Embed Size (px)
Citation preview
Chest Imaging Guidelines
Medical Guidelines Institute CHEST IMAGING GUIDELINES
Effective 06-06-2016
Medical Guidelines Institute Clinical Decision Support Tool for Advanced Diagnostic Imaging
Common symptoms and symptom complexes are addressed by this tool. Imaging requests for patients with atypical
symptoms or clinical presentations that are not specifically addressed will require physician review. Consultation with the referring physician may provide additional insight.
Authors: Bernard D. Borosky, M.D.(Diagnostic Radiology)*
A. Gray Bullard, M.D. (Pulmonology/Sleep Medicine) Emily Coe, Ph.D. (Clinical Trial Design and Analysis)
Timothy Dollear, MS (Epidemiology/Biostatistics) James N. Johnson, M.D. (Family Medicine/Sports Medicine)
Thomas H. Magee, M.D. (Musculoskeletal and General Diagnostic Radiology) Lynne Voutsinas, M.D. (Neuroradiology and General Diagnostic Radiology)
Rena Quandt Whitford, BS (Mathematics/Economics) *Clinical Topic Section Leader
CPT® (Current Procedural Terminology) is a registered trademark of the American Medical Association (AMA). CPT® five digit codes, nomenclature and other data are copyright 2015 American Medical Association. All Rights Reserved. No fee schedules, basic units, relative values or related listings are included in the CPT® book. AMA does not directly or indirectly practice medicine or dispense medical services. AMA assumes no liability for the data contained herein or not contained herein.
Effective 06-06-2016 Chest 3 of 54
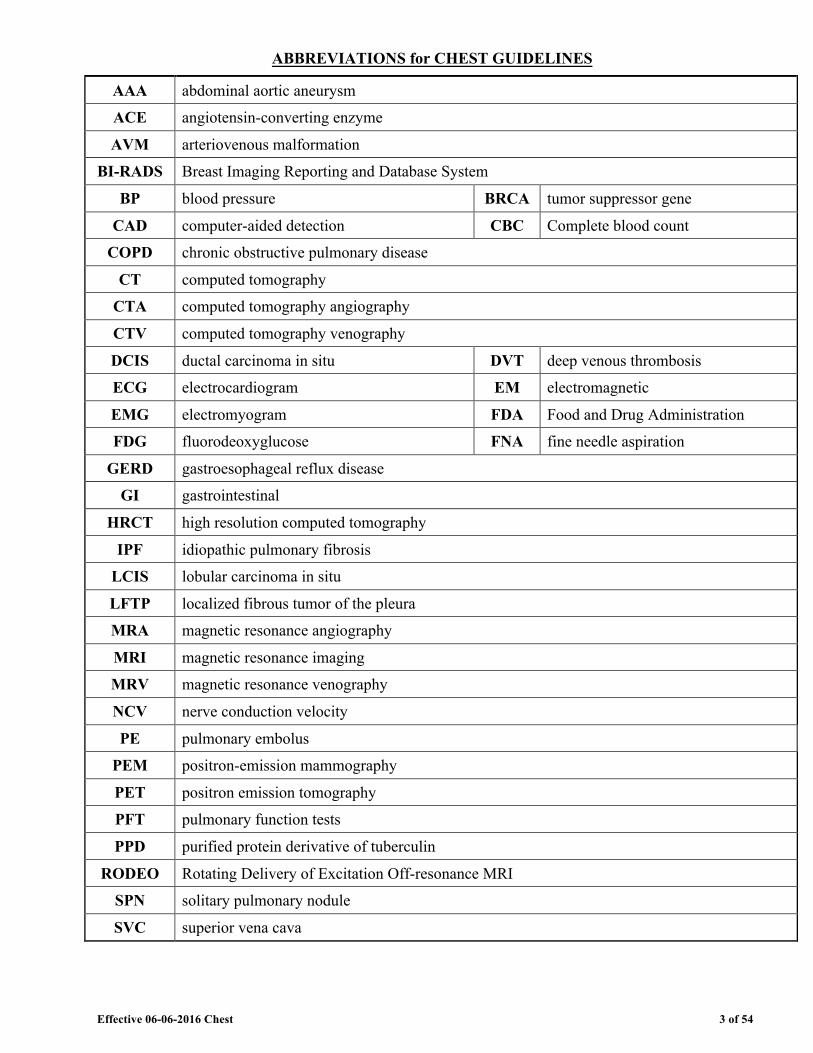
ABBREVIATIONS for CHEST GUIDELINES
AAA abdominal aortic aneurysm
ACE angiotensin-converting enzyme
AVM arteriovenous malformation
BI-RADS Breast Imaging Reporting and Database System
BP blood pressure BRCA tumor suppressor gene
CAD computer-aided detection CBC Complete blood count
COPD chronic obstructive pulmonary disease
CT computed tomography
CTA computed tomography angiography
CTV computed tomography venography
DCIS ductal carcinoma in situ DVT deep venous thrombosis
ECG electrocardiogram EM electromagnetic
EMG electromyogram FDA Food and Drug Administration
FDG fluorodeoxyglucose FNA fine needle aspiration
GERD gastroesophageal reflux disease
GI gastrointestinal
HRCT high resolution computed tomography
IPF idiopathic pulmonary fibrosis
LCIS lobular carcinoma in situ
LFTP localized fibrous tumor of the pleura
MRA magnetic resonance angiography
MRI magnetic resonance imaging
MRV magnetic resonance venography
NCV nerve conduction velocity
PE pulmonary embolus
PEM positron-emission mammography
PET positron emission tomography
PFT pulmonary function tests
PPD purified protein derivative of tuberculin
RODEO Rotating Delivery of Excitation Off-resonance MRI
SPN solitary pulmonary nodule
SVC superior vena cava
Effective 06-06-2016 Chest 4 of 54
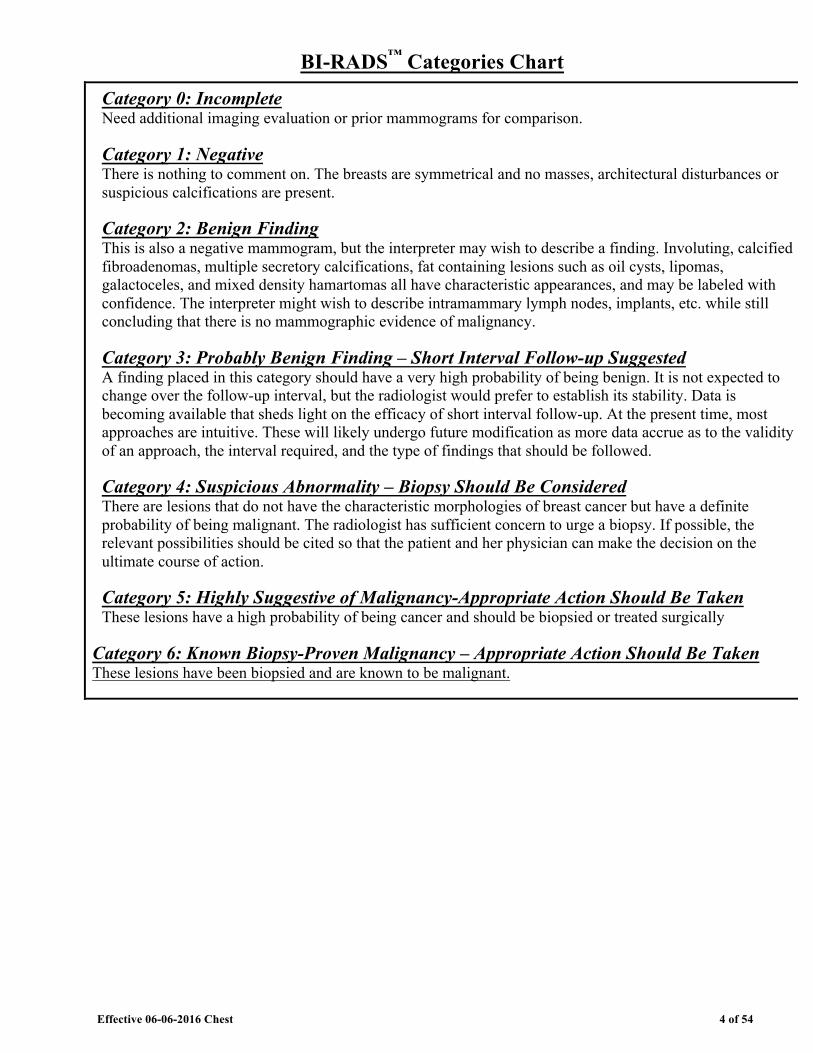
BI-RADS™ Categories Chart
Category 0: Incomplete Need additional imaging evaluation or prior mammograms for comparison.
Category 1: Negative There is nothing to comment on. The breasts are symmetrical and no masses, architectural disturbances or suspicious calcifications are present.
Category 2: Benign Finding This is also a negative mammogram, but the interpreter may wish to describe a finding. Involuting, calcified fibroadenomas, multiple secretory calcifications, fat containing lesions such as oil cysts, lipomas, galactoceles, and mixed density hamartomas all have characteristic appearances, and may be labeled with confidence. The interpreter might wish to describe intramammary lymph nodes, implants, etc. while still concluding that there is no mammographic evidence of malignancy.
