Embed Size (px)
Citation preview
Marion Rabant1 MD, Canaud G2 MD, François A3 MD, Noël LH1 MD
(1) Pathology Department, Necker Hospital, Paris, France(2) Transplantation Department, Necker Hospital, Paris, France(3) Pathology Department, Rouen Hospital, Rouen, France
Severe vascular lesions and poor functional outcome in a kidney transplant recipient
CASE 4
Seite 2
50 year old caucasian woman
Medical history: Single functioning kidneySpontaneous abortion at the age of 25Brutal nephrotic syndrom at the age of 28
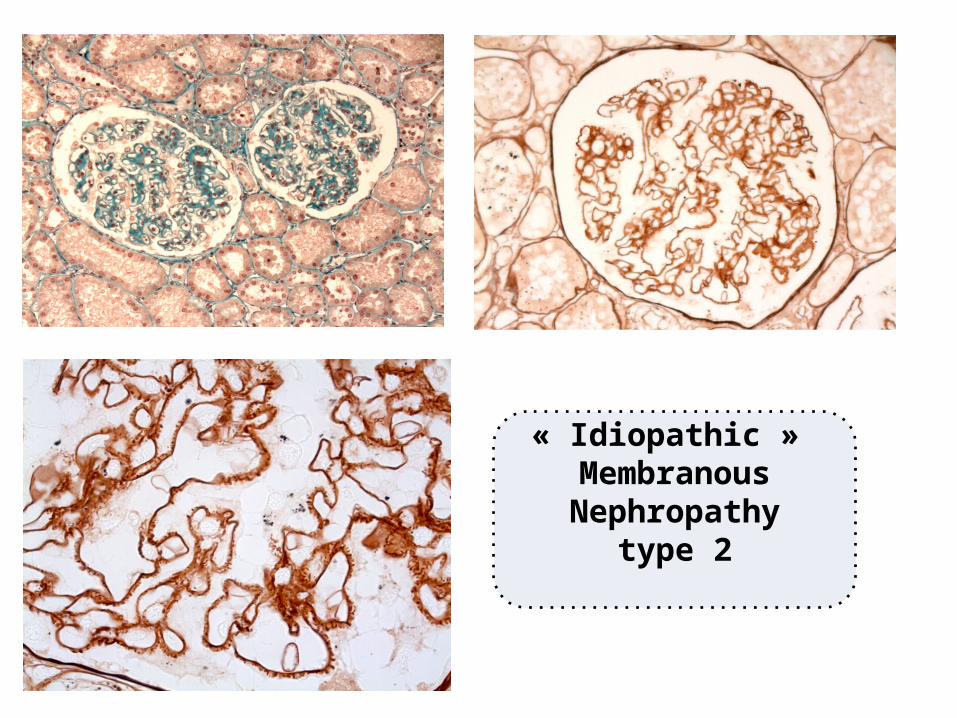
Kidney biopsy
CASE REPORTCASE REPORT
« Idiopathic » Membranous Nephropathy
type 2

Seite 3
CASE REPORTCASE REPORT
Rapidly progressive chronic kidney diseaseEnd stage renal disease at the age of 41 years
