Embed Size (px)
Citation preview

Breast Cancer Research and Treatment55: 223–229, 1999.© 1999Kluwer Academic Publishers. Printed in the Netherlands.
Report
Mechanism of captopril toxicity to a human mammary ductal carcinomacell line in the presence of copper
William Small, Jr.1,3, Agostino Molteni2,4, Yoon T. Kim1,5, Joann M. Taylor1, Chung-hsinTs’ao2, and William F. Ward11Department of Radiology,2Department of Pathology, and3Robert H. Lurie Comprehensive Cancer Center, North-western University Medical School, Chicago, USA;4Department of Pathology, University of Missouri MedicalCenter, Kansas City, USA;5Resurrection Medical Center, Chicago, USA
Key words:captopril, catalase, copper, hydrogen peroxide, mammary carcinoma cells
Summary
Captopril (D-3-mercapto-2-methylpropanoyl-L-proline) is an angiotensin converting enzyme (ACE) inhibitor, usedwidely in the treatment of hypertension and congestive heart failure. Captopril also inhibits proliferation of a varietyof cell types, including several lacking ACE and renin acitvity. We have previously demonstrated that humanmammary ductal carcinoma cells are among the cell types whose mitotic activity is inhibited by captopril. Inthose cells, captopril also reduces estrogen receptor (ER) and increases progesterone receptor (PR) concentrations.The present study evaluated the mechanism of captopril’s antiproliferative action in an ER/PR-negative humanmammary ductal carcinoma cell line, Hs578T. Cells grown in a 10% serum medium showed negligible changesin the presence of captopril alone. However, in the presence of subphysiologic concentrations of copper saltsor copper-loaded ceruloplasmin, captopril caused a dose-dependent reduction in cell number, thymidine incor-poration and mitochondrial dehydrogenase activity. In contrast, iron salts and iron-saturated transferrin had noeffect on captopril activity. Catalase and horseradish peroxidase nullified the cytotoxic effects of captopril/Cu++,whereas H2O2 mimicked those effects. These data are consistent with the notion of a copper-catalyzed oxidationof captopril, leading to the generation of H2O2 as the cytotoxin to this clinically important cell type.
Introduction
Captopril (D-3-mercapto-2-methylpropanoyl-L-proline) is an orally active competitive inhibitor of an-giotensin converting enzyme (ACE), the dipeptidasethat converts angiotensin I to the active vasocon-strictor angiotensin II and inactivates the bradykinins[1]. Captopril is prescribed to 5–10 million people inthe management of hypertension and congestive heartfailure [2, 3]. Captopril also reduces morbidity andmortality due to left ventricular dysfunction follow-ing myocardial infarction [4], and is effective againstdiabetic microangiopathy in kidney [5] and retina [6].Captopril has been found to inhibit mitosis in a vari-ety of cell types including canine renal epithelial cells[7], human neuroblastoma cells [8], human lung fibro-blasts [9], hamster pancreatic carcinoma cells [10],
and a cell line derived from a human salivary glandcarcinoma [11].
We have recently demonstrated that a line of hu-man mammary ductal carcinoma cells is among thecell types whose mitotic activity is inhibited by capto-pril [12]. In those cells, captopril inhibited thymidineincorporation as well as RNA and protein synthesis,without increasing release of prelabeled51Cr. Thedrug also caused a decrease in estrogen receptor (ER)and an increase progesterone receptor (PR) concen-trations. The mechanisms via which these changeswere brought about by captopril remain poorly un-derstood. Further, a line of human ER/PR-negativemammary ductal carcinoma cells are quite resistant tothe drug, except when copper is present. In the presentstudy we investigated the mechanism of the effect ofcaptopril/Cu++ on this line of cells. Lisinopril, a non-

224 W Small, Jr. et al.
thiol angiotensin converting enzyme (ACE) inhibitor,and penicillamine, a thiol compound with virtually noACE inhibitory activity, were co-tested with captopril.
Materials and methods
Cell culture
Hs578T human mammary ductal carcinoma cells, anestrogen and progesterone receptor-negative (ER−/PR−) cell line, were purchased from AmericanType Culture Collection (Rockville, MD). Cellswere grown in Dulbecco’s Modified Eagle’s Me-dium containing 10% newborn bovine serum (Gibco,Grand Island, NY), supplemented with penicillin G(100 U/ml), streptomycin (0.1 mg/ml), amphotericinB (0.25µg/ml), and insulin (0.2 U/ml), under 5%CO2 – 95% air in a humidified incubator at 37±0.1◦C. Captopril was generously provided by Bris-tol Myers-Squibb, Princeton, NJ; and lisinopril, byMerck Research Laboratories, West Point, PA. Allother chemicals were purchased from Sigma ChemicalCo. (St. Louis, MO).
