Embed Size (px)
Citation preview

Adjuvant and Formulation Considerations for a Subunit Blood-Stage Malaria Vaccine
Martin Chang
Molecular Biosciences and BioengineeringPlan B, Final Report
August 15, 2012
Background and Introduction
One hundred years after the identification of the mosquito transmitted blood-borne parasite Plasmodium as the causative agent of malaria, the disease remains a major cause of morbidity and mortality around the world. There are an estimated 100 million cases yearly, of which half a million of them are fatal, the deadly cases most commonly occurring in children under the age of five [1].
There are five known species of Plasmodium which cause malaria in humans: P. falciparum, P. ovale, P. vivax, P. malariae, and most recently the monkey parasite Plasmodium knowlesi, which has been found to infect humans living near the edge of forests [2, 3]. Of these, P. falciparum causes the most severe disease and accounts for the majority of malaria deaths worldwide.
Various malaria eradication programs have been attempted throughout the course of human history, some with more success than others. Malaria has been successfully eradicated in the United States, with sporadic cases occurring in foreign travelers, but transmission is controllable, such that it has not been endemic in the US since the 1950’s. DDT and swamp drainage were two major tools used for mosquito control in this program, with the goal of breaking malaria transmission to the point it could be controlled on a case-by-case basis [4, 5].
Despite successes such as this, malaria is heavily entrenched in regions such as Sub-Saharan Africa. Poverty, government inefficiency, lack of an adequate health care system, and the stronghold of the Anopheles mosquito (that transmits the disease) in that area, all contribute to its continuing devastation on the communities there. Various methods are used to attempt control of the disease: insecticide treated nets, a rudimentary but effective health care system (involving people carrying cell phones and diagnostic kits to identify malaria and people carrying drugs in backpacks, often walking the distances between villages), and the conventional methods of indoor DDT spraying and water drainage. Insecticide treated bednets, in particular, are a simple and cost-effective way of reducing malaria mortality and morbidity [6, 7]. Still, the malaria burden remains severe in some areas, and more tools are needed [8].
One such tool is a vaccine, which has met wide success in the control and eradication of other diseases such as smallpox. Currently, the vaccine closest to approval for widespread usage is RTS,S, which is about 56% effective in preventing clinical malaria and 47% effective in preventing severe malaria (and by implication, malaria deaths) in 5 to 17 month old children [9]. It targets the pre-erythrocytic stages of the Plasmodium life cycle.

To understand this a little better, let us briefly go over the life cycle of the Plasmodium parasite. The stage of the parasite that is delivered by the mosquito proboscis is called the sporozoite. When it is injected into the skin, it migrates to the liver, where it invades hepatocytes and replicates. This stage ranges from about eight days to longer, depending on the species of Plasmodium. After this, the hepatocytes burst and merozoites, or the blood stage of the parasite, are released into the blood stream, whereupon they invade red blood cells (RBCs), replicate in them and cause the red blood cells to burst. The process continues, as merozoites expand exponentially in number. This is the disease-causing stage of the parasite. Some of the merozoites differentiate into gametocytes, and when a male and female gametocyte are uptaken into the same mosquito after an infected individual is bitten, they fuse and are able to beget sporozoites, ready to infect and repeat the life cycle once again [10].
The malaria vaccine situation can be improved on in a number of ways. The reduction in severe malaria would be the most important. Individuals who have had malaria before can often still get malaria, especially when they have been out of a malarious area for some time. However, rarely do these individuals get malaria again so severe that it results in death. Natural immunity to severe malaria is often obtained in endemic areas by the time the person is five years old. If a vaccine can induce immunity to severe malaria in children under the age of five, even if efficacy against clinical malaria may be far less, many deaths can be prevented.
Immunity against uncomplicated clinical malaria is important as well. Although not as serious as severe malaria, uncomplicated malaria can put a person out of work for weeks, and this especially impacts those communities who need every able body to help with their agriculture production. Although immunity to malaria from natural exposure is often not lifelong, there have been suggestions that this is due to the parasite effecting an immune tolerance towards its antigens. If so, immunity through a vaccine may have the potential to do better and induce longer term protection. A final consideration is that protection against clinical disease may not necessitate sterile immunity (ie. no parasites in the blood, body). This phenomenon in malaria, termed premunition, is common in endemic areas—individuals do not get sick, although they have low levels of the parasite circulating in their blood[11, 12]. Although this is not of much concern to the individual with premunition, it provides a pool of parasites which mosquitos can then transmit to non-immune individuals in the community, who can and do get sick . Although sterile immunity is not a necessary criteria for the success of a malaria vaccine, such a vaccine would be a great step forward towards eradication of the Plasmodium parasite [13].
A vaccine—as it is currently understood—directs the immune response against antigens associated with a disease. The way in which the immune system is desired to respond depends on the disease, and in the case of malaria, also on its life cycle stage. Vaccines against malaria are in development against each of its stages. In this report, I will be focusing on vaccine development against blood-stage antigens. Because a blood-stage vaccine is directly targeted at the disease-causing stage and because blood-stage immunity plays a large part in protection for naturally immune individuals, many efforts are directed at a vaccine against blood stage antigens.
Blood stage vaccines have shown protection in various animal models, up to protection in non-human primates challenged by P. falciparum, provided that a potent adjuvant such as Complete Freund's Adjuvant (CFA) is used in the vaccine formulation. However, because of greater stringency in humans for the use of adjuvants such as CFA, no blood stage vaccine has demonstrated statistically significant protection or even increased time to infection, although putative correlated measures such

as decreased in vivo parasite multiplication rate [14], increased inhibition in the growth inhibition assay (GIA), and increased parasite specific antibody titers have all been shown [15, 16].
Making matters more difficult is the fact that there is no set of immunological assays which can predict with certainty the immune status of an individual. Traditional measures, such as the ones mentioned in the previous paragraph, show correlation with protection in certain studies and not others, suggesting that there are other, perhaps more important immunological correlates out there. Along those lines, other assays which have shown association with protection against blood stage malaria are the antibody-dependent cellular inhibition (ADCI) [17] and the antibody dependent respiratory burst (ADRB) assays [18]. They share a similar underlying mechanism (the assays are explained below). ADCI was suggested to be a protective mechanism in an experiment that looked at the role of direct growth inhibition and ADCI in passive immunization against malaria [19]. Sera was obtained from hyper-immune individuals from Africa and given to newly infected Thai individuals, through passive immunization. The immune sera was able to control parasitaemia, although not to the point of elimination. Direct growth inhibition, as measured by GIA, did not correlate with the control of parasitaemia, while ADCI did.
GIA measures the amount of reduction in parasitized red blood cells in vitro, when immune sera is added to the culture. Complement is inactivated and the results are normalized so as to reflectparasite-specific antibody activity only. Because white blood cells are not included in the culture, direct antibody inhibition is implicated, such as antibodies blocking parasite protein epitopes that need to be exposed in order for processing and subsequent invasion. For example, in the case of merozoite surface protein 1 (MSP1), its cleavage to a 42 kDa protein, followed by cleavage into a 33 kDa and a 19 kDaprotein needs to occur before the parasite can invade an RBC. Antibodies can be produced which block this processing [20]. Therefore, this is one way that antibodies can mediate protection. GIA levels do indeed correlate with protection in the field, but with low specificity [21], implying that there are more important mechanisms of protection. A more direct study of this was performed in a mouse model, where mice were vaccinated with MSP1 from Plasmodium yoelii (a mouse malaria parasite) and then challenged with P. yoelii [22]. GIA was performed with P. falciparum transgenic for MSP1 from P. yoelii. The results showed that GIA activity was not necessary, and perhaps not even sufficient, for protection against lethal P. yoelii infection.
The evidence suggests that a cell mediated, antibody dependent mechanism is an overlooked key to understanding protection. Two assays have been described to measure the levels of this effect for malaria. The first is the ADCI assay. The ADCI assay is performed by placing monocytes, parasites, RBCs and immune sera in culture and measuring the amount of reduction in parasitized RBCs. The results are adjusted such that the assay measures the activity of monocytes activated by cytophilic antibodies bound to merozoite proteins, and not direct growth inhibition as measured by GIA or non-specific direct killing activity by the monocytes. Of note, the main inhibitory activity by monocytes in this assay is not phagocytosis but rather the secretion of a soluble factor, evidenced by the fact that the supernatant of activated monocytes in this assay, on its own, is able to inhibit parasite growth. The growth stage that is inhibited is the trophozoite within the RBC, as many parasites at this stage are observed, without progression to the formation of the multiple merozoites which will eventually burst from the RBC. The inhibition is reversible, with the trophozoites once again able to grow and divide once the soluble factor has been removed [23].

