Embed Size (px)
Citation preview

STRATEGIES FOR BP MANAGEMENT
Akshal S. Patel, MD
Swedish Neuroscience Institute
No disclosures, no conflicts of interest
■ Not bought and paid for
GOALS
Review BP management in the setting of ICH
Review BP management in the setting of MT
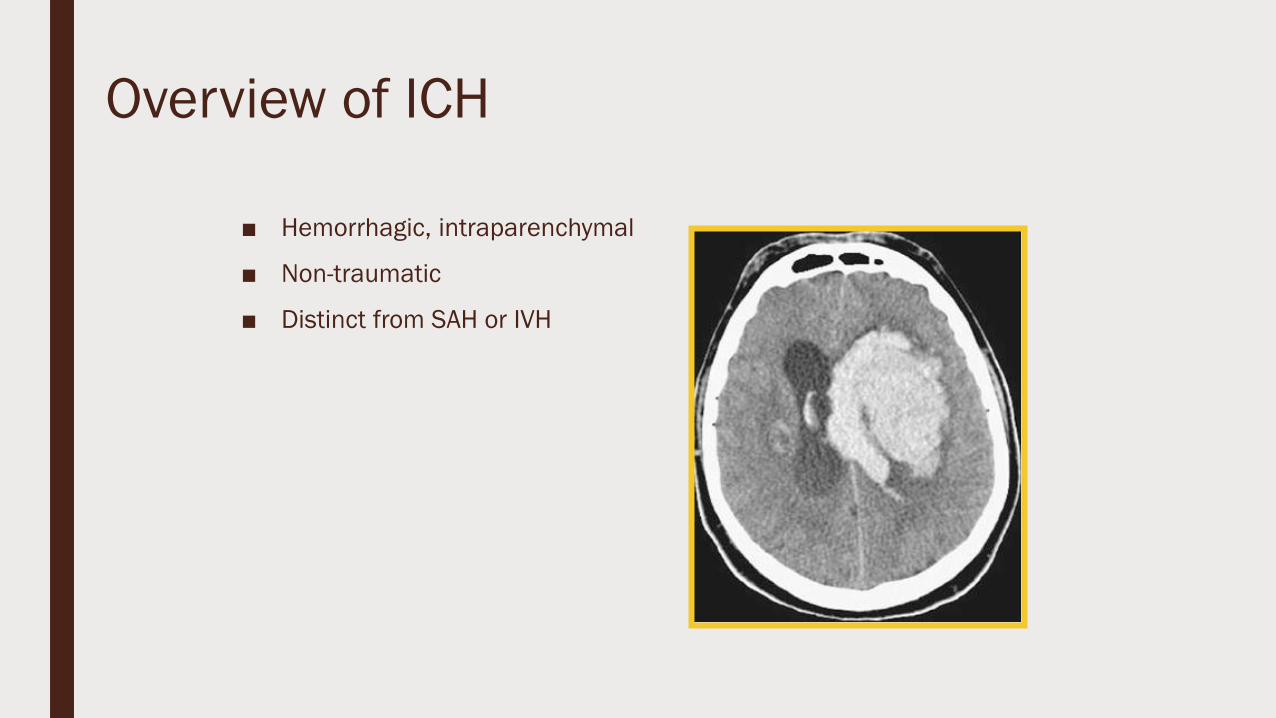
Overview of ICH
■ Hemorrhagic, intraparenchymal
■ Non-traumatic
■ Distinct from SAH or IVH

Not All Hemorrhages are Created Equal
Primary
■ HTN (60-70%)
■ CAA
■ CADASIL
■ Coagulopathy
■ Drug abuse
Secondary
▪ Vascular lesions
▪ AVM, DAVF
▪ Vasculopathy
▪ Ischemic stroke
▪ Post-tPA
▪ HT
▪ CVST
▪ Trauma
▪ Tumor
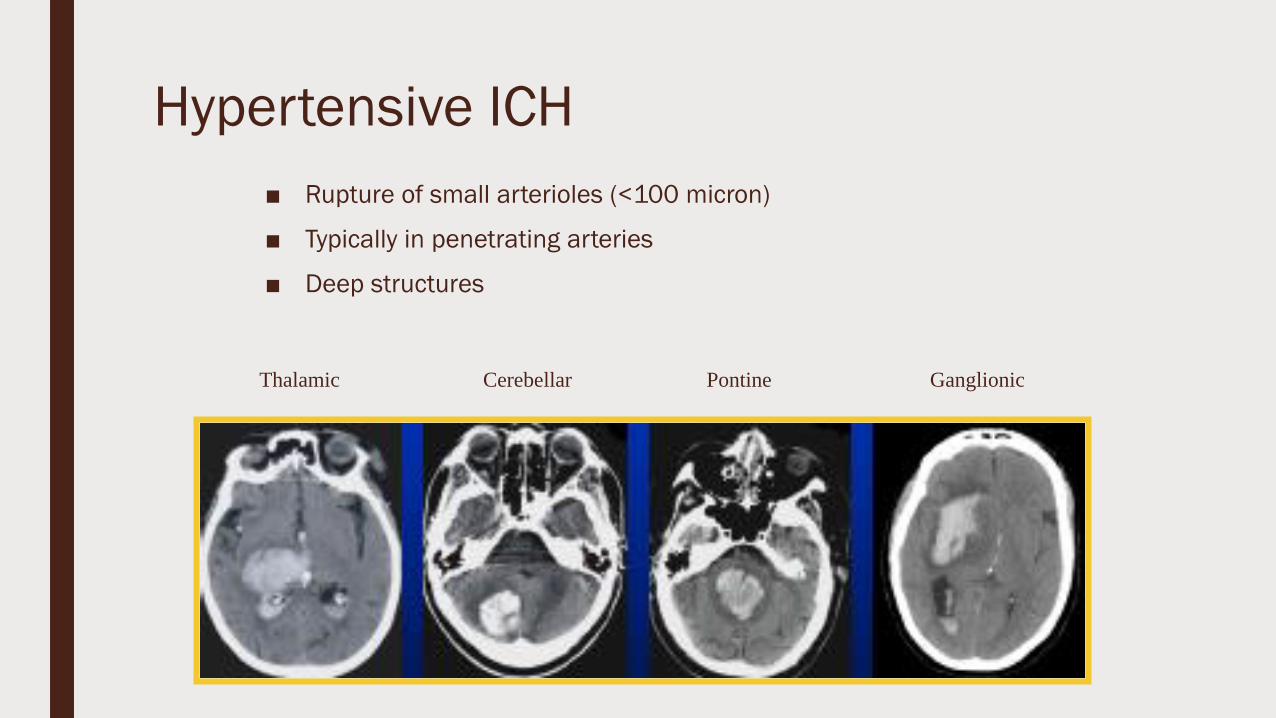
Hypertensive ICH
■ Rupture of small arterioles (<100 micron)
■ Typically in penetrating arteries