Experimental design
Hs578T cells were incubated for 48 h with captopril,lisinopril or penicillamine (up to 500µM) alone, orin the presence of one of the following compounds:CuCl2(up to 0.5µg/ml), CuSO4 (up to 0.5µg/ml),copper-loaded ceruloplasmin (20 U/ml), FeCl2(up to0.5µg/ml), FeCl3 (up to 0.5µg/ml), or iron-loadedtransferrin (40µg/ml). The doses of copper-loadedceruloplasmin and iron-loaded transferrin were chosenfor their binding of 0.5µg or more of copper or iron,respectively. In other experiments, horseradish perox-idase (300 U/ml) or catalase (150 U/ml) was includedin the trials. Because prolonged exposure to catalasewould lead to cell injury, the incubation period of ex-periments involving use of catalase was 1 h instead of48 h. After removal of captopril/Cu++ and catalase,the cells were further incubated in plain medium foranother 47 h. Finally, the effect of captopril on thecells was compared with that by hydrogen peroxide(10−6 to 10−4 M). Three end-point assays were ap-plied to assess the effects of those compounds onHs578T cells.
Cell count
Approximately 20,000 cells in 1.0 ml culture mediumwere seeded into each well of a 24-well incubationplate. After a 24-hr attachment period, the mediumwas replaced with 1.0 ml of test medium. Cells wereincubated for an additional 48 h, and then harvestedby trypsinization. Trypsinized cells were resuspendedin isotonic saline, and counted with a Coulter ModelZM counter (Coulter Electronics, Hialeah, FL).
[3H]thymidine incorporation
Approximately 5000 cells were seeded into eachwell of a 24-well incubation plate. After a 24-hrattachment period, the plain culture medium was re-placed with 1.0 ml of test medium containing 0.5µCiof [3H]thymidine (87 Ci/mM; Amersham, ArlingtonHeights, IL). Cells were incubated for an additional48 h. The culture medium then was removed, and thecells were washed twice with Dulbecco’s phosphatebuffered saline (Gibco, Grand Island, NY). They werethen rinsed three times with 10% cold (4◦C) trichloro-acetic acid (TCA), with the final rinse lasting 10 min.The cells were air-dried, followed by the addition of0.5 ml of 1.0 N NaOH to each well. The samples wereleft in NaOH at room temperature for 16–20h beforethe alkali was neutralized with 0.5 ml of 1.0 N aceticacid. The samples were transferred to vials containing5 ml of liquid scintillation cocktail. Radioactivity inthe vial was counted in a liquid scintillation counterfor 5 min. Data were expressed as counts per minute(CPM) minus background.
Mitochondrial dehydrogenase activity (MTT assay)
Approximately 5000 cells in 0.1 ml of culture mediumwere seeded in each well of a 96-well culture plate,and allowed to attach for 24 h. The medium then wasreplaced with test medium, and the cells were incub-ated for an additional 48 h. At the end of the incubationperiod, 10µl of MTT reagent (3-[4,5-dimethylthiazol-2-yl]-2,5-diphenyl tetrazolium bromide; BoehringerMannheim, Indianapolis, IN) was added to each well.The cells were incubated for 4 h, followed by the addi-tion of 100µl of the solubilization solution (0.01 Msodium dodecylsulfate, 10% in HCl) to each well.The plates were placed in the incubator for 18 h, andthen read at 550 nm with an ELISA reader. Data wereexpressed as OD550 per well.

Mechanism of Captopril Cytotoxicity 225
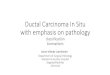
Figure 1. Cytotoxicity of human mammary ductal carcinoma cells exposed to various concentrations of captopril in the presence of 0.5µg/mlCuCl2. Mean± SEM;n = 6–10. Left panel= cell count; Middle panel = thymidine incorporation; Right panel = mitochondrial dehydrogenaseactivity. Con= control, no CuCl2 added.
Statistical analysis
Data were subjected to analysis of variance, and thesignificance of difference between group means wasdetermined by the Newman–Keuls test [13]. Data areexpressed as the mean± one standard error of themean (SEM).