The factor is as yet unidentified, but certain cytokines and certain reactive oxygen species (ROS) have been ruled out. Not all ROS have been ruled out, however, and currently a type of ROS seems more plausible than a type of cytokine or signaling molecule. For a cytokine/signaling molecule to mediate ADCI, it needs to act directly on the parasite (ie. the parasite needs to have a receptor for it and transduce the signal to stop growth and proliferation) or signal the RBC to enact an inhibitory mechanism. Because reticulocytes and mature RBCs (both of which P. falciparum invades) don’t possess nuclei, transcription can’t occur, and any RBC signaling pathway must make do with whatever mRNA and proteins it had when the cell was enucleated. While this does not preclude the possibility of a cytokine transducing an inhibitory mechanism within the RBC, in the absence of further experiments, the ROS mechanism seems more plausible. However, it does seem unusual that the effect of an ROS mechanism would be reversible. Oxygen radicals often damage cells (parasites and also RBCs) beyond repair.
The second assay is the antibody dependent respiratory burst (ADRB) assay. It measures, by fluorescence, the amount of free radicals produced by neutrophils due to bound cytophilic antibodies. Strikingly, in an area of high transmission, individuals with high ADRB indices were seventeen times less susceptible to malaria attacks than those with low ADRB indices [24].
Memory B and T cell responses are important as well for production of antibodies of the appropriate specificity, affinity and IgG subclass. In addition to the quick recall of antigen-specific antibodies of the right isotype (in humans, IgG3 and IgG1 are the cytophilic antibodies associated with cell-mediated responses) by B-cells, IFN-gamma and other cytokines released by memory T-cells can signal the build-up of the innate effector cells (neutrophils, monocytes, or macrophages, etc) to clear the parasites [25, 26].
Identifying the important immune mechanisms mediating protection against blood-stage malaria is one aspect of developing a vaccine. The other requirement is priming the adaptive immune system to use those mechanisms upon secondary exposure to the antigens (ie. actual infection). Natural infection is characterized by exposure to many different antigens, resulting in polyclonal expansion of T and B cells. In the case of blood stage vaccines, although multivalent (more than one antigen) vaccines have been developed, many vaccines that have gone to clinical trials have been directed to oneparticular antigen. However, with such a monovalent vaccine—in the cases of MSP1 and AMA1, for example—very high antibody titers and growth inhibition levels are needed for protection in non-human primates [15, 16]. There is reason to think that regulatory mechanisms in our immune system make it harder to mount an extremely high immune response against one antigen as opposed to immune responses against several different antigens (which may be more protective, as well). The Combination B vaccine showed some evidence of this [27].
Another consideration, especially in subunit vaccines, is that certain antigens intrinsically skew the immune system in a certain way. It has been shown that although almost all B-cell epitopes ofMSP1-42 (the 42 kDa C-terminal portion of the MSP1 protein) are located within MSP1-19 (the C-terminal 19-kDa fragment), T-cell epitopes in MSP1-33 (the 33kDa segment N-terminal of MSP1-42) shape the immune response (cell mediated and humoral/antibody), with the inclusion and deletion of different T-cell epitopes changing T-cell proliferation, antibody titers, Th1/Th2 cytokine profiles and antibody properties [28]. Some mechanisms for this include different processing of the antigen by the

proteosome and certain T-cell receptor specificities associated with tolerance, inflammation, or a Th1 v. Th2 phenotype.
An antigen by itself is often not immunogenic enough to induce a strong immune response. In the case of the yellow fever vaccine, for example, a similar but less virulent virus, YF-17D, is used to potentiate the immune system. Because it is a whole virus vaccine, multiple antigen epitopes are presented. Also, multiple immune potentiators—viral RNA, repetitive structures on the viral surface, and kinetics of viral invasion—are present to signal to the immune system to mount a response.
In the case of subunit vaccines, where pathogen proteins are produced using recombinant gene expression systems, an extra component, called an adjuvant—from the Latin “adjuvare,” to help—needs to be added to obtain a strong and appropriate immune response. Sometimes, the recombinant proteins can self-assemble into small structures termed virus-like particles (VLPs), and these VLPs are self-adjuvanting. In other cases, small particles such as poly(lactic-co-glycolic acid) (PLGA) beads or aluminum hydroxide (alum) or oil droplet emulsions (such as squalene) have been added. Cytokines and also pathogen associated molecular patterns (PAMPs) are also used as adjuvants. Much knowledge has accrued about the particular receptors and pathways that transduce the effects of various adjuvants. Alum activates the inflammasome and the downstream caspases in its pathway. Double-stranded RNA binds to TLR-3 and signals through the TRIF adapter molecule. Lipopolysaccharide signals through TLR 4 and both the MyD88 and TRIF adapter molecules. Various synthetic analogues of these molecules have been produced which have lower toxicity (perhaps through more specific receptor-ligand interactions) but still induce the inflammatory cytokines useful in priming the immune system.
Our studies have so far focused on the use of PAMPs as adjuvants, so I will limit the majority of my discussion to them, but other molecules such as endogenous peptides (eg. heat shock protein) have also shown adjuvant activity. In addition, formulation considerations, such as particle-formation, ability to be metabolized, size, and co-localization of vaccine components will likely play a big role in determining the immunogenicity as well as adverse toxicity and reactogenicity of the vaccine.
Background for Study Design
Pathogen recognition receptors (PRRs) detect PAMPs, and their ligation activates signaling pathways that modify the immune response. The characterization of these pathways and receptor ligands may lead to the ability to formulate vaccines that activate the immune system in specific ways.
PRRs include Toll-like receptors (TLRs), NOD-like receptors (NLRs), and various other receptor families. The simultaneous activation of two or more PRRs may lead to a higher up-regulation of genes not possible with any single ligand alone. Another possibility is that the simultaneous activation of multiple PRRs may give rise to gene expression profile that is qualitatively different than the response to a single ligand. This phenomenon is called synergy.
Dendritic cells (DCs) are the most efficient antigen presenting cells (APCs) in the immune system, being nearly 100 times more potent than macrophages in inducing the activation and proliferation of naive T cells. Our study focuses on the in vitro response of dendritic cells to stimulation with various PAMPs and their combinations. Since the initial discovery of conventional DC (cDC) having a classical dendrite morphology, other cells have been added to the DC category, based on shared precursors during development or the expression of the DC marker CD11c in the absence of typical

