Embed Size (px)
Citation preview

Systemic and topic
corticosteroids
Non steroidal anti-inflammatory
drops
Transient decrease of
macular edema of RE
1 intravitrealinjection of
triamcinolone in each eye
BCVA RE and LE: ↑ to 20/25
In the last visit the patient had
recurrence of macular edema in
the LE
In conjunction with gastroenterologist,
immunosuppressive therapy was
increased and we are considering
submit the patient to Ozurdex®
Crohn disease (CD) is primarily considered an inflammatory condition of the small and large intestine,
although associated extraintestinal inflammation is relatively common. Extra-intestinal manifestations of CD
occur in one third of patients. Ocular complications are infrequent, occurring in less than 10% of cases, but
can be associated with significant morbidity. Ocular manifestations are generally localized to the anterior
chamber and ocular surface but rarely can involve the posterior pole, orbit, and optic nerve.
This case is probably a rare example of posterior segment manifestation in CD. We are not sure if this is of
autoimmune etiology or an independent vascular disease of ischemic etiology. Other diagnostic tests,
including study of systemic vessels are essential for guiding diagnosis and future treatment.
Sílvia Monteiro MD, Inês Casal MD, Ana Figueiredo MD, Carolina Vale MD, Maria João Furtado MD, Angelina Meireles MD
Ophthalmology Department, Centro Hospitalar do Porto, EPE, Porto, Portugal
Department Director: Pedro Menéres MD
We report a case of a 61-years-old white man with the diagnosis of CD since five years ago. He was under
systemic treatment with azathioprin, adalimumab and salazopirin. The patient did not have diabetes
mellitus or arterial hypertension. He had history of an uneventful cataract surgery of both eyes in our
institution and had no other relevant ophthalmological history. Two months after the cataract surgery of
right eye (RE) he presented with decreased visual acuity of right eye (RE) from 20/30 to 20/60. One month
after the cataract surgery of left eye (LE), the visual acuity of LE also decreased from 20/25 to 20/60.
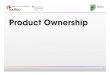
Anterior segment and IOP: normal
Fundus examination: extremely tortuous
retinal vessels, and arteriovenous crossing
changes on both eyes. No signs of vasculitis
or vitritis.
OCT: exuberant cystoid macular edema of
both eyes.
Fluorescein angiography: vascular
tortuosity, macular edema with fluorescein
leakage in macular zone; some ischemic
areas on posterior pole of both eyes.
Carotid doppler was normal. Serum
complement and immunoglobin levels were
normal and no autoantibody was detected.
All viral studies, quantiferon-TB, VDRL,
TPHA, and other biochemical studies
(angiotensin converting enzyme and plasma
lipid levels included) were negative.