Embed Size (px)
Citation preview

INTRODUCTION TO CHILD PROTECTION
AND THE PAEDIATRIC FORENSIC
EXAMINATION March 2013
Dr Amgaad FaltaousConsultant Paediatrician/ CE

INTRODUCTION Kempe 1960’s child abuse “a hidden
paediatric problem” Medical evidence only 1 piece of jigsaw successful protection of child dependant
on effective inter-agency working at every stage
legislation and guidelines

IMPORTANT DOCUMENTS Children (Scotland) Act 1995
www.hmso.gov.uk/acts Protecting Children – A Shared Responsibility.
Guidance for Health Professionals in Scotland. Scottish Executive Jan 2000
It’s Everyone’s Job to Make Sure I’m Alright. Report of the Child Protection Audit and Review.
Scottish Executive 2002 Laming Report (Victoria Climbie Enquiry)
January 2003 www.victoria-climbie-enquiry.org.uk
The Physical Signs Of Child Sexual Abuse
An Evidence-based Review and guidance for Best Practice
April 2008 RCPCH Child Protection Companion

RISK INDICATORS
Domestic Abuse Parental Alcohol Misuse Parental Drug Misuse Non-engaging family Parental Mental Health Problems

TYPES OF ABUSE Physical abuse physical neglect non-organic failure to thrive emotional abuse sexual abuse multiple abuse

ALERTING SIGNS
Unexplained delay in presenting changes in detail as the history is
repeated inconsistency between history and
clinical findings/developmental stage

WHY DO WE SEE VICTIMS OF ABUSE?Medical Assessment & treatment of injuries Assessment & treatment of medical
conditions Referral to other services e.g. Psychology Reassurance for the child
Social Aiding social work in the assessment of risk
Legal Collection of forensic evidence

THE MEDICAL EXAMINATION CANNOT ANSWER
The exact cause of the injury
When it happened - especially once the injury has healed
Who did it?
How much force?
How often?
Over what time period?

PHYSICAL ABUSE
Does the history fit with the clinical signs?
Do the history & clinical signs fit with the developmental stage of the child?

PRESENTATIONS Unexplained bruising fracture(s) different ages/inconsistent with
story/development Abusive head trauma bite mark burns: scalds or contact non-organic failure to thrive fabricated or induced illness recurrent vulvo-vaginitis/ vaginal bleeding repeated DNA’s disclosure

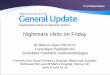
TYPICAL ACCIDENTAL INJURIES

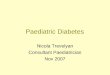
TYPICAL ABUSIVE INJURIES

CASE STUDY 2 year old boy presented on Monday by
social work as has bruises of his face. Parents said that the child came from
nursery on Friday with a red mark The nursery staff could not remember
any marks seen on Friday but were only seen when the child attended on Monday

How old are the bruises?
Are these non accidental

CAN WE AGE A BRUISE ACCURATELY?
The scientific evidence concludes that we cannot accurately age a bruise from clinical assessment or from a photograph.
Any clinician who offers a definitive estimate of the age of a bruise in a child by assessment with the naked eye is doing so without adequate published evidence

INVESTIGATION OF BRUISES
FBC, clotting screen
Infants face & neck or extensive: skeletal survey & head CT & eye examination

FRACTURES It takes a considerable force to produce a
fracture in a child or infant. All fractures require appropriate
explanation and this must be consistent with the child’s developmental age.
The younger the child the greater the likelihood of abuse.
80% of abused children with fractures are <18m, 85% of accidental ones are>5y.
Infants<4m with fractures are more likely to have been abused.

Any bone in the body can be broken in child abuse.
Many abuse # are not accompanied by bruises particularly rib #
Multiple fractures are significantly commoner in abused children.

FRACTURES MORE SUSPICIOUS OF ABUSE Spiral # of humerus are uncommon and
strongly linked with abuse. Any humeral # other than
supracondylar is suspicious of abuse. All humeral fractures in a non-mobile
child are suspicious if there is no clear history of an accident.

Femoral # in children who are not independently mobile are suspicious of abuse regardless of type
Once a child is able to walk, they can sustain a spiral fracture from running.
A transverse fracture of the femur is the commonest presentation in accidental or non accidental injury.

RIBS Rib # in very young children are highly
specific of abuse in the absence of underlying bone disease or major trauma.
Posterior rib fractures have never been described following resus. Ant. Or costochondral have been described extremely rarely.
Oblique views of the ribs maximise detection.