■ Deep structures
Thalamic Cerebellar Pontine Ganglionic
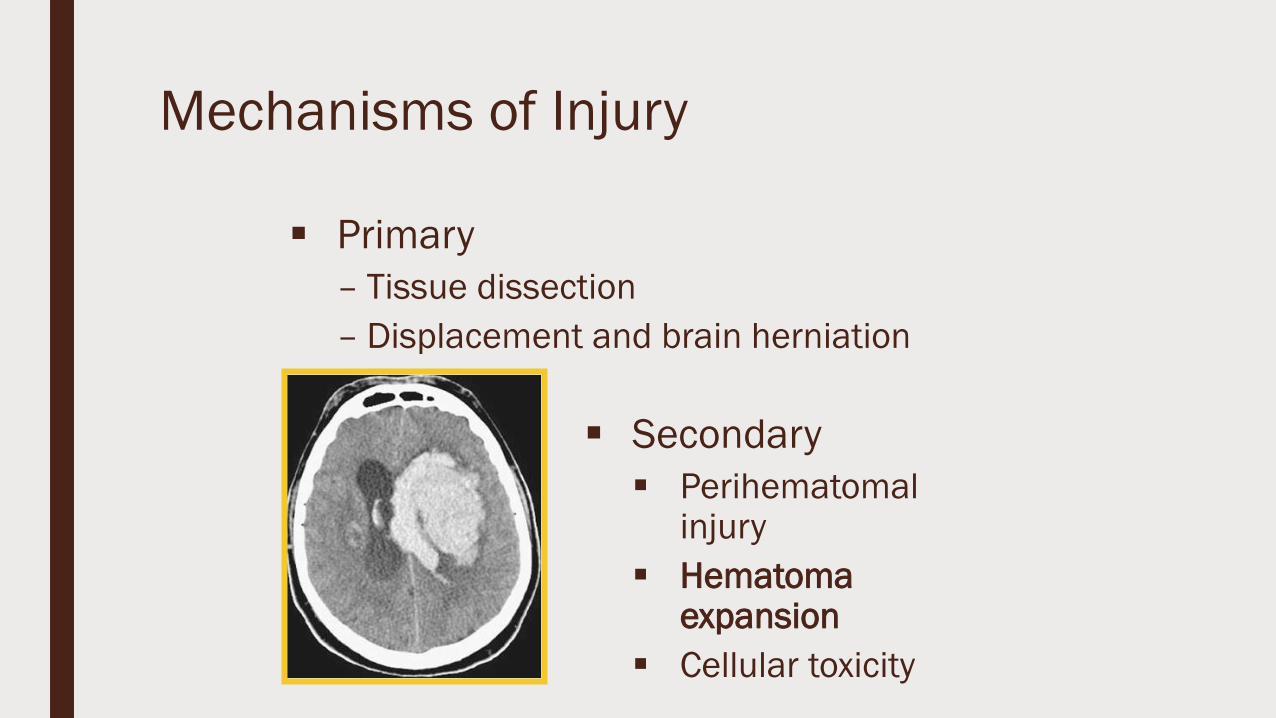
Mechanisms of Injury
▪ Primary
– Tissue dissection
– Displacement and brain herniation
▪ Secondary
▪ Perihematomalinjury
▪ Hematoma expansion
▪ Cellular toxicity

Hematoma Expansion
Hemphill, 2008
Hematoma Expansion
▪ Expansion not uncommon
▪ No longer just seen with AVMs or coagulopathy
▪ 72% have some expansion over 24h
▪ 38% have more than 33% expansion first 24h
▪ Usually clinically significant
▪ Within 1 hr in ¼ of cases
▪ Hematoma expansion worsens outcome
Davis et al., Neurology 2006
Brott et al., Stroke 1997

Hematoma Expansion
Kazui et al., Stroke 1997
Jauch et al., Stroke 2006
Powers et al., Neurology 2001
■ Mechanism unknown
– Elevated BP?
