-
TRANSCRIBED BY: FRED, GEORGE, RON, BILL, GINNY
Page 1 of 4
Alfredo Guzman, M.D.
People find it far easier to forgive others for being wrong than
being right. Albus Dumbledore, Harry Potter & The Half-Blood
Prince Paulo Coelho
Blood pressure measurement
1.2 9 June
2014
BP MEASUREMENT
Proper measurement & interpretation - essential in the dx
& management of HPN
Home BP & average 24-hr ambulatory BP are generally lower
than clinic-taken BP
BP tends to be higher in the early morning, soon after walking,
than any other time of the day
Night time BP is generally 10-20% lower than day time BP White
Coat HPN
Px manifests a higher BP in a hospital/clinical setting. They
are at risk of developing sustained HPN.
FACTORS AFFECTING BP MEASUREMENTS
Instrumentation o BP Apparatus: Mercury, Aneroid, Digital o BP
cuff size
Area of arm covered
Technique of BP Measurement
Patient Factor
Environment
BP APPARATUS / SPHYGMOMANOMETER MERCURY MANOMETER
Standard for all BP measurements
Large tube for rapid & in pressure
2mm graduated markings on tube
Mylar-wrapped glass or plastic tube preferred
Mercury is at zero and column rises and falls rapidly
TESTING THE MERCURY MANOMETER
Check the 0. Top of meniscus should rest at the zero mark
Inflate to 200 mmHg. Wait 1 min. Record Pressure.
o If
-
TRANSCRIBED BY: FRED, GEORGE, RON, BILL, GINNY
Page 2 of 4
Blood pressure
measurement
Can be used on either right or left arm,
THE STETHOSCOPE
Earpiece should face forward in the ear canal
Must have thick tubing 12-15 inches long
Bell for low pitched sounds
o Used to detect low frequency Korotkoff sounds
Diaphragm for high pitched sounds
5 PHASES OF KOROTKOFF SOUNDS
Korotkoff Sounds produced by the flowing of blood as the
cuff
is released
Phase Description Remarks
I 1st appearance of clear,
tapping sound
Represents Systolic P
(SBP)
II Soft murmurs that
replace Phase I sounds
-
III
Loud murmurs that
replace Phase II
sounds
Due to blood flow
through constricted artery
IV
Sudden muffling of
Phase III sounds
Due to constriction of
the artery; arterial
diastolic P is
approached
V
Disappearance of
Korotkoff sounds
Represents Diastolic BP
(DBP) in most pxs is
normally w/n 10mmHg
from Phase IV
(abnormal if >10mmHg
difference; Phase IV is
abruptly muffled)
The usual BP reading involves Phase I and Phase V Korotkoff
sounds for SBP and DBP, respectively.
If there is a significant difference (>10mmHg) between Phase
IV
and V, both pressures should be recorded (e.g. 130/70/10
mmHg); seen in anemia, aortic regurgitation, thyrotoxicosis.
In chronic, severe aortic regurgitation or a large
arteriovenous
fistula, where the disappearance point may reach 0 mmHg,
Phase
IV is much closer to the intraarterial diastolic pressure than
Phase
V. All 3 pressures should be noted (e.g. 140/60/0 mmHg).
Difficulty in Hearing Korotkoff Sounds
Condition Pathology
Severe aortic stenosis Arterial P rises at a slow rate
Shock Markedly constricted arteries
Severe heart failure Markedly constricted arteries
Opening and closing the fist repeatedly can help dilate
blood
vessels of the arms and make Korotkoff sounds more audible.
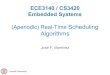
Korotkoff sounds represented during BP measurement. Note the
auscultatory gap.
TECHNIQUES IN BP MEASUREMENT 1. Support arm at the level of the
heart
2. Inflate cuff 30 mmHg above the palpatory BP
3. Release pressure at a rate of 2-3 mmHg/s
Initially, measure BP on both arms
Use arm w/ higher BP on subsequent measurements
Measure BP at least twice per visit; allow 1-2 minutes in
between measurements
If there is >5 mmHg difference between 2 consecutive
measurements, additional or continued measurements should be
made
Take the average of the last 2 BP measurements and record
TECHNIQUE OF BP MEASUREMENT IN THE DX OF HPN I. TIMING OF BP
MEASUREMENT
For Dx: Multiple readings taken at various times throughout
waking hours
For Monitoring: Measure prior to intake of anti-hypertensive
medication to determine trough or nadir effect
II. PATIENT POSITION
Usually taken while sitting slouched on the chair
o Supine position SBP & DBP by 2-3 mmHg
Allow patient to rest and sit quietly for 5 minutes
o Apprehension increases BP
Measure both sitting and standing BP to detect postural
hypotension (sudden drop in BP upon standing; in elderly, DM)
III. PATIENT & PHYSICIAN POSITION
Sitting; feet flat on the floor
Arm supported at heart level
Confirm viability of brachial pulse by palpation
Use bell (detection of low-pitched sounds)
-
TRANSCRIBED BY: FRED, GEORGE, RON, BILL, GINNY
Page 3 of 4
Blood pressure
measurement
OBSERVERS SKILL IN BP MEASUREMENT
The brain must be programmed to follow the proper guidelines
every time the P is measured.
Must be able to store the systolic and diastolic P & recall
them
accurately.
Must be able to hear the Korotkoff sounds and knowhow to
interpret them.
Must be able to recall and write down correctly & legibly
the sounds
heard.
Must be able to find & feel the pulses needed for BP
measurement.
