Embed Size (px)
Citation preview
Journal of Intellectual Disability Research
pp
‒
©
Blackwell Publishing Ltd
663
Blackwell Science, LtdOxford, UKJIRJournal of Intellectual Disability Research1365-2788Blackwell Publishing Ltd, 2003
7663671
Original Article
Intellectual disability in Pakistani children
M. Yaqoob
et al.
Correspondence: Dr Muhammad Yaqoob, Department of Paediatrics, Maternity and Children’s Hospital, PO Box
Buraidah, Al-Qassim, Saudi Arabia (e-mail: drmyaqoob
@hotmail.com).
Mild intellectual disability in children in Lahore, Pakistan: Aetiology and risk factors
M. Yaqoob,
1
A. Bashir,
2
S. Zaman,
3
H. Ferngren,
4
U. von Dobeln
5
& K.-H. Gustavson
6
1
Department of Paediatrics, Maternity and Children’s Hospital, Al-Qassim, Saudi Arabia
2
Department of Psychiatry and Behavioural Sciences, University College London, London, UK
3
Department of Preventive Paediatrics, King Edward Medical College/Mayo Hospital, Lahore, Pakistan
4
Department of Paediatrics, Astrid Lingrens Children’s Hospital, Karolinska Hospital, Stockholm, Sweden
5
Department of Clinical Chemistry, Hudding’s University Hospital, Hudding, Sweden
6
Department of Clinical Genetics, Rudbeck Laboratory, Uppsala University, Uppsala, Sweden
Abstract
Background
One of the main objectives of studying intellectual disability (ID) in children is to explore its causes. A specific aetiological diagnosis is important in determining the prognosis, nature and extent of services needed to support affected children.
Methods
Aetiology and risk factors in mild ID were studied in a cohort of longitudinally followed chil-dren (
–
years of age,
n
=
) in four population groups in and around Lahore, Pakistan.
Results
The overall prevalence of mild ID was
.
%. In
% of the cases the onset of mild ID was prenatal with small for gestational age and multifactorial inheritance as the main underlying factors. During the postnatal period (
% of the cases), social depri-vation and malnutrition were the major causes of ID. In a substantial proportion of the cases (
%), the cause of ID could not be traced.
Conclusion
The present study indicates a clear rela-tionship of mild ID with prenatal and postnatal mal-nutrition and social deprivation. Two independent variables, maternal illiteracy and small head circum-ference at birth, showed a clear association with the development of mild mental disability among chil-dren in the study population.
Keywords
head circumference at birth, malnutrition, maternal education, mild intellectual disability, social deprivation
Introduction
One of the main objectives of studying intellectual disability (ID) in children is to explore its causes. A specific aetiological diagnosis is important in deter-mining the prognosis, nature and extent of services needed to support affected children. The cause of ID may be obvious as is often the case with severe ID or untraceable especially in individuals with mild ID.
The causes of mild ID have been studied exten-sively predominantly in Western industrialized coun-tries (Crocker
). Prenatal factors have been reported as the most common,
–
%, mostly result-

Journal of Intellectual Disability Research
M. Yaqoob
et al
. •
Intellectual disability in Pakistani children664
©
Blackwell Publishing Ltd,
Journal of Intellectual Disability Research
,
‒
ing in Down syndrome, small for gestational age, hypoxic-ischaemic encephalopathy, prematurity, infections and multifactorial conditions. Postnatal causes were found less frequently,
–
%. In spite of extensive diagnostic work-up in most of these studies, the aetiology remained unknown in a large propor-tion of the cases,
–
% (Blomquist
et al.
; Hagberg
et al.
; von Wendt & Rantakallio
; Al-Ansari
; Matilainen
et al.
; Fernell
; Stromme & Hagberg
; Christianson
et al.
).Published reports on the aetiology of mild ID in
Pakistani children are scarce. A hospital-based study reported a high frequency of infectious aetiology fol-lowed by recessive genetic disorders as the main cause of ID in children (Malik
et al.
). A com-munity survey conducted in Karachi showed social class and consanguineous marriages as important risk factors for mild ID in children (Stein
et al.
). Those studies lack attempts to establish diagnosis based upon more extensive laboratory investigations like chromosomal and metabolic screening. A population-based investigation of children in four population groups in and around Lahore, Pakistan, provided an opportunity to study the epidemiology of severe ID (Yaqoob
et al.
) as well as of mild ID. The prevalence of mild ID and its associated impairments are presented elsewhere (Bashir
et al.
