Embed Size (px)
Citation preview

Milta Oyola Little, D.O. CMDSaint Louis University
PROGNOSTICATION AND UPDATED HOSPICE REGULATIONS IN CARE PLANNING FOR FRAIL ELDERS

Speaker DisclosuresDr. Little has disclosed that she has no relevant financial relationship(s).
Dr. Little will not be discussing any off-label or unapproved medications or therapies.

Objectives• By the end of the session, participants will be
able to
o Describe how trends in hospice utilization affect patient quality outcomes, Medicare reimbursement, and the development of models of care.
o Describe the proposed demonstration projects and changes to Medicare hospice reimbursement.
o List available prognostication tools to assist with clinical decision-making.

?
Created By: Medical College of Wisconsin. Available at POGOe.org, Assessed 2/16/14

Medicare Hospice Benefit
• Established in 1982 for high-quality end-of-life care
• Eligibilityo Medicare Part Ao Terminal illness (6 months or less if illness runs its natural
course)o Forgo intensive medical interventions of curative intent
• Benefit Periodo Two 90 day periods, followed by unlimited 60 day periodso Initial certification by two physicianso Recertification by hospice physician

Trends in Hospice Use• In 2012, ~1.5-1.6 million patients received
hospice services
Hospice Care in America. NHPCO Facts and Figures, 2013

Trends in Hospice Use• Cancer diagnoses now account for less than half
of all hospice admissions
Hospice Care in America. NHPCO Facts and Figures, 2013

Hospice Use in the NH
Miller SC, et al. JAGS 2010; 58:1482-1488
NEED FOR BETTERPROGNOSTICATION!

Hospice Use in the NH• Better pain management• Fewer hospitalizations• Greater family satisfaction with care at end-of-life• Lower cost across all time periods
Kelley AS, et al. Health Affairs 2013; 32(3):552-561
Miller SC, et al. JAGS 2010; 58:1482-1488

Recent Changes to the Medicare Hospice
Benefit

Medicare is Watching You
• OIG Reporto Federal oversight lackingo High deficiency rate
• NH Utilization Trendso Nebulous diagnoseso Increased Medicare expenditureso Effectiveness of NH-Hospice collaborations
OIG, “Medicare Hospices: Certification and Centers for Medicare & Medicaid Services Oversight,” OEI-06-05-00260, Apr 2007
OIG, “Medicare Hospice Care for Beneficiaries in Nursing Facilities: Compliance With Medicare Coverage Requirements,” OEI-02-06-00221,
Sept 2009
“We found that 82% of hospice claims for beneficiaries in nursing facilities in 2006 did not meet Medicare coverage requirements. Medicare paid approximately $1.8 billion for these claims. …raises concerns about the services that Medicare is paying for and the quality of care that hospices are providing to beneficiaries during their last months of life.”

How Reimbursement Currently Works
• All-inclusive per diem rateo Routine home care**o General inpatient careo Continuous careo Respite care
• Not adjusted for case-mix or NH setting
• Medicare caps aggregate payments
Huskamp HA, et al. Health Affairs 2010; 29(1):130-135
Hospice Care in America. NHPCO Facts and Figures, 2013

Proposed Changes to Reimbursement
• Move away from flat per diem rate
• Consideration for different payment structure for hospice care in the nursing home (being studied)
Enrollment
Active dying phase
Medpac Report to the Congress. Reforming Medicare’s Hospice Benefits 2009; Chap 6:347-376

Medpac Report to the Congress. Reforming Medicare’s Hospice Benefits 2009; Chap 6:347-376

Recent Reimbursement
Changes
• Failure to meet quality reporting requirement will result in 2% reduction in 2014 Market basket updateo NQF #0209: Pain Managemento Participation in QAPI with >3 quality indicators related to patient
careCMS Federal Register. FY2014 Hospice wage index and payment rate update 2013; 78(152):48234-48281
The Medicare Hospice Benefit. hospiceactionnetwork.org

Recent Regulatory Changes
• Brief Physician Narrative: Effective Oct 1, 2009
• Face-to-Face Encounter: Effective Jan 1, 2011
• 100% Medical Review of Certain Patients: Effective Jan 1, 2011
• Ineligible ICD-9 codes under “Symptoms, Signs and Ill-Defined Conditions” and “Mental, Behavioral and Neurodevelopmental Disorders”
The Medicare Hospice Benefit. hospiceactionnetwork.orgCMS Federal Register. FY2014 Hospice wage index and payment rate update 2013; 78(152):48234-48281


CMS Federal Register. FY2014 Hospice wage index and payment rate update 2013; 78(152):48234-48281

Proposed Models of Care
Concurrent Care Demonstration Projects
End-of-Life Benefit

Concurrent Care Demonstration
Hospice Care
Hospice Care
6 months
No Time Requirement
alongside
Curative
Curative

ACA Sec. 3140Medicare Hospice Concurrent Care
Demonstration Program • 3-year projects
• Modification of existing eligibility criteriao To reduce very short hospice stays (reduce delay in enrollment)o Test of need for palliative care without strict prognostic
requirement o Greater access for certain underserved groups
• To measure effects of concurrent care on cost, access, quality of care, and survival
Casarett DJ. JAMA 2011; 305(10):1031-1032

ACA Sec. 3140
Medicare Hospice Concurrent
Care Demonstration Program
• DiagnosesoCOPD, CHF, HIV/AIDS, Cancero Fact Sheet
• LimitationsoNH patients not eligibleoDementia diagnoses excluded