Results
Effect of captopril, lisinopril, penicillamine onHs578T cells: role of copper
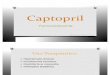
Captopril alone up to 500µM had no measurableeffect on cell count, thymidine incorporation or mi-tochondrial dehydrogenase activity in Hs578T cells.In the presence of a given concentration of CuCl2,captopril caused a dose-dependent injury to Hs578Tcells (Figure 1). Such a toxic effect of captopril wasnot observed when CuCl2 was substituted with FeCl2(Figure 2). Depending on the concentration of capto-pril tested, cytotoxic effect could be detected with aslittle as 0.1µg/ml CuCl2, reaching maximum cytotox-icity at 0.5µg/ml (Table 1). CuSO4 was as effectiveas CuCl2, but FeCl3 was as ineffective as FeCl2 (datanot shown). Further, the cytotoxic effect of captoprilwas evident with copper-loaded ceruloplasmin, but notwith iron-loaded transferrin (Figure 3). Neither lisino-pril nor penicillamine caused injury to the cell in the
absence or presence of any of the cation salts includingCuCl2 (Table 2).
Inclusion of either catalase or horseradish perox-idase in the culture medium completely preventedthe cytotoxic effect of captopril/Cu++ (Figure 4).Catalase and horseradish peroxidase themselves alonehad no significant effect on thymidine incorporation inHs578T cells.
Effect of hydrogen peroxide on Hs578T cells
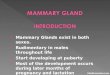
H2O2 caused similar injury to the Hs578T cellsas did captopril/Cu++. In fact, the dose-dependentcurves of direct exposure to H2O2 paralleled those ofCaptopril/Cu++ in the inhibition of cell proliferation,thymidine incorporation and mitochondrial dyhydro-genase activity as expressed in percent changes fromcontrol, as a function of log concentrations of H2O2 orcaptopril (Figure 5). It should be noted that H2O2 was5–10 times more toxic to the cell than captopril/Cu++on an equal molar basis.
Discussion
We have shown that in the presence of subphysiologicconcentrations of CuCl2, the ACE inhibitor captoprilinhibits proliferation, thymidine incorporation and mi-tochondrial dehydrogenase activity of Hs578T humanmammary ductal carcinoma cells in culture. The injuryto the cells by captopril/Cu++ appears to occur within

226 W Small, Jr. et al.
Figure 2. Mitochondrial dehydrogenase activity of human mammary ductal carcinoma cells incubated with captopril (200µM) in the presenceof CuCl2 or FeCl2 (both 0.5µg/ml). Captopril alone caused a non-statistically significant reduction of dehydrogenase activity. In the presenceof CuCl2, but not FeCl2, the reduction of enzyme activity was significant. CuCl2 and FeCl2 themselves had no effect on the enzyme activity.Mean± SEM;n = 6–10.∗ indicates significantly different(P < 0.05) from control.
Table 1. Mitochondrial dehydrogenase activity of Hs578T cellsincubated with captopril or CuCl2 or both
CuCl2 (µg/ml) Captopril (µM)
0 200 500
0 0.77± 0.02 0.73± 0.01 0.78± 0.02
0.1 – – 0.68± 0.02∗0.25 0.76± 0.01 0.56± 0.03∗ –
0.5 0.75± 0.01 0.45± 0.02∗ 0.14± 0.02∗1.0 0.77± 0.01 0.44± 0.01∗ –
1.5 0.77± 0.03 0.44± 0.01∗ –
2.0 0.78± 0.01 0.44± 0.01∗ –
∗Different from control (0µg/ml); P < 0.05.Mean± SEM;n = 4–8.
1 h and persists for at least 48 h. Copper salts havebeen reported previously to increase the antimitoticactivity of captopril and penicillamine to hematopoi-etic cells in culture [14–16]. In the present study, wedemonstrated a similar effect of captopril/CuCl2, butnot penicillamine/CuCl2, on a solid tumor cell line,and copper bound to ceruloplasmin appeared equallyeffective.
The mechanism of the cytostatic activity of capto-pril is poorly understood. One possible pathway isthrough the inhibition of angiotensin II synthesis. An-giotensin II is a potent mitogen and induces neovas-cularization in several experimental models [17–20].However, two other ACE inhibitors, lisinopril andenalaprial, with comparable angiotensin II synthesisinhibiting activity and differing from captopril by not
Figure 3. Mitochondrial dehydrogenase activity of Hs578T cellsexposed to various concentrations of captopril in the presenceof either 20 units/ml of copper-loaded ceruloplasmin (Ceru) or40µg/ml iron-loaded transferrin (Tran). Con= control, no cerulo-plasmin or transferrin added. Mean± SEM;n =6–10.
having sulfydril groups, are much less potent in inhib-iting cell proliferation than captopril [9, 10, 12, 20].Further, some cell types upon which captopril exertsa cytostatic effect lack ACE and renin activity, sug-gesting that the cytostatic action of captopril may beindependent of the renin-angiotensin system.