). The aim of the present paper is to present the aetiology and risk factors of mild ID among children in the study population.
Materials and methods
Study areas
The four study areas represented different stages of urbanization: a village, a periurban slum, an urban slum and an upper middle (UM) class group. The socio-economic background of the population belonging to these areas is described in detail else-where (Jalil
et al.
). However, a brief description of these areas is given below.
Most of the villagers were uneducated farmers, and a few were shopkeepers, blacksmiths, carpenters and masons. At the beginning of the study the village population was roughly
in
households. The economy of the village was largely dependent on agriculture. Births were assisted by untrained birth attendants. Most women were housewives. The illit-eracy rate was high:
% for men and
% for
women. There are two primary schools in the village with poor attendance. There was no health facility. An unqualified medical practitioner and a faith healer were consulted for all medical problems. In
% of the families the monthly income was less than Rs
(US$
). Mean family size was seven.The total population in the periurban area was also
about
in
households. The people in this area had migrated from villages and small towns to Lahore city in search of jobs. Mostly people were unskilled labourers, shopkeepers and beggars with
.
% adult literacy rate. The people were living in houses made of mud and straw (
%). The deliveries were conducted by untrained birth attendants or old females in the family. The sanitary conditions of this area were very poor. Health facilities were available in the vicinity but probably due to poverty and igno-rance people usually consulted local unqualified medical practitioners.
The population in the urban inner city area was also about
in
households. This group com-prised of low to middle class businessmen and low grade government servants living with their families in multistorey buildings along narrow streets. The sanitary conditions were poor. The literacy rate was
% for men and
% for women. Some women attended hospital for delivery but most of deliveries were conducted at home by traditional birth attendants.
The UM class group was registered to compare underprivileged with the privileged group. This group was scattered over the city in well-off localities. The contact with these families was made at the private clinics of obstetricians where these mothers came for antenatal check-ups during the second trimester of their pregnancies. The inclusion criteria for these families were a monthly income more than Rs
(US$
), owning a house with at least three bed rooms, not more than two children, and at least
years schooling for both the parents (Jalil
et al.
).
Study population
From March
to August
a door-to-door survey was conducted in three poor areas. The num-ber of families selected in each area was about
. All pregnancies likely to end after
September
were registered. Periodic registration and follow-up

Journal of Intellectual Disability Research
M. Yaqoob
et al
. •
Intellectual disability in Pakistani children665
©
Blackwell Publishing Ltd,
Journal of Intellectual Disability Research
,
‒
of new pregnancies continued till October
. In the UM class
expectant mothers were registered according to the above-mentioned preset criteria. During this period
pregnant mothers were recruited in the four study areas. Pregnancies in the poor areas were followed by trained female health visitors. During antenatal visits, the information regarding factors that were considered to affect devel-opment of a child during prenatal period was recorded on a structured questionnaire.
Of the
registered pregnant women,
(
%) left the study areas before delivery. The remaining resulted in
live births and
stillbirths. There were
twin pregnancies. All live-born infants in the four areas were followed by monthly home visits from birth to
years and then less frequently till years of age. The home visits were made by female health visitors supervised by field doctors to record different parameters of child health such as psychomotor development, congenital malformations, feeding pat-terns, growth, infectious diseases, morbidity and mortality. Necessary information regarding perinatal events that could affect the mental health of an infant was recorded by a doctor during the first home visit after birth.
The IQ testing of children was started in January when some of the children reached between and years of age. Out of children, % died within years of life. Because of high turnover of the population, % of the children either left the study areas or the parents refused to continue the study. So information of the present study is based upon a group of children ( males, females).
The controls were identified from the same study population. The controls had normal IQ and adaptive function. They were closely matched with cases regarding age, sex and living area. With these match-ing criteria, five controls were identified for each case.
