Embed Size (px)
Citation preview

American Journal of Medical Genetics 47:788-792 (1993)
Mesomelic Limb Shortness: A Previously Unreported Autosomal Recessive Type
W. Reardon, C.M. Hall, S. Slaney, S.M. Huson, J. Connell, N. Al-Hilaly, J. Fixsen, M. Baraitser, and R.M. Winter Departments of Paediatric Genetics (W.R., M.B., R.M.W.), Radiology (C.M.H.), and Orthopaedics (J.F.), Hospitals for Sick Children, London; Department of Medical Genetics, Churchill Hospital, Oxford (S.S., S.M.H.); and Department of Paediatrics, Wexham Park Hospital, Slough (J.C., N.A.-H.), United Kingdom
We report on sibs, the offspring of a consan- guineous mating, whose mesomelic shortness and bowing of limbs with associated skin dim- pling, retrognathia, mandibular hypoplasia, cleft palate, and camptodactyly represents a previously apparently unreported syndrome. The radiological findings are discussed, par- ticularly with regard to the main known diag- nostic possibilities.
KEY WORDS: mesomelia, cleft palate, micro-
o 1993 Wiley-Lisa, Inc.
gnathia, camptodactyly
INTRODUCTION Mesomelic limb shortness occurs in several conditions
[Winter and Baraitser, 19931. Here we present a brother and sister whose manifestations of mesomelic bowed and short limbs, retrognathia, cleft palate, and camptodac- tyly initially led to diagnosis of campomelic dysplasia. However, the radiological findings were incompatible with that diagnosis and other causes of mesomelic limb shortness and bowing had to be considered. The main alternative diagnostic possibilities of Nievergelt syn- drome, Reinhardt-Pfeiffer syndrome, Langer syndrome, and hypophosphatasia were excluded. Based on the clin- ical and radiological profile as well as the clear evidence of autosomal recessive transmission in this pedigree, we suggest that these patients represent a newly recog- nized form of mesomelic limb shortness and bowing.
CLINICAL REPORTS Patient 1
The first child of second-cousin Pakistani parents, this boy was born at term after an uncomplicated pregnancy. Initial head circumference ( O F 0 was 34.5 cm (75th
Received for publication May 4, 1993; revision received May 18, 1993.
Address reprint requests to Dr. W. Reardon, Mothercare Dept of Genetics and Fetal Medicine, Institute of Child Health, 30 Guilford St., London WClN IEH, United Kingdom.
0 1993 Wiley-Liss, Inc.
centile), birth weight was 3.17 kg ( 4 0 t h centile), and length was 45.5 cm (<3rd centile) [Hall et al., 19891. At birth short, angulated limbs with dimpling of the over- lying skin were noted, as well as a cleft palate. The latter was repaired a t 6 months. Psychomotor development was normal; he smiled at 6 weeks and sat at 7 months. At age 4 years, mobility is limited by the limb malforma- tions but he walks, weight bearing on his toes.
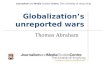
On examination there is marked mesomelic shortness and bowing with dimpling of the overlying skin of the legs and forearms (Fig. 1). He has retrognathia, with evidence of cleft palate repair. The ears are normal. There is bilateral camptodactyly involving the 3rd, 4th, and 5th fingers with full range of movements of the thumb and index finger. Elbow extension is limited to
Fig. 1. The propositus demonstrating bowed, mesomelic limbs with skin dimpling over forearms and shins.