First kidney transplantation one year later
50 year old caucasian woman
Medical history: Single functioning kidney Spontaneous abortion at the age of 25 Brutal nephrotic syndrome at the age of 28
Kidney biopsy
Seite 4
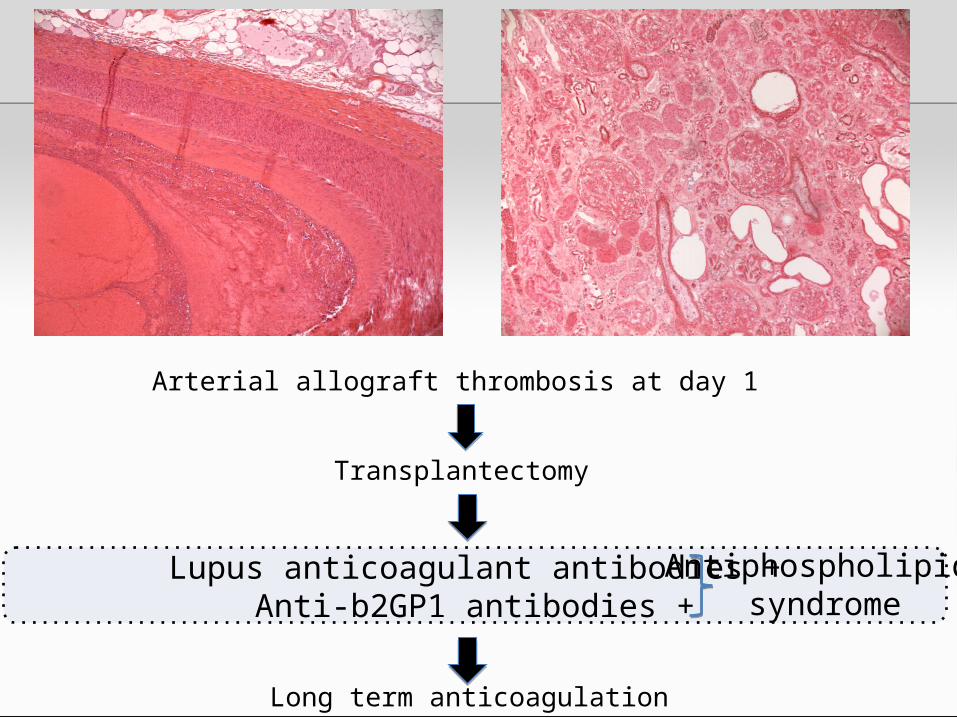
Arterial allograft thrombosis at day 1
Transplantectomy
Long term anticoagulation
Lupus anticoagulant antibodies +Anti-b2GP1 antibodies +
Antiphospholipid
syndrome
Seite 5
CASE REPORTCASE REPORT
8 years later at the age of 50Second kidney transplantation64-year-old deceased donor (ECD)
Immunosuppressive regimen: Thymoglobulin induction, Plasmapheresis and IVIG (x4) for anti HLA class I DSA Steroids, MMF, Tacrolimus
No day-0 biopsy
Seite 6
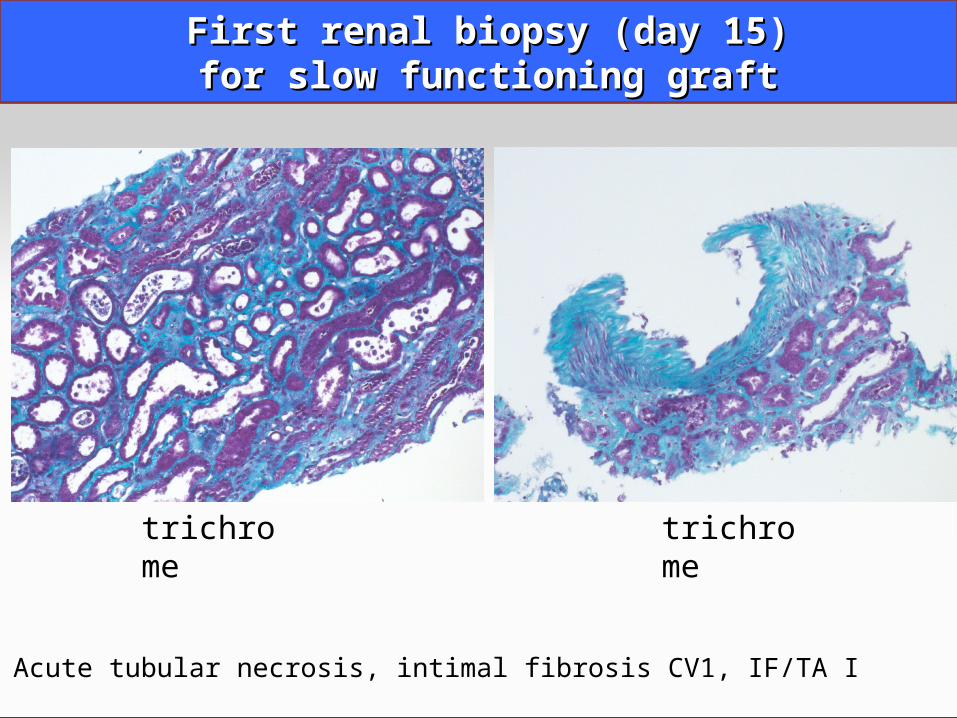