Definitions
Intellectual disability was defined as a below average general intellectual functioning existing concurrently with a deficit in adaptive behaviour and manifested during the developmental period (Moser et al. ). Intellectual function was measured by well-known intelligence tests (WISC and Griffith’s). For mild ID the selected IQ ranged from to inclusive. Mother’s age was defined as age in years at the time
of the pregnancy. Maternal age was estimated in poor areas with the help of calendars of local events. Par-ents of an index case were consanguineously married if they had at least one ancestor in common. The level of consanguinity was ascertained by interviewing mother/other relatives of each child. A neonate was labelled as full-term if gestational age was between and weeks inclusive. Gestational age was com-puted by the information on the last menstrual period and date of birth and was counter-checked when doctors examined the child at the time of birth and assessed the gestational age using Dubowitz chart (Dubowitz et al. ). Asphyxia was defined as an Apgar score less than at min for children born in hospitals. For home deliveries, asphyxia was diag-nosed only when there was a definite history of late cry, slow and/or gasping respiration, drowsiness, poor sucking and long-standing cyanosis in a newborn. Epilepsy was defined as recurrent epileptic seizures. Febrile convulsions were not included in this cate-gory. Cerebral palsy was defined as ‘a disorder of movement and posture due to a non-progressive defect or lesion of the immature brain’ (Bax ). Psychological deprivation and neglect was decided on the basis of () lack of interest of parents in child’s education (either schooling or home based coaching); () social deprivation in the form of poor hygiene, malnutrition, physical and emotional neglect; and () lack of stimulation to enhance child’s verbal compre-hension and formal cognitive abilities. Nutritional status at birth was assessed by using National Center for Health Statistics (NCHS) [USA] standards. New-borns of weight less than - SDS (standard deviation score) were labelled as small for gestational age. However, for postnatal malnutrition the inclusion cri-terion was weight less than - SD (standard devia-tion), that is, weight % or less than expected (WHO ). Weight at birth was measured to the nearest g with minimal clothing. Length and head circumference were measured to the nearest mm (Jalil et al. ).
Case ascertainment
A three stage screening method was used to identify children with mild ID. In the first stage Ten Questions Screening (TQS) with additional probes was applied (Bashir et al. ). Of the children screened by TQS, (.%) were found to have disability like

Journal of Intellectual Disability Research
M. Yaqoob et al. • Intellectual disability in Pakistani children666
© Blackwell Publishing Ltd, Journal of Intellectual Disability Research , ‒
speech disorder, hearing difficulty, learning difficulty, fits, impairment of vision, motor disability or diffi-culty in comprehension and response. TQS was applied by the psychologist. In the second stage, those children were subjected to the Weschler Intelligence Scale for Children-Revised (WISC-R) to assess their intelligence. WISC-R was also applied by the field psychologist. At the end of this screening, (.%) children were found to have IQ ranging from to . In the third stage, a team consisting of a paediatrician, child psychiatrist and psychologist assessed adaptive functioning of each child with IQ ranging from to . The adaptive functioning was assessed on the basis of detailed interview with the parents or relevant caretakers of the child. The adap-tive functioning included performance and adaptabil-ity in school, adaptability with peers, and ability to adjust to an expected social role within the family as compared to other siblings of the same family. Forty children were found having adaptive malfunctioning and so were declared as suffering from mild ID.
Altogether there were matched controls and affected children in the study, so the final total for the sample was .
Laboratory methods
Dried blood samples on filter paper were screened for phenylketonuria (PKU), galactosaemia and congeni-tal hypothyroidism (Alm & Larsson ). Screening for hypothyroidism was performed by measurement of thyroid stimulating hormone by fluoroimmunoas-say (Torresani & Scherz ). For the identification of children with PKU phenylalanine was quantified. The screening for galactosaemia was performed by a semi-quantitative determination of the deficient enzyme galactose--phosphate-uridyl transferase fol-lowed by determination of the concentrations of galactose and galactose--phosphate when the enzy-matic activity was lower than % of the controls (Therell ). Chromosomal analysis was carried out using Giemsa banding techniques. DNA-based molecular screening for Fragile-X was used to iden-tify affected male children.
Aetiological classification
Children with mild ID were classified into four groups according to the main period in which the
insult causing the ID was thought to have occurred: () prenatal, from the first day of the last menstrual period to the onset of delivery (The aetiology was considered multifactorial if first-degree relatives also suffered from mild ID and/or there was no obvious cause of ID in the child or relatives. The ID in these cases was considered as probably polygenically inher-ited but environmental influences were also possi-ble.); () perinatal, during or within days of delivery; () postnatal, from day after delivery to years of age; and () untraceable.
Statistical analysis
A battery of factors considered to be risk factors for the development of mild ID in children were selected for analysis, that is, maternal age, parity, sex, gestational age, monthly income, weight, length and head circumference at birth, consanguinity of the parents, mother’s and father’s education. These vari-ables were treated categorically in the analysis. Mother’s age was stratified into two groups: years and less, more than years. Parity was defined as number of viable pregnancies and stratified into two categories: women with less than four pregnancies and women with four or more pregnancies. Sex was dichotomized as male or female. Gestational age was also divided into two categories: gestational age less than weeks and weeks and more. Monthly income was also divided into two categories: income less than Rs (US$) and Rs and more. Consanguinity was categorized as related marriages (union between first-cousins, double first-cousins, first-cousins once removed, second-cousins, or second-cousins once removed) and unrelated mar-riages. Education level for both father and mother was stratified into two categories: illiterate and those who could read and write.