■ Elevated GLU on admission & SBP>200 mm Hg
■ Acute NCP gtt in small-to-med ICH
– MAP lowering of 15% does not affect global or peri-hematomal PET-CBF
– Preserved autoregulation– Perihematoma coagulopathy/DIC?
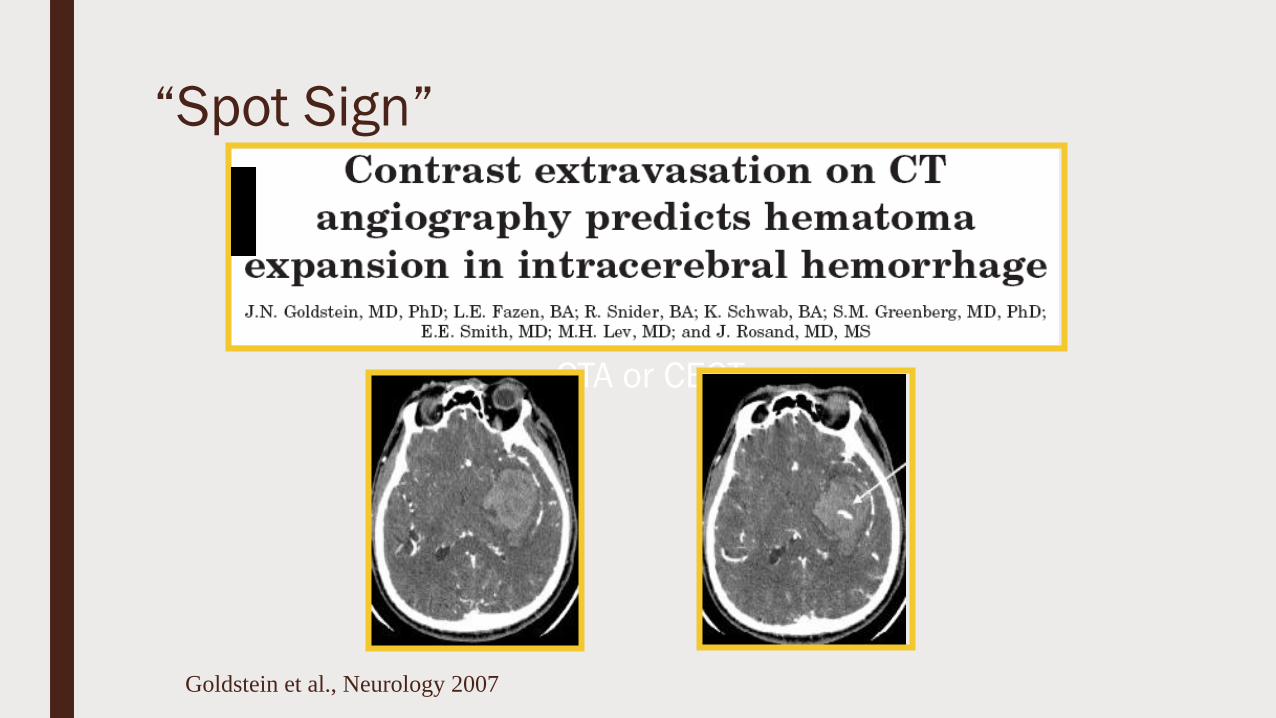
“Spot Sign”
Goldstein et al., Neurology 2007
CTA or CECT
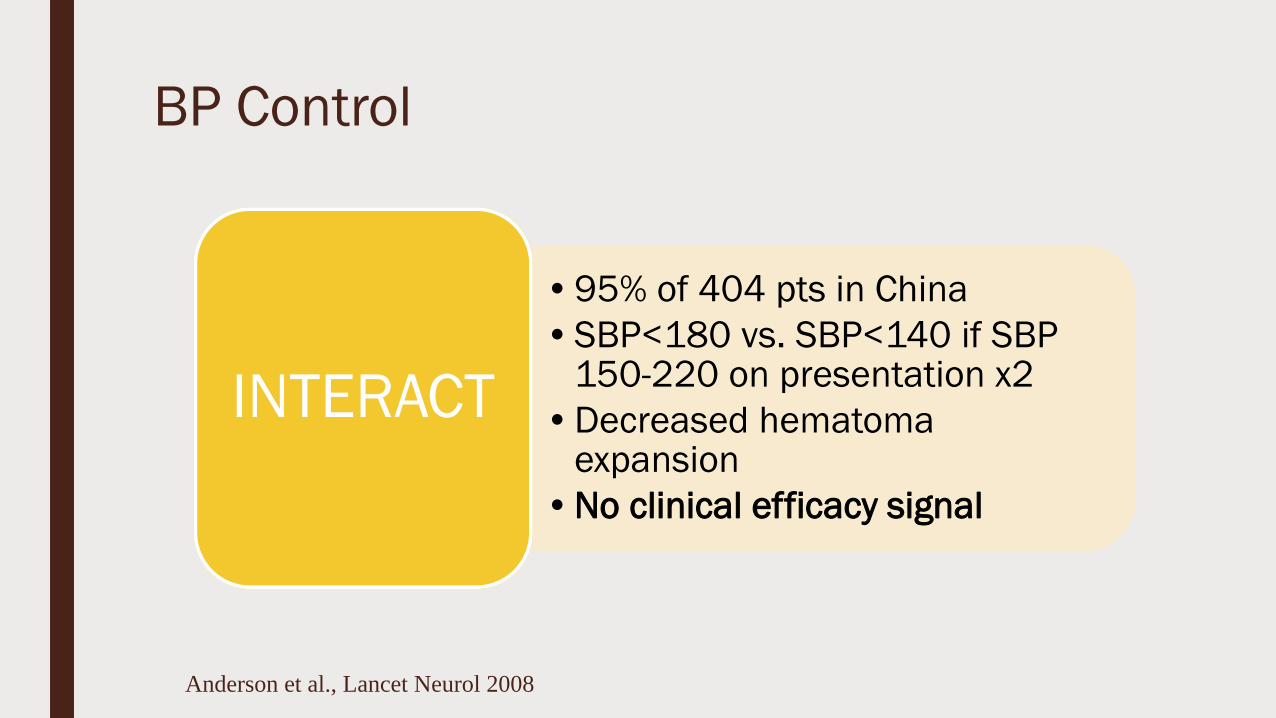
BP Control
Anderson et al., Lancet Neurol 2008
•95% of 404 pts in China
•SBP<180 vs. SBP<140 if SBP 150-220 on presentation x2
