Embed Size (px)
Citation preview

Minimal Residual Disease assessment inMultiple Myeloma by Next-Generation Sequencing
:Prof Hervé AVET-LOISEAU, MD, PhDInstitut Universitaire du Cancer
Toulouse, France
MRD Meta-Analysis in Myeloma Nikhil Munshi, MD
Lipper Myeloma CenterDana-Farber Cancer Institute

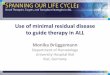
Why to assess MRD in Myeloma?The main rationale is the correlation response/outcome
CR, n=278
nCR, n=124PR, n=280
PD, n=25
0 12 24 36 48 60 72 84 96
Months from diagnosis
0,1
0,2
0,3
0,4
0,5
0,6
0,7
0,8
0,9
1,0
Cum
ulat
ive
Prop
ortio
n Su
rviv
ing
RC vs TBRP RC vs RP TBRC vs RP
P=0.01P<10-6
P=0.04
OS
Lahuerta et al. JCO 2008
CR nCR PR PDMedians EFS, months 61 40 34 13Medians OS, months NR NR 61 15

Why to assess MRD in Myeloma?Treatment advances have increased the likelihood of achieving CR.

Why to assess MRD in Myeloma?However, a large majority of pts with CR eventually relapse, suggesting that undetectable, but clinically meaningful MRD may be present.

Why to assess MRD in Myeloma?
Diagnosis 1012
CR 1010 80% HD trials

MRD: What are the techniques?
(Old) Gold Standard: Multiparametric Flow Cytometry
Myeloma cells present a specific phenotype / normal PC
This phenotype is stable during evolution
clonal PCs
normal PCs
PCA1
PCA
2
clonal PCs
normal PCs

MRD: What are the techniques?
Next-Generation Sequencing
Myeloma cells present unique Ig gene rearrangements
These clonal rearrangements are stable during evolution

Locus IGK 2p11
Mix J
Locus IGH 14q32
Mix B Mix CMix E
Mix J
Allèle IgH fonctionnelhypermuté
Functional Allele
Non-Functional allele
Mix D
Mix J
NGS: Technical principles

Non B cell LeukocytesNormal B cellsMyeloma cells
FREQUENCY OF MYELOMA CLONE
AMONG B CELLS = SL / (SL + SB)NUMBER OF MYELOMA MOLECULESPER LEUKOCYTE = SL x (NR/SR) / NTOT
NGS: Technical principles

Is MRD clinically pertinent?

BLOOD, 19 JANUARY 2012 - VOLUME 119, NUMBER 3
BLOOD, 15 MAY 2014 - VOLUME 123, NUMBER 20

Significant Impact of Minimal Residual Disease (MRD) Status On Survival Outcomes In pts (pts) With
Multiple Myeloma (MM) Who Achieve Complete Response (CR): A Meta-Analysis
• A total of 405 published articles with MRD– 25 articles recently published articles
• Of these, 21 reported overall survival (OS) or progression-free survival (PFS) results, as well as MRD status
• Overall, 2,208 pts were evaluated for MRD• Nine publications reported conventional CR at the time of
MRD measurement. Six represented unique data sets.
Munshi N et al., JAMA Oncol, in press

MM, multiple myeloma; MRD, minimal residual disease; SCT, stem cell transplant.
Refining the literature search
Exclusion criteria• Publications were excluded if they:
– Only included patients with relapsed and/or refractory MM
– Included patients who had undergone allogenic SCT– Assessed MRD in apheresis product – Reported on the same study population used in an
already-included trial• Analysis was restricted to techniques with a
detection limit of≤ 0.01%

496
496
1,329
1,515
0 500 1,000 1,500 2,000
Patientsassessed
for OS
Patientsassessedfor PFS
Number of patients assessed
Any response-achievingpatients (n = 13 studies)
CR-achieving patients(n = 4 studies)
21 articles retrieved in total
Number of patients with PFS and OS data allowing for analysis
1. Paiva B, et al. J Clin Oncol. 2011;29:1627-33.2. Paiva B, et al. Blood. 2012;119:687-91.
3. Rawstron AC, et al. J Clin Oncol. 2013;31:2540-7.4. Swedin A, et al. Br J Haematol. 1998;103:1145-51.OS, overall survival; PFS, progression-free survival.
Munshi N et al., JAMA Oncol, in press

The effect of MRD status on PFS and OS (All patients)
Munshi N et al., JAMA Oncol, in press

The effect of MRD status on PFS and OS(All patients)
Munshi N et al., JAMA Oncol, in press

The effect of MRD status on PFS and OS (CR patients)
Munshi N et al., JAMA Oncol, in press

18
The effect of MRD status on PFS (CR patients)
Data are adjusted for different proportions of patients being MRD-positive and MRD-negative by study.
100
80
60
40
20
00 2 4 6 8 10 12
Time (years)
PFS
(%)
2 (adjusted) = 35.85;P < 0.0001
MRD-negative (n=389)MRD-positive (n=155)
Number at risk by year:389 359 301 211 155 96 65 35 16 12 1155 129 86 51 33 19 12 7 7 5 0
• 3-year PFS: 70% (MRD–) vs. 46% (MRD+)
• 5-year PFS: 48% (MRD–) vs. 27% (MRD+)
• Majority of MRD-positive patients progressed by 6 years; nearly 50% of MRD-negative patients progression free
CR patients Median PFSMRD-negative 56 monthsMRD-positive 34 months
CR-achieving patients
Munshi N et al., JAMA Oncol, in press