The dependent variable was dichotomized into cases and controls.
A bivariate analysis was performed using each independent variable separately. A Chi-square test with one degree of freedom was used with an alpha level at . and odds ratio was calculated with % confidence intervals for each (analysis not shown). This was followed by multivariate analysis using mul-tiple logistic regression model to explain the relation-ship between independent and dependent variables after controlling the confounders. An alpha level of
Journal of Intellectual Disability Research
M. Yaqoob et al. • Intellectual disability in Pakistani children667
© Blackwell Publishing Ltd, Journal of Intellectual Disability Research , ‒
. in two tails was used to identify the significant factors. Parameter estimates and their standard errors were calculated (Schlesselman )
Results
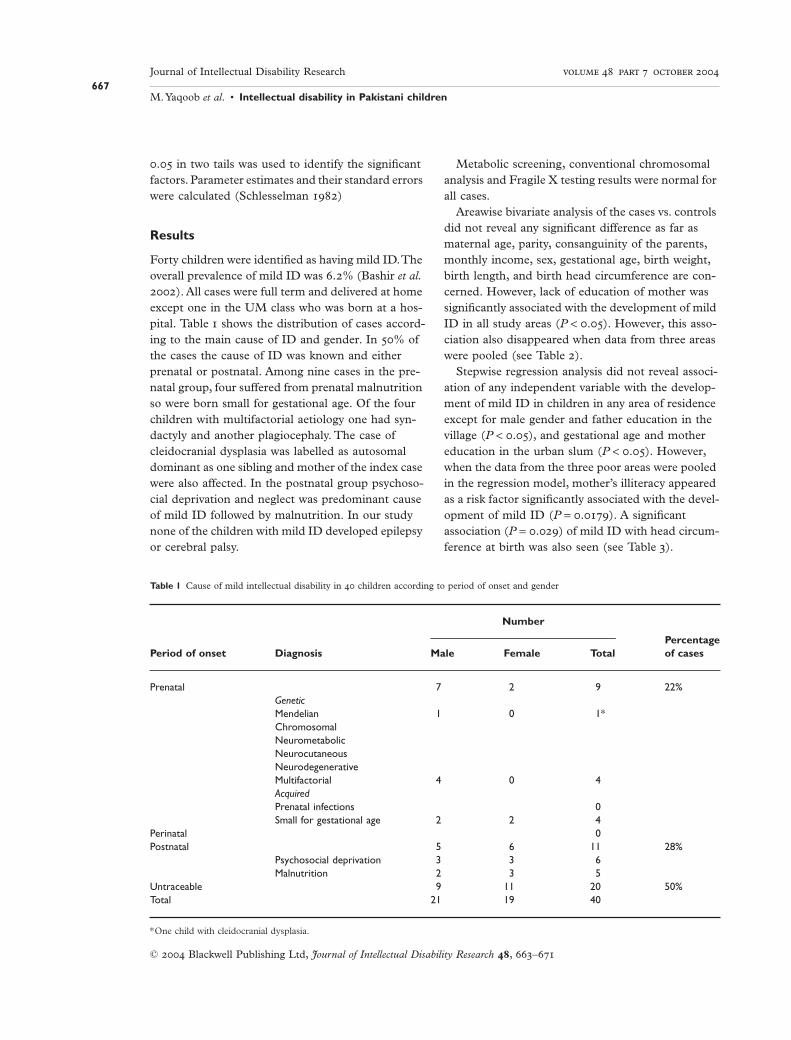
Forty children were identified as having mild ID. The overall prevalence of mild ID was .% (Bashir et al. ). All cases were full term and delivered at home except one in the UM class who was born at a hos-pital. Table shows the distribution of cases accord-ing to the main cause of ID and gender. In % of the cases the cause of ID was known and either prenatal or postnatal. Among nine cases in the pre-natal group, four suffered from prenatal malnutrition so were born small for gestational age. Of the four children with multifactorial aetiology one had syn-dactyly and another plagiocephaly. The case of cleidocranial dysplasia was labelled as autosomal dominant as one sibling and mother of the index case were also affected. In the postnatal group psychoso-cial deprivation and neglect was predominant cause of mild ID followed by malnutrition. In our study none of the children with mild ID developed epilepsy or cerebral palsy.
