Embed Size (px)
Citation preview
Mental health in acute care‘If you don’t ask, you won’t know’
Dr Immo Weichert, Arun Kirupakaran, Sereena Ansari,
Vinci Naruka, Thushyanthan Guruparan
University of
CambridgeThe Ipswich Hospital
Brantham Ward
Emergency Assessment Unit

Why mental health?2010
• Mental health is the primary driver of disability worldwide
• 40 million years of disability in 20-29 year olds
2012
• Adult Psychiatric Morbidity Survey - adults living in private housing in
England
• 1 in 4 admitted to experiencing a mental health problem in the last 12
months
2016
• Study in England estimates that 1 in 6 people in the past week
experienced a mental health problem
In summary
• Mental health is COMMON
• Mental health is IMPORTANT
• Mental health is BEING MISSED
Background Mental health in acute care
‘If you don’t ask, you won’t know’
Why mental health?
Patients with long term conditions have a 2-3 times increased risk of
developing mental health issues (cardiovascular disease, diabetes, COPD)
Epilepsy:
• Depression extremely common, life-time prevalence of 30-35%
• Direct link with the underlying pathology, not indirect/reactive
Musculoskeletal:
• 33% of women, 20% of men with all types of arthritis have depression
Costs:
• 12-18% of all NHS expenditure on long-term conditions directly linked
to poor mental health: 8-13 billion £ in England per year
• Liaison psychiatry has shown that better psychiatric support can
reduce costs for acute care
Background Mental health in acute care
‘If you don’t ask, you won’t know’

