-
7/28/2019 Measurements of Leukotrienes in the Urine- Kumlin
1/13
Review article
Measurements of leukotrienes in the urine:strategies and
applicationsKumlin M. Measurements of leukotrienand
applieations.Allergy 1997: 52: J24-135. Munksga
iene biosynthesor antagonis ts ; i
Karolinska Ir ist i tutS-171 77 S tockhoirSw eden
The biologic actions of the leukotrienes (LTs) C4,D4, and E4,
collectively referred to as the cysteinyl-eontaining leukotrienes,
support their putative roleas mediators of bronchial asthma (1, 2).
Thus, theyall provoke plasma exudation, constriction of bron-chial
smooth muscle, and increased mucus secre-tion in the airways (3-5).
In addition, asthmaticsubjects show bronchial hyperresponsiveness
tocysteinyl-leukotrienes (6,7), and these leukotrienesmay also
enhance airway reactivity to histamine inpatients with asthma (8-1
0). Furthertnore , aspirin-intolerant asthmatics, i.e., asthmatic
patients inwhom bronchoeonstriction is elicited by aspirin orother
nonsteroidal anti-inflatnmatory drugs, werefound to be
hyperresponsive to LTE4 (11), whereastheir reactivity to LTC4 and
histamine was notdifferent from other asthmatics (12). D
esensitiza-tion with aspirin attenuated the airway response toLTE4,
whereas histamine sensitivity remained un-altered (If). It has also
been shown both in vitro(13) and in vivo in asthmatics (14) that
cysteinyl-leukotrienes are chemotactic toward
eosinophilicgranulocytes, suggesting that they contribu te to
therecruitment of eosinophils into the airways duringasthtnatic
responses.Cysteinyl-leukotrienes are formed in the human
specimens from asthmatic subjects (17). Morerecently,//I vivo
formation of cysteinyl-leukotrieneshas been documented in
association with allergen-induced airway obstruction (18-20). A
number ofantileukotriene drugs, which block cither the for-mation
(biosynthesis inhibitors) or the biologicactions (receptor
antagonists) of the cysteinyl-leukotrienes, have proved beneficial
in attenuatingprovoeation-induced asthmatic reactions
(21-25).Clinical improvement of asthma has been docu-mented in a
long-term treatment study with abiosynthesis inhibitor on control
of clinical asthma(26). For evaluation of the effects of such
newantiasthmatic drugs and correlation of their effectswith the
release and action of leukotrienes, thereis a great need for safe
and reliable analyticprocedures to determine leukotriene formation
//;
To follow endogenous pulmonary production
ofcysteinyl-leukotrienes in association with airwayobstruction and
allergic responses in asthma, wehave developed methods for analysis
of LTE4 inthe urine (27). These tiiethods have been utilizedto
monitor excretion of cysteinyl-leukotrienes inhealthy subjeets and
patients suffering from differ-ent types of asthma, as well as in
association with
-
7/28/2019 Measurements of Leukotrienes in the Urine- Kumlin
2/13
M easurem ent of urinary LTE4and summarize applications of
activity originating from intravenously infused
ueh methods instudies of spontaneous or indueed [ 14,15-
-12]-LTC4. Thecause of this discrepancy issthma and theeffeets of
antileukotiiene drugs. not clear, but mayrelate to administration
of the
substrate via a bolus injection (42), as opposed to, . . , J ^.
* slow infusion (43,44), or the use of substrates withonitoring
endogenous production of ,adioactivity in different parts of the
moleeules.
cysteinyl-containing leukotrienes Nevertheless, asimilar
proportion, i.e., about 3-5%Several biologic fluids may cotne into
consideration of inhaled LTD4 (20, 46),2-6% of infused LTC4for
monitoring endogenous production of cysteinyl- (43, 44), and 7^8%
of injeeted LTE4 (45) wereleukotrienes. The release of mediators
into nasal recovered asintaet LTE4 in the urine. Tluis,
regard-secretions can be analyzed in nasal lavages after less of
isotope labeling and route of administration,antigen challenge (28,
29). Local production in the it appears that about 5% of
exogenously suppliedairways canalso beestimated bymeasuiements in
leukotrienes arerecovered as urinary LTE4.bronchial lavage fluid
(30-33), ormediator release More importantly, in none of these
studies wasin themueosa of the airways can be estimated by
LTC4orLTD4 recovered inthe urine, and A^-acetyl-analysis in
nasopharyngeal or traeheobronchial LTE4, the major metabolite in
rodents, was foundsecretions (34, 35). Monitoring circulating meta-
to be only a tninor tnetabolite in tnan (43-45).bolites in whole
blood or plasma is another After allergen-ehallenge. uiinary
16-carboxytetranoi-approach tomeasure in vivo production, but
circu- dihydro-LTE4 was detected by specific radioimmuno-lating
levels of LTE4 seem to be too low to be assay (RIA), but LTE4 was
still found to be thereliably detected (36, 37). However, all these
major urinary leukotriene derivative up to3 h afterstrategies may
encounter difficulty; e.g., irreproduei- theallergen-indueed airway
obstruction (48). Inte-ble sample collection and artifactual
formation of restingly, inhalation ofbronchoconstrictive doses
ofcompounds during sampling. Furthermore, inva- LTC4 or LTE4 in
asthmatics altered urinary excre-sive techniques arealways
associated with certain tion of LTE4 in a dose-dependent fashion
(47).risks and can be used to obtain only a relatively Again,
however, about 7% of inhaled LTC4waslimited number of samples.
Urine, on the other recovered asurinary LTE4 (47). Tliese data
stronglyhand, is a biologic fluid that is easy to eollect support
the use of urinary LTE4 as a marker ofwithout any significant risk
of artifactual c.\vivo leukotriene biosynthesis in the airways of
asthma-formation of metabolites. Thepattern of metabo- tics.