Metabolic screening, conventional chromosomal analysis and Fragile X testing results were normal for all cases.
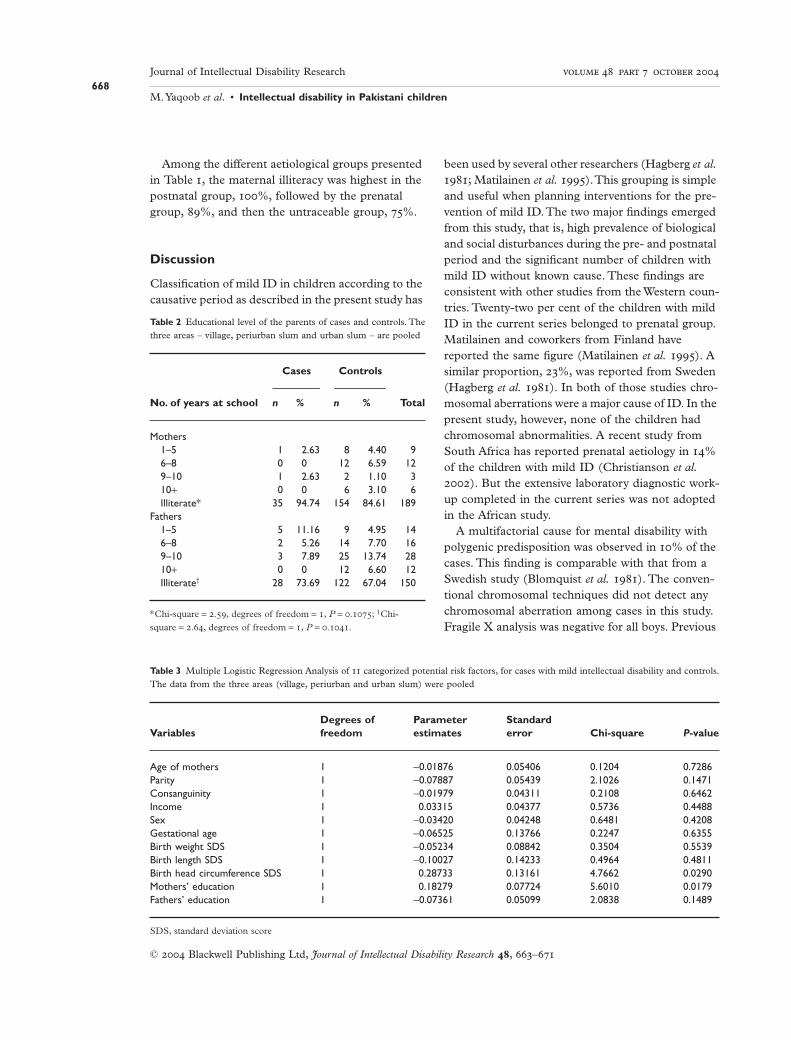
Areawise bivariate analysis of the cases vs. controls did not reveal any significant difference as far as maternal age, parity, consanguinity of the parents, monthly income, sex, gestational age, birth weight, birth length, and birth head circumference are con-cerned. However, lack of education of mother was significantly associated with the development of mild ID in all study areas (P < .). However, this asso-ciation also disappeared when data from three areas were pooled (see Table ).
Stepwise regression analysis did not reveal associ-ation of any independent variable with the develop-ment of mild ID in children in any area of residence except for male gender and father education in the village (P < .), and gestational age and mother education in the urban slum (P < .). However, when the data from the three poor areas were pooled in the regression model, mother’s illiteracy appeared as a risk factor significantly associated with the devel-opment of mild ID (P = .). A significant association (P = .) of mild ID with head circum-ference at birth was also seen (see Table ).
Table 1 Cause of mild intellectual disability in children according to period of onset and gender
Period of onset Diagnosis
Number
Percentageof casesMale Female Total
Prenatal 7 2 9 22%GeneticMendelian 1 0 1*ChromosomalNeurometabolicNeurocutaneousNeurodegenerativeMultifactorial 4 0 4AcquiredPrenatal infections 0Small for gestational age 2 2 4
Perinatal 0Postnatal 5 6 11 28%
Psychosocial deprivation 3 3 6Malnutrition 2 3 5
Untraceable 9 11 20 50%Total 21 19 40
*One child with cleidocranial dysplasia.