First renal biopsy (day 15)First renal biopsy (day 15)for slow functioning graftfor slow functioning graft
Acute tubular necrosis, intimal fibrosis CV1, IF/TA I
trichrome trichrome

Vacuoles
cv2
IF/TAGrade II
Tubular necrosis
Trichrome
Creatinine 120 umol/LGFR 40 mL/min
3-months protocol biopsy
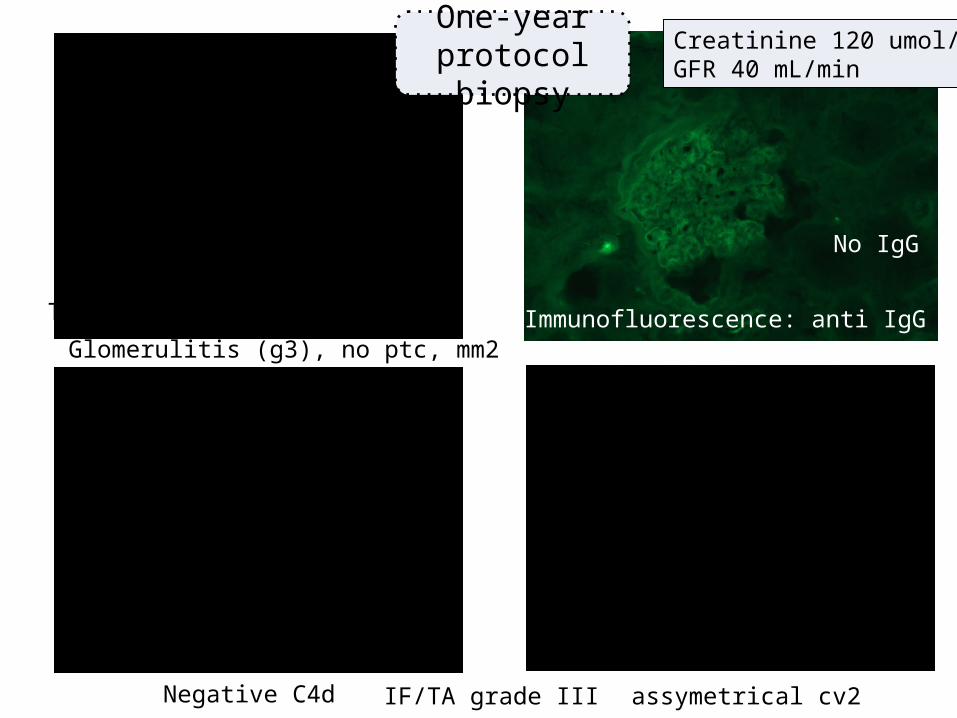
Glomerulitis (g3), no ptc, mm2
No IgG
Negative C4d assymetrical cv2
Trichrome
PAS
Immunofluorescence: anti IgG
C4d
IF/TA grade III
One-yearprotocol biopsy
Creatinine 120 umol/LGFR 40 mL/min
Seite 9
CASE REPORTCASE REPORT
Conclusion: sub-clinical acute humoral rejection
Treatment with:•Steroids•Plasmapheresis (x5)•Rituximab•Intravenous immunoglobulin (x4)
Trichrome
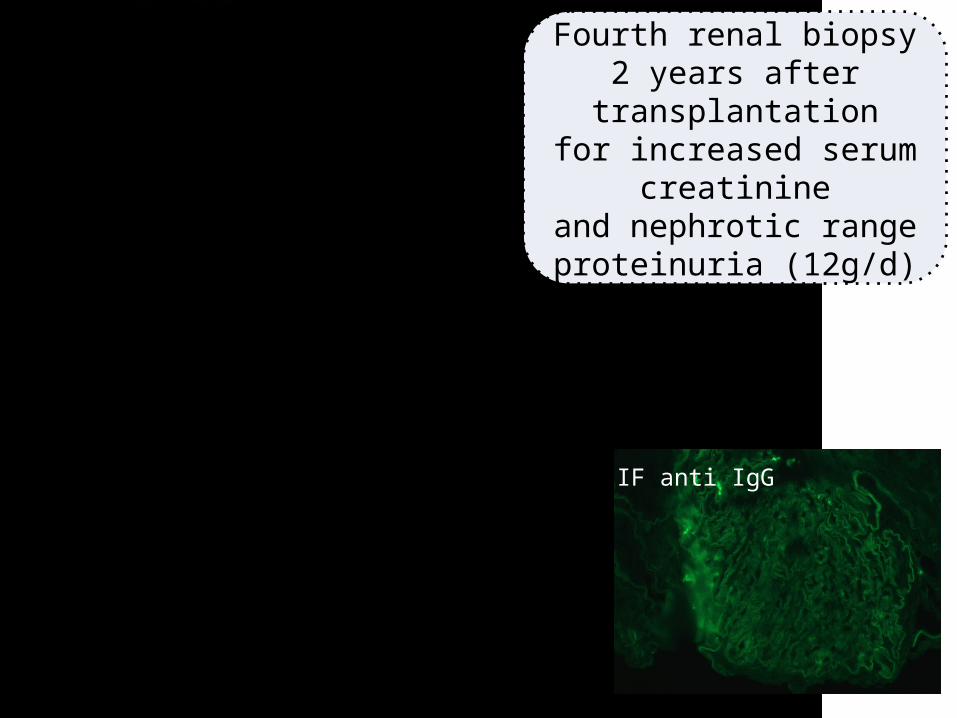
