-433Hills RK, et al., NEJM 2016;375(6):e9

Application of next generation sequencing approaches for MRD detection
E8E7E6E5
TADRHD
E4
p. P he 1
3Leu
fs* 9
8
E3
p. Val9
2 Gly
fs* 2
0p. s p
lice- s it
e
p. G ly2
3Ar g
fs* 8
8p. G l
u 27 G
lyfs
* 84
p. Leu 3
1Tr p
fs* 5
p. Pro 3
4Ar g
fs* 1
1p. A l
a 39G
lyfs
* 97
p. Ser 5
0Ar g
fs* 6
2
p. Val5
4 Ser
fs* 5
7
p. Asp5
7 Ar g
fs* 5
4
p. G lu 6
1 Ar g
fs* 5
0p. Ar
g64A
lafs
* 47
p. Ser 6
7Lys
fs* 4
4p. P h
e 70S
erp. Le
u 71 S
erfs
* 24
p. H is 7
8_ Trp7
9 de l
ins G
lnPr
oLe
u Ar g
p. H is 7
8Ar g
p. Trp7
9_ Arg8
0 in s
6p. Tr
p79A
r gp. Tr
p79C
ysp. Ar
g80C
ysp. Ar
g80S
erp. Ar
g80H
isp. Ar
g80G
ly
2 2
p. Asn 8
2 Ser
p. T hr 8
4Asn
p. T hr 8
4Pr o
2
p. L ys 8
3Ar g
2
p. T hr 8
4Tyr
fs* 2
7p. Le
u 85A
r gp. Le
u 85P
r ofs
* 26
p. Val9
2Va l
fs* 1
9p. A l
a 93G
lyfs
* 18
p. Leu 9
4 Gly
fs* 1
8
p. Me t
1 06I
le
p. G lu 1
11Va
l fs* 5
p. Glu
111_ As
n 11 2
ins A
lap. As
n 11 2
delin
s Va l
ArgS
erG
lyPr
o Gly
p. Asn 1
1 2I le
p. T hr 8
4_ Leu 8
5 de l
p. T yr 1
1 3Le
u fs*
4p. Se
r 11 4
Leu f
s*3
p. Ser 1
1 4Pr
o fs*
5p. Se
r 11 4
*
2 4
p. Ser 1
1 4Le
u
p. A la 1
1 5G l
y fs*
2p. A l
a 11 5
Asp f
s*2
p. Ser 1
1 4_ A l
a 11 5
ins G
lyT
yrLe
up. Le
u 117
G ly f
s*2
p. Asn 1
1 9L y
sp. T h
r 121
A la f
s*1 6
p. G ln 1
27*
p. P he 1
31Se
rp. P h
e 131
Leu f
s*1 8
p. Leu 1
34Pr
op. Ar
g135
G ly
p. Arg1
35L y
sp. Ar
g135
T hr
p. Arg1
35Se
r
p. Arg1
35L y
s fs*
4 9p. P h
e 136
Cys
2 12
p. P he 1
36Le
u fs*
1 4p. Va
l137
T hr f
s*1 2
p. G ly1
38Ar
g fs*
1 6p. G l
y138
Ser fs
* 14
p. G ly1
38Ar
g fs*
4 3p. G l
y138
Ser fs
* 54
p. Arg1
39G l
yp. Ar
g139
G ln
p. Arg1
39Le
u
p. G ly1
38Ar
g
2
p. G ly1
38du
p
42
p. Arg1
39*
5
p. Arg1
39_ Se
r 14 0
ins P
r o
7
p. Ser 1
4 0As
np. Ar
g14 2
L ys f
s*44
p. Arg1
4 2T h
rp. G l
y14 3
Arg f
s*4 3
p. G ly1
4 3Ar
g
2
p. P he 1
4 6Cy
sp. Le
u 14 8
Pro
p. Val1
52Le
u fs*
33
p. G lu 2
89*
p. Val1
52As
pp. G l
n 15 8
Pro f
s*2 3
p. G ln 1
5 8*
p. A la 1
60Va
lp. I le
1 68A
snfs
* 18
p. Asp1
7 1As
np. As
p17 1
A la
p. Asp1
7 1G l
yp. G l
y17 2
Val
p. Pro 1
7 3T h
r
p. Arg1
7 4*
4
p. Arg1
7 4G l
np. Ar
g17 4
Leu
7 8
p. Arg1
77*
3
p. Arg1
77G l
n
p. Arg1
80Le