Munshi N, et al. IMW 2015, abstract 0394.
Data are adjusted for different proportions of patients being MRD-positive and MRD-negative by study.
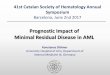
The effect of MRD status on OS (CR patients)
CR, complete response; MRD, minimal residual disease; NR, not reached; OS, overall survival.
100
80
60
40
20
00 2 4 6 8 10 12
Time (years)
OS
(%)
2 (adjusted) = 15.06;P < 0.0001
MRD-negative (n=362)MRD-positive (n=134)
Number at risk by year:362 359 331 274 218 138 76 34 8 3 1134 131 111 81 55 35 20 10 5 5 2
• Median OS was not reached for MRD-negative pts versus 82 months for MRD-positive pts)
• OS @ 3-years, 94% versus 80% OS @ 7-years, 67% versus 47%• OS @ 5-years, 80% versus 61%
CR patients Median OSMRD-negative 112 monthsMRD-positive 82 months
CR-achieving patients
19

Conclusions of the meta-analysis
MRD is definitely predictive of both longer PFS and OS
Most of the available results are from MFC
MFC has a quite low sensitivity (10-4)
Following question:
Would a higher sensitivity have a better predictivity?

Higher sensitivity: NGS
Martinez-Lopez J et al., Blood 2014;123:3073

IFM DFCI 2009 Trial700 patients < 66y,
Newly diagnosed symptomatic MM
3 RVD
5 RVD MEL200 + ASCT
2 RVD
12 months Lenalidomide maintenance
MRD*
MRD*
MRD*
MRD** Primary objective = 7-color Flow, Secondary objective = Molecular

54% Conventional CR
289 patients analyzed by NGS
Applicability of NGS: 92% (8% clone ID failure)
Median follow-up: 44 months
IFM 2009 trial

P-value (trend) : p<0.0001
<10-6
[10-6;10-5[
[10-5;10-4[
>=10-4
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1.0
Patie
nts
with
out p
rogr
essi
on (%
)
79 79(0) 70(9) 59(11) 50(9) 38(11) 28(6) 6(9) 0(3)[10-4;10-3[49 49(0) 47(2) 45(2) 43(2) 34(7) 22(4) 8(6) 2(0)[10-5;10-4[31 31(0) 30(1) 28(2) 27(0) 22(4) 17(1) 8(2) 4(1)[10-6;10-5[87 87(0) 87(0) 85(2) 83(2) 74(6) 54(4) 31(3) 8(0)<10-6
N at risk(events)
06
1218
2430
3642
48
Months since randomization
MRD at pre-maintenance
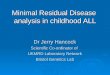
IFM 2009 trial

P-value (trend) : p<0.0001
<10-6
[10-6;10-5[[10-5;10-4[
>=10-4
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1.0
Patie
nts
with
out p
rogr
essi
on (%
)
40 40(0) 40(0) 40(0) 33(6) 23(9) 15(6) 4(4) 2(1)[10-4;10-3[23 23(0) 23(0) 23(0) 22(1) 19(3) 14(2) 3(5) 2(0)[10-5;10-4[29 29(0) 29(0) 29(0) 28(0) 22(5) 16(3) 4(4) 1(1)[10-6;10-5[86 86(0) 86(0) 86(0) 86(0) 77(5) 61(3) 36(5) 10(0)<10-6
N at risk(events)
06
1218
2430
3642
48
Months since randomization
MRD at post-maintenance
IFM 2009 trial

P-value : p<0.0001
Negative (<10-6)
Positive
0.0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1.0
Patie
nts
with
out p
rogr
essi
on (%
)
159 159(0) 147(12) 132(15) 120(11) 94(22) 67(11) 22(17) 6(4)MRD positive87 87(0) 87(0) 85(2) 83(2) 74(6) 54(4) 31(3) 8(0)MRD neg (<10-6)
N at risk(events)
06
1218
2430
3642
48
Months since randomization
MRD at pre-maintenance
IFM 2009 trialFCM Negative Patients

P-value : p<0.0001
Negative (<10-6)
Positive
0.0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1.0
Patie
nts
with
out p
rogr
essi
on (%
)
92 92(0) 92(0) 92(0) 83(7) 64(17) 45(11) 11(13) 5(1)MRD positive86 86(0) 86(0) 86(0) 86(0) 77(5) 61(3) 36(5) 10(0)MRD neg (<10-6)
N at risk(events)
06
1218
2430
3642
48
Months since randomization
MRD at post-maintenance
IFM 2009 trialFCM Negative Patients

MRD by NGS vs MFC
NGS• Highly sensitive (> 10-6)• Standardized• Informative in 92% of pts• Frozen samples
FCM• Less sensitive (10-5)• Many different panels• Informative in 100% of pts• Fresh samples

Conclusions
The highest sensitivity is the most discriminant 10-6 is required
NGS is probably the technique of choice
MFC should be used in case of clone ID failure
MRD could (should?) be the main objective of future trials
MRD could identify cured patients

Conclusions
Limitations: MRD evaluates MM in one BM region
What about other regions?
Solutions:
• cfDNA sequencing analyses? ongoing• Imaging techniques: PET-TDM+++

Bartel et al. Blood 2009;114:2068-2076

Zamagni et al, Blood 2011;118:5989-5995

IFM 2009 trialPET‐CT normalisation before maintenance
Impact on PFS (62% normalised)
p < 0.001
69%
51.6%

Conclusions
New concepts in assessment of response in MM
IMWG consensus (Kumar S et al., Lancet Oncol, in press)
- MRD in BM with the most sensitive technique
- PET-TDM