Fourth renal biopsy 2 years after transplantation
for increased serum creatinine
and nephrotic range proteinuria (12g/d)
IF anti IgG
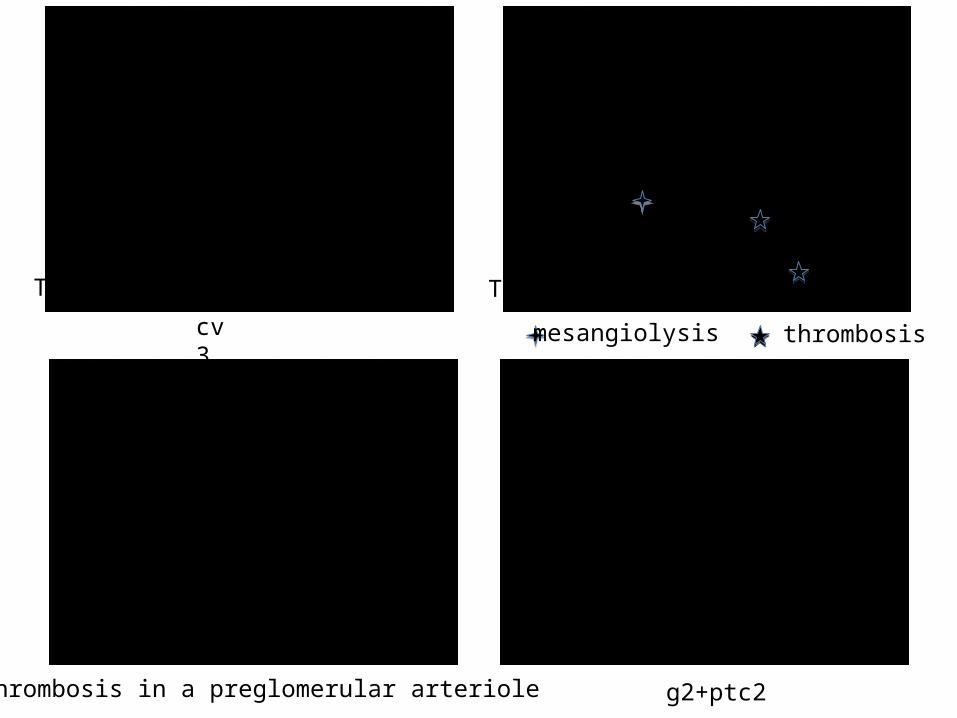
cv3 mesangiolysis thrombosis
g2+ptc2Thrombosis in a preglomerular arteriole
Trichrome Trichrome
Jones
Seite 12
CASE REPORTCASE REPORT
Conclusion of the 4th biopsy
Persistent acute humoral rejection
Thrombotic microangiopathy
Severe fibrous intimal hyperplasia
No recurrence of membranous nephropathy
Recurrence ofAPS nephropathy
Creatinine 230 μmol/LNephrotic range proteinuria
Seite 13
Antiphospholipid syndrom (APS) and kidneyAntiphospholipid syndrom (APS) and kidney
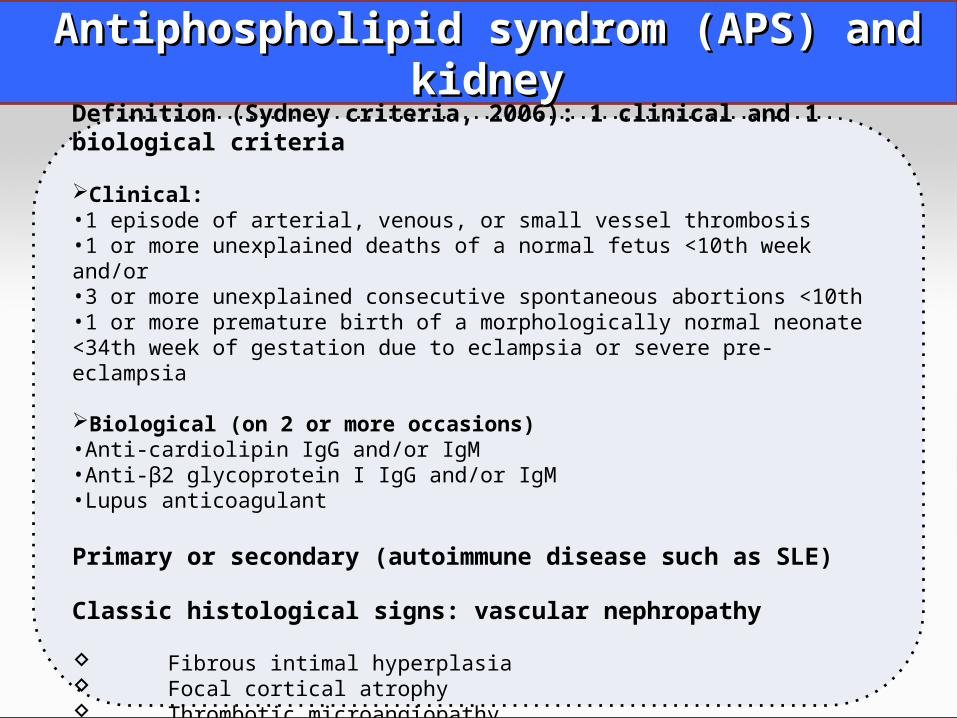
Definition (Sydney criteria, 2006): 1 clinical and 1 biological criteria