Journal of Intellectual Disability Research
M. Yaqoob et al. • Intellectual disability in Pakistani children668
© Blackwell Publishing Ltd, Journal of Intellectual Disability Research , ‒
Among the different aetiological groups presented in Table , the maternal illiteracy was highest in the postnatal group, %, followed by the prenatal group, %, and then the untraceable group, %.
Discussion
Classification of mild ID in children according to the causative period as described in the present study has
been used by several other researchers (Hagberg et al. ; Matilainen et al. ). This grouping is simple and useful when planning interventions for the pre-vention of mild ID. The two major findings emerged from this study, that is, high prevalence of biological and social disturbances during the pre- and postnatal period and the significant number of children with mild ID without known cause. These findings are consistent with other studies from the Western coun-tries. Twenty-two per cent of the children with mild ID in the current series belonged to prenatal group. Matilainen and coworkers from Finland have reported the same figure (Matilainen et al. ). A similar proportion, %, was reported from Sweden (Hagberg et al. ). In both of those studies chro-mosomal aberrations were a major cause of ID. In the present study, however, none of the children had chromosomal abnormalities. A recent study from South Africa has reported prenatal aetiology in % of the children with mild ID (Christianson et al. ). But the extensive laboratory diagnostic work-up completed in the current series was not adopted in the African study.
A multifactorial cause for mental disability with polygenic predisposition was observed in % of the cases. This finding is comparable with that from a Swedish study (Blomquist et al. ). The conven-tional chromosomal techniques did not detect any chromosomal aberration among cases in this study. Fragile X analysis was negative for all boys. Previous
Table 2 Educational level of the parents of cases and controls. Thethree areas – village, periurban slum and urban slum – are pooled
No. of years at school
Cases Controls
Totaln % n %
Mothers1–5 1 2.63 8 4.40 96–8 0 0 12 6.59 129–10 1 2.63 2 1.10 310+ 0 0 6 3.10 6Illiterate* 35 94.74 154 84.61 189
Fathers1–5 5 11.16 9 4.95 146–8 2 5.26 14 7.70 169–10 3 7.89 25 13.74 2810+ 0 0 12 6.60 12Illiterate† 28 73.69 122 67.04 150
*Chi-square = ., degrees of freedom = , P = .; †Chi-square = ., degrees of freedom = , P = ..
Table 3 Multiple Logistic Regression Analysis of categorized potential risk factors, for cases with mild intellectual disability and controls.The data from the three areas (village, periurban and urban slum) were pooled
VariablesDegrees offreedom
Parameterestimates
Standarderror Chi-square P-value
Age of mothers 1 -0.01876 0.05406 0.1204 0.7286Parity 1 -0.07887 0.05439 2.1026 0.1471Consanguinity 1 -0.01979 0.04311 0.2108 0.6462Income 1 0.03315 0.04377 0.5736 0.4488Sex 1 -0.03420 0.04248 0.6481 0.4208Gestational age 1 -0.06525 0.13766 0.2247 0.6355Birth weight SDS 1 -0.05234 0.08842 0.3504 0.5539Birth length SDS 1 -0.10027 0.14233 0.4964 0.4811Birth head circumference SDS 1 0.28733 0.13161 4.7662 0.0290Mothers’ education 1 0.18279 0.07724 5.6010 0.0179Fathers’ education 1 -0.07361 0.05099 2.0838 0.1489
SDS, standard deviation score

Journal of Intellectual Disability Research
M. Yaqoob et al. • Intellectual disability in Pakistani children669
© Blackwell Publishing Ltd, Journal of Intellectual Disability Research , ‒
studies have also detected few children with mild ID having chromosomal aberrations (Hagberg et al. ). Hereditary neurometabolic, neurocutaneous and neurodenegerative disorders are rare causes of mild ID. In one family in the periurban slum two children suffered from mild ID but conventional screening results for metabolic diseases were negative.
Small for gestational age is another important underlying cause of ID in children (Durkin et al. ). The present investigation also shows similar results.
Several researchers have shown that home-based stimulation of children is directly related with the socio-economic status of the family (Buchanan & Oliver ; Upadhyay et al. ; Duncan et al. ). The present investigation also shows similar results, as the psychosocial under stimulation of chil-dren was limited to the underprivileged population groups of periurban slum and the village and fre-quency of mild ID was least prevalent in the UM class. The population in the periurban slum migrated from far villages and small towns and settled in the peripheral areas of the city. Probably because of high prevalence of illiteracy, poverty and ignorance, the childcare practices are undermined. Our report of severe ID showed that frequency of this handicap was also highest in the periurban slum (Yaqoob et al. ). Most likely several social and biological factors are operating in this group, which need further research to provide an important breakthrough in lowering the high frequency of ID among children in this population group.