morphological features of DCs. Furthermore, the conventional DC has been found not to be a homogenous cell population either, with a major division based on expression of CD8 (CD8+ cDCs and CD8- cDCs).
In this study, we examined the activation and functional properties of DC subsets in response to various PAMPs, individually and in combination. We used a mouse model of bone-marrow derived dendritic cells obtained from culture with the Flt3-L growth factor (FL-DCs), which allows us to study thethree major splenic DC subsets: the plasmacytoid DC (pDC), the CD8+ cDC, and the CD8- cDC. Surface and intracellular protein expression was evaluated by flow cytometry after FL-DCs were stimulated with various combinations PRR ligands, which were chosen as potential adjuvant formulations for use with vaccines in humans.
We attempt to predict the characteristics of the in vivo immune response due to different PAMP combinations, based preliminarily on protein expression profiles by dendritic cells. We chose to look at the expression of particular proteins, which when expressed by dendritic cells, have been identified as modulators of the immune system.
Table 1.
Antibodies selected for protein expression analysis on FACSAria flow cytometer
General DC marker Anti-CD11c-PE-Cy7
Plasmacytoid DC marker Anti-CD45RA-biotin/SA-PE-Texas Red
Cell activation markers Anti-CD80-PerCP-Cy5.5; anti-CD86-FITC
DC co-stimulatory molecules: Anti-Dll4-APC (Th1); anti-Jag1-PE (Th2)
DC Th-polarizing cytokines Anti-IFN-FITC (pDC)Anti-IL12p35-PerCP (Th1) Anti-IL-10-PE (Th2)Anti-IL23p19-eFluor 660 (Th17)
T-cells differentiating in the presence of IL-12 are polarized to become Th1 cells, which express IFN-gamma and cause B-cells to class switch their antibodies to cytophilic isotypes. T-cells presented with antigen in the presence of IL-10 and IL-4 often obtain a more Th2 or regulatory phenotype, although a Th2-polarizing cytokine analogous to IL-12 for Th1 has not been identified.
The expression of notch receptor ligands Delta-like-ligand 4 (Dll4) and Jagged1 (Jag1) were also examined. Notch signalling has many roles, such as preserving pluripotency in stem cells, angiogenesis, and differentiation of different cell types, including immune cells. Expression of Dll4 on CD8- dendritic cells is able to induce IFN-gamma production in T-cells (Th1) without the help of IL-12 [29]. Jag1 has been implicated in exacerbating Th2 diseases such as asthma [30-32]. However, not all results show that DC-expressed Dll4 induces Th1 cells [33-35] and that Jag1 induces Th2 cells [36-38]. Likely, the co-expression of these Notch ligands with other surface proteins, along with the cytokine mileu, is important—the lesson being that there is a complicated interplay of many different signaling proteins.
Studies have shown that in animal models a strong adjuvant is required for immunity from MSP1 vaccination [39, 40]. Complete Freund’s Adjuvant remains the standard to which other adjuvants

are compared, in MSP1 vaccinations of non-human primates. However, it is too reactogenic to be used in humans. Several components of Freund’s adjuvants have been identified as agonists of PRRs, found on cells such as DCs, and they function as molecular adjuvants [41]. Certain PRR ligand combinations are able to synergize to produce an enhanced Th1 response [42].
In our studies, we evaluated the responses to TLR ligands that signal through MyD88-dependent and/or MyD88-independent (TRIF-dependent) signaling pathways; an agonist for nucleotide-binding oligomerization domain protein (Nod1); and a ligand for the C-type lectin Mincle (Table 2). Because these receptors signal through distinct intracellulular signaling pathways, they have the potential of synergistic DC activation and improved priming of the immune response.
Table 2. Intracellular location and signaling pathways of PRR ligands evaluated as molecular adjuvants.PRR PRR Ligand Location Signaling Pathway [ref.]TLR4 GLA (non-toxic synthetic lipid A) Cell surface membrane TRIF [43]TLR3 Poly(I:C) (dsRNA analog) Endosomal membrane TRIF [44]TLR7/8 R848 (imidazoquinoline
compound) Endosomal membrane MyD88 [45]
Nod1 (NLR)
C12-iE-DAP (peptidoglycan subunit)
Cytosolic RIP2 [46]
Mincle (CLR)
TDB (synthetic trehalose dimycolate)
Cell surface membrane Syk/CARD9/Bcl10/Malt1 [47]
Specific Aim 1.
Hypothesis: Specific combinations of pattern-recognition receptor (PRR) agonists will be effective in vitro in inducing optimal activation of DC subpopulations.
Rationale: This strategy will allow us to identify combinations of PRR ligands that synergize to activate DCs to express cell surface markers and cytokines that polarize the immune response to a Th1 response, a Th2 response, or a mixed Th1/Th2 response. Selected combinations that differ in their induction of DC activation markers, co-stimulatory molecules associated with T cell polarization, and/or cytokine profiles will subsequently be evaluated in vivo in Specific Aim 2 as adjuvants for the immune response to a blood stage malaria antigen.
Experimental Plan: Bone marrow-derived DC expression of genes for cell surface markers and cytokines will be evaluated. DCs will be stimulated in vitro with various individual and combinations of PRR ligands. RNA transcription will be measured by real-time PCR and protein expression will be measured by flow cytometry, and ELISA or multiplex cytokine assays.
Methods:
Stimulation of bone-marrow derived DCs with PRR ligands: Bone marrow cells were obtained from C57BL/6 mice and cultured for 9 days in RPMI 1640 containing 10% fetal bovine serum (FBS) and 200 ng/ml Flt3-L (GenWay Biotech, San Diego, CA). Bone marrow-derived DCs, containing both pDCs and cDCs, were harvested, adjusted to a concentration of 1X106 cells/ml and stimulated with various PRR ligands for 3 or 8 h before RNA analysis. For cell surface marker and intracellular cytokine detection by flow cytometry, cultures were stimulated with PRR ligands for 8h, 24h, and 48 h. PRR ligand-stimulated