Clinical:•1 episode of arterial, venous, or small vessel thrombosis•1 or more unexplained deaths of a normal fetus <10th week and/or•3 or more unexplained consecutive spontaneous abortions <10th•1 or more premature birth of a morphologically normal neonate <34th week of gestation due to eclampsia or severe pre-eclampsia
Biological (on 2 or more occasions)•Anti-cardiolipin IgG and/or IgM•Anti-β2 glycoprotein I IgG and/or IgM•Lupus anticoagulant
Primary or secondary (autoimmune disease such as SLE)
Classic histological signs: vascular nephropathy
Fibrous intimal hyperplasia Focal cortical atrophy Thrombotic microangiopathy
Seite 14
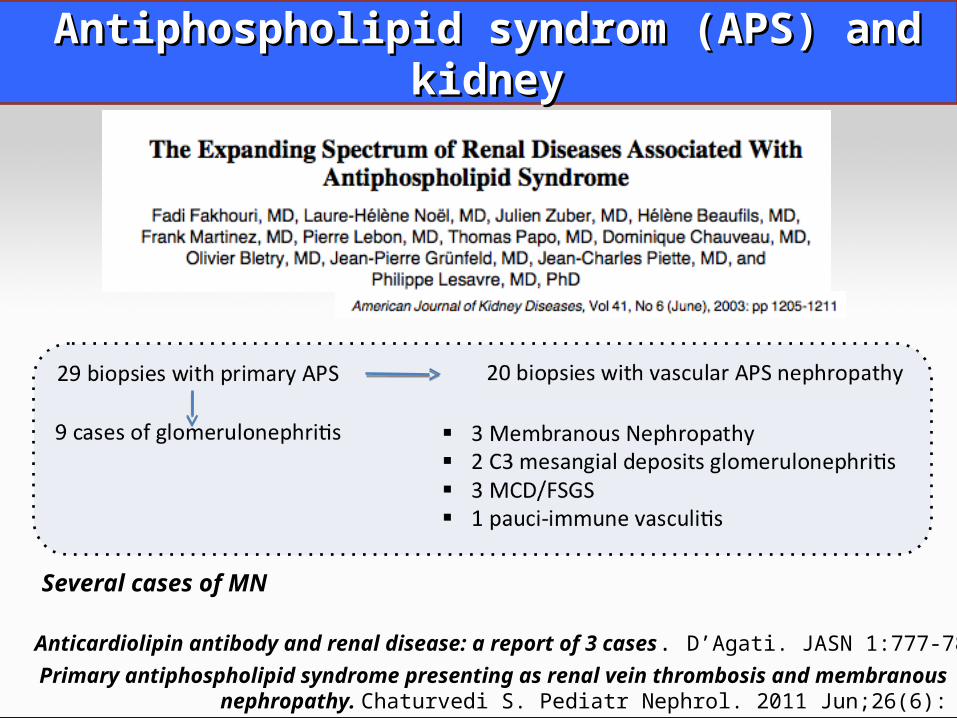
Antiphospholipid syndrom (APS) and kidneyAntiphospholipid syndrom (APS) and kidney