u fs*
6p. Ar
g180
Trp
3
3
p. Pro 2
1 3G l
n fs*
22p. Pr
o 21 8
G ln f
s*1 3
p. T hr 2
1 9H i
s fs*
1 5
3
p. s plic
e- s ite
p. H is 2
2 8Pr
o fs*
6p. G l
n 235
*
p. G ln 2
37*
p. G ln 2
41Ar
g fs*
44
p. G ln 2
47*
p. T yr 2
60Se
r fs*
314
p. Ser 2
87Cy
s fs*
2 85
p. Arg2
93*
8
p. A la 2
7 2Se
r fs*
301
p. Trp2
52*
p. Ser 2
91Pr
o fs*
1 0
p. L 286
P fs*
2 87
p. G lu 2
89Ar
g fs*
2 85
p. Leu 2
90Pr
o fs*
2 84
p. Ser 2
95*
p. Leu 2
94Se
r fs* 7
p. Ser 2
95As
n fs*
277
p. Asp2
99G l
yp. Le
u 300
Pro f
s*2 6
4
p. G ln 3
08H i
sp. A l
a 311
Arg f
s*25
6p. I le
315H
is fs*
258
p. Arg3
1 9Pr
o fs*
254
3
p. Pro 3
2 3Ar
g fs*
247
p. P he 3
2 6G
lyfs
* 24 0
p. P he 3
2 6Se
rp. T y
r 32 8
Pro f
s*24
4p. T h
r 331
Leu f
s*24
4p. T h
r 331
Asp f
s*24
2p. Pr
o 332
H is f
s*2 3
9p. Va
l333
A la f
s*24
1p. Va
l333
G ly f
s*24
0p. Va
l333
G ly f
s*2 3
5
p. G ly 3
4 5As
p fs*
229
p. Ser 3
4 6Le
u fs*
227
p. T hr 3
4 8G l
y fs*
221
p. T hr 3
4 8As
n fs*
225
p. T yr 3
5 0*
p. Ser 3
62*
p. G ly 3
66A l
a fs*
2 05
p. G ly 3
67Pr
o fs*
2 03
p. Pro 3
68Ar
g fs*
1 89
p. P he 3
69Va
l fs* 2
04
2
p. G ln 3
7 0L y
s fs*
1 97
2
p. Ser 3
7 5I le
fs* 1
98p. H i
s 377
Pro f
s*1 9
6
2
p. A la 3
82P h
e fs*
1 90
p. A la 3
82Pr
o fs*
1 89
p. Ser 3
90H i
s fs*
1 82
p. Me t
391L
eufs
* 17 6
p. Me t
391 A
r g
p. Pro 3
98Le
up. Pr
o 399
Leu f
s*17
4p. Pr
o 399
*
p. Cys 4
05Le
u fs*
1 68
p. G ly4
11Le
u fs*
1 68
p. Ser 4
1 2Pr
o fs*
1 60
p. A la 4
1 3G l
y fs*
1 60
p. Ser 4
1 8A l
a fs*
1 49
p. Val4
2 6T h
r fs*
1 43
p. Pro 4
36Le
u fs*
1 43
p. Arg4
44Pr
o fs*
1 28
p. G lu 4
47G l
y fs*
1 21
p. Trp4
5 0*
p. *4 5
4 Ser
ext*
5 3
4
p. s plic
e- s ite
7
p. s plic
e- s ite
4
2
p. T hr 2
96I le
fs* 9
p. T hr 3
01Ar
g fs*
1 4
p. Arg1
1 Gly
fs* 1
04
p. Asp5
7_ Cys 8
1 de l
ins G
lyp. A l
a 56C
ysfs
* 41
p. G lu 6
1*
p. Me t
51I le
fs* 6
0
p. Asp4
8Ar g
fs* 6
3
p. G ly 6
0Pr o
fs* 5
2
p. T hr 6
5 Cys
fs* 3
2
2
p. Val7
4 Gln
fs* 4
2p. P h
e 70S
erfs
* 24
p. Pro 7
6Ar g
fs* 3
5
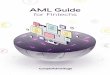
RUNX1missense
nonsense
frame-shift
in-frame
splicing
Kohlmann et al., Leukemia 2014;28:129-37RUNX1 residual mutation load at first follow-up(n=103)
EFS