DCs were (a) analyzed by real-time PCR for selected immune transcripts, or (b) stained with various fluorescent-labeled antibodies specific for selected cytokines or cell surface markers and analyzed by flow cytometry.
PRR ligands: Poly (I:C), R848, and C12iE-DAP were obtained from Invivogen (San Diego, CA), trehalose-dibehenate was obtained from Avanti Polar Lipids (Alabaster, AL), and synthetic lipid A (GLA) was a gift from Dr. Tom Vedvick (Infectious Disease Research Institute, Seattle, WA).
RNA transcription analysis: Total RNA was extracted using the RNeasy Mini Kit (Qiagen, Valencia, CA). cDNA was synthesized using the iScript cDNA synthesis kit (BioRad, Hercules, CA). Quantitative PCR primers were obtained from Qiagen. Transcripts were measured using an iCycler iQ Real-Time PCR Detection System (BioRad). Fold changes in gene expression were calculated by the Pfaffl method [48],with 18S rRNA as the reference gene. Cytokine transcripts measured included general inflammatory cytokines (TNF-α, IFN- α) along with Th1 polarizing (IL-12), Th2 polarizing (IL-10), Th17 polarizing (IL-23, TGF-β with IL-6), and Treg polarizing (IL-10, TGF-β without IL-6) cytokines. Co-stimulatory molecules included general co-stimulatory markers (CD80) along with markers associated with Th1 (Dll1, Dll4) and Th2 (Jag1) co-stimulation. We also measured an apoptosis marker (Nur77) associated with activation-induced cell death.
Flow cytometry: DCs were stimulated with PRR ligands for various times. Bafilomycin A1 (0.5 uM; Biomol) was added 3 h after the start of culture and Brefeldin A (10 ug/ml; Sigma) during the last 1 h. Cells were fixed with 2% paraformaldehyde, permeabilized with PBS containing 2% FBS and 0.5% saponin, and stained with the fluorescent-labeled antibodies. Flow cytometry detected DC production of cytokines and surface markers associated with Th polarization. CD11c-PE-Cy7 (BD Biosciences, San Jose, CA), CD45RA-biotin (BD Biosciences), and Sirp-alpha/CD172a-biotin (eBioscience, San Diego, CA) antibodies were used to differentiate the three major DC populations: pDCs (CD11c+CD45RA+Sirp-a-), CD8+-equivalent cDCs (CD11c+CD45RA-Sirp-a-), and CD8--equivalent cDCs (CD11c+CD45RA-Sirp-a+) [49]. Biotinylated antibodies were detected using streptavidin-PE-Texas Red or streptavidin-APC-Cy7 (BD Biosciences, San Jose, CA). Antibodies for DC co-stimulatory molecules are Jag1-PE (BD Biosciences), CD80-PerCP-Cy5.5 (BioLegend, San Diego, CA), CD86-FITC (eBioscience), and Dll4-APC (BioLegend). CD80 expression is associated with Th2 activation and CD86 expression with Th1 activation. Intracellular cytokine production was evaluated using the following: IL-10-PE (BioLegend); IL-12p35-PerCP (R&D Systems); IL-23p19-eFluor 660 (eBioscience); IFN-α-FITC (InterferonSource). The FACSAria and LSRFortessa flow cytometers (Becton Dickinson) were used.

Results
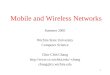
RNA expression of the CD80 activation marker by total bmDCs indicated that several combinations of PRR ligands were additive or synergistic for DC activation: R848+GLA, R848+p(I:C), R848+iE-DAP, GLA+p(I:C), and iE-DAP+p(I:C) (Figure 1). Th1 co-stimulatory molecule Dll1 was induced in cultures containing GLA, with similar levels obtained with R848+iE-DAP and iE-DAP+p(I:C). In another experiment, RNA expression of the Th1-costimulatory Dll4 was much higher than Th2 co-stimulatory molecule Jag1, and PRR ligand combinations did not increase Jag1 RNA expression over single PRR ligand-containing cultures (data not shown). TNF-α was the most abundant cytokine at the RNA level, with maximum responses seen for R848+p(I:C) and GLA+p(I:C). Most single PRR ligands were poor inducers of IL-12 (Figure 1) and IL-23 (data not shown) while ligand combinations generated
higher levels of these cytokine transcripts. Optimal stimulation of IL-12 and IL-23 was obtained with the R848+p(I:C) combination. IFN-α RNA was undetectable in cultures stimulated with individual ligands, with the exception of p(I:C), and detectable but low in cultures stimulated with several combinations
(data not shown). We then examined cell surface markers and
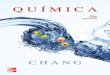
cytokines at the protein level by flow cytometry. The highest expression of activation marker CD86 was obtained using R848, with the response hierarchy being: R848 > GLA > TDB > p(I:C) > iE- DAP (Figure 2). Comparable CD86 expression was seen for most combinations containing R848 or GLA. The combination p(I:C)+GLA+TDB resulted in CD86 expression comparable to R848 (data not shown) although pairs of any of these ligands were lower.
We also determined the expression of the co-stimulatory molecules Dll4 and Jag1 by flow cytometry. Both R848 and GLA induced expression of Th1-polarizing Dll4 in a portion of CD86+ DCs (22% and 16%, respectively) (Figure 3). While both ligands also induced expression of Th2-polarizing Jag1 within CD86+ DCs, R848 alone induced a distinct subpopulation of cells that were CD86loJag1+. Clear synergy of Dll4 expression could be seen in R848+GLA cultures which displayed two discrete populations of CD86+ cells, one Dll4- and one Dll4+, and
Figure 2. Expression of CD86 activation marker by CD11c+ DCs stimulated with selected PRR ligands. Stimulation conditions: shaded boxes corresponding to stimulating ligands.
Figure 1. RNA expression of activation marker (CD80), co-stimulatory molecule (Dll1), cytokines (IL-12, TNF-alpha) by bmDCs stimulated with PRR ligands. Results expressed as fold-change of stimulated vs. unstimulated cultures.

a higher percentage of Dll4+ DCs (35.3%) than cultures stimulated with either ligand. Although not shown here, the highest Dll4 expression was observed for R848+GLA+iE-DAP-stimulated DCs.
Flow cytometry data for the CD86 activation marker indicated that while R848 is a potent activator of both conventional DCs (cDCs: CD11c+
CD45RA-) and plasmacytoid DCs (pDCs: CD11c+CD45RA+)(Figure 4, top right),
other PRR ligands were more effective activators of cDCs than pDCs, as exemplified by p(I:C) and GLA (Figure 4, bottom).
Using a multiplex assay for detection of secreted cytokines (Table 3), we found that R848 was the most potent PRR ligand for induction of T cell-activating cytokines, consistent with our other studies. High levels of the Th1 cytokines IL-12 and IFN-γ and the Th2 cytokine IL-6 were observed in R848 cultures. Th2 cytokines such as IL-4 and IL-10 were also detected in R848-stimulated cultures. Additive or synergistic responses were observed for several PRR ligand pairs, and further enhancement of IL-6 and IFN-γ were observed with certain triple ligand combinations.
Conclusions and Significance
Several patterns emerged from these in vitro DC stimulation studies. R848 proved to be the strongest inducer of DC activation in vitro. R848 stimulated high levels of TNF-α, IL-10, IL-6, and Dll4 transcription. R848 induced the highest CD86+
DC protein expression, which was not enhanced by other ligands. R848 stimulated DCs expressing Dll4 or Jag1 co-stimulatory molecules, suggesting that R848 promotes a mixed Th1/Th2 response. However, Dll4+ cells were found among CD86+ DCs while Jag1+ cells were found in both CD86+ and CD86lo DCs. In follow-up studies we will test whether Jag1+CD86lo DCs co-express CD80. Furthermore, R848 was effective in activating both cDCs and pDCs as measured by CD86 expression of CD11c+CD45RA- and CD11c+CD45RA+, respectively.
Finally, R848 was the most potent ligand for secretion of Th1 (IL-12, IFN-γ) and Th2 (IL-6, IL-4, IL-10) cytokines.
GLA was a strong inducer of IL-12, CD80, and TNF-α transcription and the second most potent inducer of CD86. In addition, GLA selectively stimulated Dll4 and Jag1 expression in CD86+ DCs. The association of GLA with a predominantly Th1 response [43] may be related to its lack of induction of the CD86loJag1+ subset.
Figure 3. Expression of co-stimulatory molecules Dll4 and Jag1 by DCs stimulated with selected PRR ligands. Control=unstimulated bmDCs.
Figure 4. CD86 expression of cDCs and pDCs stimulated with PRR ligands.