Mechanism of Captopril Cytotoxicity 227
Table 2. Mitochondrial dehydrogenase activity of Hs578T cellsexposed to various concentrations of captopril, lisinopril or peni-cillamine in the presence of 0.5µg/ml of CuCl2 in the culturemedium
Compounds Control CuCl2
(µM) medium (0.5µg/ml)
Captopril
0 0.68± 0.01 0.69± 0.01
100 0.70± 0.02 0.45± 0.02∗200 0.72± 0.03 0.46± 0.01∗500 0.68± 0.01 0.24± 0.01∗
Lisinopril
0 0.78± 0.01 0.64± 0.01
100 0.69± 0.01 0.70± 0.02
200 0.69± 0.02 0.71± 0.01
500 0.69± 0.02 0.74± 0.01
Penicillamine
0 0.75± 0.01 0.66± 0.02
100 0.70± 0.01 0.67± 0.01
200 0.70± 0.01 0.63± 0.01
500 0.69± 0.01 0.69± 0.01
∗Different from control (0µM); P < 0.05.Mean± SEM;n = 4–8.
The finding of injury of Hs578T cells bycaptopril/Cu++ in the present study suggests a copper-catalyzed oxidation of captopril being the causativefactor. The observations that peroxidase and catalasehave prevented the cytotoxicity of captopril/Cu++,whereas H2O2 mimicked that toxicity, are consistentwith the notion. H2O2 generation has been speculated
Figure 4.Prevention of captopril/Cu++ -induced reduction of thymidine incorporation in Hs578T cells by catalase (150 U/ml) and horseradishperoxidase (300 U/ml). Mean± SEM; n = 6–10 wells per group.∗ indicates significantly(P < 0.05) different from control. Cat= catalase;HRPO= horseradish peroxidase.
as the causative agent that inhibits granulocyte pro-liferation by penicillamine [15]. The oxidation re-action of captopril appears to be specific for cop-per, since neither FeCl2 nor iron-saturated transferrincould substitute copper in bringing about toxicity tothe tumor cells by the ACE inhibitor. Thiol-containingcompounds such as captopril are known to undergocopper-catalyzed oxidation reactions that consume su-peroxide radicals and generate hydrogen peroxide[22]. Interestingly, captopril-copper and captopril-ironcomplexes have been reported to exhibit superoxidedismutase (SOD)-like activity [22–24], as would beexpected if oxidation of the drug consumes superoxideradicals. Captopril frequently is described as possess-ing antioxidant activity [25–29]. Nevertheless whencomplexed with divalent cations, captopril also canexhibit pro-oxidant actions [30, 31]. Thus the relat-ive activities of catalase, peroxidase and SOD withina particular cell type may influence the net biolo-gical consequence of the captopril oxidation mech-anism. Cells with high catalase and peroxidase andlow SOD activities may be less deleteriously impactedby captopril oxidation than are cells with the oppos-ite enzyme profile. In our studies, we found that theestrogen/progesterone receptor-negative Hs578T cellsare quite resistant to captopril as compared to the hor-mone receptor-positive T47-D ductal carcinoma cells[12]. The fact that exogenous catalase and peroxidaseprotect against the cytotoxicity of captopril/Cu++ alsosuggests that extracellular events might influence thispathology.
It is not clear from the present data whether H2O2is indeed the active cytotoxin, or is the precursor of

228 W Small, Jr. et al.
Figure 5. Cell count (left), thymidine incorporation (middle) and mitochondrial dehydrogenase activity (right) of Hs578T cells exposed tovarious concentrations of H2O2 or captopril in the presence of CuCl2 (0.5µg/ml). Mean± SEM;n = 12–16.
hydroxyl radicals (OH−) via metal-catalyzed Fentonreactions [21]. Fe2+ is an important although not ex-clusive catalyst of the Fenton reaction, but FeCl2 doesnot appear to have an effect on captopril toxicity. Fur-thermore, captopril itself is a potent scavenger of OH−[32–34], and does not react well with H2O2 [20]. Thestriking similarity in the shape of Captopril/Cu andH2O2 dose-response curves further indirectly arguesin favor of hydrogen peroxide being the active agent.