Thirteen per cent of children in this study devel-oped severe malnutrition under year of age that most probably affected their brain development resulting in ID. Similar observation has been reported by other researchers (Freeman et al. ; Upadhyay et al. ). It is argued that protein energy malnutrition in infancy adversely alters the biochem-istry of the developing brain leading to tissue damage and global ID. Researchers have reported that younger children with severe protein energy malnu-trition prolonging for a longer duration are at higher risk for developing ID (Udani ).
In a significant number of the children in the present series no possible cause of ID could be traced. Probably minor prenatal or perinatal events that are not recorded in our routine evaluation may affect the genetic potential of these children for brain
development. However, this group of children needs further evaluation to explore more demographic and biological factors based upon laboratory technology.
It was an advantage for us that we had all the available information recorded in a standardized manner both for cases and controls. Less number of cases was an important limitation of the study. A large proportion of families with children recruited at birth in the main longitudinal study could not be followed because of high under-five mortality, migration out of study areas, and refusals. But we believe that this high dropout rate would not affect the results of the study as the distribution of biological and social vari-ables was the same for both who declined and those who continued.
Mother illiteracy and head circumference at birth appeared as two significant independent predictors of mild ID in the present study. Most probably because of ignorance and household responsibilities, the uneducated mothers do not give sufficient time to the psychomotor stimulation of their children and are less motivated in learning skills of childcare. Similar findings have been reported by another group of researchers from Bangladesh (Durkin et al. ). The % maternal illiteracy among children who are malnourished or faced psychosocial deprivation is an important finding and highlights the significance of this preventable factor which is directly linked with the intellectual and physical development of a child. The smaller head size at birth among children with mild ID was independent of weight and length at birth. The association of this growth parameter with the development of mild ID has been discussed else-where (Dobbing ).
Parental consanguinity was shown as one of the important risk factors for developing severe ID in children in this population (Yaqoob et al. ). However, the present study did not show any rela-tionship between parental consanguinity and mild ID. This observation supports the previous finding that biological factors are important in causing severe ID and social factors predominate in the origin of mild ID in children (Moser et al. ).
Conclusions
The present study highlights a clear relationship of mild ID with prenatal and postnatal malnutrition and

Journal of Intellectual Disability Research
M. Yaqoob et al. • Intellectual disability in Pakistani children670
© Blackwell Publishing Ltd, Journal of Intellectual Disability Research , ‒
social deprivation. Two significant independent vari-ables, maternal illiteracy and small head circumfer-ence at birth, showed a significant association with the development of mild ID.
Acknowledgements
This study was supported by grants from Swedish Agency for Research Cooperation with the Develop-ing Countries (SAREC), Maud and Birger Gustavs-son Foundation, Swedish Medical Research Council and Medical Faculty, University of Uppsala, Upp-sala, Sweden, and King Edward Medical College, Lahore, Pakistan. The authors appreciate the help of Professor Khalida Tareen, Professor Emeritus at the Department of Child and Family Psychiatry, King Edward Medical College, Lahore, Pakistan.
References
Al-Ansari A. () Aetiology of mild mental retardation among Bahraini children: a community-based case con-trol study. Mental Retardation , –.
Alm J. & Larsson A. () Evaluation of a nation-wide neonatal metabolic screening programme in Sweden. Acta Paediatrica Scandinavica , –.
Bashir A., Yaqoob M., Ferngren H., Gustavson K.-H., Rydelius P.-A., Ansari T. & Zaman S. () Prevalence and associated impairments of mild mental retardation in six- to ten-year old children in Pakistan: a prospective study. Acta Paediatrica , –.
Bax M. C. O. () Terminology and classification of cerebral palsy. Developmental Medicine and Child Neurol-ogy , –.
Blomquist H. K., Gustavson K.-H. & Holmgren G. () Mild mental retardation in children in a Northern Swed-ish county. Journal of Mental Deficiency Research , –.
Buchanan A. & Oliver J. E. () Abuse and neglect as a cause of mental retardation. Child Abuse and Neglect , –.