SKULL FRACTURES A linear parietal fracture is the commonest
accidental and non-accidental #. Of particular concern, occipital, depressed,
growing, complex, multiple, wide or # crossing the suture line/ with intracranial injury.
A history of fall less than 3 feet rarely produces a fracture.
assess not only the height, the force of the fall and the landing surface.

DIFFERENTIAL DIAGNOSIS Accidental Birth trauma Physiological periosteal reaction OI (ligamentous laxity, blue sclera, FH) Osteopenia (prematurity, chronic illness) Nutritional, malignancy, infection

CASE STUDY 14 months old presented to A&E with
leg fracture. Brought to A&E by the mother and her
partner. Fell of a high surface in the kitchen. What do you need to know?

What exactly happened? Where? When? Who was there at the time? While the mothers partner was looking
after the child, he had put him on a high surface in the kitchen, the child wiggled, fell off the high surface to the floor.

Child screaming, he noticed a twist of the child’s leg, put him in pram, taken him to the mother at work.
Any concerns at this point?

ABUSIVE HEAD TRAUMA:Presenting symptoms A small percentage dead on arrival Commonest symptoms – drowsy/
seizures/ abnormal neurology, apnoea Smaller number – fluctuating
consciousness Very small number- minimal fussiness/
malaise Diagnosed cases – tip of iceberg?

HISTORY
TBI but no history of trauma. TBI and persistent neurological
impairment with a history of low impact fall (<3 ft)
Out of hospital cardio pulmonary resuscitation
An initial history that changed Alternative traumatic explanations
offered

INVESTIGATIONS Haematology, including extended coagulation
screen Septic screen CT scan, MRI Skeletal survey Ophthalmology Metabolic screen

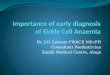
SUBDURAL HAEMORRHAGE



CLINICAL FEATURES ASSOCIATED WITH AHT
Apnoea 93% Rib fractures 73% Retinal haemorrhage 71% Seizures 66% Long bone fractures 59% Skull fractures 44% Head and neck bruising 37%

RETINAL HAEMORRHAGES

Whilst no single feature exclusive to AHT, combinations of features have a high specificity
Bruise + seizure 47% Bruise +apnoea 54% Apnoea + seizure 58% Long bone# +bruise 60% Long bone# + seizure 63% Long bone# + apnoea 84% Rib fractures or RH plus any other feature
PPV>85%

SCALDS AND THERMAL INJURIE Scalds are the commonest intentional
burn injury recorded Apart from head injury, intentional burns
are the most likely injury to cause death or long term morbidity.
A child can sustain a full thickness scald in one second from liquids at a temperature of 60°C.
The diagnostic challenges include distinguishing intentional from unintentional scalds and distinguishing burns from other skin diseases.

ACCIDENTAL SCALDS Majority are non tap water Hot beverages / liquids pulled off table
top/stove / opening the microwave and pulling beverage out
Water used in cooking

Accidental scalds are predominantly spill injuries.Few are immersion
Head, neck and trunk, Face and upper body. 90%of pull down burn were to front of body face/trunk, 20% went to a second location.if somebody else spilled fluid on the child, usually will be on chest and possible LL.
Lack of circumferential (stocking) distribution.Irregular margin
Irregular burn depth, deepest at point of contact, depth decreases following gravity.
Asymmetric involvement

INTENTIONAL SCALDS Majority scald injuries are hot tap water Forced immersion scald injuries are commonest Scald margins have clear upper limits Scald is symmetrical Skin fold sparing is found, eg in popliteal area Central sparing of buttocks, sometimes referred to
as “doughnut ring” pattern may be found in immersion injuries

NON DISTINGUISHING FEATURES Age, gender Severity Few hours delay in presentation as
burns sometimes do not appear that bad till few hours later
Splash marks are not helpful in differentiation.