Why mental health? Ipswich Perspective
Since 2016
'Under the current SLA, Psychiatric Liaison Service will provide
a service to ED and the Assessment Areas only.
There is no current provision to support in-patients in IHT
requiring Mental Health input.'
Background Mental health in acute care
‘If you don’t ask, you won’t know’
Why mental health? Ipswich Perspective
Solutions
• Identify patients with psychiatric needs at the entrance to
the system and if necessary flag up to primary care or refer
whilst still in acute medicine where there is still a
psychiatric liason service available
• This is a pilot project introducing a recognised screening
tool in Acute Medicine
Background Mental health in acute care
‘If you don’t ask, you won’t know’
Aims
• To offer mental health screening to all acute admissions (pilot
run)
• To identify the prevalence of mental health problems in acute
care.
• To identify the prevalence of patients requesting help for their
mental health problems in acute care.
• To identify the demographics and co-morbidities of these
patients.
Aims Mental health in acute care
‘If you don’t ask, you won’t know’
Methods Mental health in acute care
‘If you don’t ask, you won’t know’
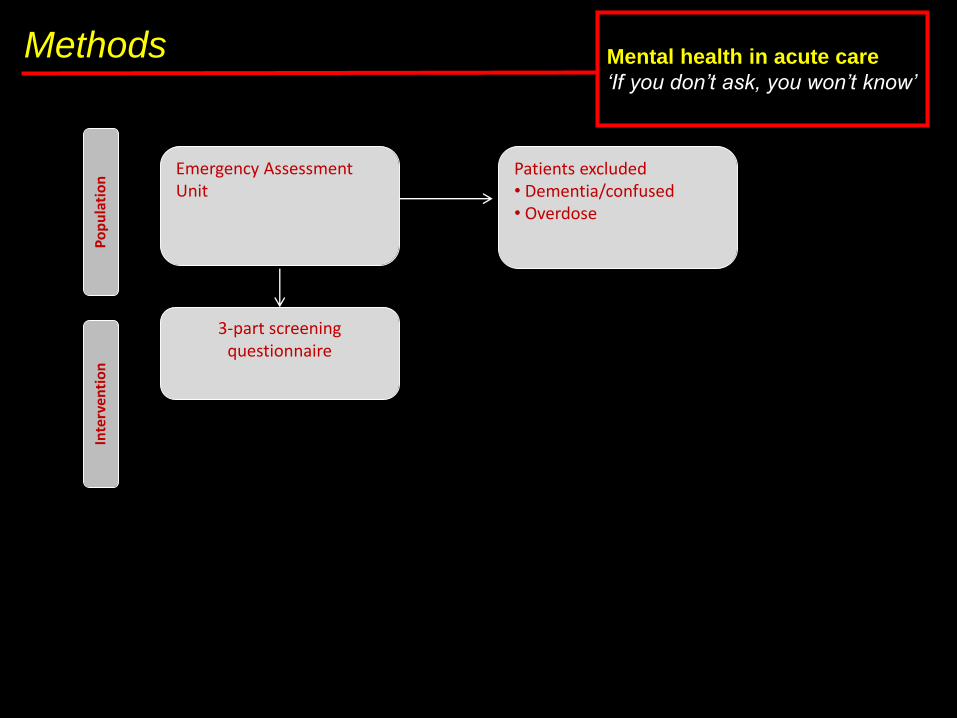
Emergency Assessment Unit
Patients excluded• Dementia/confused• Overdose
3-part screening questionnaire
Interven
tion
Population
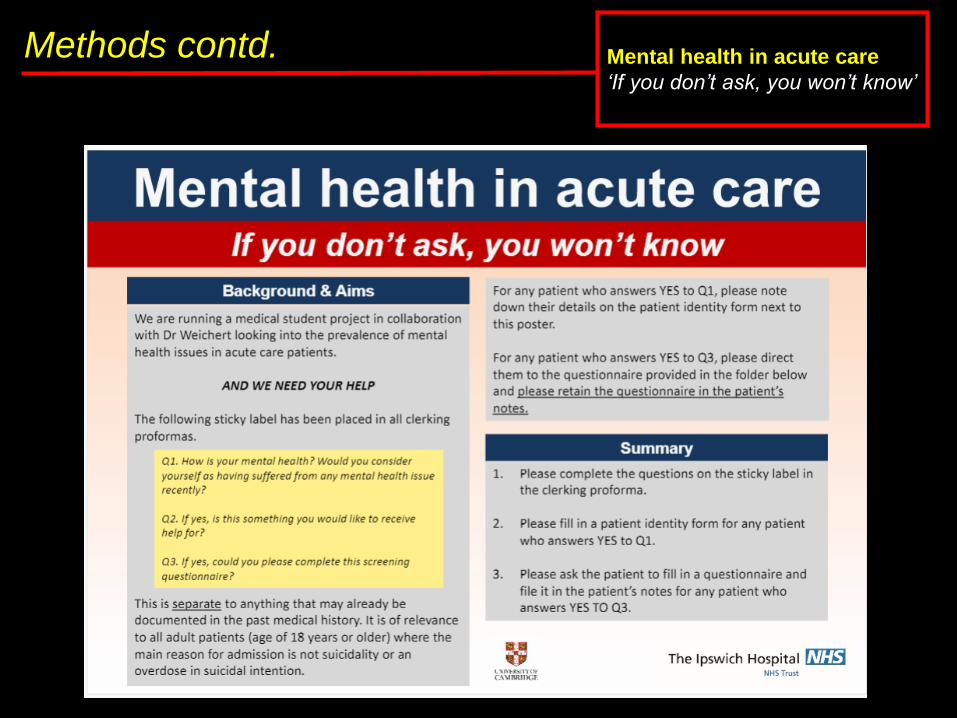
Methods contd. Mental health in acute care
‘If you don’t ask, you won’t know’
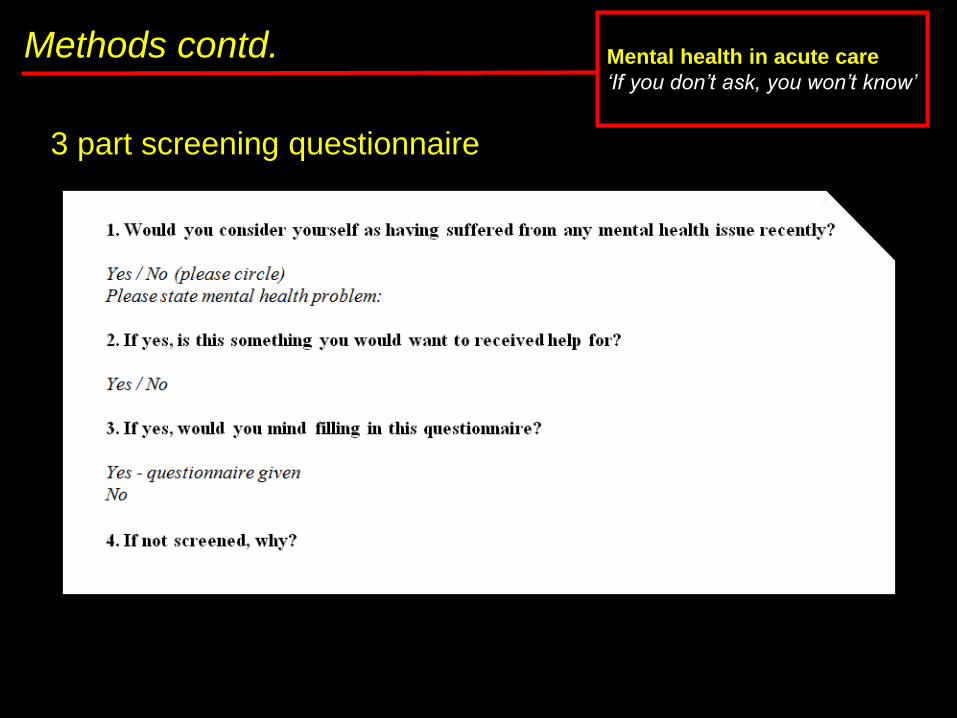
3 part screening questionnaire
Methods Mental health in acute care
‘If you don’t ask, you won’t know’
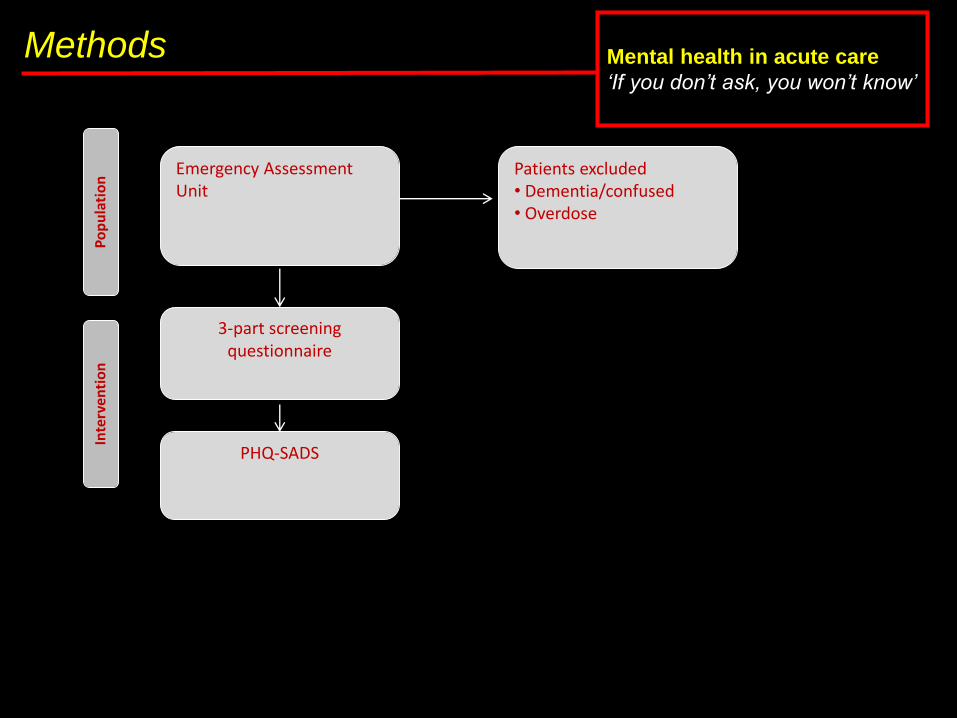
Emergency Assessment Unit
Patients excluded• Dementia/confused• Overdose
3-part screening questionnaire
PHQ-SADS
Interven
tion
Population