AR Mesomelic Dysostosis 789
the distal radial metaphyses. The radii and ulnae are short with striking bowing of the proximal ulna and a bony spur a t the apex, with overlying skin dimpling (Fig. 4). The radial head is dislocated and the distal radial epiphysis flat. There is shortness of the first metacarpal. Lateral clavicular “hooks,” which are fre- quently associated with congenital elbowlforearm ab- normalities, are seen on the chest roentgenogram. The lower limbs show flat, irregularly ossified capital femoral epiphyses, with broad femoral necks, flared irregular metaphyses, and possible acetabular “dysplasia” (Fig. 5). The tibiae and fibulae are short, with anterior bow- ing and skin dimpling at the apices over the midshaft of the tibiae and fibulae (Fig. 6). The talus is abnormally shaped and muscle bulk is reduced.
Plasma calcium and alkaline phosphatase levels were normal. Results of renal ultrasound were normal with no evidence of nephrocalcinosis.
120” and flexion to 45”. Radiological examination shows flatness of the frontal bone with some midface hypo- plasia (Fig. 2) and significant shortness of the mandible. There is mild generalized platyspondyly with slight ir- regularity of vertebral endplates in the upper lumbar region, prominent anteroinferior parts of lumbar ver- tebral bodies, and mild posterior scalloping (Fig. 3). In the upper limbs there is flare of the distal humeral and
Fig. 2. Skull radiograph of patient 1 demonstrating frontal flatness and midface hypoplasia.
Fig. 4. Shortness of the radius and ulna, patient 1, with proximal ulnar bowing and bony spur at the apex.
Fig. 5. Pelvis ofpatient 1 with broad femoral necks, flared irregular metaphyses and flattened, irregularly ossified capital femoral epi- physes.
Fig. 3. Lumbar vertebrae, patient 1, showing anteroinferior promi- nence of the vertebral bodies and mild posterior scalloping.

790 Reardon et al.
Fig. 8. “Crumpled, dysplastic” ear, patient 2. Fig. 6. Patient 1, shortness and anterior bowing of the tibia and
fibula.
Patient 2 The sister of patient 1 was born at 39 weeks of gesta-
tion, weighing 4.4 kg. Ultrasound investigation at 19 weeks had shown shortness of the limbs. Resuscitation was initially successful at the time of delivery but was followed within a few hours by cardiorespiratory arrest. Clinical examination showed an OFC of 38 cm (>97th centile), crown rump length of 37 cm (>97th centile), and crown heel length of 48 cm (50th centile). The palate was cleft (Fig. 71, the ears overfolded, “crumpled” and apparently low-set (Fig. 8). The face was unremarkable apart from thin lips and retrognathia (Fig. 9). The limbs were clearly short with camptodactyly of the hands and limited extension at the elbows (Fig. 10). There was bony angulation of both upper and lower limbs, associ- ated with dimpling of the overlying skin.
Fig. 9. Patient 2 ernphasising retrognathia and thin lips with ab- sence of other minor anomalies.
Fig. 7. Cleft palate, patient 2.
Autopsy showed small, hypoplastic lungs with only two lobes present on the right. The examination was otherwise unremarkable. Death was attributed to the gross lung hypoplasia with pneumothorax.
Radiological investigation showed a normal spine and pelvis except for acetabular “dysplasia.” The long bones of the lower limb were short and angulated with promi- nent spurs at the site of maximum angulation. In the tibiae and fibulae this site was at the junction of the upper two thirds and the lower third (Fig. 11). The knee epiphyses were present, which is appropriate for gesta- tional age, and the metaphyses were smooth. Films of the upper limb and skull were not available.