End of Life Benefit• Modified program for LTC residents
o Drops 6-month prognostic requiremento Drops requirement to forgo curative treatmentso Combination of palliative and psychosocial-spiritual support
• Supplemental payments made directly to NHo End-of-life services “carved-in” and adjusted to needo Provide care directly or contract with local hospiceo NH accountable for quality of care – quality indicators TBD
• Threshold for patient eligibility TBD
Huskamp HA, et al. Health Affairs 2010; 29(1):130-135

Prognostication Issues

“Difficult to see. Always in motion is the future”
Slide used with permission, courtesy of Eric Widera, MD

Dying is Individual
Lynn J, Adamson DM. Living well at the end of life. Adapting health care to serious chronic illness in old age. Washington: Rand Health, 2003
Lunney, J. R. et al. JAMA 2003;289:2387-2392

What is Prognostication?
Foreseeing(determining)
Foretelling(relaying)
Slide used with permission, courtesy of Lindy Landzaat, DO

Why Prognosticate?• Hospice eligibility
• Goals of care
• Advanced care planning (financial, ADL)
• Resource allocation
• Clinical decision-making
Alrawi YA, et al. Q J Med 2013; 106:51-57Chan TC, et al. Geriatr Gerontol Int 2012; 12:555-562Widera E, et al. JAMA 2011; 305(7):698-706. Yourman LC, et al. JAMA 2012; 307(2):182-192

Ways to Prognosticate
Clinical Judgment
Slide used with permission, courtesy of Eric Widera, MD

Shortcomings of Clinical
Predictions
• Tend to overestimate patient survival by a factor of between 3 and 5.
• Tend to be more accurate for very short-term prognosis than long-term prognosis.
• Influenced by relationships
Slide used with permission, courtesy of Eric Widera, MD
Christakis NA and Lamont EB. BMJ. 2000 Feb 19;320(7233):469-72

Ways to Prognosticate
Clinical Judgment
Life Tables
Slide used with permission, courtesy of Eric Widera, MD

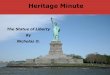
Great Variation in Life
Expectancy
for People of Similar Ages
0
5
10
15
20
25
70 75 80 85 90
Top 25th Percentile
50th Percentile
Lowest 25th Percentile
Age (years)
Years
Walter LC. JAMA 2001;285:2750-56
Life Expectancy for Women
Slide used with permission, courtesy of Eric Widera, MD

Use Functional Status
Life Expectancy (years)
AgeIndepende
ntMobility disabled
ADL disabled
70 16.7 15.7 11.5
75 13.2 12 8.2
80 10.3 9 6
85 8 6.9 4.6
Keeler et al. J Gerontol A Biol Sci Med Sci. 2010
Slide used with permission, courtesy of Eric Widera, MD

Prognostication is more accurate if you
combine clinical judgment with life tables, functional
status and comorbid conditions
Walter LC. JAMA 2001;285:2750-56Christakis & Iwashyna, Arch Intern Med 1998Keeler et al. J Gerontol A Biol Sci Med 2010McGinn, JAMA 2000

Ways to Prognosticate
Clinical Judgment
Life Tables Prognostic Indices
Slide used with permission, courtesy of Eric Widera, MD

Prognostic Indices
Physicians can use prognostic indices to lend confidence to their judgments about prognosis
National survey of 697 physicians: 57% felt inadequately trained in prognostication
Christakis & Iwashyna, Arch Intern Med 1998
Slide used with permission, courtesy of Eric Widera, MD

• Identified 16 validated non-disease specific prognostic indices for older adults• 6 for community dwelling adults• 2 for nursing home• 8 for hospitalized patients
• Results used to form ePrognosis.ucsf.edu
Yourman LC, et al. JAMA 2012; 307(2):182-192


Used with permission, courtesy of Eric Widera, MD

• Identified 8 risk factors
• ROC 0.76
• Compared to Flacker long-stay NH index (ROC 0.73)
Chan TC, et al. Geriatr Gerontol Int 2012; 12:555-562

?
Created By: Medical College of Wisconsin. Available at POGOe.org, Assessed 2/16/14
How do Prognostic IndicesCompare to MedicareHospice Guidelines?

Medicare Hospice Criteria for Dementia
• Stage 7 or beyond on the Functional Assessment Staging Scale (FAST)
• One of the following within the past 12 mo:o Aspiration pneumoniao Pyelonephritis or other upper UTIo Septicemiao Decubitus ulcers, multiple, stage 3-4o Fever, recurrent after antibioticso Inability to maintain sufficient fluid and calorie intake with 10%
weight loss during the previous six months or serum albumin < 2.5

• C-statistic for ADEPT 0.62-0.72
• C-statistic for Medicare hospice eligibility 0.55
Mitchell, SL, et al. JAMA 2010; 304(17):1925-1935

Prognostication: limitations
• Medicare hospice criteria are guidelines, not hard and fast rules
• Indices may have limited clinical utility outside of the population in which they were created
• Indices based on MDS 2.0 or ICD-9 codes no longer useful as data management changes
• Questionable discriminatory ability of indices
Yourman LC, et al. JAMA 2012; 307(2):182-192

Used with Permission

Acknowledgements• A special thank you to those who shared
articles, web resources, slides and supporto Amy Corcoran, MD, CMD – U of Pennsylvaniao Eric Widera, MD – U of California San Franciscoo Lindy Lanzaat, DO – U of Kansas Medical Centero Paul Tatum, MD – U of Missouri