However, further studies are required tolites in urine probably
refleets a whole-body pro- eharacterize fully the //; vivo
metabolism of theduetion, with a fewexceptions where thekidney is
eysteinyl-leukotrienes in man.known to be a main producer of a
certain com- Maelouf et al. eoncluded from a study on thepound,
such as intact urinary prostaglandin (PG)E2 metabolism of LTC4 that
LTE4 is the best para-andTXB,. Production of the
eysteinyl-leukotrienes meter for short-time /// vivo release,
whereas theby thehuman kidney andurinary tract has not yet w- and
(3-oxidized metabolites may better reflectbeen eompletely
aseertained. Nevertheless, as indi- chronic changes in
cysteinyl-leukotriene productioncated below, urine has been found
useful for meas- (49). However, theusefulness of measurements
ofuring whole-body production of the cysteinyl- co- and |3-oxidized
metabolites ofLTE4 in theurineleukotrienes (18-20, 33, 38-41).
needs further evaluation. For example, we must
One important aspeet in the seleetion of com- discover whether
disease processes alter the nor-pounds tomeasure is knowledge of
the metabolism mal excretion pattern of the compounds. It hasof the
cysteinyl-leukotrienes. Metabolic studies been suggested that
allergen challenge of asthma-have shown that LTE4 is the end
metabolite of ties may affect thetransfer of formed
leukotrienes,cysteinyl-leukotrienes in human lung invitro (16).
leading to longer duration of elevated leukotrieneA few studies
have focused on the //; vivo metabolic levels in theairways (50), a
condition which, how-fate inman of LTC4, LTD4, or LTE4,
administered ever, was not reflected as altered urinary
excretion,intravenously (42-45) or byinhalation (46, 47), or At the
moment, the most important factors toendogenously formed after
allergen challenge (48). consider appear to be liver and kidney
diseases thatMost radioactivity administered was at all times
clearly alter the excretion of metabolites althoughrecovered in
urine and bile, although with //; i/vo produetion is unchanged (39,
51). Normalsomewhat different relative distributions. Orning
variations in diuresis are routinely corrected foret al.recovered
about 50% of administered radio- by expressing the results in
relation to urinaryactivity in urine after intravenous injection of
creatinine levels (27).[5,6,7,8,ll,12,14,15--^H,s]-LTC4(42),
whereas, in two Taken together, the results obtained to date
-
7/28/2019 Measurements of Leukotrienes in the Urine- Kumlin
3/13
cysteinyl-leukotrienes and thus appears to be thebest parameter
to select for analysis.Methods for analysis of nrinary LTE4For
several applications, including clinical trials ofnew
antileukotriene drugs, it is of the utmostimportance to have
sensitive, specific, and simplemethods for analysis of urinary
LTE4. Immuno-assays utilizing polyclonal or monoclonal,
virtuallyspecific, LTE4 antibodies, together with radioactivetracer
(RIA) or enzyme-linked tracer (enzymeimmunoassay; EIA) have so far
been used.However, though sensitive and relatively easy toperform,
immunoassays may have methodologicalproblems. For instance,
structurally similar com-pounds may cross-react with the antibody,
andsubstances in the biologic matrix may nonspecifi-cally interfere
with the antigen-antibody inter-action. Most data on immunoreactive
urinary LTE4have so far been generated with the combinationof
reversed-phase high-performance liquid chroma-tography (RP -HPL C)
and immunoassay, in attemptsto increase the specificity of the
assay (33, 38, 40,52).We have validated a simpler strategy using
EIAor RIA analysis of serially diluted, unextractedurine samples,
and compared the results withmeasurements of the same samples after
solid-phase extraction (SPE) and R P- H PL C separation.Fractions
at the retention time of authentic LTE4were assayed directly with
RIA (20, 27) with amouse monoclonal antibody directed against
LTD4with around 51% cross-reactivity to LTE4 (Adv.Magn. Inc.,
Boston, MA, U SA ). Alternatively, theLTE4 fractions were pooled,
evaporated, andassayed for content of LTE4 with EIA (27) with
arabbit polyclonal antiserum specific for LTE4 andacetylcholine
esterase-linked tracer (CaymanChemical Company, Ann Arbor, MI, US
A). Lossesduring purification were estimated by the use
oftritium-labeled leukotrienes. For RIA measure-ments, 'H-labeled
LTC4 was employed as internalstandard, whereas, in the case of EIA
analysis, thehomologous tracer ^H-labeled LTE4 could be
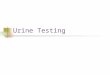
used.Considerable losses of leukotrienes during thepurification
were documented with the internalstandards (Fig. 1). However, there
was no signifi-cant difference between the recoveries of -
H-labeled LTC4 and ^H-labeled LTE4 in SPE andRP-H PLC (Fig. 1; 27).
The cross-reactivities of thedifferent antibodies were also
carefully determined(27).Comparisons were then made, on the one
hand,between analyses of unextracted samples with RIA
4 2 2 3 % 58+23%Fig. 1. Purification of urine samples. Results
obtained by EIAor RfA analysis of unpurified samples were compared
withmeasurements after two steps of purification.
Tritium-labeledleukotrienes (^H-labeled LT Q and ^H-labeled LTE4)
were usedas internal standards. Recoveries were measured after each
stepof purification. Results of immunoassay analyses were
finallyrecovery. Means SD.
immunoassays. More than 80 individual urine sam-ples were
analyzed with EIA and RIA in parallel.Although RIA analysis
consistently gave highervalues, which in part was due to the use of
a differentantibody, a very good correlation between theresults was
obtained (r^-0.81). Furthermore, in twosets of experiments,
analysis in unextracted andpurified samples was compared. First,
RIA measure-ments were applied on a total of more than 40samples
collected before and after bronchial provo-cation (23). Although
the average amounts of immu-noreactivity detected in the purified
samples weresomewhat lower than values obtained in
unpurifiedsamples, the differences did not reach
statisticalsignificance. Rather, a similar ratio bet-ween pre-and
postchallenge levels of urinary LTE4 wasobtained when analyzing
unpurified or purified sam-ples (23). Similar comparisons were
performed inanother study where a number of samples coUeetedhourly
during allergen provocation were analyzedwith EIA before and after
purification (27). Again,values obtained by analysis of
HPLC-fractions cor-responding to the retention time of LTE4 were at
alltime points somewhat lower than the valuesobtained by direct
analysis of unextracted samples.However, the difference between
baseline andpostchallenge samples were the same regardless
ofwhether or not the samples were purified (27).Furthermore, when a
larger number of urine sam-ples were analyzed before and after
purification andthe results were validated according to Bland
&Altman's measure of repeatability (53), there wasan excellent
correlation between results obtainedwith the different assay
procedures (27).
-
7/28/2019 Measurements of Leukotrienes in the Urine- Kumlin
4/13
addition of preservatives. For example, the influ-ence of an
antioxidant on the stability of LTE4 wasinvestigated with urine and
buffer samples spikedwith -^H-labeled LTE4. Samples were either
storedwithout additions or supplied with the
antioxidant4-hydroxy-TEMPO free radical to a final concen-tration
of 1 mM, and the pH was adjusted to 9 withNaOH before freezing.