Jongen-Lavrenic M, et al., N Engl J Med 2018:378;1189-99
MRD in AML/MDS: NGS and FCM

MRD in AML/MDS: NGS and FCM
Jongen-Lavrenic M, et al., N Engl J Med 2018:378;1189-99

ELN: consensus document and strategiesmultiparameter flow cytometry
• Goal: harmonize approaches, improve quality– Approach: “LAIP-based different-from-normal (DfN)”– Marker panels– Technical requirements for specimen
collection/processing, flow cytometers– Calculation of MRD burden– Thresholds and time points for MRD assessments– Reporting
Schuurhuis GJ, et al., Blood 2018;131:1275

Principles of Flowcytometric MRD in AMLLAIP and DfN (different-from-normal)
Leukemia Associated Immunophenotype (LAIP) • CD45 WBC marker• CD34 primitive marker
CD117 primitive and myeloid marker• CD33 myeloid marker• CD38 activation and differentiation marker• CD7 lymphoid marker• CD14 monocyte marker• CD56 NK cell marker
• Cross-lineage antigen expression• Asynchronous antigen expression• Antigen over-expression• Antigen under-expression
Note: in > 90% of the cases ≥ 1 LAIP can be defined

MRD detection by first defining Leukemia Associated (Immuno)Phenotypes (LAIP) in diagnosis AML
R
AML
normal BM
Combination of markers used for MRD
* primitive (CD34, CD133, CD117)* myeloid (CD13, CD33)* aberrancy defining (eg CD2)* CD45 (pan-leukocyte)
CD2 is lymphoid markerCD13 is myeloid marker
See also: Cloos J, et al., J Visualized Exp 2018;133:e56386

Cloos J, et al., J Visualized Exp 2018;133:e56386
LAIPs at AML diagnosis

R2
Diagnosis AML BM after 1st cycle BM after 2nd cycle relapse
75% 0.16% 0.21% 24%
FSC SSC
CD2
CD
117
Flow Cytometry Strategies for MRD detection
See also: Cloos J, et al., J Visualized Exp 2018;133:e56386

Sequential MRD monitoring in allo Tx
Ossenkoppele GJ, Schuurhuis G. Hematology Am Soc Hematol Educ Program 2016;(1):356-365

• EDTA vs heparin
• BM sampling first pool/hemodilution vs PB
• BM transport (< 72h)
• Instruments (settings/harmonisation [Harmonemia, Euro-flow consortium])
• Preparation of samples (stain/lyse/wash vslyse/wash/stain/wash); fluorchromes
Technical requirements
Schuurhuis GJ, et al., Blood 2018;131:1275

• Define LAIP (vs normal)• Use the most specific and/or highest frequency LAIP• Relate LAIP to CD45+ cells (excl CD45- (erythroblasts)
• Use LAIP at diagnosis to optimally inform MRD gating• Use DfN approach to identify any new LAIP
• Require between 0.5-1 x106 events (excluding; CD45- and debris) unless cluster of MRD is obvious)
• Perform in well experienced lab and trained operator
Schuurhuis GJ, et al., Blood 2018;131:1275
How to calculate LAIP?