In conclusion, the present study clarifies the mech-anism of captopril cytotoxicity in a human mammaryductal carcinoma cell line, and implicates a copper-catalyzed, H2O2-mediated pathway. In this case thethiol group rather than ACE inhibition would appearto be the basis of captopril’s activity. Negative resultswith lisinopril support this hypothesis. However, theinactivity of penicillamine indicates that captopril’s ef-ficacy is not shared by all thiols. These data, and therecently reported angiostatic activity of captopril [20],identify novel and potentially important actions of acommon cardiovascular drug in oncology.
Acknowledgement
This study was supported in part by the Park RidgeHealth Foundation, Park Ridge, IL.
References
1. Migdalof BH, Antonaccio MJ, McKinstry DN, Singhvi SM,Lan SJ, Egli P, Kripalani KJ: Captopril: Pharmacology, meta-bolism, and disposition. Drug Metab Rev 15: 841–869, 1984
2. Burris JF: The expanding role of angiotensin converting en-zyme inhibitors in the management of hypertension. J ClinPharmacol 35: 337–342, 1995
3. Garg R, Yusef S (for the Collaborative Group on ACE In-hibitor Trials): Overview of randomized trials of angiotensin-converting enzyme inhibitors on mortality and morbidity inpatients with heart failure. JAMA 273: 1450–1456, 1995
4. Pfeffer MA, Braunwald E, Moye LA et al.: Effect of captoprilon mortality and morbidity in patients with left ventriculardysfunction after myocardial infarction. N Engl J Med 327:669–677, 1992
5. Lewis EJ, Hunsicker LG, Bain RP, Rohde RD: The effect ofangiotensin-converting-enzyme inhibition on diabetic nephro-pathy. N Engl J Med 329: 1456–1462, 1993
6. Jackson WE, Holmes DL, Garg SK, Harris S, Chase HP:Angiotensin-converting enzyme inhibitor therapy and diabeticretinopathy. Ann Opthalmol 24: 99–103, 1992
7. Bauer HA, Lametschwandtner A, Steiner M, Bauer HC: In-fluence of angiotensin converting enzyme inhibitor (captopril)on kidney epithelial cellsin vitro: Studies on potassium (86Rb)influx and cellular proliferation. Clin Chim Acta 187: 47–54,1990.
8. Chen L, Re RN, Prakash O, Mondal D: Angiotensin-converting enzyme inhibition reduces neuroblastoma cellgrowth rate. Proc Soc Exp Biol Med 196: 280–283, 1991
9. Nguyen L, Ward WF, Ts’ao C, Molteni A: Captopril inhibitsproliferation of human lung fibroblasts in culture: A potentialantifibrotic mechanism. Proc Soc Exp Biol Med 205: 80–84,1994
10. Reddy MK, Baskaran K, Molteni A: Inhibitors of angiotensinconverting enzyme modulate mitosis and gene expression inpancreatic cancer cells. Proc Soc Exp Biol Med 210: 221–226,1995
11. Nittler T, Stone M, Shroff O, McAuthur C, Veno P, Dobbs L,Brizio-Molteni L, Molteni A: Effect of captopril on the pro-liferation of a human salivary gland adenocarcinoma cell line(Abstract). FASEB 12: A811, 1998
12. Small Jr. W, Molteni A, Kim YT, Taylor JM, Chen Z, WardWF: Captopril modulates hormone receptor concentration andinhibits proliferation of human mammary ductal carcinomacells in culture. Breast Cancer Res Treat 44: 217–224, 1997
13. Zar JH: Biostatistical Analysis. Prentice-Hall, EnglewoodCliffs, NJ, 1974, pp 121–181
14. Lipsky PE, Ziff M: The effect of D-penicillamine on mitogen-induced human lymphocyte proliferation: Synergistic inhib-ition by D-penicillamine and copper salts. J Immunol 120:1006–1013, 1978.