Aliquots of the sampleswere withdrawn after t, 8, 30, and 60 days,
andrecovery of intact ''H-labeled LTE4 was determined.The stability
of LTE4 in urine at -20C was notimproved by addition of the
antioxidant and pHadjustment (27).One important aspect of urinary
ETE4 analysesis the procedure for collection of the urine
samples.We have found that the peak increase in urinaryETE4, as a
result of provoked release of leuko-trienes, generally is fairly
short-lasting (20, 23, 27).In order to trap such an instantaneous
release,collection of urine with short intervals is necessary.In
our bronchial provocation studies, we usedhourly collected samples.
If samples are collectedwith longer time intervals, the
leukotrienesexcreted into the urine will be diluted and may
thusescape detection. It is of interest that, in oneparticular
study (25), we were unable to detect asignificant postehallenge
inerease in urinary ETE4when an average value was ealculated for
the foursamples collected hourly after the maximal
airwayobstruction, whereas a significant increase wasdocumented
when the highest concentration in the1- or 2-h postehallenge sample
was selected indi-vidually (25). Tliis point was further
illustrated ina study by Christie et al., which showed a
peakincrease in urinary LTE4 1.5 h after inhalation ofLTC4 or LTE4
in asthmatics, with levels almost backto baseline after 3.5 h
(47).Gas chromatography-mass spectrometry (GC-MS), which is a
highly sensitive and specificmethod, may be an alternative for
measurementsof urinary LTE4. However, derivatization pro-eedures
used for other eicosanoids before GC-MScannot be used for
cysteinyl-containing leuko-trienes. Recently, an alternative GC-MS
methodwas described where the cysteinyl-leukotrieneswere subjected
to catalytic reduction and desulfuri-zation before conversion into
the pentafluorobenzyl(PFB) ester trimethylsilyl (TMS) ether
derivatives(54). Analysis with GC-MS was subsequently per-formed
with selected ion monitoring (SIM) usingstable isotope-labeled LTE4
analogs as internalstandards. Interestingly, the values obtained
withquantitative GC-MS for basal urinary LTE4 inhealthy subjects
(52) correlated very well withvalues reported from immunoassay
analyses (22,
Measurement of urinary LTE4spectrometric procedures demand
eunibersomeand time-consuming purification of the samples.Although
GC-MS is an important tool to quantifyurinary LTE4 reliably and may
serve as a "goldstandard" for calibration of other analytic
methods,it is unlikely that GC-MS will become useful forhigh-output
routine purposes. Another sophisti-cated teehnique, capillary
electrophoresis, wasrecently employed for measurements of
eieosa-noids, among them LTE4 and its metabolites (60).However, the
sensitivity of the electrophoresis waseven less than that of HPLC
with UV detection formeasurements of leukotrienes, and thus was
about100 times less sensitive than the immunoassays.Basal levels of
urinary LTE4Tlie procedure with imm unoassay analysis of
unex-tracted urine samples, stored without preservatives,has been
applied to samples collected during clini-cal experimental studies.
First, UrE4 was measuredby EIA in urine samples collected every
third hour,for a period of 24 h, from a group of
healthynonasthmatic subjects without diurnal variation inpeak
expiratory flow. In this group of nonasthmaticsubjects, there were
no signs of diurnal variation inthe excretion of urinary LTE4 (27).
In line with thisobservation, Asano et al. eould not identify
diurnalvariation in the excretion of LTE4 in either normalsubjects
or a group of patients with asthma (61).On the other hand, it was
recently reported thatpatients experiencing nocturnal exacerbation
showedincreased excretion of urinary LTE4 in samplescollected from
9 pm to 9 am (62). There was a linearcorrelation between morning
dip in lung functionand urinary excretion of LTE4 (62). However, in
astudy by Wenzel et al., the dil'ferenee from day tonight in
urinary LTE4 in patients with nocturnalasthma was not significant,
but the levels weresignificantly higher than in the controls in
samplescollected between 11 pm and 7 am, as well asbetween 3 pni
and 11 pm (63). Treatment with the5-lipoxygenase inhibitor Zileuton
showed signifi-cant attenuation of urinary LTE4 in the
asthmaticpatients together with a trend to improvement inlung
function (63).The mean baseline level of LTE4 in morningurine
samples (at 6 am) from the healthy, non-asthmatic subjeets was not
different from a groupof atopic asthmatics (27). Basehne values
given inthe literature for asthmatic and nonasthmatic sub-jects
vary considerably, mainly because of varyingassay procedures.
Nevertheless, the studies gener-ally show no significant
discrepancies betweenbaseline urinary LTE4 in healthy nonasthmatic
and
-
7/28/2019 Measurements of Leukotrienes in the Urine- Kumlin
5/13
-
7/28/2019 Measurements of Leukotrienes in the Urine- Kumlin
6/13
Measurement of urinary LTE4An increased excretion of urinary
LTE4 after ehallenge was oral or by inhalation (20, 23, 58,
66,allergen-induced airway obstruction was initially 73, 75, 76);
in one ease, it was as much as sevenfolddocumented by Taylor et al.
(18), and later con- (67). Interestingly, inhaled PG E, was shown
tofirmed by us and others (19, 20, 48, 69, 71 , 72). prevent
aspirin-induced bronchoeonstriction as wellBronchial provocation by
cumulative ehallenge as to attenuate the aspirin-induced rise in
urinarywith increasing doses of specific allergen in atopic LTE4
excretion (76). However, baseUne levels of
asthmatics was followed by a significant, twofold urinary LTE4
in these aspirin-sensitive asthmaticsincrease in urinary eoncen
tration of LTE4 (20). In were not affected by PG Ej
inhalation,anothe r study, after a single dose of allergen, the
Another type of trigger in asthma is exercise,postchallenge urinary
LTE4 values increased by causing exercise-induced
bronchocotistriction. Studiesabout 40% above prechallenge baseline,
and the of exereise-induced asthmatic responses have pro-peak
excretion occurred in the first two hourly duced somewhat
contradictory results regardingsamples, collected after the induced
bronchial the role of leukotrienes. It has not been
possibleobstruction (25). A correlation between the airway to
document increased excretion of LTE4 afterresponse and urinary
exeretion of LTE4 could be exercise-induced airway obstruction (57,
78), withseen when the area under the curve representing the
exception of one report on elevated urinaryairway obstruction was
com pared with the net LTE4 levels after exercise ehallenge in a
group ofrelease of urinary LTE4 (25). Studies repo rted in children
(79). Therefore, at present, the role ofthe literature have been
perfonned according to cysteinyl-leukotrienes in this type of
asthma eandifferent protocols; nevertheless, the increase in not be
determined solely on the basis of analysesurinary LTE4 after
allergen challenge has been of urinary LTE4. However, since several
differentshown to be between two- and fivefold in a number
antileuko triene drugs provide significant protec -of independent
reports (18 -20 , 57). Tlie end-point tion in exercise-induced
asthma, it has been sug-in most provocation protocols has been a
decrease gested that leukotrienes mediate also this type ofin FE"V,
by 20% ; thus, approximately the same airway obstruction (80 -83 ).