Tresholds and time points of MRD assessments and reporting
• LAIP treshold: 0.1% (positive vs negative)• Sequential monitoring after induction and/or consolidation
• Reporting:• Absolute numbers of LAIP and % to CD45+ (WBC)• MRD pos vs neg vs no MFC MRD identified• Detection sensitivity• Comments on quality of the sample (i.e. hemodilution)• Clinical relevance i.e.
• MRD < 0.1%: MFC MRD detectable andquantifiable with uncertain significance
Schuurhuis GJ, et al., Blood 2018;131:1275

Summary:Flow cytometry-based MRD detection in AML
Advantages Disadvantages Pitfalls
• Widely applicable (>90% of AML cases)
• Not as sensitive as PCR • Not all AML cells have abnormal phenotype
• Quantification of abnormal cells
• Sensitivity not uniform across patients
• More than 1 phenotype possible
• Quantification of abnormal “stem/progenitor” cells
• Best results with fresh material • Phenotype shift, loss
• Relatively sensitive • Analysis, interpretation operator-dependent
• Abnormal cells may not have relapse potential
• Quick turn-around time • Challenging to standardize/harmonize
• Separation live/dead cells
• Assessment of hemodilution
• Identification of therapeutic target(s)
Hourigan CS, et al., Leukemia 2017;31:1482Schuurhuis GJ, et al., Blood 2018;131:1275

(1) Molecular MRD: markers
• (validated) Markers for molecular MRD by qPCR- NPM1 mutations- Fusion genes CBF-AML:
- RUNX1-RUNX1T1 (t(8;21))- CBFB-MYH11 (inv(16))
- Fusion genes: - PML-RARA (t15;17))
- Rare: AML with BCR-ABL1 (p190 transcript)
• No role for CHIP related mutations: DNMT3A, ASXL1 and TET2• No role for germ-line mutations: GATA2, RUNX1, CEBPA, DDX41,
ANKRD26• No role for WT1 (low sensitivity and specificity)
Schuurhuis GJ, et al., Blood 2018;131:1275

(2) Molecular MRD: markers
• In alloTx: role for chimerism as MRD marker
• Due to losses or gains of mutations at relapse• no role for mutations in FLT3-ITD, FLT3-TKD, NRAS, KRAS, IDH1/2,
MLL-PTD
• For AML patients not in the moleculair defined subgroups (NPM1; CBF, APL) MRD should be assessed by FCM
• Failure to achieve MRD-neg CR or rising MRD levels are associated with relapse
Schuurhuis GJ, et al., Blood 2018;131:1275

Molecular assessments and definitions of molecular responses
• Timepoints (note: for different markers; different interpretations- At diagnosis- > 2 cycles induction CT- > end of treatment
• Definitions:- CR MRD-- Molecular persistance at low copy numbers- Molecular progression- Molecular relapse
Schuurhuis GJ, et al., Blood 2018;131:1275

Solutions to problem of “false-negative” MRDExperimental approaches on FCM MRD
35%-40% of the MRD “low” patients nevertheless relapse
How to identify these patients?
Increase sensitivity
a. of immuno-MRD
b. +/- molecular MRD (NPM1)
Differences in time of onset of relapses
identifiable by sequential MRD
Contribution of leukemia stem cells
Take into account possible IF shiftsp<0.001
RFS (months)
MRD ≤0.1% n=141
MRD >0.1% n=42
Schuurhuis GJ, et al., 2016 (with courtesy); see also Hanekamp D, et a., Int J Heamtol 2017:105;549

• CD123 Jordan et al, Leukemia 2000, 14: 1777• CD33 Taussig et al, Blood 2005; 106: 4086• CD44 Jin et al, Nat Med 2006, 12: 1167• CLL-1 (CLEC12A) van Rhenen et al, Blood 2007, 110: 2659• Lineage markers van Rhenen et al, Leukemia, 2007; 21: 1700• CD96 Hosen et al, PNAS 2007, 104: 11008• CD47 Majeti et al, Cell 2009; 138: 286• CD25 Saito et al, Sci. Transl. Med. 2010; 2: 17ra9• CD31 Saito et al, Sci. Transl. Med. 2010; 2: 17ra9• TIM-3 Jan et al, PNAS 2011; 108: 5009• Hif1α Wang et al. Cell Stem Cell 2011; 8: 399• CD99 Chung et al, Blood 2013, 122: • CD45RA Goardon et al, Cell Stem Cell 2011, 19: 138-152
Kersten et al, Br J Haematol 2016• ALDH Pearce 2005, Cheung 2007, Ran 2009, Gerber 2012, Schuurhuis et al,
PlosONE 2013• Scatter aberrancies Terwijn et al, PLoSOne 2014 Sep 22; 9(9):e107587
Current known AML stem cell markers
Lineage aberrancies:• CD2, CD7, CD11b,CD14, CD15, CD19, CD20, CD22, CD56,• HLADR-CD15-, CD13-/+CD33+/-, CD13-CD33-
Schuurhuis GJ, et al., 2016 (with courtesy); see also Hanekamp D, et a., Int J Hematol 2017:105;549