Primary antiphospholipid syndrome presenting as renal vein thrombosis and membranous nephropathy. Chaturvedi S. Pediatr Nephrol. 2011 Jun;26(6):
Several cases of MN
Anticardiolipin antibody and renal disease: a report of 3 cases. D’Agati. JASN 1:777-784, 1990

Seite 15
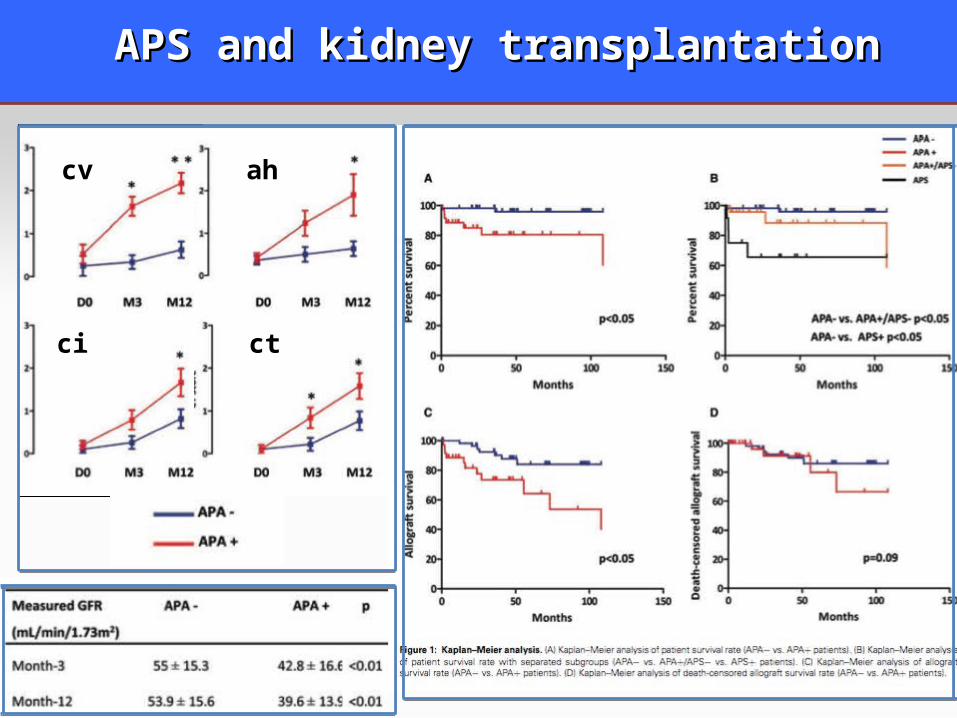
APS and kidney transplantationAPS and kidney transplantation
1359 transplantations (January 1, 2000 and Decembre 31, 2009)
AP antibodies (APA+)n=37 (2,7%)
APS n=12
Primary APSn=3
Secondary APSN=9
APA+n=25
• Lupus anticoagulantn=37/37 (100%)• Anti β2GP1 (n=7/37)• Anti CL (n=11/37)
Compared to 59 matched APA- transplant recipients
Canaud G, et al
To assess the long term clinical and histological significance of APA+ and APS