In fact, since exercise-degree of bronchoeonstriction was elicited
in all induced airway obstruction is relatively brief, thepatien
ts. brief stimulation by exereise may be insufficient toIt is still
not clear how the release of leukotrienes generate enough
leukotrienes detectab le abovein the airways is regulated. In
studies of leukotriene basal levels. Tliis further suggests that
the durationreceptor antagonists (see also above), we could of the
ehallenge eontributes to the amount of LTE4show an even more
pronounced increase in urinary excreted in the urine (see
discussion of allergenLTE4 when higher doses of allergen were
tolerated above).by the patients in the presence of the receptor It
should also be mentioned in this context thatantagonist (which
attenuated the airway obstruction) airway obstruction induced by
histamine or metha-(20). Tliis would point to a dose-dependent
release choline, two compounds commonly used to assessof
leukotrienes. W hether there is a relation to airway reactivity,
does not lead to increased excre-the tiine-span over which the
cells are activated tion of urinary LTE4, as shown by us and others
(20,and whether repeated bursts of activation of the 84). Hence,
there are no indications that leuko-leukotriene-producing cells by
several ehallenges trienes are second messengers in the
smooth-muscleare involved in the meehanism is currently under
contraction induced by histamine or methacholine.investigation. On
the other hand, airway obstruction induced by
Eurthennore, inhalation of lysine-aspirin in aspirin-
platelet-activating factor (PAF) was followed byintolerant pa
tients, leading to a significant airway augmented LTE4 levels in
the urine (84), and a roleobstruction, was shown to be assoeiated
with for leukotrienes in PAF-induced bronchial obstruc-increased
excretion of urinary LTE4 (20). This was tion was further supported
by the beneficial effectexclusive for the intolerant patients,
whereas aspirin- of leukotriene recep tor antagonists on the
broncho-toleran t asthmatics did not react with either bron-
constrictor effect of inhaled PAF (85, 86).chial obstruction or
increased excretion of urinary Whether urinary LTE4 is increased
also in associ-LTE4 in response to inhaled lysine-aspirin (20).
ation with late-phase asthmatic responses has alsoIncreased urinary
LTE4 excretion in aspirin-sensitive been unclear. A limited number
of bronchial provo-subjects has been confirmed by others using oral
cation studies have considered the role of leuko-as well as inhaled
routes of aspirin administration trienes in the late asthmatie
response. Generally, a(58, 66, 67 ,13-16). How ever, the oral
challenge is prolonged elevation of the urinary levels of LTE4often
associated with severe systemie reactions has been doeumented,
rather than a significant(77). Although absolute values vary
between the distinct second peak of increase (18,1 9, 22, 48, 5 5
-
-
7/28/2019 Measurements of Leukotrienes in the Urine- Kumlin
7/13
Kumlincontinuous excretion of leukotrienes previouslyformed
during the early response is not possible todetermine at the mom
ent, and contradictory resultshave been presented (19, 55, 56, 69).
How ever, therapid m etabolic clearance of
cysteinyl-Ieukotrienes(43, 45) rather supports de novo formation
ofleukotrienes also during the late-phase response.Recent data from
our laboratory further support arelease of cysteinyl-Ieukotrienes,
as well as PGD2,during the late asthmatic response to
allergenchallenge in dual responders (87), and this wascorroborated
by results from pharmacologic inter-vention (88). These latter data
confirm earherreports on significant attenuation of the
late-phaseresponse by antileukotriene drugs, which in turnstrongly
supports the view that leukotrienes alsocontribute to the late
phase of antigen-inducedairway obstruction (21, 22, 69).
Concerning pharmacologic regulation of leuko-triene formation, a
few studies on inhaled steroids,(3-agonists, and sodium
cromoglycate have concen-trated on the relationship between effects
onallergen-provoked airway obstruction and increasedurinary LTE4
excretion (56, 89, 90). With all threedrugs, a significant
attenuation of the airwayresponse was observed, whereas the
allergen-induced increase in urinary LTE4 was not affected.This may
reflect differences between in vitro andin vivo actions of
glucocorticoids on leukotrienebiosynthesis and also that the
pharmacologicactions of [3-agonists and sodium cromoglycate donot
primarily involve interference with leukotrieneformation or action.
There are several other pos-sible explanations of these findings
which cannotbe elaborated on here. However, a less cumber-some
method for measurement of urinary LTE4, asdescribed in this
chapter, might give better oppor-tunities to elucidate further the
effect of currentasthma therapy on the leukotriene pathway.
Con-sidered together, however, the current data supportthe view
that glucocorticosteroids have no signifi-cant direct effects on
leukotriene formation in asthma.Effects of leukotriene
biosynthesisinhibitors and leukotriene receptorantagonists on
induced increase in urinaryThe effects of two specific leukotriene
receptorantagonists (ICI 204, 219 and MK-0679) andone leukotriene
biosynthesis inhibitor (the FLAP-inhibitor BAY xlOO5) on airway
response andurinary LTE4 were evaluated in bronchoprovoca-tion
studies (20, 23, 25). The trials followed adouble-blind,
placebo-controlled, crossover design.