Aberrant marker expression
Inter-patient heterogeneity of marker expression inCD34+CD38- LSC forces use of >>1 stem cell marker (1)
marker performance
patient 1patient 2CLL-1 ++ -CD7 - ++
MRD 2068 MRD 1959
All within CD45dim/ SSClow /CD34+ gate
Zeijlemaker W, et al., Leukemia 2016;30:439
CD38
Aberrant marker

Intra-patient heterogeneity of marker expression in CD34+CD38- LSC requires >>1 stem cell marker (2)
CLL-1 and CD33 are good markers in this patientAll within CD45dim/ SSClow /CD34+
gate Zeijlemaker W, et al., Leukemia 2016;30:439

Prognostic value CD34+CD38- LSC at diagnosis
EFS (months)
Terwijn M, et al. PloSOne 2014;9:e107587

LSC frequency : Prognostic value after therapy
Induction Cycle I Induction Cycle II Cycle III
pLSC- n=49
pLSC- n=22
pLSC- n=36
pLSC- n=41
pLSC- n=28
pLSC- n=20
pLSC= putative leukemic stem cell
Terwijn M, et al. PloSOne 2014;9:e107587

Prognostic value MRD/LSC combination after induction therapy
Still relapses in LSC “low”/MRD “low” patientsSolved by incorporating clonal/immunophenotype shifts?

Present panel for LSC characterization
31
Tube FITC PE PerCP-CY5.5 PC7 APC APC-H7 HV450 KO
1 HLA-DR CD33 CD13 PBS CD38 PBS CD34 CD45
2 CD44 Clec12a CD13 CD56 CD38 HLA-DR CD34 CD45
3 CD7 TIM-3 CD13 CD117 CD38 CD19 CD34 CD45
4 CD2 CD133 CD13 CD117 CD38 CD19 CD34 CD45
5 CD36 CD123 CD13 CD33 CD38 CD14 CD34 CD45
6 CD11b CD96 CD13 CD117 CD38 CD14 CD34 CD45
7 CD15 CD22 CD13 CD117 CD38 HLA-DR CD34 CD45
Problem: availability of bone marrow
Zeijlemaker W, et al., Leukemia 2016;30:439

TubeFITC PE PerCP-CY5.5 PeCy7 APC APC-H7 BV421 HV500C
1 CD45ra CLL-1 CD123 CD33 CD38 CD44 CD34 CD45
TIM-3
CD7
CD11b
CD22
CD56
• 1 tube for LSC detection at diagnosis and follow-up
• Identifies almost all CD34+CD38- LSC
• Needs no extensive experience in BM immunophenotyping
• Multi-institutional approach possible • Takes into account immunophenotypic shifts• Can be extended with other markers in the PE-channel
LSC detection kit for diagnostic purposes: assessment of totalstem cell load (including vanishing and evolving populations)(1 tube, 8 colors, 13 markers)
PE channel contains antibodies negative on HSC
Zeijlemaker W, et al., Leukemia 2016;30:439

A B
after cycle I
MRD BM (log transformed)
after consolidation therapy
MR
D P
B (l
og tr
ansf
orm
ed) r =0.67
p <0.001
MR
D P
B (l
og tr
ansf
orm
ed)
MRD BM (log transformed)
r =0.70p <0.001
after cycle II
Correlation between BM MRD and PB MRD in AML/MDS
All LAIPs (1-5 per patient) considered Only LAIPs used for correlations with clinical outcome considered
Zeijlemaker W, et al., Leukemia 2016;30:708-715