Methods contd. Mental health in acute care
‘If you don’t ask, you won’t know’
PHQ-SADS
• A screening tool for mental health disorders
• Well validated and widely accepted
• In public domain (no costs)
• 3 main aspects:
1. Somatisation (PHQ-15)
2. Anxiety (GAD-7)
3. Depression (PHQ-9)
Developed by Drs. Robert L. Spitzer, Janet B.W. Williams, Kurt Kroenke and colleagues, with an educational grant from
Pfizer Inc.
Methods contd. Mental health in acute care
‘If you don’t ask, you won’t know’

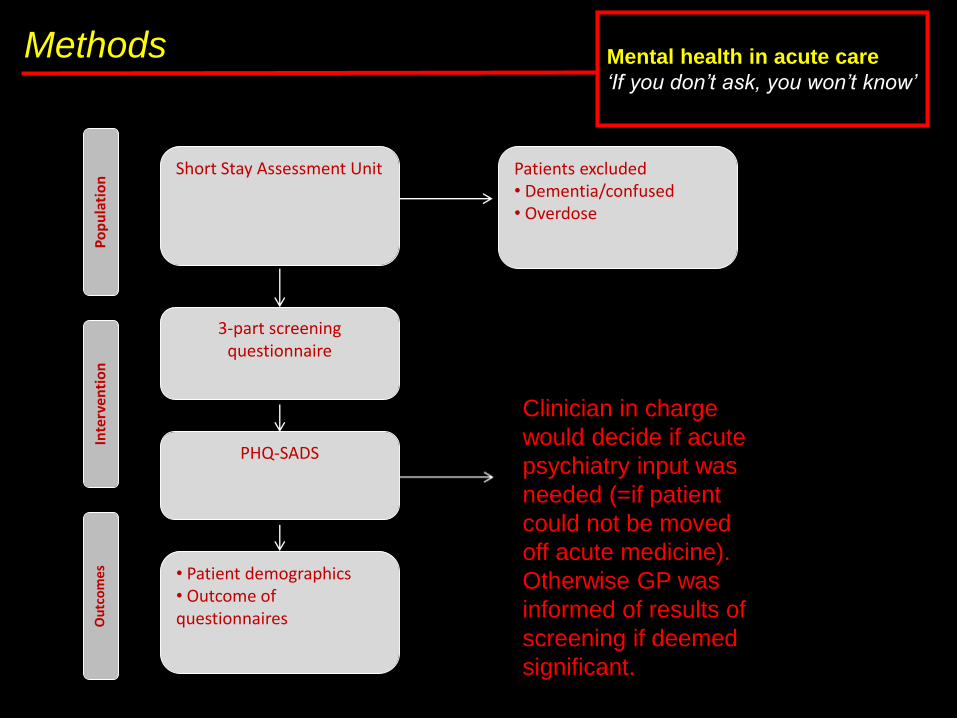
Methods Mental health in acute care
‘If you don’t ask, you won’t know’
Short Stay Assessment Unit Patients excluded• Dementia/confused• Overdose
3-part screening questionnaire
• Patient demographics• Outcome of questionnaires
PHQ-SADS
Interven
tion
Outcomes
Population
Methods Mental health in acute care
‘If you don’t ask, you won’t know’
Short Stay Assessment Unit Patients excluded• Dementia/confused• Overdose
3-part screening questionnaire
• Patient demographics• Outcome of questionnaires
PHQ-SADS
Interven
tion
Outcomes
Population
Clinician in charge
would decide if acute
psychiatry input was
needed (=if patient
could not be moved
off acute medicine).
Otherwise GP was
informed of results of
screening if deemed
significant.