Seite 16
cv ah
ci ct
cv ah
ci ct
APS and kidney transplantationAPS and kidney transplantation
Seite 17
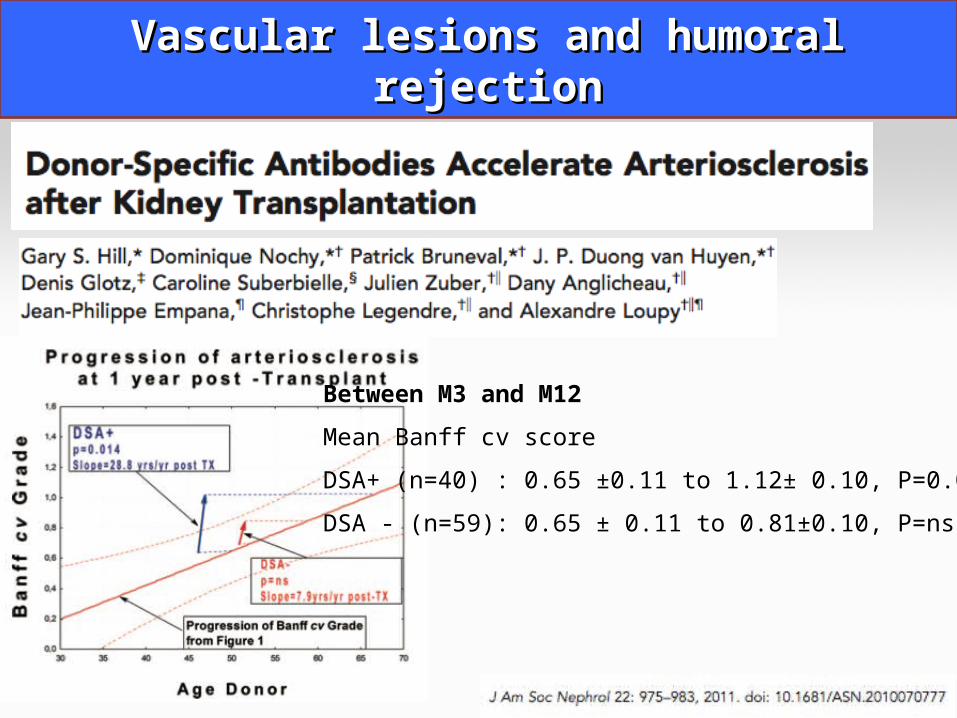
Vascular lesions and humoral rejectionVascular lesions and humoral rejection
Between M3 and M12
Mean Banff cv score
DSA+ (n=40) : 0.65 ±0.11 to 1.12± 0.10, P=0.014
DSA - (n=59): 0.65 ± 0.11 to 0.81±0.10, P=ns
Seite 18
CONCLUSIONCONCLUSION
Antiphospholipid syndrome is a severe disease with o More thromboembolic events after transplantationo Poor graft outcomeo Recurrence of APS nephropathy o Progression of IF/TA
Importance of screening APA in case of thromboembolic events
High risk renal transplantation in APS patients
DSA and humoral rejection may have contributed to accelerate vascular lesions