UNEQUAL BP IN BOTH ARMS
STEPS IN MEASURING THE BP
STEPS TO ENSURE ACCURATE BP MEASUREMENT
Instruct px to avoid smoking/drinking caffeinated drinks 30
mins
prior to BP measurement
Make the examining room as quiet & comfy as possible
Arm should be supported at heart level. Ask px to sit quietly
for 5
mins on chair
Make sure the arm is free of clothing. There should be NO
arteriovenous fistulas for dialysis, scarring from prior
brachial
artery cutdowns, or signs of lymphedema
Palpate the arm so that the brachial artery (located at the
antecubital crease) is at heart level (roughly level w/ the
4th
interspace at its junction w/ the sternum
If the px is seated, rest the arm on a table a little above the
pxs
waist, if standing, try to support the pxs arm at the mid-chest
level
STEPS IN MEASURING THE BP
Center the inflatable bladder over the brachial artery. Lower
border
of cuff should be 2.5cm above the antecubital crease. Secure
the cuff snugly. Position arm so that it is slightly flexed at
the
elbow,
To determine how high to raise the cuff P, 1st estimate the
systolic
pressure by palpation. As you feel the radial artery w/ the
fingers
of one hand, inflate the cuff until the radial pulse disappears.
Read
this P on the manometer & add 30 mmHg to it. Use of this sum
as
the target for the next inflation prevents discomfort from
unnecessary high cuff P. This also avoids the occasional
error
caused by an auscultatory gap (a silent interval that may be
present between the systolic & diastolic pressure)
Deflate cuff promptly & completely & wait 15-30
seconds
Next, place the bell of a stethoscope lightly over the brachial
artery,
taking care to make an air seal w/ its full rim. Because the
sounds
to be heard, the Korotkoff sounds, are relatively low
pitched,
they are better heard w/ the bell.
Inflate the cuff rapidly again to the level determined, then
deflate it
slowly (2-3mmHg/sec), Note the level at w/c you hear the
sounds
of at least 2 consecutive beats. This is the Systolic
Pressure.
Continue to lower the P slowly until the sounds become muffled
&
then disappear. To confirm the disappearance of sounds, listen
as
the P falls another 10-20mmHg. Then deflate the cuff rapidly
to
zero. The disappearance point, w/c is usually only a few
mmHg
below the muffling pt, provides the best estimate of true
diastolic P
in adults.
Read both the systolic & diastolic levels to the nearest
2mmHg.
Wait 2 mins & repeat. Average your findings. If the 1st 2
readings
differ by 5mmHg, take additional readings,
Avoid slow/ repetitive inflations of the cuff, because the
resulting
venous congestion can cause false readings.
BP should be taken in both arms at least once. Normally,
there
may be a difference in P of 5mmHg & sometimes up to
10mmHg.
Subsequent readings should be made on the arm w/ the higher
pressure.
o Loose cuff/bladder = false high readings
o Earpiece should face forward in the ear canal.
o Bell of the stethoscope is used for low-frequency sounds
o Auscultatory gaps are associated w/ arterial stiffness
&
atherosclerotic disease
o P difference of >10-15mmHg seen in subclavian steal
syndrome
& aortic dissection
o BP of 110/70 is usually normal, but could indicate
significant
hypotension if previous readings are high
DEFINITIONS OF NORMAL & ABNORMAL LEVELS
CATEGORY SBP
(mmHg) DBP
(mmHg)
Normal < 120 and < 80
Prehypertension 120 - 139 or 80 - 89
Hypertension
Stage 1
Stage 2
140 159
160
or
or
90 99
100
BP goal for pxs w/ HPN, DM, or renal disease is
-
TRANSCRIBED BY: FRED, GEORGE, RON, BILL, GINNY
Page 4 of 4
Blood pressure
measurement
o A femoral pulse that is smaller & later than the radial
pulse
suggests coarctation of the aorta or occlusive aortic
disease.
BP is lower in the legs than in the arms in these
conditions.
THE APPREHENSIVE PATIENT
Try to relax the px
Repeat the measurement later in the encounter
Some px will say their BP is only elevated in the office (White
Coat
HPN) & may need to have their BP measured several times
at
home or in a community setting.
THE OBESE OR VERY THIN
For the obese, the a wide cuff (15cm)
If arm circumference exceeds 41cm, us a thigh cuff (18cm
wide)
For the very thin arm, use a pediatric cuff
WEAK/ INAUDIBLE KOROTKOFF SOUNDS
To rule out Coartation of the aorta, consider: Technical
problems: wrong placement of stethoscope, failure to
make full skin contact w/ bell venous engorgement of the arm
from
repeated inflations of the cuff
Consider shock
WHEN KOROTKOFF SOUNDS CANT BE HEARD AT ALL Estimate systolic P
via palpation. Alternative methods such as
Doppler techniques or direct arterial pressure tracings may be
necessary.
To intensify the Korotkoff sounds, these may be done: o Raise
the arm before & while you inflate the cuff. Then lower the
arm & determine the BP. o Inflate the cuff. Ask the px to
make a fist several times. Then take
the BP.
ARRHYTHMIAS
Irregular rhythms produce variations in Pand therefore
unreliable measurements.
Ignore the effects of an occasional premature contraction.
W/ frequent premature contractions or atrial fibrillation,
determine the average of several observations and note that your
measurements are approximate.
THE HYPERTENSIVE PX W/ UNEQUAL BP IN BOTH ARMS
To detect coarctation of the aorta, make 2 further BP
measurements at least once in every hypertensive px:
Compare BP in the arms and legs.
Compare the volume and timing of the radial and femoral pulses.
Normally, volume is equal and the pulses occur simultaneously.
Coarctation of the aorta arises from narrowing of the thoracic
aorta, usually proximal but sometimes distal to the left subclavian
artery.
Coarctation of the aorta & occlusive aortic disease are
distinguished by hypertension in the upper extremities & low BP
in the legs and by diminished or delayed femoral pulse.