Category 3: Probably Benign Finding – Short Interval Follow-up Suggested A finding placed in this category should have a very high probability of being benign. It is not expected to change over the follow-up interval, but the radiologist would prefer to establish its stability. Data is becoming available that sheds light on the efficacy of short interval follow-up. At the present time, most approaches are intuitive. These will likely undergo future modification as more data accrue as to the validity of an approach, the interval required, and the type of findings that should be followed.
Category 4: Suspicious Abnormality – Biopsy Should Be Considered There are lesions that do not have the characteristic morphologies of breast cancer but have a definite probability of being malignant. The radiologist has sufficient concern to urge a biopsy. If possible, the relevant possibilities should be cited so that the patient and her physician can make the decision on the ultimate course of action.
Category 5: Highly Suggestive of Malignancy-Appropriate Action Should Be Taken These lesions have a high probability of being cancer and should be biopsied or treated surgically
Category 6: Known Biopsy-Proven Malignancy – Appropriate Action Should Be Taken These lesions have been biopsied and are known to be malignant.
Effective 06-06-2016 Chest 6 of 54
CH-1.3 General Guidelines - Chest CT ü Intrathoracic abnormalities found on chest x-ray, fluoroscopy, abdominal CT scan, or
other imaging modalities may be further evaluated with chest CT with contrast (CPT®71260). o “Abnormalities” through these guidelines may include suspected lung or pleural
nodules or masses, pleural effusion, adenopathy or other findings that are not considered benign.
o Lung nodule(s) identified incidentally on Chest CTA without and with contrast (CPT®71275), Chest MRI without contrast (CPT®71550), Chest MRI without and with contrast (CPT®71552) or Chest MRA without and with contrast (CPT®71555) can replace Chest CT with contrast (CPT®71260) or Chest CT without contrast (CPT®71250) as the initial dedicated study.
o See also: CH-16~Solitary Pulmonary Nodule (SPN)
o See also: ONC-8 Non-Small Cell Lung Cancer, Suspected/Diagnosis
ü Chest CT without contrast (CPT®71250) can be used for the following: o Patient has contraindication to contrast o Follow-up of pulmonary nodule(s) o High Resolution CT (HRCT) o Low-dose chest CT (HCPCS code G0297 ) may be appropriate for lung cancer
screening if all of the following NCD 210.14 criteria are met: a. Patient has not received a low-dose CT lung screening in less than 12
months; and b. Patient has NO signs or symptoms suggestive of underlying lung cancer;
and c. Patient is between 55 and 77 years of age; and d. Patient has at least a 30 pack-year history of cigarette smoking; and e. Currently smokes or quit less than 15 years ago; and f. A written order for LDCT lung cancer screening that documents counseling
and shared decision making o See also: ONC-8.1 Non-Small Cell Lung Cancer, Asymptomatic Screening
o Other circumstances as specified in the guidelines
ü Chest CT without and with contrast (CPT®71270) does not add significant diagnostic information above and beyond that provided by chest CT with contrast, unless a question regarding calcification, most often within a lung nodule, needs to be resolved.
Effective 06-06-2016 Chest 7 of 54
Chest CT Coding Notes: High resolution chest CT should be reported only with an appropriate code from the set CPT®71250-CPT®71270. No additional CPT® codes should be reported for the “high resolution” portion of the scan. The “high resolution” involves additional slices which are not separately billable.
CH-1.4 General Guidelines - Chest CTA (CPT®71275) ü Chest CTA can be considered for suspected Pulmonary Embolism and Thoracic
Aortic disease ü CTA prior to minimally invasive or robotic surgery.