•Decreased hematoma expansion
•No clinical efficacy signal
INTERACT
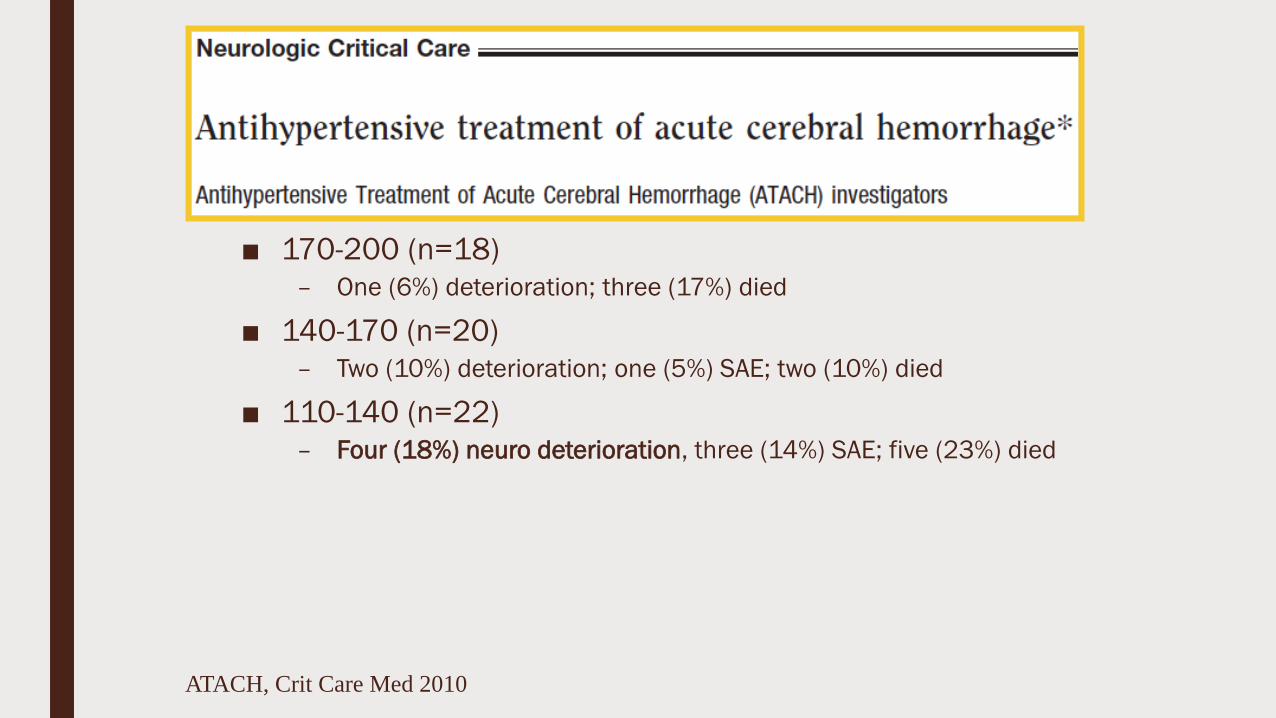
ATACH, Crit Care Med 2010
■ 170-200 (n=18)
– One (6%) deterioration; three (17%) died
■ 140-170 (n=20)
– Two (10%) deterioration; one (5%) SAE; two (10%) died
■ 110-140 (n=22)
– Four (18%) neuro deterioration, three (14%) SAE; five (23%) died

BP Control
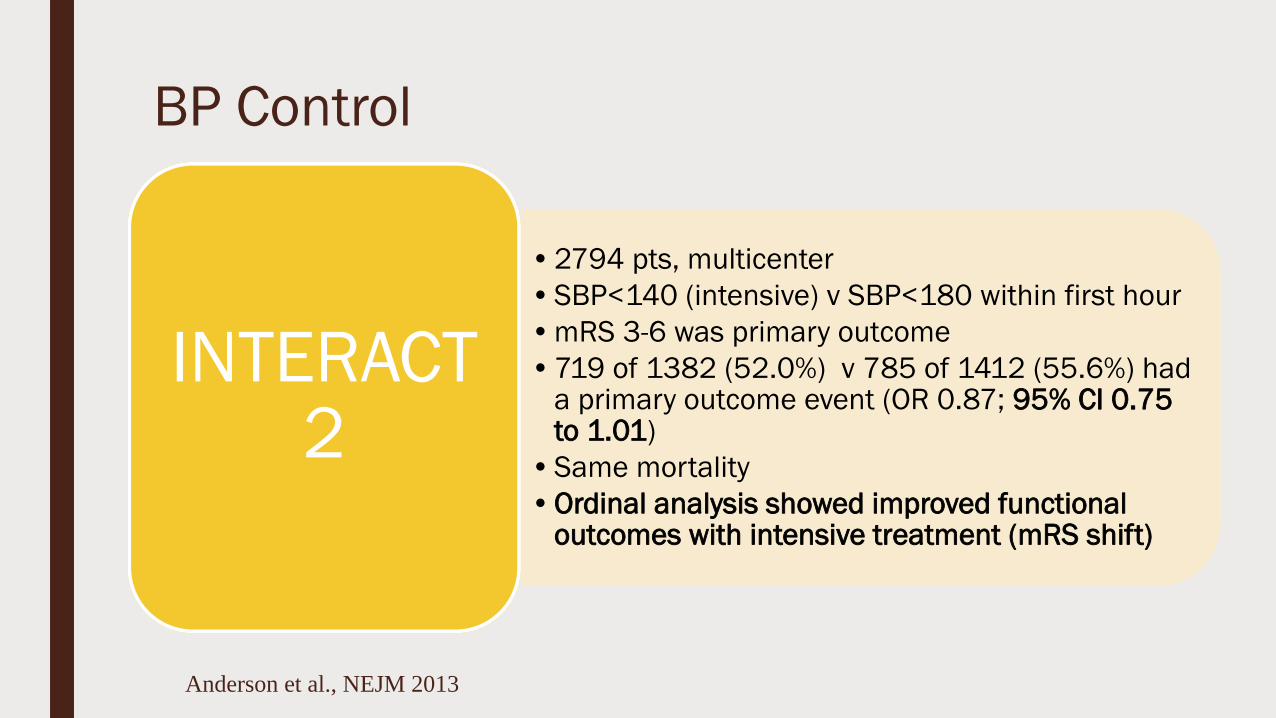
Anderson et al., NEJM 2013
BP Control
•2794 pts, multicenter
•SBP<140 (intensive) v SBP<180 within first hour