Conclusions: MRD/LSC in AML
• A standard panel for MRD and LSC detection is available in AML
• MRD and LSC frequency is highly predictive for DFS/OS
• MRD in PB is a new tool and correlated with BM MRD: validation studies are needed
• MRD/LSC is not the only explanation for risk of relapse
Schuurhuis GJ, et al., Blood 2018;131:1275

• International pro-spective multi-centerstudy
• Patients 18- 60 years• n = 517• 31 Centers:
− Netherlands− Belgium− Switzerland
+/- G-CSF
HOVON/SAKK 42a: MRD in AML< 60yrstreatment and sampling scheme
M. Terwijn, et al. J Clin Onco 2013;31:3889-97
: MRD sampling point

M R D -M R D +L o g ra n k
N1 0 9
5 5
F2 92 5
P = 0 .0 0 5
M R D -M R D +
A t r is k :1 0 95 5
8 12 8
6 22 2
4 51 5
1 1
8
M R D -
M R D +
0
2 5
5 0
7 5
1 0 0
m o n th s0 1 2 2 4 3 6 4 8
Cum
ula
tive p
erc
enta
ge
A f te r C y c le I
M R D -M R D +L o g ra n k
N1 4 1
4 2
F5 32 9
P < .0 0 1
M R D -M R D +
A t r is k :1 4 14 2
9 61 3
7 81 2
5 7
6
1 8
2
M R D -
M R D +
0
2 5
5 0
7 5
1 0 0
m o n th s0 1 2 2 4 3 6 4 8
Cum
ula
tive p
erc
enta
ge
A f te r C y c le I I
M R D -M R D +L o g ra n k
N9 72 4
F2 31 6
P < .0 0 1
M R D -M R D +
A t r is k :9 72 4
6 9
8
5 3
5
2 4
3
51
M R D -
M R D +
0
2 5
5 0
7 5
1 0 0
m o n th s0 1 2 2 4 3 6 4 8
Cum
ula
tive p
erc
enta
ge
A f te r C o n s o lid a t io n
M R D -M R D +L o g ra n k
N3 81 4
F97
P = 0 .0 5
M R D -M R D +
A t r is k :3 81 4
3 1
7
2 4
7
1 8
5
62
M R D -
M R D +
0
2 5
5 0
7 5
1 0 0
m o n th s0 1 2 2 4 3 6 4 8
Cum
ula
tive p
erc
enta
ge
A f te r C y c le I I - G o o d r is k
M R D -M R D +L o g ra n k
N8 81 9
F3 61 4
P < .0 0 1
M R D -M R D +
A t r is k :8 81 9
5 8
6
4 8
5
3 6
1
1 1
0
M R D -
M R D +
0
2 5
5 0
7 5
1 0 0
m o n th s0 1 2 2 4 3 6 4 8
Cum
ula
tive p
erc
enta
ge
A f te r C y c le I I - In te rm e d ia te r is k
F88
P = 0 .0 0 7
N1 5
9
M R D -M R D +L o g ra n k
M R D -M R D +
A t r is k :1 59
70
60
30
10
M R D -
M R D +
0
2 5
5 0
7 5
1 0 0
m o n th s0 1 2 2 4 3 6 4 8
Cum
ula
tive p
erc
enta
ge
A f te r C y c le I I - P o o r r is k
MRDneg n=141
MRDpos n=42
MRDnegn=97
MRDposn=24
MRDneg n=109
MRDposn=55
MRDpos n=14 MRD+ n=19
MRD-n=89
MRD -n=38
MRD+n=9
MRD- n=15
After Cycle II Good Risk
After Cycle I After Cycle II After Consolidation
After Cycle II Interm Risk After Cycle II Poor Risk
Relapse incidence after different therapy cycles (A)and after cycle II in different risk groups(B)
A
B

Implementation of flow-cytometric MRD detection in a multicenter clinical trial setting for older patients
Freeman et al, J Clin Oncol 2013;31:4123-31
AML16 (2006 – 2011)• 892 AML patients • (median age 67 years)• LAIP-MRD - prospectively
assessed(blind to clinical outcome)
• >2200 samplesPre = 833/ 892/ 1006 (~12%
inadequate)- C1 = 286 /739 (~10% inadequate)- C2 = 279 /503 (~11% inadequate)
• >100 UK centers
• 2/3 labs centralised analysis
Prognostic impact of flow MRD independent of:• Age• Cytogenetics• Wheatley index• NPM1/FLT3-ITD status