(See: CD-1.10 in the Cardiac Imaging Guidelines.) CH-1.5 General Guidelines-Chest MRI without and with contrast (CPT®71552)
ü Indications for chest MRI are infrequent and include:Concerns about CT contrast such as renal insufficiency or contrast allergy
o Clarification of some equivocal findings on previous imaging studies, which are often in the thymic mediastinal region or determining margin (vascular/soft tissue) involvement with tumor and determined on a case by case basis
o Certain conditions, including • Chest wall mass (CH-23~Chest Wall Mass) • Chest muscle tendon injuries (MS-11~Muscle/Tendon Injuries) • Brachial plexopathy (PN-4~Brachial Plexus) and • Thymoma (ONC-10.2 Thymoma)
Effective 06-06-2016 Chest 9 of 54
CH-2.3 Mediastinal Lymphadenopathy ü Chest CT with contrast (CPT®71260) can be performed if mediastinal abnormalities
are detected on a chest x-ray (overread by a radiologist) or other non-dedicated advanced chest imaging.
ü Follow-up chest CT (CPT®71260) can be performed at 4 weeks if o Enlarged lymph nodes are in the mediastinum with no other thoracic abnormalities;
and o Low risk or no clinical suspicion for malignancy o Thereafter, stability does not require further advanced imaging
ü Further evaluations o Lymph node biopsy (see methods below) should be considered for:
1.) persistent lymphadenopathy on follow-up chest CT; or 2.) suspected malignancy
Practice Notes Lymphadenopathy from neoplasms as well as from benign sources of inflammation can result in a positive PET scan. Therefore, the use of PET may not be helpful prior to histologic diagnosis. Less invasive methods of mediastinal biopsies are percutaneous biopsy, transbronchial biopsy, transbronchial biopsy using endobronchial ultrasound, and endoscopic ultrasound-guided FNA. More invasive and traditional methods are mediastinoscopy or thoracoscopy/thoracotomy. References 1. van Overhagen H, Brakel K, Heijenbrok MW, et al. Metastases in supraclavicular lymph nodes in
lung cancer: assessment with palpation, US, and CT. Radiology 2004;232:75-8 Non-randomized Clinical Trails. AAFP Evidence Grade: B
2. Lehman CD, DeMartini W, Anderson BO, et al. Indications for breast MRI in the patient with newly diagnosed breast cancer. J Natl Compr Canc Netw 2009;7(2):193-201. Analysis of National Comprehensive Cancer Network (NCCN) guidelines. AAFP Evidence Grade: A
3. Yamaguchi H, Ishikawa M, Hatanaka K, et al. Occult breast cancer presenting as axillary metastases. The Breast 2006;15:259-262. Case report conducted with single subject. AAFP Evidence Grade: C
4. Stigt, Jos A. MD; Boers, James E. MD, PhD; Oostdijk, Ad H. MD; van den Berg, Jan-Willem K. MD, PhD; Groen, Harry J. MD, PhD. Mediastinal Incidentalomas, Journal of Thoracic Oncology: August 2011 – Volume 6 – Issue 8 – pp 1345-1349. Cohort Study conducted without significant finding. AAFP Evidence Grade: B

Effective 06-06-2016 Chest 12 of 54
Appropriateness Criteria® acute nonspecific chest pain - low probability of coronary artery disease. American College of Radiology (ACR); 2011. Systematic review. AAFP Evidence Grade: A
2. Woodard PK, White RD, Abbara S, Araoz PA, Cury RC, Dorbala S, Earls JP, Hoffmann U, Hsu JY, Jacobs JE, Javidan-Nejad C, Krishnamurthy R, Mammen L, Martin ET, Ryan T, Shah AB, Steiner RM, Vogel-Claussen J, White CS, Expert Panel on Cardiac Imaging. ACR Appropriateness Criteria® chronic chest pain - low to intermediate probability of coronary artery disease. American College of Radiology (ACR); 2012. Meta-analysis. AAFP Evidence Grade: A
3. Proulx AM, Zryd TW. Costochondritis: diagnosis and treatment. Am Fam Physician. 2009 Sep 15;80(6):617. Expert opinion. AAFP Evidence Grade: C
4. UpToDate, Clinical Evaluation of Musculoskeletal Pain, acquired April 15, 2014 Case study. AAFP Evidence Grade: C
Effective 06-06-2016 Chest 23 of 54
Repeat PET is discouraged, since if the original PET is positive, biopsy may be performed. If the original PET is negative but subsequent chest CT shows increase in size of the nodule, biopsy may be performed. False positive PET can occur with infection or inflammation; false negatives can occur with small size nodule, ground glass lesions and indolent cancers such as bronchoalvealor or carcinoid. References 3. ACR Appropriateness Criteria, Solitary pulmonary nodule, 2008. Guideline. AAFP Evidence Grade:
A 4. Benjamin MS, Drucker EA, McLoud TC, Shepard JAO. Small pulmonary nodules: detection at
chest CT and outcome. Radiology 2003;226:489-493. Retrospective study with finding. AAFP Evidence Grade: A
5. Fletcher JW, Kymes SM, Gould M, et al. A comparison of the diagnostic accuracy of 18F-FDG PET and CT in the characterization of solitary pulmonary nodules. J Nucl Med 2008;49:179-185. Prospective study with significant finding. AAFP Evidence Grade AAFP: A
6. Henschke CI, McCauley DI, Yankelevitz DF, et al. Early Lung Cancer Action Project: overall design and findings from baseline screening. Lancet 1999 July;354(9173):99-105. Prospective study with finding. AAFP Evidence grade: B
7. Henschke CI, Yankelevitz DF, Mirtcheva R, et al. CT screening for lung cancer: frequency and significance of part-solid and nonsolid nodules. AJR 2002 May:178(5):1053-1057. Case study. AAFP Evidence grade: C
8. Henschke CI, Yankelevitz DF, Naidich DP, et al. CT screening for lung cancer: suspiciousness of nodules according to size on baseline scans. Radiology 2004;231:164-168. Retrospective study without finding. AAFP Evidence Grade: C
9. Libby DM, Smith JP, Altorki NK, et al. Managing the small pulmonary nodule discovered by CT. Chest 2004 April;125(4):1522-1529. Prospective non-comparative study. AAFP Evidence Grade: A
10. Lindell RM, Hartman TE, Swensen SJ, et al. Lung cancer screening experience: a retrospective review of PET in 22 non-small cell lung carcinomas detected on screening chest CT in a high-risk population. AJR 2005;185:126-131. Respective study without finding. AAFP Evidence Grade: C
11. MacMahon H, Austin JHM, Gamsu G, et al. Guidelines for management of small pulmonary nodules detected on CT scans: a statement from the Fleischner Society. Radiology 2005;237:395-400. Guideline. AAFP Evidence Grade: A
12. Michael K. Gould, MD, FCCP; James Fletcher, MD; Mark D. Iannettoni, MD, FCCP; William R. Lynch, MD; David E. Midthun, MD, FCCP; David P. Naidich, MD, FCCP; David E. Ost, MD, FCCP, Evaluation of Patients With Pulmonary Nodules: When Is It Lung Cancer? ACCP Evidence-Based Clinical Practice Guidelines (2nd Edition), Chest, September 2007, Vol 132, No. 3_suppl. Guidelines based on systematic review. AAFP Evidence Grade: A
13. Naidich et al, Recommendations for the Management of Subsolid Pulmonary Nodules Detected at CT: A Statement from the Fleischner Society, Radiology: Volume 266: Number 1—January 2013 Guideline. AAFP Evidence Grade: A
14. Swensen SJ, Jett JR, Hartman TE, et al. CT screening for lung cancer: five-year prospective experience. Radiology 2005;235:259-265. Prospective study with finding. AAFP Evidence Grade: A
15. Winer-Muram HT. The solitary pulmonary nodule. Radiology 2006 April;239(1):34-49. Expert opinion. AAFP Evidence Grade: C

Effective 06-06-2016 Chest 33 of 54
Breast MRI - Practice Notes The American Cancer Society, the Society of Breast Imaging, and the National Comprehensive Cancer Network (NCCN) Clinical Guidelines in Oncology recommend breast MRI be performed in facilities that have the capability to perform MRI-guided breast biopsies. Although breast MRI has superior sensitivity in identifying new unknown malignancies, it carries a significant false positive risk when compared to mammogram and ultrasound. Incidental lesions are seen on 15% of breast MRI’s and increase with younger age The percentage of incidental lesions that turn out to be malignant varies from 3% to 20% depending on the patient population. Cancer is identified by breast MRI in only 0.7% of those with “inconclusive mammographic lesions.”