presence of the leukotriene receptor antagonistAccolate (ICI
204, 219; 20 mg, 2 h before start ofprovocation), the amount of
allergen required toprovoke a 20% drop in FEV,, i.e. the PD20
forallergen, was significantly increased. In line withthis increase
in allergen dose, there was a meanfivefold postchallenge increase
in urinary LTE4 inthe presence of the leukotriene receptor
antago-nist, as compared to a twofold increase during theplacebo
session (20). This supports dose- and per-haps also
exposure-time-dependent influences onthe leukotriene
formation.Since it was clear that aspirin-intolerant asthma-tics
had a higher basal excretion of LTE4, it was ofinterest to see
whether this group of asthmaticswould benefit from treatment with a
leukotrienereceptor antagonist. The patients were given either750
mg of MK-0679 or placebo 1 h before inhalation challenge with
increasing doses of lysine-aspirin (23). Pretreatment with MK-0679
caused adistinct rightward shift of the dose-response rela-tionship
for all subjects, three out of eight failingto produce a 20%
decrease in FEV, after inhala-tion of the highest possible
aspirin-dose. UrinaryLTE4 was determined in hourly collected
samplesby RIA. It was confirmed that the bronchoconstrictorresponse
to aspirin was again associated withincreased levels of urinary
LTE4, with peak concen-tration in the first hourly collected
samples aftermaximal airway response. As was seen for ICI204,219 in
the allergen challenge, the urinary LTE4levels were found to be
higher after pretreatmentwith MK-0679, in association with the
augmentedPD20 for lysine-aspirin (23), indicating a
similardose-dependence for aspirin-induced leukotrienerelease as
for allergen-provoked release (see above).In neither of these
studies did the leukotrieneantagonists cause significant elevation
of basalurinary LTE4 (20, 23). Partial inhibition of
aspirin-induced asthma was reported by Christie et al. forthe
leukotriene receptor antagonist SK&F 104353in an oral challenge
study (91), and a role for 5-lipoxygenase products in
aspirin-induced asthmawas corroborated in a 3-week trial with the
leuko-triene biosynthesis inhibitor Zileuton (92) andmore recently
with the 5-lipoxygenase inhibitorZD2138, where the inhibition of
the aspirin-induced fall in FEVi was associated with substan-tial
inhibition of leukotriene production (75).Next, bronchial
provocation with a single pre-determined PD20 for allergen was
performed in thepresence or absence of the leukotriene
biosynthesisinhibitor BAY xlOO5 (25). The airway response tothe
inhaled dose of allergen was significantly inhib-ited on the day
when BAY xlOO5 (750 mg) was
-
7/28/2019 Measurements of Leukotrienes in the Urine- Kumlin
8/13
the reaction. The calculated mean inhibition of themaximal drop
in FEV, was approximately 65%.Basal urinary excretion of LTE4 was
not signifi-cantly different on the two study days. The netrelease
(postchallenge level minus prechallengelevel) of LTE4 was
significantly less during the BAYxlOO5 session than the placebo
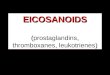
session. Tlie inhibi-tions of the airway response and
postchallengeincrease in urinary LTE4 were 73% and
88%,respectively, and thus correlated very well (Fig. 3)(25).To
date, data have been published on the cor-relation between the
effects of leukotriene bio-synthesis inhibitors on airway response,
excretionof urinary LTE4, and ionophore-stimulated ex vivoformation
of LTB4 in whole blood. The results fromtwo studies performed with
Zileuton and MK-886indicated that an inhibition of up to almost
100%of ex vivo LTB4 formation does not correlatedirectly with the
effect of the drugs on the airwayresponse to allergen (69, 71).
Although the effectof Zileuton on the airway response was
nonsignifi-cant for the group as a whole, some correlationbetween
inhibition of the early asthmatic responseand urinary LTE4
excretion was obtained for theindividual subjects (71). Nasser et
al. could notdocument any protection against
allergen-inducedasthmatic responses by the 5-lipoxygenase
inhibitorZD2138, despite 82% inhibition of LTB4 atid 52%inhibition
of urinary LTE4 excretion (72). On theother hand, Friedman et al.
could document asignificant correlation only between plasma
levelsof MK-886 and the attenuation of ex vivo LTB4production (69).
Together with our own data onBAY xlOO5, the results obtained so far
suggestthat a high degree of in vivo inhibition of pul-monary
leukotriene production is necessary toobtain a significant effect
on the airway responseby the leukotriene biosynthesis inhibitor.
Moreover,
Measurement of urinary LTE4determination of inhibition of ex
vivo formation ofLTB4 may well correlate with the drug plasma
level,but not necessarily with inhibition of enzymaticactivity in
target cells in the lutig.Conclusions on methodological aspectsand
further applications of m easuremen tsof urinary LTE4We have
validated a simple strategy for tneasure-nients of urinary LTE4 and
successfully applied thisprocedure in some clinical studies of
antileuko-triene drugs. In summary, there was no diurnalvariation
in urinary LTE4 excretion in healthysubjects, and we could document
that aspirin-intolerant asthmatics as a group had higher
basallevels of urinary LTE4, whereas there was nodifference
betweeti other asthmatics and normalcontrols. Furthermore,
lysine-aspirin-induced air-way obstruction in aspirin-intolerant
asthmaticsresulted in increased levels of urinary LTE4. Like-wise,
allergen challetige in atopies caused increasedurinary excretion of
LTE4, whereas airway ob-struction induced by histamine did not
cause anyalteration in urinary LTE4. Furthermore, the leuko-triene
biosynthesis inhibitor BAY xlOO5 inhibitedpostchallenge increase in
urinary LTE4, as well asimmediate airway response to a single dose
ofinhaled allergen.
Tlie methodological coticlusions that emergefrom the published
data are as follows. First,immunoassay of serially diluted
unextracted urinesamples is a reliable means to measure in
vivoproduction of cysteinyl-leukotrienes. Purificationof the
samples causes substantial losses of leuko-trienes and does not
necessarily improve the assay.Second, inhibition of postchallenge
increase inurinary LTE4 appears to correlate with inhibitionof
allergen-induced airway obstructioti, whereas
Fig. 3. InhibilBAY xlOO5 inhibited allergen-induced :(AUC) for
change in FEV ,, as compare on by 73% (left panel, elosed bar) when
expt:atment session (open bar). BAY xlOO5 likewise
-
7/28/2019 Measurements of Leukotrienes in the Urine- Kumlin
9/13
Kumlin
inhibition ofexvivo formation of LTB4 correlates choline and
histamine in normal and asthmatic subjectswith plasma concentration
of drugs ra the r than Eur Respir J I988;l:9l3-17.inhibition of
airway response. Third, measurements ' j,.jg"g ^^ th
'alr'waes^ons'iv*eneLio'\'ii t'a'mine' iiof basal urinary LTE4
alone may be a poor index siibje'cts wi'th asthnTa' ^nd iToTmars
titijec s.*J Aller'gy^Cliiito assess the in vivo effects of
different doses of Immunol ]988;82:654-60.leukotriene biosynthesis
inhibitors on pulmonary 9 Jacques CAJ, Spur BW Johnson M, Lee TH.
Tlie mecha-production ofcysteinyl-Ieukotrienes. It is proposed "''
"i ''LTE4-induced histamine hyperresponsiveness intha t bronchial
provocati on studies with allergen, L"'Xo''lfrTptiar iLicMl 1991 ^
^ ^aspirin, or PAF preferentially be used in at te mp ts IQ
O'Hickey SP, Hawksworth RJ Fong CY Arm JR Spur BWto establish the
effective doses of biosynthesis Lee TH. Leukotrienes C4, D4 and E4
enhance histamineinhibi tors. responsiveness in asthmatic airways.