AR Mesomelic Dysostosis 791
melic dysplasia. However, most patients with this auto- soma1 recessive disorder are stillborn or succumb early [Houston et al., 19831, many having a congenital heart defect. Those few who do survive are generally deaf and mentally retarded, unlike the survivor in this report. Moreover, the radiological changes in our patients are unlike the characteristic skeletal changes of cam- pomelic dysplasia. In particular, the scapulae in cam- pomelic dysplasia are characteristically hypoplastic as opposed to the normal scapulae in both these patients. The skull in this latter syndrome is often dolichocepha- lic, whereas patient 1 of this report had flat frontal bones. Finally, the characteristic pelvic changes of nar- row iliac wings with shallow acetabula and vertical, widely spaced ischia seen in campomelic dysplasia are absent in our patients [Hall and Spranger, 19791. Al- though variants of campomelic dysplasia are described [McPherson et al., 1989; Friedrich et al., 19921, the car- dinal radiological changes in the scapulae and pelvis are consistently observed, in contrast to our patients.
The long bone radiological changes of our patients are more reminiscent of the Reinhardt-Pfeiffer type of meso- melic limb shortness, although more severe than is usually seen in that condition. However, patients with Reinhardt-Pfeiffer type mesomelic dysplasia character- istically have straight ulnae, upper limb bowing, and straight tibiae in distinct contrast to the radiological characteristics we describe [Taybi and Lachman, 19901. Moreover, mandibular hypoplasia is not a component of Reinhardt-Pfeiffer syndrome and, furthermore, the lat- ter is an autosomal dominant disorder.
Mandibular hypoplasia occurs in Nievergelt meso- melic dysplasia as does camptodactyly. The long bone changes in this condition are typified by the triangular configuration of the tibiae, which are markedly short, with less severe shortness of the fibulae. The ulnae may also be short and the elbow joint restricted due to radio- ulnar synostosis and radial head dislocation. However, this mesomelic condition is transmitted as an autosomal dominant condition, unlike the situation we describe.
Although Langer type mesomelic dysplasia is an au- tosomal recessive trait and is characterized by mandib- ular hypoplasia, the limbs are shorter and less bowed than we describe. In contrast to our cases, the distal ulnae are frequently hypoplastic with absence of ossi- fied distal ulnar epiphysis and there is no camptodac- tyly [Spranger et al., 19741. Additionally, the parents of our patients do not show clinical evidence of dyschon- drosteosis which has been regarded as one of the clinical manifestations of heterozygosity for Langer type dys- plasia.
In conclusion, the sibs we describe appear to represent a newly observed form of autosomal recessive mesomelic limb shortness and bowing with mandibular hypo- plasia, retrognathia, cleft palate, and camptodactyly.
REFERENCES Friedrich U, Schaefer E, Meinecke P (1992): Campomelic dysplasia
without overt campomelic. Clin Dysmorphol 1:172-178. Hall JG, Froster-Iskenius UG, Allanson JE (1989): “Handbook of Nor-
mal Physical Measurements.” Oxford: Oxford Medical Publications. Hall BD, Spranger JW (1979): Familial congenital bowing with short
bones. Radiology 132:611-614.
Fig. 10. Limitation of elbow extension, patient 2.
Fig. 11. Long bone angulation of the lower limbs, patient 2.
DISCUSSION The evidence for autosomal recessive transmission is
strong in this brother and sister sib pair, offspring of clinically normal consanguineous parents. Their condi- tion comprises mesomelic limb shortness and bowing with skin dimpling, cleft palate, retrognathia, camp- todactyly, and limitation of elbow joint movement. The predominant radiological abnormalities relate to the mesomelic malformations. The normal biochemical and renal investigations exclude hypophosphatasia as a likely cause and the radiological and clinical findings are such as to limit diagnostic considerations to a few possibilities.
Foremost among these, based on the presence of bowed, short limbs, skin dimples, and cleft palate, is campo-

792 Reardon et al.
Houston CS, Opitz JM, Spranger JW, Macpherson RI, Reed MH, Gilb- ert EF, Herrmann J, Schinzel A: The campomelic syndrome: Re- view, report of 17 patients and follow-UP on the currently 17-Year- old boy first reported by Maroteaux et a1 in 1971. AmJ Med Genet 15:3-28. Publishers, Inc. 3rd ED.
McPherson RI, Skinner SA, Donnelfeld AE (1989): AcamPomelic cam- pomelic dysplasia. Pediatr Radio1 20:90-93.
Spranger JW, Langer LO Jr, Wiedemann H-R (1974): “Bone dysplasias:
An Atlas of Constitutional Disorders of Skeletal Development.” Philadelphia: WB Saunders.
Taybi H, Lachman RS (1990): “Radiology of Syndromes, Metabolic Disorders and Skeletal Dysplasias.” Chicago: Year Book Medical
Winter RM, Baraitser M (1993): ‘‘The London Dysmorphology Data- base.” Oxford Oxford University Press.




![Autosomal recessive ichthyosis with limb reduction defect ... · including autosomal dominant, autosomal recessive and X-linked inheritance [1,2]. Associated cutaneous and extracutaneous](https://img.pdfslide.us/doc/110x75/5ec8c9b91adfdf12ab3e663c/autosomal-recessive-ichthyosis-with-limb-reduction-defect-including-autosomal.jpg)