GLA preferentially activated cDCs over pDCs. While only low cytokine levels were detected with GLA alone, the GLA+R848 combination was synergistic for several cytokines including IL-6, IL-12, IFN-γ, TNF-α and IL-10.
Table 3. CD86 expression of cDCs and pDCs stimulated with PRR ligands.
Although several PRR ligands were individually ineffective in activating DCs, they enhanced specific aspects of DC differentiation when combined with other ligands. For example, R848+p(I:C) had the highest levels of IL-12, IL-23, and TNF-alphatranscription and was a strong inducer of IL-12, IFN-alpha and IL-6 secretion. This combination activated both cDCs and pDCs
similarly to R848. Other notable combinations included R848+GLA+iE-DAP, which induced the highest level of Dll4 expression, consistent with a highly Th1-polarized response. This was accompanied by enhanced levels of many secreted cytokines (IL-1β, IL-6, IL-10, IL-12, IFNγ, TNFα). Additional combinations inducing high cytokine secretion were R848+GLA+TDB and R848+iE-DAP+TDB. p(I:C)+GLA+TDB was the only combination lacking R848 that led to high levels of cytokine secretion and CD86 expression. Finally, p(I:C)+iE-DAP+TDB was the sole combination with high CD86 expression but low secreted cytokines.
pIC R84
8
IE-
DA
P
GL
A
TD
BIL-1 IL-10 IL-6 IL-12 IFN- TNF- IL-2 IL-414.3 6.2 1.8 8.8 2.9 2.3 6.1 8.6
x 14.3 9.5 3.9 32.0 2.9 3.4 6.1 11.2x 45.9 41.4 405.4 278.3 683.2 37.8 17.9 24.9
x 14.3 4.5 1.8 9.3 2.2 2.3 7.3 8.6x 14.3 6.2 18.5 35.2 7.7 11.3 7.3 10.3
x 11.0 6.2 2.2 19.3 N/A 7.0 4.9 8.6x x 59.9 78.6 748.1 424.1 1350.6 80.1 22.9 38.4x x 11.0 6.2 5.2 36.9 1.9 3.4 4.9 6.8x x 17.2 9.5 44.8 75.5 8.8 19.4 8.2 10.3x x 14.3 6.2 4.2 36.1 2.2 6.2 4.9 8.6
x x 50.7 52.3 630.3 371.8 829.3 54.9 20.2 30.8x x 55.3 59.0 741.1 384.3 759.8 77.7 22.0 36.8x x 55.3 90.2 714.4 418.1 979.5 74.3 21.7 34.2
x x 11.0 6.2 30.6 40.9 12.5 13.7 7.3 11.2x x 7.7 N/A 1.8 15.9 ND 5.3 ND 6.0
x x 14.3 6.2 44.8 60.6 11.0 25.4 4.9 8.6x x x 11.0 6.2 31.1 34.8 9.9 15.0 4.9 9.5
x x x 66.6 86.4 1089.8 482.4 1168.3 126.7 25.8 46.0x x x 57.6 72.1 817.6 435.5 1240.3 79.7 23.4 37.6x x x 57.6 60.3 928.1 402.7 1068.5 91.4 24.0 41.0
x x x 50.7 52.3 801.3 338.3 859.3 71.8 22.0 33.0x x x 7.7 2.8 28.9 35.2 7.2 16.9 4.9 9.5

A repeat of the flow cytometry experiment with the added time point of 8 hours post stimulation revealed some further features. poly(I:C)+R848+iE-DAP and poly(I:C)+R848+GLA induced the most number of CD86+Dll4+ cells at 8 hours. However, at 24 hours, R848+iE-DAP+GLA and R848+iE-DAP+TDB overtook them and had the highest percentages of CD86+Dll4+ cells. A possible explanation for the faster up-regulation of CD86 and Dll4 by poly(I:C)+R848+iE-DAP and poly(I:C)+R848+GLA is therelease of type 1 interferons induced by poly(I:C) and R848, as reported in other studies. Indeed, the combination poly(I:C)+R848 induced one of the highest levels of CD86 and Dll4, and one of the highest levels of cytokines as well. The fact that R848+iE-DAP+GLA-stimulated cells, for example, continued increasing their levels CD86 and Dll4, beyond that of poly(I:C)+R848+iE-DAP and poly(I:C)+R848+GLAstimulated cells, suggests that in addition to IFN-α signalling, there are other, slower-acting signaling pathways that are important for CD86 and Dll4 expression.
The kinetics of expression of activation markers on DCs may be important in shaping a Th1 v. Th2 immune profile. Recent studies suggest that [50] when APCs present antigen to T-cells before the APCs have up-regulated such molecules as CD86, those T-cells become Th2 or regulatory T-cells, and are able to abrogate Th1 immunity to a subsequent immunization. Therefore a quick DC activation might be desirable for a Th1 response. On the other hand, a quick activation followed by an earlier exhausted phenotype may not be better than a slower response with more sustained activation kinetics. Differences in kinetics might result in subtle differences in immunogenicity, at which point formulation issues might be more important than which PAMP combinations are used.
In summary of the results so far obtained, there are about five distinct DC activation phenotypes that are qualitatively different in protein and cytokine expression and kinetics, and which may result in different immune responses in vivo (Table 4). The first contains a population of CD86-Jag1+ cells. R848 alone induces the greatest proportion of these cells. The second contains high levels of CD86 and Dll4, coexpressed, but low to mid levels of various cytokines. iE-DAP+GLA+TDB was the lone combination inducing this group phenotype. The third phenotype contains the highest levels and numbers of CD86+Dll4+ cells after 24 hours of stimulation. This is induced by the R848+iE-DAP+GLA combination. The fourth contains high levels of CD86 but very low levels of Dll4. poly(I:C)+iE-DAP+TDB induced this phenotype. Low levels of cytokines were induced by this combination, as well. Finally, the fifth phenotype is a rapid up-regulation of CD86 and Dll4 (ie. the highest levels at 8 hours post stimulation), followed by a modest increase of these proteins, such that 24 hours post-stimulation, the cells have high, but not the very highest, levels of CD86 and Dll4. This phenotype kinetics is exemplified by poly(I:C)+R848+iE-DAP stimulation, followed in potency by poly(I:C)+R848+GLA stimulation (Table 4).
Figure 5.