Am Rev Respir Dis
Taken together, thesensi tive and ra ther simple
i99l;l44;l053-7.method we describe for analysis of excretion of '^
- '"^ ' ' O'Hickey SR Spur BW Lee TH. Airway respon-LTE4 in human
urine may be useful in further rs^I^lri inlcrd Ts\hU" A nrReT Rer
p'i r" D r^chnical trials with an ti-leuko triene drugs. Since
148-53.many disorders, such as other pulmonary diseases 12.
Christie PE, Schmitz-Schumann M, Spur BW Lee TH(33, 93, 94), atopic
diseases (95), anaphylact ic Airway responsiveness to leukotriene
C4 (LTC4), leuko-reactions (70), cardiovascular disorders (96, 97)
, tnene E4 (LTE4) and histamme in aspirm-sensitive asth-and
autoimmune diseases (98-100), have been jj slsadVcs' ' Nieves AL'"'
Krauss AH-P Woodward DF.associated with altered excretion of
urinary LTE4, ' Comparison of leukotriene B4 and D4 effects on
humanthis method may be applicable in a broad range of eosinophil
and neutrophil motility in vitro. J Leukoc Bioexperimental clinical
studies. 1994;55:]83-91.
14. Laitinen LA, Laitinen A, Haahtela T, Vilkka V Spur BWLee TH.
Leukotriene E4 and granulocytic infiltration intoasthmatic airways.
Lancet 1993;341:989-90.Acknowledgments 15. MacGlashan DWJ,
Schleimer RR Peters SR et al. Gener-
Tliese studies were supported by grants from the Swedish ^' '" '
leukotrienes by purified human lung mast cells.Medical Research
Council (projects 14X-09071 03X-217) the J Chn Invest
1982;70:747-51.Swedish Association Against Asthma and Allergy
(A&A), the 1^. Kumlin M, Dahlen S-E. Character.st.es of
formation andSwedish Heart Lung Foundation, Vardalstiftelsen, the
Swedish ^'''^^'"' metabolism of leukotrienes m the chopped
humanSociety of Medicine, Stiftelsen Lars Hiertas Minne, Stiftelsen
'""8- Biochim Biophys Acta f990;1044:201-10.Ragnhild ochEinar
Lundstroms Minne, the Institute of 17. Dahlen S-E, Hansson G,
Hedqvist R Bjorck T Granstrom EEnvironmental Medicine, the Swedish
Environment Protection Dahlen B. Allergen ehallenge of lung tissue
from asthma-Board (312049), and Karolinska Institutet '"^^ "^ ' ' "
'^ bronchial contraction that correlates with the^ ' release of
leukotrienes C4, D4 and E4.Proc Natl Acad Sci
USA 1983;80:1712-16.18. Taylor GW Taylor I, Black R et al.
Urinary leukotriene E4after antigen challenge and inacute asthma
and allergic
1. Arm J, Lee T Sulphidopeptide leukotrienes in asthma. Clin
rhinitis. Lancet 1989;l:584-8.Sci 1993;84:501-10. 1' - Sladek K
Dworski R Fitzgerald GA, et al. Allergen-
2. Dahlen S-E. Leukotrienes as mediators of airway obstruc-
stimulated release of thromboxane Aj and leukotriene E4tion
andbronchial hyperresponsiveness. In: Page C ' " humans. Effects of
indomethacin. Am Rev Respir DisGardiner P, editors. Airway
hyperresponsiveness: is it really 1990;]41:1441-5.important for
asthma? Oxford: Blackwell Scientific, 1993: 20. Kumlin M, Dahlen B,
Bjorck T, Zetterstrom O, Granstrom E,188-205. Dahlen S-E. Urinary
excretion of leukotriene E4 and
3. Dahlen S-E, Bjork J, Hedqvist P et al. Leukotrienes
11-dehydro-thromboxane B2 in response to bronchial pro-capillary
venules- in vivo effects with relevanee to the acute mine in
asthmatics. Am Rev Respir Dis 1992;146;96-1()3.inflammatory
response. Proc Natl Acad Sci USA 1981; 21. Taylor IK, O'Shaughnessy
KM, Fuller RW, Dollery CT78:3887-91. Effect of
cysteinyl-leukotriene receptor antagonist ICI
4. Dahlen S-E, Hedqvist P, Hammarstrom S, Samuelsson B. 204,219
on allergen-induced bronehoeonstriction and air-Leukotrienes are
potent constrictors of human bronchi. way hyperreactivity in atopic
subjects. Lancet 1991;337;Nature 1980;288:484-6. 690-4.
5. Marom Z, Shelhamer JH, Bach MK, Morton DR, 22. Rasmussen JB,
Eriksson L-O, Margolskee DJ, TagariRKaliner M. Slow-reacting
substances, leukotrienes C4 and Williams VC, Andersson K-E.
Leukotriene D4 receptorD 4, increase the release of mucus from
human airways in blockade inhibits the immediate and late
broncho-vitro. Am Rev Respir Dis 1982;126:449-51. constrictor
responses to inhaled antigen inpatients with
6. Arm JR O'Hickey SP, Hawksworth RJ, et al. Asthmatic asthma. J
Allergy Clin Immunol 1992;90:193-20f.airways have a
disproportionate hyperresponsiveness to 23. Dahlen B, Kumlin M,
Margolskee D.I, et al. The leuko-LTE4, as compared with normal
airways, but not to LTC4, triene-receptor antagonist MK-0679 blocks
airway obstruc-LTD4, methaeholine, and histamine. Am Rev Respir Dis
tion induced by inhaled lysine-aspirin in
aspirin-sensitive1990;142:ll]2-18. asthmatics. Eur Respir J
1993;6:I018-26.
-
7/28/2019 Measurements of Leukotrienes in the Urine- Kumlin
10/13
Measurem ent of urinary LTE4
umlin M, Ihre E, Zetter strom O, Dahlen S-E.generation in atopie
asthmatics by the leuko-
E4. Biochem Biophys Res Commun 1985:130:214-20.43. Huber M,
Muller J,'Leier I, et al. Metabolism of cystei
leukotrienes in monkey and man. Eur J Bioch1990:194:309-15.
44. Maltby NH, Taylor GW Ritter JM, Moore K Fuller RWtabolis
;l E, Cohn J, Dube L, Drazen JM. Effe( of tre ti tman. J Allergy
Clin Immunol 1990:85:3-9.