Results Mental health in acute care
‘If you don’t ask, you won’t know’
• Total number of patients asked - 129
• Patients who self-reported mental health issues – 49/129
(38%)
• Patients who completed PHQ-SADS completed - 48
• Completion rate – 98%
• Mean age – 60 years
• Male – 32%
• Female - 68%
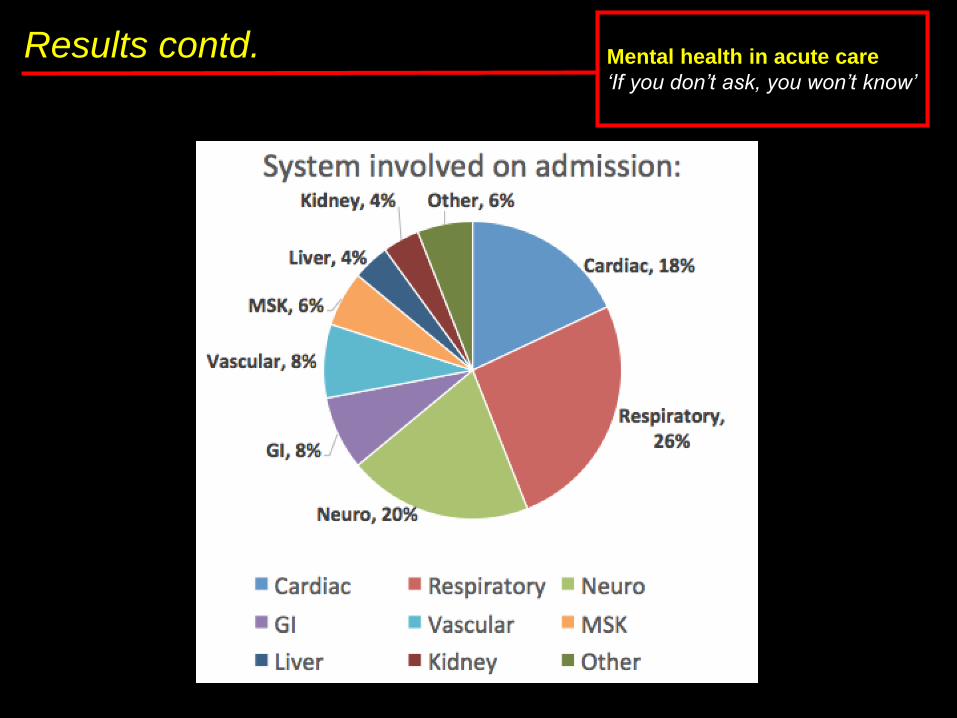
Results contd. Mental health in acute care
‘If you don’t ask, you won’t know’

Results contd. Mental health in acute care
‘If you don’t ask, you won’t know’
Of patients self reporting:
• Median number of admissions in last year: 1 (IQR 2)
• Current admission is a 30 day readmission: 13 (26.5%)
• Prior psychiatric illness documented – 36%
• On psychiatric medications – 40%
• Median Charlson age-co-morbiditiy score: 3 (IQR: 3.75)
• Median clinical frailty index score: 3 (IQR: 2)
• Mean length of stay: 3.3 days (SD: 3)
• 6% of patients seen by psychiatry during admission

Results contd. Mental health in acute care
‘If you don’t ask, you won’t know’
Median scores for PHQ-SADS components:
• PHQ-15 (somatisation): 12 (IQR 8.5)
• GAD-7 (anxiety): 13 (IQR 14)
• PHQ-9 (depression): 15 (IQR 16)
Interpretation of scores:
• 5 - 9: Mild
• 10 - 14: Moderate
• 15 or more: severe