CH-25.3 Breast Reconstruction ü CTA or MRA of the body part from which the free tissue transfer flap is being taken,
can be performed for breast reconstruction preoperative planning. o For example, CTA (CPT®74175 and CPT®72191) or MRA (CPT®74185 and
CPT®72198) of the abdomen and pelvis for Deep Inferior Epigastric Perforators (DIEP) flap
ü There is currently insufficient evidence-based data to support the need for routine advanced imaging for TRAM flaps or other flaps performed on a vascular pedicle.
CH-25.4 CAD for Breast MRI ü The use of CAD with breast MRI is currently considered investigational,
experimental, and/or unproven. o 3D rendering codes (CPT®76376 or CPT®76377) should not be used in
conjunction with code 0159T. See: Preface-4.1 3D Rendering
CH-25.5 Breast MRI Indications ü Breast MRI is indicated for Breast Augmentation, Breast Implants (saline or silicone),
Breast Reconstruction, Free Injection, and Capsular Contracture to: o Evaluate or confirm breast implant rupture when mammography or ultrasound is
uninterpretable • If leakage is detected on MRI or any other modality, the implant(s) should be
removed and no further surveillance MRI of the affected breast(s) is indicated. • Surveillance for silent/asymptomatic rupture of silicone implants is considered
investigational. ü Annual breast MRI is indicated for high risk histologies:
o Atypical ductal hyperplasia (ADH); Atypical lobular hyperplasia (ALH); Lobular carcinoma in situ (LCIS)
ü Annual breast MRI should begin at age 25 for patients considered high risk:
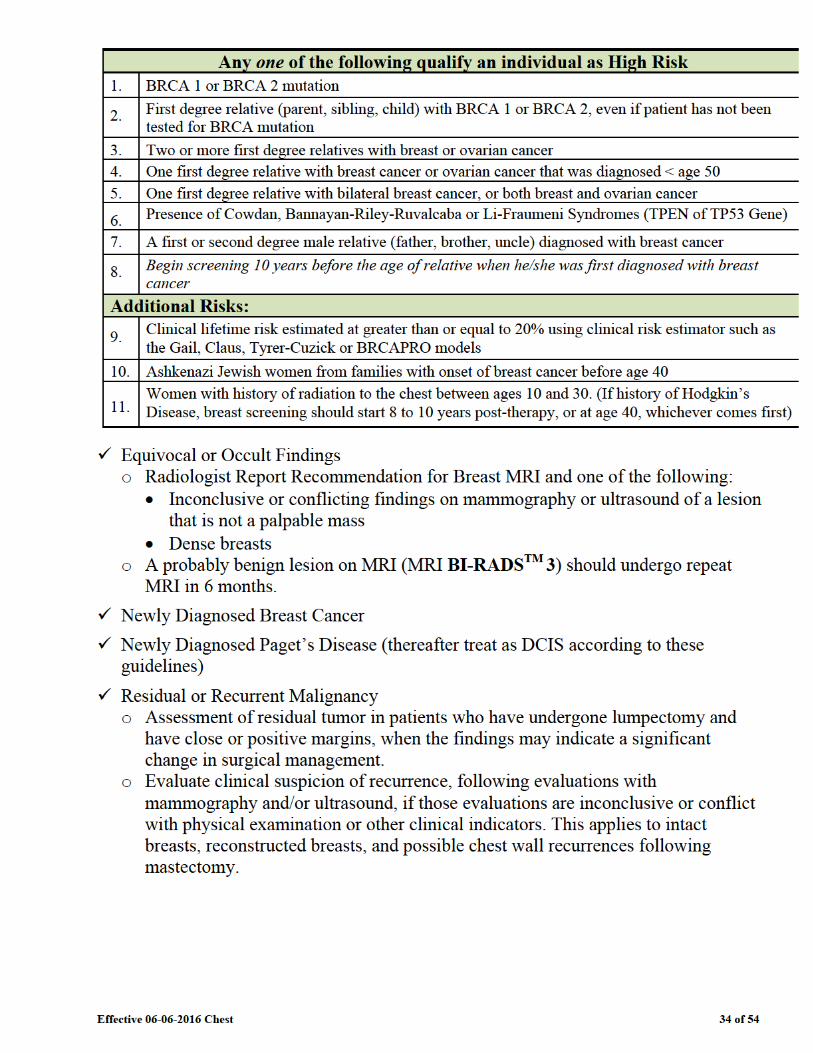
Effective 06-06-2016 Chest 35 of 54
Breast MRI Indications - Practice Notes MRI should not be used in lieu of mammographically, clinically, and/or sonographically suspicious findings (ACR Practice Guidelines).
CH-25.6 Breast MRI is NOT Indicated ü Breast MRI should not be used to determine biopsy recommendations for suspicious
or indeterminate lesion(s) that can be readily biopsied, either using imaging guidance or physical exam, such as palpable masses and microcalcifications.