45. Sala A, VoeFkel N, Maclouf J, Murphy RC. Leukola. JAMA
1996;275:931-6.
mlin M, Stensvad F, Larsson L, Dahlen B, Dahlen S-E.tion and
applieation of a new simple strategy for
J Biol Chem 1990:265:21771-8.46. Verhagen J, Bel EH, Kijne GM,
e
1 Rosello J, e al. Release of peptideCommun 1987:] 48:864-8.
47. Christie PE, Tagari P, Ford-Hut
r Dis 1992:145:65-9.is 1 Catafau JR, Serra .T Bulben O, Picado
C, Gelpi E.
LTE4 in asth48. lagari P Ras
: subjects. Eur Respir J 1994:7:907-13.en JB, Delormc D, et al.
Comparison olnc E4 and 16-carboxytetranordihydrc
alle: afteirly allergic n
aglandins 1991:42:411-21JC, Chan-Yeung M, Si
s JV Kay A
ac- antigen. Eicosanoids J 990:3:75-80.49. Maclouf J, Antoine C.
De Caterina R. et al. Entry rate andH. metabolism of leukotriene C4
into vascular compartment
na. in healthy sut jects. Am J Physiol 1992:263:H244-9.50.
Westcott JY, Voelkel NF Jones K Wenzel SE. Itiactivation
of leukotriene C4 in the airways and subsequent urinarybronchial
asthma and other respiratory diseases.
Wenzel SE, Larsen GL, Johnston K Voelkel NF,steott JY Elevated
levels of leukot riene C4 in broncho-
d from atopic asthmatics after endo-
-51.. Mayatepek E, Peeher G. 1
Clin Chim Acta 1993:218:185-92.52. NicoU-Griffith D, Zamboni R,
Ras n JB,
Johnston K Bat t RA, Wenzel SE, Voelkel NF
release in upper respi ratory mueosa during naturalragweed in
ragweed-sensitive children. J Allergy
lovitz B, Nathanson I, DeCastro G, et al. Relationshi p
eukotrienes in plasma. Prostaglandins 1987;ent
a. Arch Dis Child 1995:73:221-5.
ment high-performance liquid ehromatographyasthmatics. J
Chromatogr 1990:526:341-54.
53. Bland J, Altman D. Statistical methods for assesment between
two methods of clinical meLancet 1986:1:307-10.
54. Tsikas D, Fauler J, Gutzki FM, Roder TH, BesFrolich JC. Gas
chromatographic-mass spectrerium-labelled leukot riene E4
standards. J Chrom622:1-7.
55. Manning PJ, Rokaeh J, Malo J-L, et al. Uri nary leukE4
levels during early and late asthmatic res]J Allergy Clin Inimunol
1990:86:211-20.
asthma. Effects of' j
Ethier D.iple treat-and radio-
ng deute-logr 1993:
vays
P Ethier D, Carry M, et al. Measurements of urinary challenge in
brobv revcrsed-phase liQUid cliromato^rHpny and 144il41 l-l^ .
Clin Chem 1989:35:388-91. 58. Christie PE, TligM, Kastner S,
Scholmerich ,1, Gerok W Keppler D. leukotri ene E4 i
reactivity and sodiu1991:143:1322-8.57. Smith CM, Christie PE,
Hawksworth RJ. Thien F. Lee TH.
s E4 levels after allergen and echial 11 Rev Respir Dis 1991
1 paI syndrome. Eur J Clin Invest 1989:19:53-60.1 JM, O'Brien
,1, Sparrow D, et al. Recovery of
ne E4 from the urine of patients with airwayRJ, Tliien FCK,
Christie PE, Lee TH.
S. Iti vivo metabolism
59. Israel E, Rubin P Kemp JP et al. Tlie effect of inhibiticof
5-lipoxygenase by Zileuton in mild-to-moderate asthmAnn Intern Med
1993:119:1059-66.
60. Tsikas D, Fauler J, Bracht S, Brunner G, Frolich J.
Analy;metabolites by eapillary isotaehophoresis.
Electrophore;1993:14:664-6.
61 . Asano K Lilly CM, O'Donell WJ. et al. Diurnal variati(
-
7/28/2019 Measurements of Leukotrienes in the Urine- Kumlin
11/13
asthma. .1 Allergy Clin Immunol 1995;96:643-51. effect of ICI
204,219, a potent leukotriene D^ rece'ptor62. Bellia V Bonanno A,
Cibella F, et al. Urinary leukotriene antagonist. Am Rev Respir Dis
]992;145:746-9.
E4 in the assessment of nocturnal asthma. J Allergy Clin 82.
Robuschi M, Riva E, Fucella LM, et al. Prevention ofImmunol
1996;97:735-4]. exercise-induced bronchoconstriction by a new
leukotriene
63 . Wenzel SE, Trudeau JB, Kaminsky DA, Cohn J. Martin RJ,
antagonist (SK&F 104353). A double-blind study versusWestcott
JY. Effect of 5-lipoxygenase inhibition on disodium cromoglyeate
and plaeebo. Atn Rev Respir Disasthma. Am J Respir Crit Care Med
1995;152:897-905. 83. Meltzer'SS, Hasday JD, Cohn J, Bleecker ER.
Inhibition
64. Greally P, Cook A.T, Sampson AP, et al. Atopic children of
exercise-induced bronchospasm by Zileuton: a 5-with cystic fibrosis
have increased leukotriene E4 concen- lipoxygenase inhibitor. Am J
Respir Crit Care Med 1996;trations and more severe pulmonary
disease. J Allergy Clin 153:931 -5 .Immunol 1994;93:100-7. 84.
Taylor IK, Ward PS, Taylor GW Dollery CT, Fuller RW
65. Szczeklik A. Aspirin-induced asthma; pathogenesis and
Inhaled PAF stimulates leukotriene and thromboxane A4clinical
presentation. Allergy Proc 1992;13; 163-73. production in humans. J
Appl Physiol 1991;71;t396-1402.
66. Christie PE, Tagari P, Ford-Hutchinson AW et al. Urinary 85.
Spencer DA, Evans JM, Green SE, Piper PJ, Costello JF.leukotriene
E4 concentrations increase after aspirin chal- Participation of the
cysteinyl leukotrienes in the acutelenge m aspirin-sensitive
asthmatic subjects. Am Rev bronchoconstrictor response to inhaled
platelet activatingRespir Dis 1991;143;1025-9. (actor in man.
Thorax 1991;46;44]-5.