Table 4. Phenotypes of bm-DCs stimulated by PAMP combinations
Phenotype of stimulated bm-DCs
PAMP combinationinducing the
prototype phenotype
Generalizations of PAMP combinations inducing this phenotype
large population of CD86-
Jag1+ cells; mid to high levels of cytokines
R848 inclusion of R848; combining other PRR ligands with R848 reduces CD86-Jag1+ population.
large population of CD86+Dll4+ cells; low levels of cytokines
iE-DAP+GLA+TDB
non-inclusion of R848 and non-inclusion of poly(I:C) in combination with GLA leads to low cytokine levels. iE-DAP+GLA+TDB was the lone tested combination that synergized for CD86, Dll4 coexpression without high cytokine production.
large population of CD86+Dll4+ cells; high levels of cytokines
R848+iE-DAP+GLA
R848 and GLA synergized for high CD86, Dll4 co-expression and cytokine production. Adding iE-DAP induced the highest tested CD86, Dll4 levels; while adding TDB induced the highest tested cytokine levels.
large population of CD86+Dll4- cells; small population of Dll4+ cells; low levels of cytokines
poly(I:C)+iE-DAP+TDB
non-inclusion of R848 and GLA resulted in low Dll4 levels; and poly(I:C), iE-DAP, and TDB do not synergize to induce Dll4 production.
rapid up-regulation of CD86 and Dll4 (8 hr post-stimulation), followed by modest (ie. relatively slow) increases of these markers.
poly(I:C)+R848+iE-DAP
inclusion of the poly(I:C)+R848 combination led to rapid upregulation of CD86 and Dll4. However, the slower but steadier upregulation by R848+iE-DAP+GLA resulted in a comparatively larger CD86+Dll4+ population after 24 hours of stimulation.
Each of the PAMP combinations exemplifying the five different phenotypes could potentially be the best adjuvant for a particular type of immune response. Different types of immune responses in vivo may include (1) a primarily CD8+ cytotoxic T-cell response, (2) a primarily high antibody response, with Ab specificities and isotypes favoring neutralization, immune complexes, and other predominantly non-cell-mediated mechanisms, (3) a high antibody response of the cytophilic variety, accompanied by an increase in particular innate effector cells which are dependent on the cytophilic antibodies to carry out its function, and (4) any combination of these, with different longevities of adaptive immune memory cells, and different predominances of different cells, cell subtypes, antibody isotypes, and mechanisms such as the role of complement.
Based on the above data, we propose to use selected PRR ligand combinations for mouse vaccination studies. C57BL/6 mice will be immunized with MSP1.42 and PRR ligands in an oil-in-wateremulsion [52] or encapsulated in biodegradable nanoparticles such as poly(lactic-co-glycolic acid) (PGLA). Mice will be immunized at 3 wk intervals for a total of 3 immunizations. Blood samples will be collected before and 2 wks after immunization. Serum antibody titers and IgG subclasses will be measured by ELISA. Splenic T cells will be re-stimulated with MSP1.42 in vitro [53] and secreted

cytokines measured using a multiplex cytokine kit. We also will evaluate lymph nodes to determine if DC and T cell activation has occurred.
We also plan to do the malaria ADRB assay, which has not been attempted in animals in the literature before. It is possible that this assay will better correlate with protection than the traditional measures of ELISA titers and GIA activity.
We plan to do some in vitro functional T-cell priming assays with selected PRR ligand combinations. One possibility is the allogeneic and syngeneic mixed lymphocyte reaction. The mixed lymphocyte reaction can be performed by putting irradiated (non-proliferating) stimulator cells in culture with responder cells marked with a dye to measure proliferation. The responder cells are a mixed population of lymphocytes (usually the buffy coat fraction of a splenocyte suspension). An allogeneic MLR uses stimulator cells from a slightly different MHC allelic background than that of the responder cells. A syngeneic MLR uses stimulator and responder cells with the same MHC allelic background. Usually, syngeneic MLR proliferation is quite low compared to allogeneic MLR proliferation. However, with the use of stimulator cells that have been pre-stimulated with various PAMP combinations, syngeneic stimulation may be enhanced.
Studies have suggested that immunogenic events, such as the response to leukemia, can trigger auto-immune responses, which can be measured by the syngeneic mixed lymphocyte reaction [51]. An extrapolation of this conclusion is that allogeneic reactivity is associated with inflammatory recognition of foreign MHC-peptide pairs while syngeneic reactivity is associated with inflammatory recognition of self MHC-peptide pairs. Allogeneic and syngeneic MLRs will be performed using stimulator cells pre-cultured (for 8h and 24h) with various PRR ligand combinations. The MLRs will be analyzed by looking at proliferation as well as secreted cytokines using a Luminex assay. My hypothesis is that high proliferation in the allogeneic MLR will correlate with antigen-specific T-cell immunogenicity in vivo, and that high proliferation in the syngeneic MLR will correlate with non-specific immunogenicity (ie. toxic reactogenicity and auto-immunity) in vivo. Of greatest interest would be an adjuvant combination that elicited low proliferation in the syngeneic MLR while inducing high proliferation in the allogeneic MLR.

References Cited:
Chang, Sandra Perreira. COBRE Renewal, Research Plan. 2012. (unpublished)[1] W.H. Organization, World malaria report 2011, Geneva: World Health Organization 246 (2011).[2] I. Vythilingam, Y.M. NoorAzian, T.C. Huat, A.I. Jiram, Y.M. Yusri, A.H. Azahari, I. NorParina, A. NoorRain, S. LokmanHakim, Plasmodium knowlesi in humans, macaques and mosquitoes in peninsular Malaysia, Parasit Vectors 1 (2008) 26.[3] N.J. White, Plasmodium knowlesi: The Fifth Human Malaria Parasite, Clinical Infectious Diseases 46 (2008) 172-173.[4] S.I. Hay, C.A. Guerra, A.J. Tatem, A.M. Noor, R.W. Snow, The global distribution and population at risk of malaria: past, present, and future, The Lancet Infectious Diseases 4 (2004) 327-336.[5] A. Hamoudi, J. Sachs, The changing global distribution of malaria: a review, Center for International Development, Harvard University, 1999.[6] P.L. Alonso, S.W. Lindsay, J.R.M.A. Schellenberg, K. Keita, P. Gomez, F.C. Shenton, A.G. Hill, P.H. David, G. Fegan, K. Cham, B.M. Greenwood, A malaria control trial using insecticide-treated bed nets and targeted chemoprophylaxis in a rural area of The Gambia, West Africa: 6. The impact of the interventions on mortality and morbidity from malaria, Transactions of the Royal Society of Tropical Medicine and Hygiene 87, Supplement 2 (1993) 37-44.[7] C.G. Nevill, E.S. Some, V.O. Mung'ala, W. Muterni, L. New, K. Marsh, C. Lengeler, R.W. Snow, Insecticide-treated bednets reduce mortality and severe morbidity from malaria among children on the Kenyan coast, Tropical Medicine & International Health 1 (1996) 139-146.[8] K. Mendis, A. Rietveld, M. Warsame, A. Bosman, B. Greenwood, W.H. Wernsdorfer, From malaria control to eradication: The WHO perspective, Tropical Medicine & International Health 14 (2009) 802-809.[9] S.C.T.P. The RTS, First Results of Phase 3 Trial of RTS,S/AS01 Malaria Vaccine in African Children, New England Journal of Medicine 365 (2011) 1863-1875.[10] L. Florens, M.P. Washburn, J.D. Raine, R.M. Anthony, M. Grainger, J.D. Haynes, J.K. Moch, N. Muster, J.B. Sacci, D.L. Tabb, A.A. Witney, D. Wolters, Y. Wu, M.J. Gardner, A.A. Holder, R.E. Sinden, J.R. Yates, D.J. Carucci, A proteomic view of the Plasmodium falciparum life cycle, Nature 419 (2002) 520-526.[11] T. Smith, I. Felger, M. Tanner, H.P. Beck, 11. Premunition in Plasmodium falciparum infection: insights from the epidemiology of multiple infections, Transactions of the Royal Society of Tropical Medicine and Hygiene 93 (1999) 59-64.[12] J.L. Pérignon, P. Druilhe, Immune mechanisms underlying the premunition against Plasmodium falciparum malaria, Memórias do Instituto Oswaldo Cruz 89 (1994) 51-53.[13] J.M. Vinetz, R.H. Gilman, Asymptomatic Plasmodium parasitemia and the ecology of malaria transmission, The American Journal of Tropical Medicine and Hygiene 66 (2002) 639-640.[14] C.J.A. Duncan, S.H. Sheehy, K.J. Ewer, A.D. Douglas, K.A. Collins, F.D. Halstead, S.C. Elias, P.J. Lillie, K. Rausch, J. Aebig, K. Miura, N.J. Edwards, I.D. Poulton, A. Hunt-Cooke, D.W. Porter, F.M. Thompson, R. Rowland, S.J. Draper, S.C. Gilbert, M.P. Fay, C.A. Long, D. Zhu, Y. Wu, L.B. Martin, C.F. Anderson, A.M. Lawrie, A.V.S. Hill, R.D. Ellis, Impact on Malaria Parasite Multiplication Rates in Infected Volunteers of the Protein-in-Adjuvant Vaccine AMA1-C1/Alhydrogel+CPG 7909, PLoS ONE 6 (2011) e22271.[15] S. Singh, K. Miura, H. Zhou, O. Muratova, B. Keegan, A. Miles, L.B. Martin, A.J. Saul, L.H. Miller, C.A. Long, Immunity to Recombinant Plasmodium falciparum Merozoite Surface Protein 1 (MSP1): Protection in Aotus nancymai Monkeys Strongly Correlates with Anti-MSP1 Antibody Titer and In Vitro Parasite-Inhibitory Activity, Infection and Immunity 74 (2006) 4573-4580.