Christianson A. L., Zwane M. E., Manga P., Rosen E., Venter A., Downs D. & Kromberg J. G. R. () Chil-dren with intellectual disability in rural South Africa: prevalence and associated disability. Journal of Intellectual Disability Research , –.
Crocker A. C. () The causes of mental retardation. Paediatric Annals , –.
Dobbing J. () Pathology and Vulnerability of the Develop-ing Brain. Scientific Studies in Mental Retardation. The
Royal Society of Medicine and the Macmillan Press Ltd, London, pp. –.
Dubowitz L. M. S., Dubowitz V. & Goldberg C. () Clinical assessment of gestational age in the newborn infant. Journal of Pediatrics , –.
Duncan G. J., Brooks-Gunn J. & Klebanov P. K. () Economic deprivation and early childhood development. Child Development , –.
Durkin M. S., Khan N. Z., Davidson L. L., Huq S., Munir S., Rasul E. & Zaman S. () Prenatal and postnatal risk factors for mental retardation among children in Bangladesh. American Journal of Epidemiology , –.
Fernell E. () Mild mental retardation in schoolchildren in a Swedish suburban municipality: prevalence and diag-nostic aspects. Acta Paediatrica , –.
Freeman H. E., Klein R. E., Townsend J. W. & Lechtig A. () Nutrition and cognitive development among rural Guatemalan children. American Journal of Public Health , –.
Hagberg B., Hagberg G., Leverth A. & Lindberg U. () Mild mental retardation in Swedish school children. II. Etiology and pathogenetic aspects. Acta Paediatrica Scan-dinavica , –.
Jalil F., Lindblad B. S., Hanson L. A., Khan S. R., Ashraf R. N., Carlsson B., Zaman S. & Karlberg J. () Early child health in Lahore, Pakistan. I. Study design. Acta Pediatrica (Suppl.), –.
Malik M. S., Masheer M. & Zafar M. H. () Mental retardation in children. Journal of Pakistan Medical Asso-ciation , –.
Matilainen R., Airaksinen E., Mononen T., Launiala K. & Kaarianen R. () A population-based study on the causes of mild and severe mental retardation. Acta Paedi-atrica , –.
Moser H. W., Ramey C. T. & Leonard C. O. () Mental retardation. In: Principles and Practice of Medical Genetics, Vol. . (eds A. E. H. Emery & D. L. Rimoin), pp. –. Churchill Livingstone, Edinburgh.
Schlesselman J. J. () Case-Control Studies: Design, Conduct, Analysis. Oxford University Press, New York/Oxford.
Stein Z., Belmont L. & Durkin M. () Mild mental retardation and severe mental retardation compared: experiences in eight less developed countries. Upsala Jour-nal of Medical Sciences (Suppl.), –.
Stromme P. & Hagberg G. () Aetiology in severe and mild mental retardation: a population-based study of Norwegian children. Developmental Medicine and Child Neurology , –.
Therell B. L. (ed.) () Laboratory Methods for Neonatal Screening. American Public Health Association, Washing-ton DC.
Torresani T. E. & Scherz T. () Neonatal thyroid screening by a non-radioactive method: evaluation of thy-

Journal of Intellectual Disability Research
M. Yaqoob et al. • Intellectual disability in Pakistani children671
© Blackwell Publishing Ltd, Journal of Intellectual Disability Research , ‒
rotropin time-resolved fluoroimmunoassay. Clinical Chemistry , –.
Udani P. M. () Protein energy malnutrition (PEM), brain and various facets of child development. Indian Journal of Pediatrics , –.
Upadhyay S. K., Agarwal K. N. & Agarwal D. K. () Influence of malnutrition on social maturity, visual motor coordination & memory in rural school children. Indian Journal of Medical Research , –.
Upadhyay S. K., Saran A., Agarwal D. K., Singh M. P. & Agarwal K. N. () Growth and behavior development in rural infants in relation to malnutrition and environ-ment. Indian Paediatrics , –.
von Wendt L. & Rantakallio P. () Mild mental retarda-tion in Northern Finland. Upsala Journal of Medical Sci-ences , –.
WHO Working Group () Use and interpretation of anthropometric indicators of nutritional status. Bulletin of the World Health Organization , –.
Yaqoob M., Bashir A., Tareen K., Gustavson K.-H., Nazir R., Jalil F., von Dobeln U. & Ferngren H. () Severe mental retardation in to -month-old children in Lahore, Pakistan: a prospective cohort study. Acta Pedi-atrica , –.
Accepted August





