67. Nasser SMS, Patel M, Bell GS, Lee TH. The effect of 86.
Kidney JC, Ridge SM, Chung KF, Barnes PJ. Inhibition ofaspirin
desensitization on urinary leukotriene E4 concen-
platelet-activating factor-induced bronchoconstriction byMed
f995;151;1326-30. ' ' T ' ? ' ' ' ^ " " ^
68. O'Sullivan S, Dahlen B, Dahlen S-E, Kumlin M.
Increaseurinary excretion of the prostaglandin Dj metabolit 49a,l
lP-prostaglandin F2 after aspirin challenge supports
9a,ll(3-prostaglandin F2 during allergen-induced early andmast cell
activation in aspirin-induced bronchoconstriction. late phase
asthmatic reactions Am J Respir Crit Care MedJ Allergy Clin Immunol
1996;98;421-32. 1996;153;A250.
69. Friedman BS, Bel EH, Buntinx A, et al. Oral leukotriene 88.
Roquet A, Dahlen B, Kumlin M, et al. Combinedinhibitor (MK-886)
blocks allergen-induced airway res- antagonism of leukotrienes and
histamine produces pre-ponses. Am Rev Respir Dis l993;147;839-44.
dominant inhibition of allergen-induced early and late
70. Denzlinger C, Habert C, Wilmanns W Cysteinyl leuko- phase
airway obstruction in asthmatics. Am J Respir Crittriene production
in anaphylaclic reactions. Int Arch Care Med 1997 (in
press).Allergy Immunol 1995;] 08; 158-64. 89. Taylor IK,
O'Shaughnessy KM, Choudry NB, Adachi M,Hui KP Taylor IK T l GW t l
E f f t f P l JBD Fl l RW A i
R e v87. O'Siexcr
kcspiretion
D iss..f leKumliukotrin M,ene E4Larsscan d inth L, e(e mas alt
cell t ) lark
gy71 . Hui KP, study, y , almer JBD, Fuller RW A comparative
study in
5-lipoxygenase inhibitor on leukotriene generation and atopic
subjects with asthma of the effects of salmeterolairway responses
after allergen challenge in asthmatic and salbutamol on
allergen-induced bronchoconstriction,patients. Thorax
199t;46:184-9. increase in airway reactivity, and increase in
urinary leuko-
72. Nasser SMS, Bell GS, Hawksworth RJ, et al. Effect ol the
triene E4 excretion. J Allergy Clin Immunol 1992;89:5-lipoxygenase
inhibitor ZD2138 on allergen-induced early 575-83.and late
asthmatic responses, lliorax 1994;49:743-8. 90. O'Shaughnessy KM,
Welling R, Gillies B, Fuller RW
73 . Knapp HR, Sladek K, Fitzgerald GA. Increased excretion
Differential effects of fluticasone propionate on allergen-of
leukotriene E4 during aspirin-induced asthma. J Lab Clin evoked
bronehoeonstriction and increased urinary leuko-Med 1992;!
19:48-51. triene E4 excretion. Am Rev Respir Dis
1993;147:1472-6.
74 . Sladek K, Szczeklik A. Cysteinyl leukotrienes over- 91.
Christie P, Smith C, Lee TH. The potent and selectiveproduction and
mast cell activation in aspirin-provoked sulfidopeptide leukotriene
antagonist, SK&F tO4 353,bronchospasm in asthma. Eur Respir J
1993;6:39]-9. inhibits aspirin-induced asthma. Am Rev Respir Dis
1991-75 . Nasser SMS, Bell GS, Foster S, et al. Effect of the 5-
144:957-8.lipoxygenase inhibitor ZD2138 on aspirin-induced asthma.
92. Israel E, Fischer AR, Rosenberg MA, et al. The pivotallliorax
1994;49:749-56. role of 5-lipoxygenase products in the reaction of
aspirin-76. Sestini P, Armetti L, Gambaro G, et al. Inhaled PGEj
sensitive asthmatics to aspirin. Am Rev Respir Dis 1993;prevents
aspirin-induced bronchoconstriction and urinary 148;1447-51.LTE4
excretion in aspirin-sensitive asthma. Am J Respir 93. Davidson D,
Drafta D, Wilkens BA. Elevated urinaryCrit Care Med 1996;153;572-5.
leukotriene E4 in chronic lung disease of extreme pre-
77 . Dahlen B, Zetterstrom O. Comparison of bronchial and
maturity. Am J Respir Crit Care Med 1995;151;841-5.per oral
provocation with aspirin in aspirin-sensitive 94. Cook AJ, Yuksel
B, Sampson AP, Greenough A Price JFasthmatics. Eur Respir J
1990;3;527-34. Cysteinyl leukotriene involvement in chronic lung
disease
78 . Taylor IK, Wellings R, Taylor GW, Fuller RW Urinary in
premature infants. Eur Respir J 1996;9;1907-12.leukotriene E^
excretion in exercise-induced asthma. 95. Fauler J, Neumann CH,
Tsikas D, Frolich JC EnhancedJ Appl Physiol ]992;73;743-8.
synthesis of cysteinyl leukotrienes in atopic dermatitis. Br
79. Kikawa Y, Miyanomae T, Inoue Y, et al. Urinary leuko- J
Dermatol 1993;128;627-30.triene E4 after exercise challenge in
children with asthma. 96. Carry M, Korley V Willerson JT, Weigelt L
Ford-J Allergy Clin Immunol 1992;89;1111-19. Hutchinson AW Tagari P
Increased urinary leukotriene
80. Manning PJ, Watson RM, Margolskee DJ, Williams VC, excretion
in patients with cardiac ischemia. In vivo evi-Schwartz Jl, O'Byrne
PM. Inhibition of exercise-induced dence for 5-lipoxygenase
activation. Circulation 1992;85;bronchoconstriction by MK-571; a
potent leukotriene D4- 230-6.
-
7/28/2019 Measurements of Leukotrienes in the Urine- Kumlin
12/13
Measurement of usurgery. Coron Artery Dis 1993:4:899-904.
1992:19:252-8.98. Fauler J, Thon A. Tsikas D, von der Hardt H,
Froiich JC. 100. Hackshaw KV, Yuhong SHI, Brandwein SR. Jones
K.Enhaneed synthesis of cysteinyl leukotrienes in juvenile Westcott
JY. A pilot study of Zileuton, a novel selectiverheumatoid
arthritis. Arthritis Rheum 1994;37:93-7. 5-lipoxygenase inhibitor,
in patients with systemic lupus
99. Hackshaw KV, Voelkel NF, Thomas RB, Westcott JY.
erythematosus. J Rheumatol 1995:22:462-8.
-
7/28/2019 Measurements of Leukotrienes in the Urine- Kumlin
13/13