•mRS 3-6 was primary outcome
•719 of 1382 (52.0%) v 785 of 1412 (55.6%) had a primary outcome event (OR 0.87; 95% CI 0.75 to 1.01)
•Same mortality
•Ordinal analysis showed improved functional outcomes with intensive treatment (mRS shift)
INTERACT 2
Anderson et al., NEJM 2013
BP Control
Qureshi et al., NEJM 2016

BP Control
•1000 pts, multicenter, GCS >4
•SBP<140 (intensive) v SBP<180 within 4.5 hours of symptom onset with IV nicardipine
•mRS 4-6 was primary outcome
•38.7% (186 of 481) v 37.7% (181 of 480), RR 1.04; 95% CI 0.85 to 1.27
•More renal adverse events in intensive group (9.0% vs. 4.0%, P=0.002)
ATACH 2
Qureshi et al., NEJM 2016

The Devil in the Details

Blood Pressure Variability (BPV)
■ Failure of two RCTs to answer the
question
■ The question was maybe too simple
■ FAST-MAG trial
INCREASED VARIABILITY
F
A
v
O
R
A
B
L
E
O
U
T
O
C
M
E

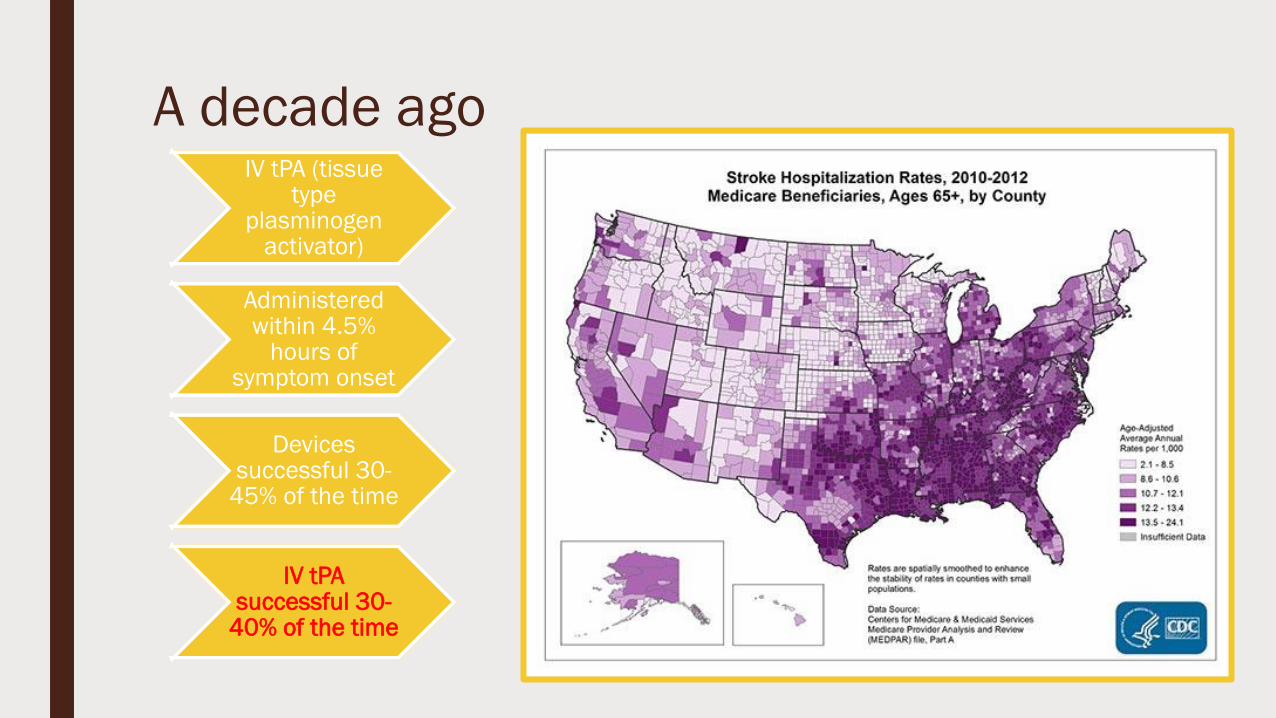
A decade agoIV tPA (tissue
type plasminogen
activator)