ü MRI should not be used for routine surveillance in patients with history of breast cancer, unless there are physical exam, imaging findings, recurrent, or residual disease at the mastectomy site o Annual screening breast MRI study is indicated for high risk patients as outlined in
CH-25.5 Breast MRI Indications
ü Patients with dense breasts as determined by mammogram o To date, evidence does not suggest improved outcomes for women whose only risk
factor is breast density (see heading “Equivocal or Occult Findings” (Radiologist Report) in CH-25.5 Breast MRI Indications)
ü Low risk, probably benign (BI-RADS™ 3) lesions o Repeat the original type study (mammogram, US or MRI) in 6 months, thereafter
screening or surveillance does not require MRI
ü Suspicious (BI-RADS™ 4 or 5) lesion on mammogram and/or ultrasound o Bilateral total breast ultrasound (CPT®76641: unilateral, complete), and bilateral
axillary ultrasound (CPT®76882) are recommended for patients who have BI-RADSTM 4 or 5 abnormalities. If additional suspicious breast lesions or more extensive malignant breast disease is detected by ultrasound, the extent of disease can be mapped with ultrasound-guided biopsies (CPT®76942).
o A lesion categorized as have BI-RADSTM 4 or 5 should be biopsied. o A palpable lesion should be considered for biopsy.
Effective 06-06-2016 Chest 36 of 54
CH-25.7 Nipple Discharge/Galactorrhea ü Mammogram should be obtained. Ultrasound (CPT®76641: unilateral, complete or
CPT®76642: unilateral, limited), may be helpful to locate a duct papilloma, an intraductal nodule, or dilated duct.
ü Current evidence does not support the use of MRI in the evaluation of nipple discharge/galactorrhea.
ü If examination and laboratory findings reveal: o Bloody or palpable abnormality – consider open biopsy o Milky or clear discharge - Prolactin and TSH levels to diagnose prolactinoma;
pituitary imaging is not needed if normal serum Prolactin o Ductogram and duct excision can be considered for papilloma which can undergo
excisional biopsy. Nipple Discharge/Galactorrhea – Practice Notes If mammography and endocrine studies are normal, observation and clinical re-evaluation should be performed. If clinical evaluation at the time of follow- up does not reveal any palpable or visible abnormalities, the patient should return to routine screening interval studies with mammogram or clinical exam.
CH-25.8 Breast Pain ü Mammogram and ultrasound are the initial imaging for breast pain ü Advanced imaging is NOT routinely indicated in patients with breast pain and
negative evaluation (evaluation includes patient history and physical exam, pregnancy test, mammogram and ultrasound (CPT®76641: unilateral, complete or CPT®76642: unilateral, limited).
o If evaluation is not negative, see CH-25.5: Indications for Breast MRI
Breast Pain – Practice Notes The risk of malignancy following a negative examination has been estimated to be only 0.5%.
CH-25.9 Newer Breast Imaging Techniques ü RODEO MRI: Rotating Delivery of Excitation Off-Resonance MRI is a trademarked
version of MRI. o There is no unique CPT® code or different reimbursement for breast MRI scans
performed using the RODEO system, and the indications for breast MRI are no different (see CH-25.5 Breast MRI Indications).
ü Positron-Emission Mammography (PEM) or Naviscan®: See: CH-25.9
Effective 06-06-2016 Chest 37 of 54
ü Scintimammography o Nuclear medicine study that uses a radioisotope such as Tc-99 tetrofosmin to
image the breast. Breast cancer typically shows increased uptake of the radioisotope compared to benign lesions.
o There is insufficient data currently to generate appropriateness criteria for the use of scintimammography
o Scintimammography is not currently an MSI contracted service
References 1. Moy, L, Elias, K, Pate, V, et al., (2009). Is breast MRI helpful in the evaluation of inconclusive
mammographic findings? American Journal of Roentgenology, 193(4), 986-993. Retrospective study, with recommendation for stricter patient selection criteria. AAFP Evidence Rating: C
2. ACR Practice Guidelines. Guideline. AAFP Evidence Rating: A 3. Pinel-Giroux FM, El Khoury MM, Trop I, et al. (2013). Continuing medical education: Breast
reconstruction: review of surgical methods and spectrum of imaging findings. Radiographics, 33, 435-453. Retrospective analysis, without significant finding. AAFP Evidence Grade: C
4. Lehman CD, Gatsonis C, Kuhl CK, et al. MRI evaluation of the contralateral breast in women with recently diagnosed breast cancer. N Engl J Med 2007 March;356(13):1295-1303. Prospective study with finding. AAFP Evidence Grade: A
5. Lim HS et al. (2011). Paget Disease of the breast: mammographic, US, and MR imaging findings with pathologic correlation. Radiographics, 31(7), 1973-1987. Expert opinion. AAFP Evidence Grade: C
6. Saslow D, Boetes C, Burke W, et al. American Cancer Society guidelines for breast screening with MRI as an adjunct to mammography. CA Cancer J Clin 2007;57:75-89. http://ghr.nlm.nih.gov/gene/TP53 Guideline. AAFP Evidence Grade: A
7. Morrogh M, Morris EA, Liberman L, et al., (2007). The predictive value of ductography and magnetic resonance imaging in the management of nipple discharge. Ann Surg Oncol, 14, 3369. Retrospective analysis without finding. AAFP Evidence grade: B
8. Institute for Clinical Systems Improvement (ICSI), Health Care Guideline: Diagnosis of Breast Disease. Fourteenth Edition. Updated January 2012 .http://www.icsi.org. Accessed May 28, 2016. Guideline. AAFP Evidence Rating: A