[16] S. Dutta, J.S. Sullivan, K.K. Grady, J.D. Haynes, J. Komisar, A.H. Batchelor, L. Soisson, C.L. Diggs, D.G. Heppner, D.E. Lanar, W.E. Collins, J.W. Barnwell, High Antibody Titer against Apical Membrane Antigen-1 Is Required to Protect against Malaria in the Aotus Model, PLoS ONE 4 (2009) e8138.[17] P. Druilhe, H. Bouharoun-Tayoun, Antibody-dependent cellular inhibition assay, Methods in molecular medicine 72 (2002) 529-534.[18] C. Joos, Antibody dependent oxidative burst and phagocytosis of Plasmodium falciparum merozoites by activated neutrophils: a functional antibody assay for malaria vaccine candidates[19] H. Bouharoun-Tayoun, P. Attanath, A. Sabchareon, T. Chongsuphajaisiddhi, P. Druilhe, Antibodies that protect humans against Plasmodium falciparum blood stages do not on their own inhibit parasite growth and invasion in vitro, but act in cooperation with monocytes, J Exp Med 172 (1990) 1633-1641.[20] D.K. Moss, E.J. Remarque, B.W. Faber, D.R. Cavanagh, D.E. Arnot, A.W. Thomas, A.A. Holder, Plasmodium falciparum 19-Kilodalton Merozoite Surface Protein 1 (MSP1)-Specific Antibodies That Interfere with Parasite Growth In Vitro Can Inhibit MSP1 Processing, Merozoite Invasion, and Intracellular Parasite Development, Infection and Immunity 80 (2012) 1280-1287.[21] K. Crompton Pd Fau - Miura, B. Miura K Fau - Traore, K. Traore B Fau - Kayentao, A. Kayentao K Fau - Ongoiba, G. Ongoiba A Fau - Weiss, S. Weiss G Fau - Doumbo, D. Doumbo S Fau - Doumtabe, Y. Doumtabe D Fau - Kone, C.-Y. Kone Y Fau - Huang, O.K. Huang Cy Fau - Doumbo, L.H. Doumbo Ok Fau -Miller, C.A. Miller Lh Fau - Long, S.K. Long Ca Fau - Pierce, S.K. Pierce, In vitro growth-inhibitory activity and malaria risk in a cohort study in mali.[22] E.E.H. Murhandarwati, L. Wang, H.D. de Silva, C. Ma, M. Plebanski, C.G. Black, R.L. Coppel, Growth-Inhibitory Antibodies Are Not Necessary for Protective Immunity to Malaria Infection, Infection and Immunity 78 (2010) 680-687.[23] H. Bouharoun-Tayoun, C. Oeuvray, F. Lunel, P. Druilhe, Mechanisms underlying the monocyte-mediated antibody-dependent killing of Plasmodium falciparum asexual blood stages, J Exp Med 182 (1995) 409-418.[24] C. Joos, L. Marrama, H.E.J. Polson, S. Corre, A.-M. Diatta, B. Diouf, J.-F. Trape, A. Tall, S. Longacre, R. Perraut, Clinical Protection from Falciparum Malaria Correlates with Neutrophil Respiratory Bursts Induced by Merozoites Opsonized with Human Serum Antibodies, PLoS ONE 5 (2010) e9871.[25] C.A. Bonville, C.M. Percopo, K.D. Dyer, J. Gao, C. Prussin, B. Foster, H.F. Rosenberg, J.B. Domachowske, Interferon-gamma coordinates CCL3-mediated neutrophil recruitment in vivo, BMC Immunol, England, 2009, p. 14.[26] R. Appelberg, Interferon‐gamma (IFN‐γ) and macrophage inflammatory proteins (MIP)‐1 and‐2 are involved in the regulation of the T cell‐dependent chronic peritoneal neutrophilia of mice infected with mycobacteria, Clinical & Experimental Immunology 89 (1992) 269-273.[27] B. Genton, I. Betuela, I. Felger, F. Al-Yaman, R.F. Anders, A. Saul, L. Rare, M. Baisor, K. Lorry, G.V. Brown, D. Pye, D.O. Irving, T.A. Smith, H.P. Beck, M.P. Alpers, A recombinant blood-stage malaria vaccine reduces Plasmodium falciparum density and exerts selective pressure on parasite populations in a phase 1-2b trial in Papua New Guinea, J Infect Dis, United States, 2002, pp. 820-827.[28] K.M. Pusic, C.N. Hashimoto, A. Lehrer, C. Aniya, D.E. Clements, G.S. Hui, T cell epitope regions of the P. falciparum MSP1-33 critically influence immune responses and in vitro efficacy of MSP1-42 vaccines, PLoS One, United States, 2011, p. e24782.[29] D. Skokos, M. Nussenzweig, CD8− DCs induce IL-12–independent Th1 differentiation through Delta 4 Notch-like ligand in response to bacterial LPS.[30] M. Okamoto, H. Matsuda, A. Joetham, J.J. Lucas, J. Domenico, K. Yasutomo, K. Takeda, E.W. Gelfand, Jagged1 on Dendritic Cells and Notch on CD4+ T Cells Initiate Lung Allergic Responsiveness by Inducing IL-4 Production, The Journal of Immunology 183 (2009) 2995-3003.