Administered within 4.5%
hours of symptom onset
Devices successful 30-
45% of the time
IV tPAsuccessful 30-
40% of the time

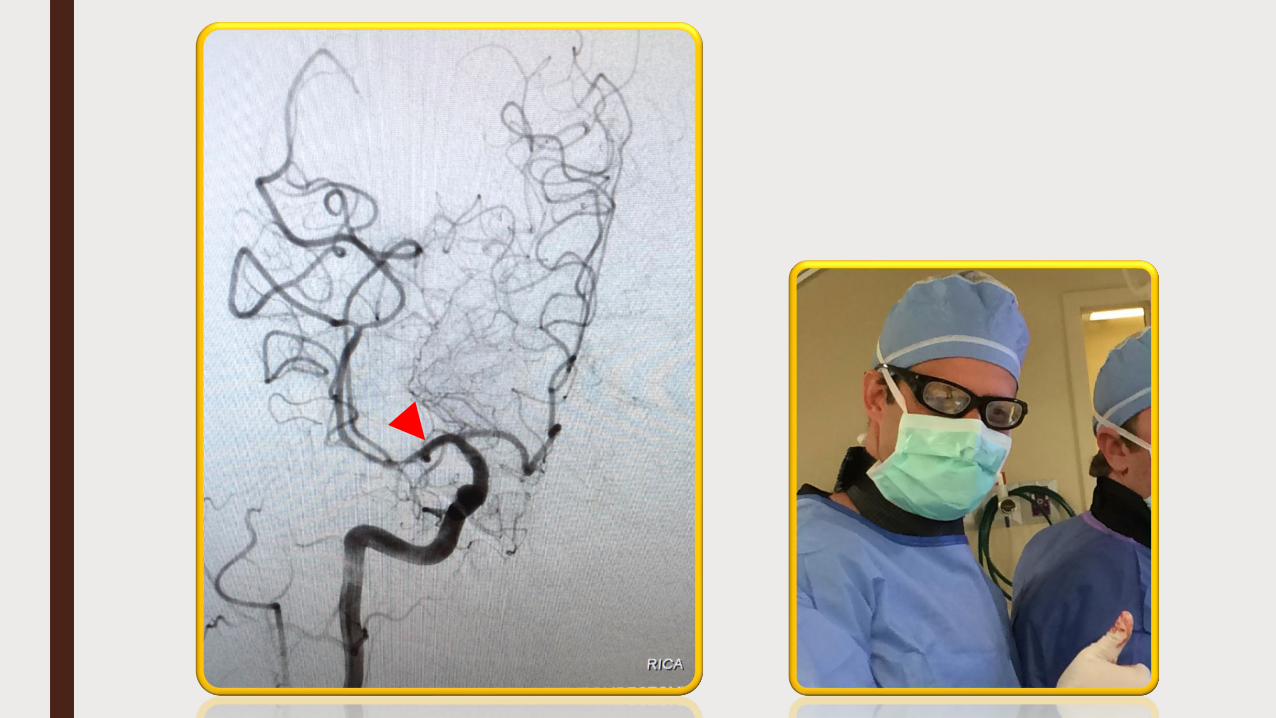
49 yo M, Pre-stoke mRS 0, LKN 3h, ASPECTS 8
0
10
20
30
40
50
60
70
80
90
100
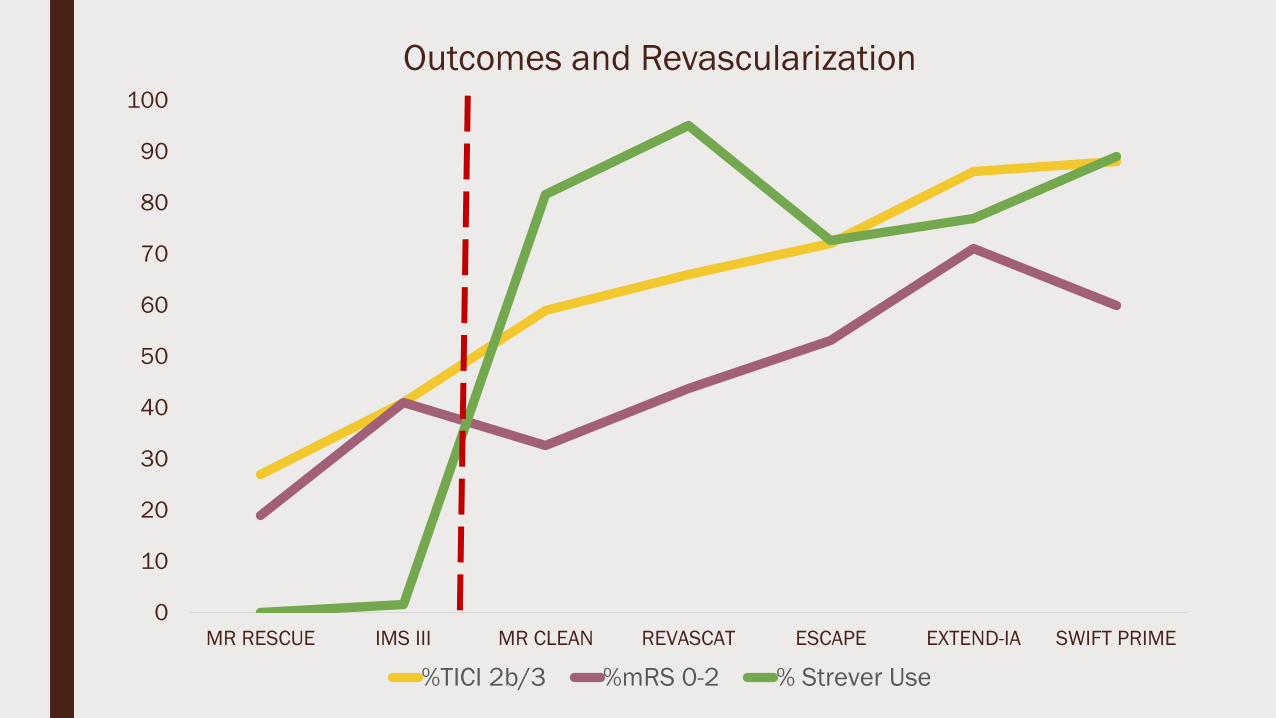
MR RESCUE IMS III MR CLEAN REVASCAT ESCAPE EXTEND-IA SWIFT PRIME
Outcomes and Revascularization
%TICI 2b/3 %mRS 0-2 % Strever Use

BP Control
■ 217 acute ischemic patients with LVO, retrospective analysis