9. ACOG. Management of women with dense breasts diagnosed by mammography. Committee Opinion, 2014; number 593. Expert opinion. AAFP Evidence Grade: C
Effective 06-06-2016 Chest 40 of 54
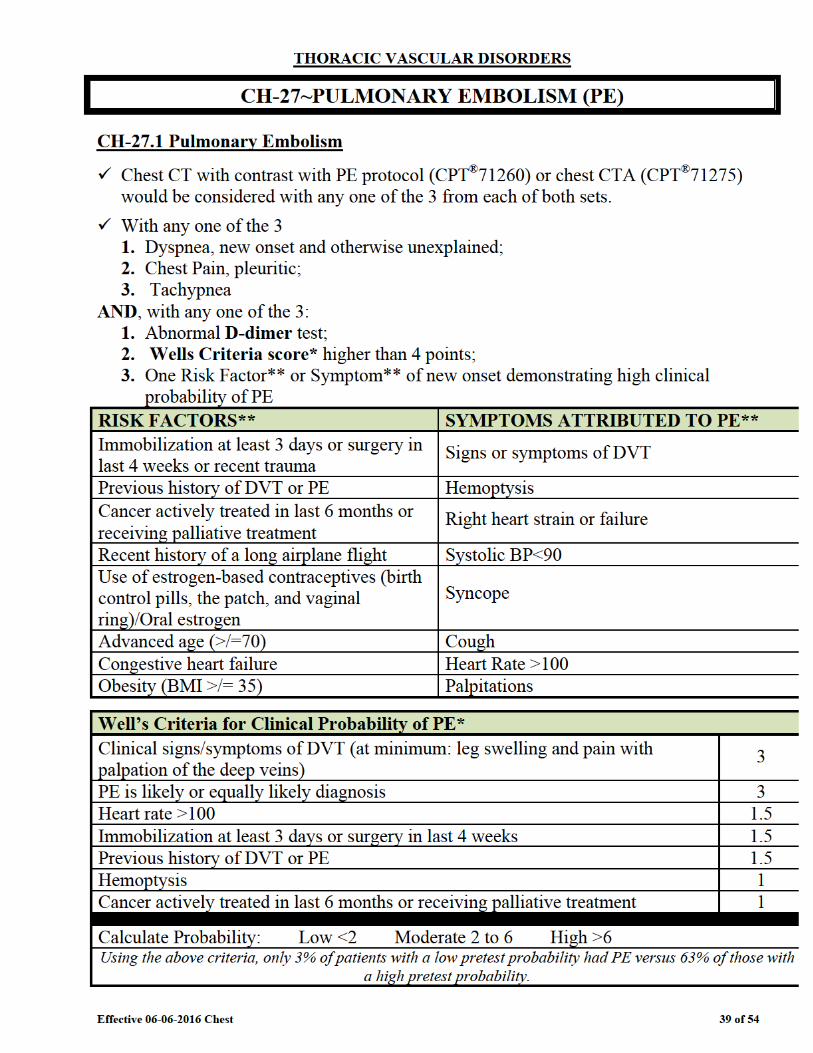
ü Non-urgent cases which do not meet above 2-step criteria, should undergo prior to advanced imaging: o Chest x-ray (to rule out other causes of acute chest pain) o Primary cardiac and pulmonary etiologies should be eliminated.
ü Pregnant women with suspected PE are suggested to proceed with o D-dimer and/or; o Doppler studies of the lower extremities; o V/Q preferred if Doppler negative; Chest CTA (CPT®71275) or chest MRA
(CPT®71555) can be performed if V/Q scanning is not available. ü Follow-up Imaging in Stable or Asymptomatic Patients with Known PE is not warranted
o Chest CT with contrast with PE protocol (CPT®71260) or chest CTA (CPT®71275) can be performed for any of the following indications:
• Recurrent signs or symptoms such as dyspnea, or • Elevated d-dimer which is persistent or recurrently elevated, or • Right heart strain or failure identified by EKG, ECHO or Heart
catheterization Practice Notes Pulmonary embolism is found in approximately 10% of all those that present with suspicion of PE. Dyspnea, pleuritic chest pain and tachypnea occur with about 50% incidence with leg swelling or pain just over 50%. D-dimer level has a high sensitivity and low specificity for diagnosing PE. o A negative D-dimer in combination with low or moderate PE risk classification has a
negative predictive value approaching 100%. o D-dimer can be falsely elevated with recent surgery, injury, malignancy, sepsis,
diabetes, pregnancy, or other conditions where fibrin products are likely to be present.
CT imaging has supplanted V/Q scanning since the latter is difficult to obtain quickly, does not provide a substantial cost savings, and does not diagnose other pulmonary pathology. The decision to terminate anticoagulation treatment after previous pulmonary embolism (PE) with absent or stable symptoms is based on clinical evaluation and risk factors.
o Repeat studies do not allow one the ability to distinguish new from residual clot, with luminal diameter and clot character poorly correlated to symptoms and ECHO findings.
o Two thirds after primary thromboembolism have residual pulmonary artery clot at 6 months and 50% remains at one year.
o Subsequent persistence or elevation of D-dimer is associated with increased risk of recurrent PE. ECHO and Right Heart Catheterization (RHC) can identify those with pulmonary hypertension. Yet, 1/2 of all have persistent or new pulmonary hypertension after primary thromboembolism and only half of this latter group has dyspnea at rest or exercise intolerance.
Effective 06-06-2016 Chest 41 of 54
References 1. Abcarian PW. Role of a Quantitative D-Dimer Assay in Determining the Need for CT Angiography
of Acute Pulmonary Embolism. AJR 2004;182:1377-1381. Prospective analysis with finding. AAFP Evidence Grade: A
2. Canonico M, Plu-Bureau G, Lowe GDO, Scarabin, P., (2008). Hormone replacement therapy and risk of venous thromboembolism in postmenopausal women: systematic review and meta-analysis. BMJ 2008;336:1227 Systematic review and meta-analysis. AAFP Evidence Grade: A
3. Courtney, D. M., et al. (2010). "Prospective diagnostic accuracy assessment of the HemosIL HS D-dimer to exclude pulmonary embolism in emergency department patients." Thromb Res 125(1): 79-83. Prospective observational study with finding. AAFP Evidence grade: A
4. Di Nisio M, Squizzato A, Rutjes AW, Buller HR, Zwinderman AH, Bossuyt PM. Diagnostic Accuracy of D-Dimer Test for Exclusion of Venous Thromboembolism: A Systematic Review. J Thromb Haemost. 2007 Feb;5(2):296-304. Meta-analysis. AAFP Evidence Grade: A
5. Fedullo PF, Auger WR, Kerr KM, et al. Chronic thromboembolic pulmonary hypertension. N Engl J Med 2001;345:1465-1472. Quantitative research. AAFP Evidence Grade: C
6. Kass SM, Williams PM, Reamy BV. Pleurisy. Am Fam Physician 2007 May;75(9):1357-1364. Expert opinion. AAFP Evidence Grade: C
7. Kavanagh EC, O’Hare A, Hargaden G, Murray JG. Risk of pulmonary embolism after negative MDCT pulmonary angiography findings. AJR 2004;182:499-504. Prospective study without finding. AAFP Evidence Grade: B
8. Kline JA, Steuerwald MT, Marchick MR, et al. Prospective evaluation of right ventricular function and functional status 6 months after acute submassive pulmonary embolism: frequency of persistent or subsequent elevation in estimated pulmonary artery pressure. Chest 2009;136:1202-1210. Prospective study with finding. AAFP Evidence Grade: A
9. Kruip MJ, Slob MJ, Schijen JA, et al. Use of a clinical decision rule in combination with D-dimer concentration in diagnostic workup of patients with suspected pulmonary embolism: A prospective management study. Arch Intern Med 2002;162:1631-1635. Prospective management study with finding. AAFP Evidence Grade: A
10. Nijkeuter M, Hovens MMC, Davidson BL, et al. Resolution of thromboemboli in patients with acute pulmonary embolism. A systematic review. Chest 2006;129:192-197. Systematic review. AAFP Evidence Grade: A
11. Palareti G, Cosmi B, Legnani C, et al. d-Dimer testing to determine the duration of anticoagulation therapy. N Engl J Med 2006;355:1780-1789. Prospective study of foreign origin, with finding. AAFP Evidence Grade: B