OS and DSF with MRD Negative vs Positive Multi-Parameter Flow Cytometry
0.4
1 2 30
Years after HCT
Prob
abilit
y
0.8
0.04
0.2
0.6
1.0
MRD-, Overall Survival
MRD-, Disease-Free Survival
MRD+, Overall Survival
MRD+, Disease-Free Survival
Walter RB, et al. J Clin Oncol. 2011 Mar 20;29(9):1190-7
Does MRD neg pretransplant implies alloSCT? Or is CT/AuPBSCT also sufficient?
Does MRD pos pretransplant implies no alloSCT or should we try to convert to MRD neg by f.e. Epigenetic treatment?

Induction cycle I Induction cycle II
R
Good risk
Ida 12 mg/m2
Ara-C 200 mg/m2AMSA 120 mg/m2
Ara-C 1000 mg/m2
Intermediate risk
MRD-
Good risk
Poor
+/- experimental drug: Lenalidomide
MRD +
MRD -
Poor risk
Very poor risk Very poor
MRD +
Poor
Very poor
Int
MRD evaluation
After Cycle IIAuto-Tx Allo-Tx
HO132 AML study: risk adapted consolidation based on MRD after induction cycle II

MRD by NPM1 identifies distinct outcomes in AML and is influenced by gemtuzumab ozogamicin (ALFA-0701 trial).
91%
61%
39%
7%
Lambert J, et al, Oncotarget 2014;5:6280-6288
• Add. of GO no increaseof CR
• Add. of GO improves 2y OS and EFS
• MRD might be useful as surrogate marker in new drug development

MRD directed treatment in CBF AML:Trial design and patient accrual flowchart.
Hong-Hu Zhu et al. Blood 2013;121:4056-4062

Hong-Hu Zhu et al. Blood 2013;121:4056-4062
MRD directed treatment in CBF AML

Ara-C 200mg/m2 d1-7c.i.
Idarubicin 12 mg/m2 3-hr d1-3
Ara-C 1000mg/m2 3-hr bid d1-6
Amsacrine 120 mg/m2 iv d4, 5, 6
R
Cycle III, autoSCT, alloSCT
Ara-C 200mg/m2 d1-7c.i.
Idarubicin 12 mg/m2 3-hr d1-3
Clofarabine 10 mg/m2 days 1-5
Ara-C 1000mg/m2 3-hr bid d1-6
Amsacrine 120 mg/m2 iv d4, 5, 6
Clofarabine, 10 mg/m2iv days 1-5
HOVON-SAKK AML-102 phase III study in AML/RAEB, 18-65 yrs

Lowenberg B et al., Blood 2017;129:1636-1645
Clofarabine in AML (HOVON102)

MRD status correlates with clinical results of HOVON 102 trial
MRD Status
Control arm
Clofarabine Total
Negative 24(53%) 34(77%) 58(65%)
Positive 21(47%) 10(23%) 31(35%)
P=0.018
Lowenberg B et al., Blood 2017;129:1636-1645

Conclusions: MRD YES!
• Provide objective methodology to establish remission status
• Refine outcome prediction and may inform post remission treatment: randomized studies should be performed
• Identify impending relapse to enable early intervention: randomized studies still to be performed
• Post-transplant surveillance with early intervention (IS/DLI)
• Surrogate endpoint to fasten drug approval
Schuurhuis GJ, et al., Blood 2018;131:1275

47
Department of Hematology VU University Medical Center, CCA
Amsterdam, Netherlands
Wendelien ZeijlemakerAngèle KelderWillemijn Scholten Sander Snel Monique TerwijnYvonne Oussoren-Brockhoff
Dennis VeldhuizenArjo RuttenJannemieke HamDiana HanekampGert Ossenkoppele Jacqueline CloosGerrit Jan Schuurhuis
All patients> 50 centers