A detailed history of the events immediately prior to, and the scene of, the injury must be taken in all children with scalds
Consideration of scene of injury assessment including measurement of tap water temperature and height and location of scalding source if doubts remain

NEGLECT Unkempt, inadequate clothing Infestation Nappy rash Poor growth Developmental delay Dental decay

Emotional deprivation- withdrawn, attention seeking
Poor school/nursery attendance repeated DNAs Repeated accidental injuries/ingestions obesity


FABRICATED AND INDUCED ILLNESS Children whose mothers invent stories
of illness in their children and substantiate the stories by fabricating false physical signs.
Very significant morbidity and mortality difficult to identify and intervene

CASE STUDY 6 month old baby admitted with a
history of passing black tarry stool . Spent a couple of days in hospital with
no abnormality detected. Returned to hospital late one evening
with history of baby being blue,stopped breathing and had a seizure.
By the time she arrived at the hospital she was fine.
Investigations were all normal and she was discharged.

This was not the end. 3 weeks later she came back with
another seizure. Admitted and next day had a further
seizure. No underlying cause detected. This became a pattern. Staff noticed seizures only happen when
the mother is with the child.

SEXUAL ABUSE Presentation: Disclosure Suspicion by carer Self destructive or antisocial behaviour Withdrawn Sexualised behaviour Sexual abuse of others

SEXUAL ABUSE Non contact
FlashingShowing pornographyTaking pictures
ContactTouchingMasturbationDigital penetrationVaginal or anal intercourse

FINDINGS Bruising/ injury to external genitalia. Hymenal bruising, laceration or
transection. Anal/ perianal bruising, fissures or
lacerations. Bleeding or discharge.

INTERAGENCY WORKING-KEY PLAYERS
Health Social Work Procurator fiscal/police Reporter Education

Initial Referral Discussion:Initial Referral Discussion:
• Share relevant information
• Plan investigation: interview, Medical, etc.
• Agree sequence, timing, venue, People.
• Share relevant information
• Plan investigation: interview, Medical, etc.
• Agree sequence, timing, venue, People.
PolicePolice Social work
Social work
HealthHealth
referrerreferrer

JPF- AIM OF JOINT EXAMINATION
JPF encompasses within a single examination the child’s needs for medical evaluation and health care and the need to obtain forensic evidence.

TIMING OF EXAMINATION Forensic evidence deteriorates
exponentially over time Likelihood of positive forensic
samples after 72 hours is extremely small, but possible
Evidence of semen may be found up to 7 days after the assault
Important superficial physical signs (erythema, abrasions) may disappear within 24 hours and may be important forensically

JPF-PROCESS
Comprehensive assessment of health, growth and development
Efficiently documented: -records, drawings and photo-documentation
Skilled examiners: bringing together paediatric and forensic skills
Child friendly well equipped facilities

JPF- PAEDIATRIC ROLE ‘Engage’ with the child and family and
obtain informed consent. Assess general health, growth and
development consider differential diagnoses eg brittle
bone disease, bleeding disorder collate relevant past medical and family
history (liaise with HV etc.) arrange appropriate
investigations/specialist opinions provide ongoing health care

JPF- FORENSIC ROLE
To describe and interpret injuries Collection of appropriate samples for
forensic analysis Advising police on investigating the locus,
alleged perpetrator, clothing etc) Arrange specialist forensic opinion if
required eg forensic odontology

JPF- JOINT RESPONSIBILITIES Ensure effective documentation of all the
findings, including accurate measurements, drawings and photo-documentation
Reach an agreed opinion (preliminary) Provide an immediate statement to police
and social workers Provide clear evidence/opinion for
subsequent legal and child protection procedures




CONSENT TO MEDICAL EXAMINATION AND TREATMENT OF CHILDREN
Age of legal capacity (Scotland) Act 1991 “A person under the age of 16 years shall
have the legal capacity to consent on his own behalf to any surgical, medical or dental procedure or treatment, where in the opinion of a qualified medical practitioner attending him, he is capable of understanding the nature and possible consequences of the procedure or treatment”.

CONFIDENTIALITY – GMC 2000Para 36: disclosure without consent where failure to do may expose the patient to risk of death or serious harmPara 37: disclosure to assist in the detection, prevention, or prosecution of a serious crimePara 39: disclosure if doctor believes the
patient to be victim of neglect or physical, sexual or emotional abuse and the patient cannot give or withhold consent..in the patient’s best interests…

PROTECTING CHILDREN AND YOUNG PEOPLE: THE RESPONSIBILITIES OF ALL DOCTORS GMC 2012 Children, young people and their families
have a right to receive confidential medical care and advice- but this must not prevent doctors from sharing information if this is necessary to protect children and young people from abuse or neglect
Also applies when the adult parent or carer is the patient