[31] B. Bleck, D.B. Tse, T. Gordon, M.R. Ahsan, J. Reibman, Diesel exhaust particle-treated human bronchial epithelial cells upregulate Jagged-1 and OX40 ligand in myeloid dendritic cells via thymic stromal lymphopoietin, J Immunol, United States, 2010, pp. 6636-6645.[32] D. Amsen, A. Antov, R.A. Flavell, The different faces of Notch in T-helper-cell differentiation, Nat Rev Immunol 9 (2009) 116-124.[33] N. Kassner, M. Krueger, H. Yagita, A. Dzionek, A. Hutloff, R. Kroczek, A. Scheffold, S. Rutz, Cutting Edge: Plasmacytoid Dendritic Cells Induce IL-10 Production in T Cells via the Delta-Like-4/Notch Axis, The Journal of Immunology 184 (2010) 550-554.[34] S. Rutz, M. Janke, N. Kassner, T. Hohnstein, M. Krueger, A. Scheffold, Notch regulates IL-10 production by T helper 1 cells, Proceedings of the National Academy of Sciences 105 (2008) 3497-3502.[35] S. Mukherjee, M.A. Schaller, R. Neupane, S.L. Kunkel, N.W. Lukacs, Regulation of T cell activation by Notch ligand, DLL4, promotes IL-17 production and Rorc activation, J Immunol 182 (2009) 7381-7388.[36] C.-T. Ong, J.R. Sedy, K.M. Murphy, R. Kopan, Notch and Presenilin Regulate Cellular Expansion and Cytokine Secretion but Cannot Instruct Th1/Th2 Fate Acquisition, PLoS ONE 3 (2008) e2823.[37] R. Lisak, J. Benjamins, B. Bealmear, L. Nedelkoska, D. Studzinski, E. Retland, B. Yao, S. Land, Differential effects of Th1, monocyte/macrophage and Th2 cytokine mixtures on early gene expression for molecules associated with metabolism, signaling and regulation in central nervous system mixed glial cell cultures, Journal of Neuroinflammation 6 (2009) 4.[38] W. Elyaman, E.M. Bradshaw, Y. Wang, M. Oukka, P. Kivisakk, S. Chiba, H. Yagita, S.J. Khoury, JAGGED1 and delta1 differentially regulate the outcome of experimental autoimmune encephalomyelitis, J Immunol, United States, 2007, pp. 5990-5998.[39] M.F. Good, D.C. Kaslow, L.H. Miller, Pathways and strategies for developing a malaria blood-stage vaccine, Annu Rev Immunol 16 (1998) 57-87.[40] F. Engelbrecht, I. Felger, B. Genton, M. Alpers, H.P. Beck, Plasmodium falciparum: malaria morbidity is associated with specific merozoite surface antigen 2 genotypes, Exp Parasitol, United States, 1995, pp. 90-96.[41] Q. Zhu, C. Egelston, A. Vivekanandhan, S. Uematsu, S. Akira, D.M. Klinman, I.M. Belyakov, J.A. Berzofsky, Toll-like receptor ligands synergize through distinct dendritic cell pathways to induce T cell responses: implications for vaccines, Proc Natl Acad Sci U S A, United States, 2008, pp. 16260-16265.[42] G. Napolitani, A. Rinaldi, F. Bertoni, F. Sallusto, A. Lanzavecchia, Selected Toll-like receptor agonist combinations synergistically trigger a T helper type 1-polarizing program in dendritic cells, Nat Immunol, United States, 2005, pp. 769-776.[43] R.N. Coler, S. Bertholet, M. Moutaftsi, J.A. Guderian, H.P. Windish, S.L. Baldwin, E.M. Laughlin, M.S. Duthie, C.B. Fox, D. Carter, M. Friede, T.S. Vedvick, S.G. Reed, Development and characterization of synthetic glucopyranosyl lipid adjuvant system as a vaccine adjuvant., PLoS One 6 (2011) e16333.[44] H.R. Bohnenkamp, K.T. Papazisis, J.M. Burchell, J. Taylor-Papadimitriou, Synergism of Toll-like receptor-induced interleukin-12p70 secretion by monocyte-derived dendritic cells is mediated through p38 MAPK and lowers the threshold of T-helper cell type 1 responses, Cell Immunol 247 (2007) 72-84.[45] F. Heil, H. Hemmi, H. Hochrein, F. Ampenberger, C. Kirschning, S. Akira, G. Lipford, H. Wagner, S. Bauer, Species-specific recognition of single-stranded RNA via toll-like receptor 7 and 8., Science 303 (2004) 1526-1529.[46] J.H. Fritz, L. Le Bourhis, G. Sellge, J.G. Magalhaes, H. Fsihi, T.A. Kufer, C. Collins, J. Viala, R.L. Ferrero, S.E. Girardin, D.J. Philpott, Nod1-mediated innate immune recognition of peptidoglycan contributes to the onset of adaptive immunity, Immunity 26 (2007) 445-459.[47] M.J. Marakalala, L.M. Graham, G.D. Brown, The role of Syk/CARD9-coupled C-type lectin receptors in immunity to Mycobacterium tuberculosis infections., Clin Dev Immunol 2010 (2010) 567571.[48] M.W. Pfaffl, A new mathematical model for relative quantification in real-time RT-PCR.

[49] S.H. Naik, P. Sathe, H.-Y. Park, D. Metcalf, A.I. Proietto, A. Dakic, S. Carotta, M. O'Keeffe, M. Bahlo, A. Papenfuss, J.-Y. Kwak, L. Wu, K. Shortman, Development of plasmacytoid and conventional dendritic cell subtypes from single precursor cells derived in vitro and in vivo, Nat Immunol 8 (2007) 1217-1226.[50] A.T. Kamath, B. Mastelic, D. Christensen, A.-F. Rochat, E.M. Agger, D.D. Pinschewer, P. Andersen, P.-H. Lambert, C.-A. Siegrist, Synchronization of Dendritic Cell Activation and Antigen Exposure Is Required for the Induction of Th1/Th17 Responses, The Journal of Immunology 188 (2012) 4828-4837.[51] R.G. Devlin, J.D. McCurdy, P.E. Baronowsky, MIXED LYMPHOCYTE REACTIVITY AGAINST NORMAL CELLS BY SPLENIC LYMPHOCYTES FROM TUMOR-BEARING MICE, The Journal of Experimental Medicine 139 (1974) 230-237.[52] C.B. Fox, R.C. Anderson, T.S. Dutill, Y. Goto, S.G. Reed, T.S. Vedvick, Monitoring the effects of component structure and source on formulation stability and adjuvant activity of oil-in-water emulsions, Colloids Surf B Biointerfaces, Netherlands, 2008, pp. 98-105.[53] S.L. Baldwin, N. Shaverdian, Y. Goto, M.S. Duthie, V.S. Raman, T. Evers, F. Mompoint, T.S. Vedvick, S. Bertholet, R.N. Coler, S.G. Reed, Enhanced humoral and Type 1 cellular immune responses with Fluzone adjuvanted with a synthetic TLR4 agonist formulated in an emulsion, Vaccine, Netherlands, 2009, pp. 5956-5963.