Goyal et al. Neurology 2017
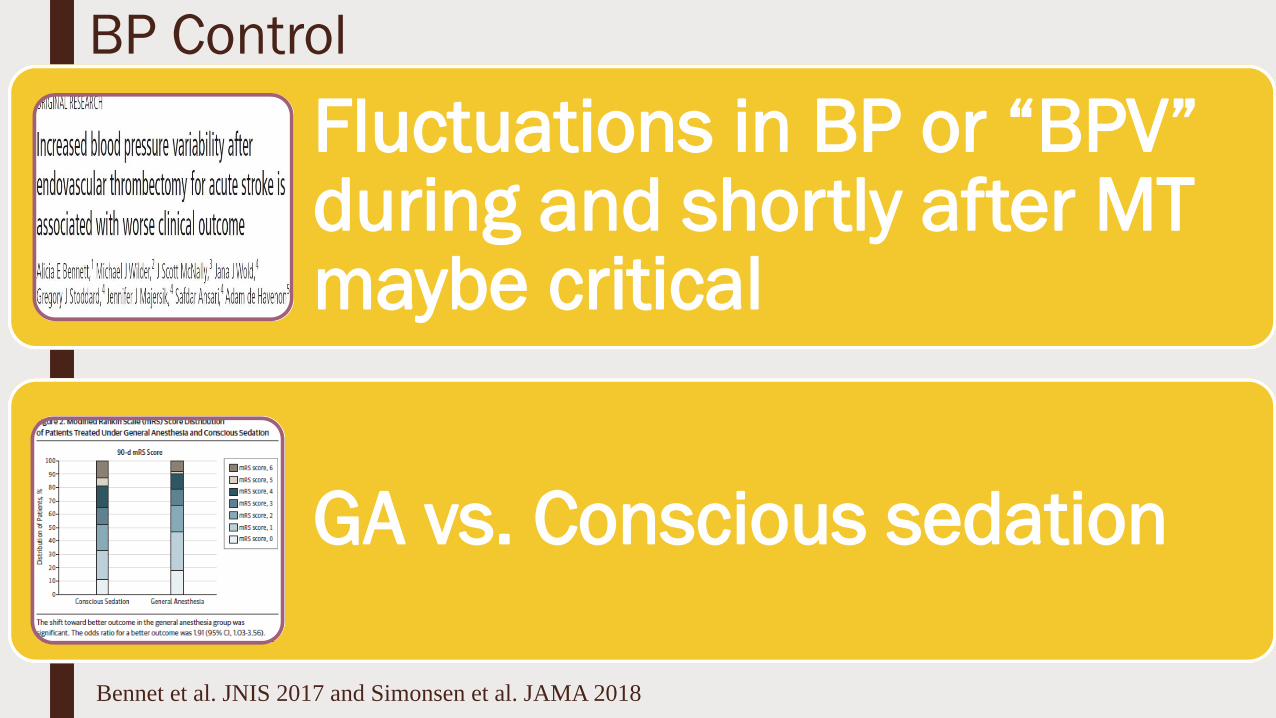
BP Control
Fluctuations in BP or “BPV” during and shortly after MT maybe critical
GA vs. Conscious sedation
Bennet et al. JNIS 2017 and Simonsen et al. JAMA 2018

Future Directions: Transcranial Doppler Monitoring
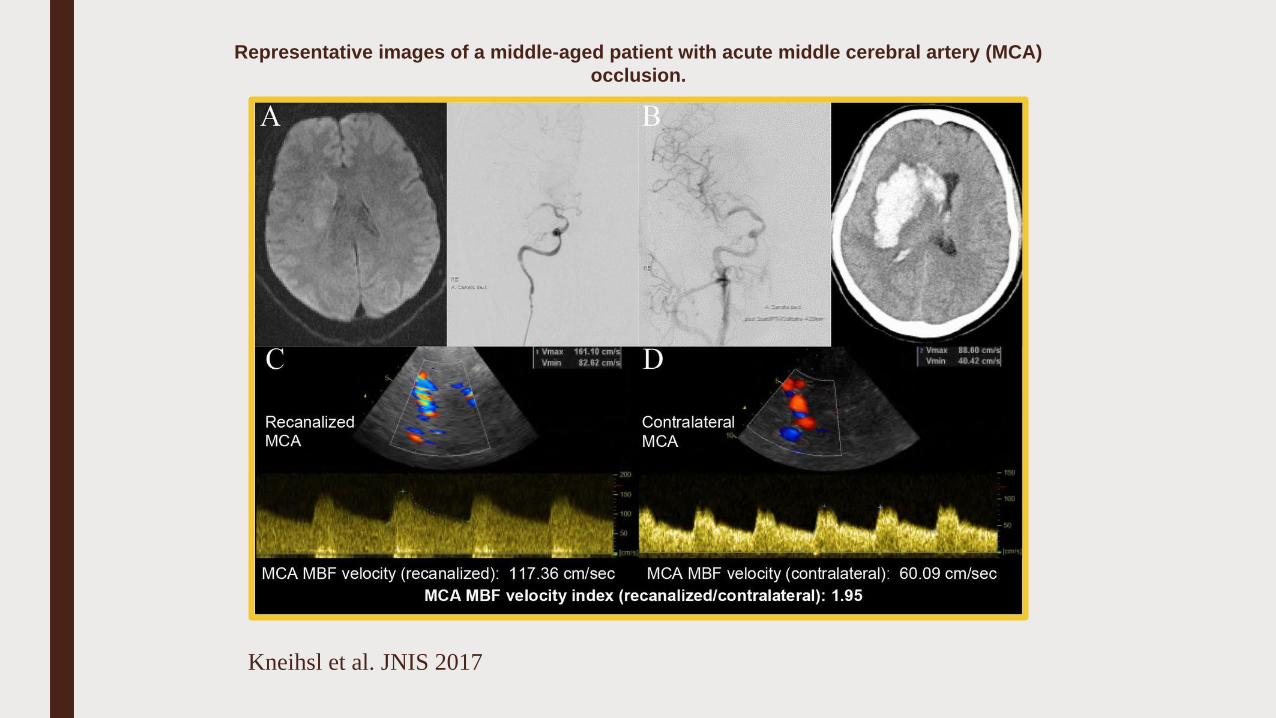
Representative images of a middle-aged patient with acute middle cerebral artery (MCA)
occlusion.
Kneihsl et al. JNIS 2017
BP control
■ What’s next?





