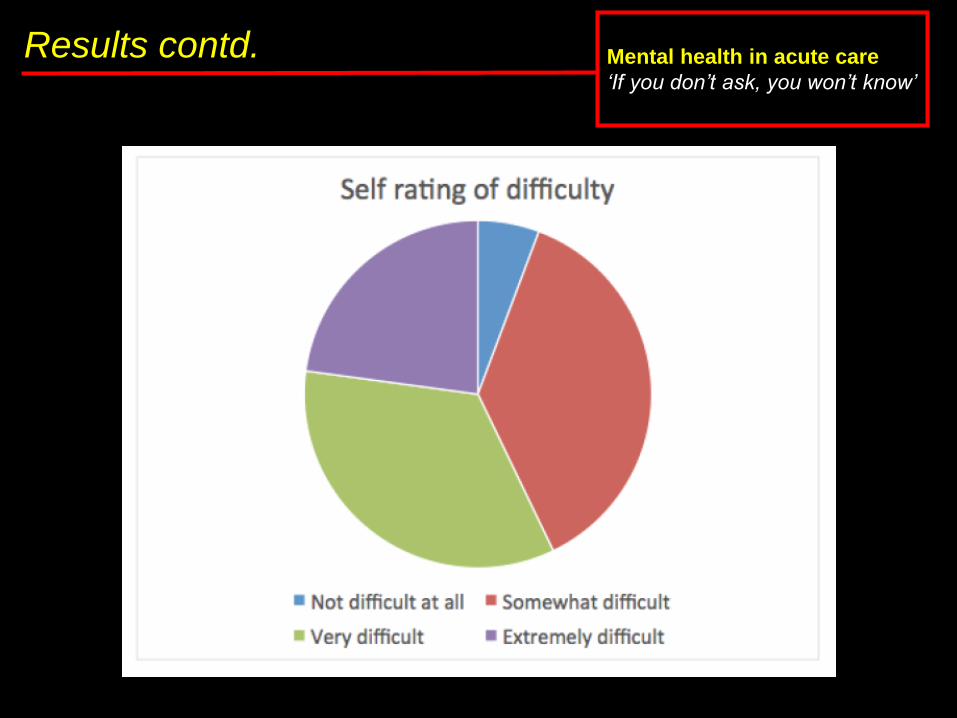
Results contd. Mental health in acute care
‘If you don’t ask, you won’t know’
Results contd. Mental health in acute care
‘If you don’t ask, you won’t know’
2 main issues
• Not all doctors may have been aware of the stickers
• Changes in shifts
• Not all patients were asked by doctors:
• Time constraints in Acute Medicine
• No clear guide for doctors to offer patients help
• Uncomfortable asking about mental health
problems when patients have come in with other
problems.
Limitations Mental health in acute care
‘If you don’t ask, you won’t know’
Conclusion Mental health in acute care
‘If you don’t ask, you won’t know’
• Screening has a high response rate amongst patients in acute
care.
• PHQ-SADS can help identify psychiatric co-morbidities in
patients presenting in acute care.
• Barriers amongst staff must be addressed to successfully
integrate this with medical history taking.
• Patients don’t seem to have any problems self reporting
mental health issues.

Where we go from here...... Mental health in acute care
‘If you don’t ask, you won’t know’
• After the successful pilot run this is now integrated into the
clerking proforma (as direct questions).
• Inform junior doctors and involve the multidisciplinary team,
raising awareness about this new screening tool.
• Change attitudes towards mental health in acute care.

Thank you.
“The future is today”
- William Osler
Thank you Mental health in acute care
‘If you don’t ask, you won’t know’


![Increasing Sucrose Uptake Capacity of Wheat Grains Sucrose Uptake Capacity of Wheat Grains Stimulates Storage Protein Synthesis1[W] Nicola Weichert, Isolde Saalbach, Heiko Weichert,](https://img.pdfslide.us/doc/110x75/5b002dc87f8b9af1148c4dcc/increasing-sucrose-uptake-capacity-of-wheat-sucrose-uptake-capacity-of-wheat-grains.jpg)