15. Hammond WP, Miller JE, Starkebaum G, Zweernick HJ,Rosenthal AS, Dale DC: Suppression ofin vitro granulo-cytopoiesis by captopril and penicillamine. Exp Hematol 16:674–680, 1988
16. Held KD, Biaglow JE: Mechanisms for the oxygen radical-mediated toxicity of various thiol-containing compounds incultured mammalian cells. Radiat Res 139: 15–23, 1994

Mechanism of Captopril Cytotoxicity 229
17. Fernandex LA, Twickler J, Mead A: Neovascularization pro-duced by angiotensin 2. J Lab Clin Med 105: 141–145,1985
18. LaNoble FAC, Schreurs NHJS, Van Straaten JFM, Rogg H,Strijker-Boudier HA: Evidence for a novel angiotensin II re-ceptor involved in chick embryo chorionallantoic membrane.Am J Physiol 246: R460–R463, 1993
19. Hernandex I, Cowley AW, Lanbard JH, Greene AS: Salt intakeand angiotenin II alter microvessel density in the cremastermuscle of normal rats. Am J Phsyiol 263: H8664–H8667,1992, 1996
20. Volpert OV, Ward WF, Lingen MW, Chesler L, Solt DB,Johnson MD, Molteni A, Polverini PJ, Bouck NP: Captoprilinhibits angiogenesis and slows the growth of experimentaltumors in rats. J Clin Invest 98: 671–679, 1996
21. Roberts NA, Robinson PA: Copper chelates of antirheumaticand anti-inflammatory agents: Their superoxide dismutase-like activity and stability. Br J Rheumatol 24: 128–136,1985
22. Reguli J, Misik V: Superoxide scavenging by thiol/coppercomplex of captopril – an EPR spectroscopy study. FreeRadical Res 22: 123–130, 1995
23. Jay D, Cuella A, Jay E: Superoxide dismutase activity of thecaptopril-iron complex. Mol Cell Biochem 146: 45–47, 1995
24. Keidar S, Kaplan M, Shapira C, Brook JG, Aviram M:Low density lipoprotein isolated from patients with essen-tial hypertension exhibits increased propensity for oxidationand enhanced uptake by macrophages: A possible role forangiotensin II. Atherosclerosis 107: 71–84, 1994
25. Clearfield MB, Lee N, Armstrong L, DeFazio P, KudchodkarBJ, Lacko AG: The effect of captopril on the oxidation ofplasma lipoproteins. Pharmacol Toxicol 75: 218–221, 1994
26. Zieden B, Wuttge DM, Karlberg BE, Olsson AG: Effects ofin vitro addition of captopril on copper-induced low densitylipoprotein oxidation. Br J Clin Pharmacol 39: 201–203, 1995
27. de Cavanagh EM, Inserra F, Ferder L, Romano L, Ercole L,Fraga CG: Superoxide dismutase and glutathione peroxidaseactivities are increased by enalapril and captopril in mouseliver. FEBS Lett 36: 22–24, 1995
28. Sogaard P, Klausen IC, Rungby J, Faergeman O, Thygesen K:Lipoprotein(a) and oxygen free radicals in survivors of acutemyocardial infarction: Effects of captopril. Cardiology 87: 18–22, 1996
29. Lapenna D, DeGioia S, Mezzetti A, Ciofani G, Di Ilio C,Cuccurullo F: The prooxidant properties of captopril. BiochemPharmacol 50: 27–32, 1995
30. Clapperton M, Beswick PH, Abdullah I, Dargie HJ, Fisher AC,McMurray J: Effect of captopril, enalaprilat and mercaptop-ropionyl glycine (MPG) on the oxidative activity of humanisolated neutrophils. Br J Clin Pharmacol 40: 31–35, 1995
31. Bagchi D, Prasad R, Das DK: Direct scavenging of free rad-icals by captopril, an angiotensin converting enzyme inhibitor.Biochem Biophys Res Comm 158: 52–57, 1989
32. Chopra M, Scott N, McMurray J, McLay J, Bridges A, SmithWE, Belch JJF: Captopril: A free radical scavenger. Br J ClinPharmacol 27: 396–399, 1989
33. Mak IT, Freedman AM, Dickens BF, Weglicki WB: Protectiveeffects of sulfhydryl-containing angiotensin converting en-zyme inhibitors against free radical injury in endothelial cells.Biochem Pharmacol 40: 2169–2175, 1990
34. Aruoma OI, Akanmu D, Cecchini R, Halliwell B: Evaluationof the ability of the angiotensin-converting enzyme inhibitorcaptopril to scavenge reactive oxygen species. Chem-BiolInteractions 77: 303–314, 1991
Address for offprints and correspondence:William Small, Jr., Ra-diation Oncology Center, Northwestern Memorial Hospital, 250E. Superior Street, Wesley B-44, Chicago, IL 60611, USA;Tel:312-908-2520;Fax: 312-503-8521