12. Paterson DI, Schwartzman K. Strategies incorporating spiral CT for the diagnosis of acute pulmonary embolism: a cost-effectiveness analysis. Chest 2001 June;119(6):1791-1800. Simulated cohort study. AAFP Evidence Grade: B
13. Ramzi DW and Leeper KV. DVT and pulmonary embolism: part II. Treatment and prevention. Am Fam Physician 2004 June;69(12):2841-2848. Expert opinion. AAFP Evidence Grade: C
14. Stein PD, Terrin ML, Hales C, et al. Clinical, laboratory, roentgenographic, and electrocardiographic findings in patients with acute pulmonary embolism and no pre-existing cardiac or pulmonary disease. Chest 1991;100(3):598-603. Prospective study with finding. AAFP Evidence Grade: A
15. Stein PD, Woodard PK, Weg JG, et al. Diagnostic pathways in acute pulmonary embolism: Recommendations of the PIOPED II investigators. Radiology 2007 Jan;242(1):15-21. Expert recommendations. AAFP Evidence Grade: C
16. Stein PD, Fowler SE, Goodman LR, et al. Multidetector computed tomography for acute pulmonary embolism. N Engl J Med 2006 June;354(22):2317-2327. Prospective investigation with finding. AAFP Evidence Grade: A
17. Wells PS, Anderson DR, Rodger M, et al. Derivation of a simple clinical model to categorize
Effective 06-06-2016 Chest 42 of 54
patient’s probability of pulmonary embolism: increasing the models utility with the SimpliRED D-dimer. Thromb Haemost 2000 Mar;83(3):416-420. Retrospective analysis with finding. AAFP Evidence Grade: B
18. Wells PS. Anderson DR. Rodger M,et al. Excluding pulmonary embolism at the bedside without diagnostic imaging: management of patients with suspected pulmonary embolism presenting to the emergency department by using a simple clinical model and d-dimer. Ann Intern Med. 2001 Jul 17:135(2): 98-107. PubMed PMID: 11453709. Prospective study with finding. AAFP Evidence Grade: A
19. Wolf SJ. McCubbin TR Feldhaus KM. Faragher JP. Adcock DM. Prospective validation of Wells Criteria in the evaluation of patients with suspected pulmonary embolism. Ann Emerg Med. 2001 Nov:44(5): 503-10. PubMed PMID: 15520710. Prospective observational study without finding. AAFP Evidence Grade: B
20. Writing Group for the Christopher Study Investigators. Effectiveness of managing suspected pulmonary embolism using an algorithm combining clinical probability, D-dimer testing, and computed tomography. JAMA 2006 Jan;295(2):172-179. Prospective cohort study. AAFP Evidence Grade: A
21. van Belle, A., et al. (2006). "Effectiveness of managing suspected pulmonary embolism using an algorithm combining clinical probability, D-dimer testing, and computed tomography." JAMA 295(2): 172-179. Prospective cohort study. AAFP Evidence Grade: A
Effective 06-06-2016 Chest 44 of 54
ü Upper extremity MRA (CPT®73225) or CTA (CPT®73206) can be performed in symptomatic patients if needed to exclude pathology distal to the subclavian artery and if they will substitute for invasive angiography.
See also HD-21.1 Vertebrobasilar Ischemia in the Head Imaging Guidelines.
Treatment options include ligation of the ipsilateral vertebral artery, aorta-subclavian artery bypass graft, or subclavian endarterectomy.
References 1. Potter B, Pinto D. Subclavian Steal Syndrome. Circulation. 2014;129:2320-2323, published online
before print June 2, 2014. Expert review of current practices. AAFP Evidence Grade: C 2. Van Brimberge F, Dymarowski S, Budts W, Bogaert J. Role of magnetic resonance in the diagnosis
of subclavian steal syndrome. J Magn Reson Imaging. 2000;12(2):339. Descriptions of two cases of subclavian steal syndrome. AAFP Evidence Grade: C


Effective 06-06-2016 Chest 47 of 54
month interval advanced imaging o Surgery or Stent
• Preoperative open or endovascular (stent) repair imaging is appropriate • Open Repair imaging every 3 to 5 years
o Endovascular graft/stent • First year: 1 month, 3 months, 6 months, 12 months, then annually
ü Screening with Abdominal Aortic Aneurysm (AAA) o Known TAA can be screened for AAA using Abdominal Imaging Guidelines
(usually US) (see: AB-17.1 Abdominal Aortic Aneurysm) o Known AAA screening for TAA is not supported by sufficient evidence
.
CH-30.3 Screening Guidelines for Familial Syndromes ü Screening for Familial Syndromes and Genetic Syndromes
o Suspected Familial Thoracic Aortic Aneurysm • ECHO (CPT®93306, CPT®93307, or CPT®93308) and CXR for all First-
degree relatives (parents, siblings, children) of patients with TAA and/or dissection
o Any imaging listed can be performed if these studies identify a TAA or are equivocal or do not visualize the ascending aorta adequately
o Follow-Up per TAA Follow-Up guidelines ü Screening for Marfan Syndrome or Ehlers-Danlos Syndrome, Vascular form or Type
IV o Suspected, ECHO (CPT®93306, CPT®93307, or CPT®93308) at the time of
diagnosis. o Follow-up:
• Annual ECHO (CPT®93306, CPT®93307, or CPT®93308) or per TAA Follow-Up guidelines
CH-30.4 Thoracic Aorta in Indiviuals with Bicuspid Aortic Valve ü Screening for Bicuspid Aortic Valve
o Suspected, any requested imaging from the “Table of Thoracic Aorta Imaging Options” and/or ECHO (CPT®93306, CPT®93307, or CPT®93308) • Additional imaging such as cardiac MRI, cardiac CT, or CCTA is NOT
generally indicated. • There is no evidence-based data to support screening relatives of patients
with bicuspid aortic valve. o Follow-up per TAA Follow-Up guidelines
• If no dilatation of the aortic root or ascending thoracic aorta is found, there is no evidence-based data to support continued surveillance imaging.
Practice Notes
Aortic Dissection
Effective 06-06-2016 Chest 48 of 54
There are two general types of aortic dissection: 1. Type A: Those that begin in the ascending aorta 2. Type B: Those that begin from just distal to the left subclavian artery branch of the
aorta Type A often requires urgent surgical intervention with placement of an aortic graft or endovascular stent graft. Type B can usually be treated medically with careful blood pressure control. Surgery is reserved for distal dissections that are leaking, ruptured, or compromising blood flow to a vital organ, or if there is inability to control the blood pressure. Transesophageal echo may be equally diagnostic compared to CT or MRI. Routine follow-up imaging is important because 30%-40% of chronic dissections will become aneurysmal in 5 years and will require intervention, with less patent false lumina at higher risk. Penetrating ulcer (through the intima) and intramural hematoma (no intimal tear) are variant forms of aortic dissection and should follow that of aortic dissection, since they are considered precursors of aortic dissection. TAA The normal size of the aortic arch and descending thoracic aorta is 3 cm. The aortic root is normally 3.5 cm:
o TAA occurs most often in the descending (50%) and then equally likely in the ascending or arch aorta.
o Risk factors include atherosclerosis, prolonged hypertension and trauma with mean age 65.
o Risk of rupture is 0% if < 4 cm and 31% if > 6 cm, which is when surgery is often recommended.
Familial TAA Familial TAA presents at an earlier age, has a faster aortic growth rate, is seen in about 20% or non-Marfan TAA and has autosomal dominant inheritance, when compared to non-familial TAA. Bicuspid Aortic Valve Since 20% of individuals who underwent bicuspid aortic valve surgery had concurrent ascending aortic aneurysms that needed repair. All patients with bicuspid aortic valve should have both the aortic root and ascending thoracic aorta evaluated for evidence of aortic dilatation.
Effective 06-06-2016 Chest 49 of 54
References
1. Albornoz G, Coady MA, Roberts M, et. al. Familial thoracic aortic aneurysms and dissections—incidence, modes of inheritance, and phenotypic patterns. Annals of Thoracic Surgery 2006 Oct;82(4):1400-1405. Prospective study with finding. AAFP Evidence Grade: A
2. Elefteriades JA. Natural history of thoracic aortic aneurysms: indications for surgery, and surgical versus nonsurgical risks. Ann Thorac Surg 2002;74:S1877-S1880. Statistical analysis of prospective database. AAFP Evidence Grade: A
3. Evangelista A and Eagle KA. Is the optimal management of acute type a aortic intramural hematoma evolving? Circulation 2009;120:2029-2032. Expert opinion. AAFP Evidence Grade: C
4. Ganaha F, Miller DC, Sugimoto K, Do YS, Minamiguchi H, Saito H, Mitchell RS, Dake MD. Prognosis of aortic intramural hematoma with and without penetrating atherosclerotic ulcer: a clinical and radiological analysis. Circulation 2002 Jul 16;106(3):342-8. Retrospective analysis with finding. AAFP Evidence Grade: A
5. Hiratzka LF, Bakris GL, Beckman JA, et al. 2010 ACCF/AHA/AATS/ACR/ASA/SCA/SCAI/SIR/STS/SVM guidelines for the diagnosis and management of patients with thoracic aortic disease. J Am Coll Cardiol 2010;55:e27-e129. Guideline. AAFP Evidence Grade: A
6. Loren F. Hiratzka MD, et al, 2010 ACCF/AHA/AATS/ACR/ASA/SCAI/SIR/STS/SVM Guidelines for the Diagnosis and Management of Patients With Thoracic Aortic Disease Circulation 2010; 121: e266-e369. Guideline. AAFP Evidence Grade: A
7. Shiga T, Wajima Z, Apfel CC, InoueT, Ohe Y. Diagnostic Accuracy of Transesophageal Echocardiography, Helical Computed Tomography, and Magnetic Resonance Imaging for Suspected Thoracic Aortic Dissection: Systematic Review and Meta-analysis. Arch Intern Med 2006;166(13):1350-1356. Systematic review. AAFP Evidence Grade: A
8. Song JK, Yim JH, Ahn JM, et al. Outcomes of patients with acute type A aortic intramural hematoma. Circulation 2009;120;2046-2052. Prospective study with finding. AAFP Evidence Grade: A
9. Tadros TM, Klein MD, and Shapira OM. Ascending aortic dilatation associated with bicuspid aortic valve. Circulation 2009;119:880-890. Expert opinion. AAFP Evidence Grade: C
Effective 06-06-2016 Chest 53 of 54
ü The spatial resolution of this technique matches individual duct level (1.5 mm full-width at half-maximum) and allows visualization of intraductal as well as invasive breast cancers.
ü Early clinical trials have shown high clinical accuracy in characterizing lesions identified as suspicious on conventional imaging or physical examination.
ü A prospective multi-center clinical trial for women with newly diagnosed breast cancer anticipating breast-conservation surgery was performed. These women underwent both high-resolution PEM imaging and breast MRI. Results showed that PEM and MRI had comparable breast-level sensitivity, although MRI had greater lesion-level sensitivity and more accurately depicted the need for mastectomy. PEM had greater specificity at the breast and lesion levels. 3.6% of the women had tumors seen only at PEM.
ü The radiation exposure from a PEM study is 23 times higher than for digital mammography.
References 1. Weinberg IN, Beylin D, Zavarzin V, et al. Positron emission mammography: high-resolution
biochemical breast imaging. Technol Cancer Res Treat 2005 Feb;4(1):55-60. Overview synthesis. AAFP Evidence Grade: C
2. Tafra L, Cheng Z, Uddo J, et al. Pilot clinical trial of 18F-fluorodeoxyglucose positron-emission mammography in the surgical management of breast cancer. Am J Surg 2005 Oct;190(4):628-632. Prospective study, with recommendation for further investigation. AAFP Evidence grade: B
3. Murthy K, Aznar M, Thompson CJ. Results of preliminary clinical trials of the positron emission mammography system PEM-I: a dedicated breast imaging system producing glucose metabolic images using FDG. J Nucl Med 2000 Nov;41(11):1851-1858. Prospective study with finding. AAFP Evidence Grade: A
4. Hendrick RE. Radiation doses and cancer risks from breast imaging studies. Radiology. August 24, 2010, http://radiology.rsna.org/content/early/2010/08/09/radiol.10100570.full. Meta-analysis. AAFP Evidence Grade: A