Embed Size (px)
Citation preview

16/09/2015
1
ROYAL FREE CHILDREN’SSERVICES
Rahul Chodhari , Consultant Paediatrician07711808012, [email protected]
Aims of the talk• Opportunities to improve asthma care in
Camden• Diagnosis in primary care• Preschool wheeze v asthma
– When to refer?
A belief that asthma could be cured bythe sound of a violin
Asthma, caricature from 'Album Comique de Pathologie Pittoresque', published in Paris, 1823

16/09/2015
2
NRAD and Children• 28 children died of asthma (CF registry 0%)• 80% died before reaching hospital• 42% who died were labelled as mild /
moderate asthma• “Asthma attack” kills rather than severe asthma
label• 80% had one or more avoidable Factors• 30% had an inhaler assessment in 10 care
Thx to Dr. James Paton, Clinical Audit Lead, RCPCH, NRAD – May 2014
are likely to have asthma.*75% of asthma admissions are preventable.
On average, 3 children in a classroom of 30
Asthma UK -2010*Epidemiology and Statistics Unit. Trends in Asthma Morbidity and Mortality. NYC: ALA, July 2006.
22%
24%
20%
14%
14%
23%
24%
31%
52%
11%
18%
5%
0
10
20
30
40
50
60
70
0 1 2 3 4 5 6 7 8 9 10 11 12 13
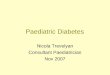
Totalmonthly
Paediatricasthma
attendances
Months
RFH Paediatric asthma admission rates (%) 2014
January February March April May June July August September October November December
1/3 of A&Eattendances arerepeat attendances

16/09/2015
3
Chimat atlas of Paediatric admissions
Camden 119
Barnet 55
Islington282
Haringey185
Brent 452RFH
http://www.chimat.org.uk/resource
Cases: Asthma, episodic wheeze ormulti trigger wheeze?
• 3 year old Gemma• 4 year old Jonny
Definitions• Preschool children
– Episodic viral wheeze – the child is only wheezing duringclinically diagnosed URTI
– Multiple trigger wheeze – URTI, smoke, allergens, exercise,food allergy and pollution
• Asthma is a chronic disease characterised bywheezing, breathlessness, night time or earlymorning coughing– Episodes are usually associated with airflow obstruction
within the lungs that is reversible with treatment

16/09/2015
4
Preschool wheeze clinical categoriesEpisodic viral wheeze
(EVW)Multiple trigger wheeze (MTW):
Viral URTI inducedwheeze
+++ +++
Interval symptoms None. Wheeze with triggers, such as exerciseand smoke and allergen exposure.
Treatment Symptomatic only forthe episode
Rx is ↑ or ↓depending on symptompattern and severity
Eosinophilicinflammation &remodelling
None Similar to asthma
Will it lead to asthma? Not in long runprovided there is noh/o of atopy.
More likely with higher number oftriggers.
European Respiratory Society Task Force classification
Case: Episodic Viral Wheeze (EVW)
• What are treatment options for EVW?• Would you prescribe Montelukast, inhaled
steroids or oral prednisolone?• Would you prescribe prophylactic
Montelukast or inhaled steroids?
Royal Free Out patientspictures.
Episodic Viral Wheeze (EVW)• PREEMT trial – Use of Montelukast resulted in fewer
visits to GP’s/ED & fewer days away from nursery– Start Rx at the first sign of a viral cold and discontinue it when
the child has recovered• No evidence that inhaled corticosteroids or oral
prednisolone helps in treatment or prevention of futureepisodes
• Some hospitalised children may need steroids• Long acting β2 agonists are not licensed for use in
preschool children

16/09/2015
5
Multiple Trigger Wheeze (MTW)• Treat acute episodes with Salbutamol or
anticholinergics• Pragmatic regimen for treatment (Prof Bush, 2014)
– Step 1: Trial of inhaled corticosteroids or Montelukast instandard dose for max eight weeks
– Step 2: Stop treatment; either there has been noimprovement, in which case further escalation is notvaluable, or symptoms have disappeared
– If there is no benefit and the symptoms are worse – refer.– Step 3: Restart treatment only if symptoms recur; then
reduce treatment to the lowest level that controlssymptoms.
Prevalence of asthma• It is the most common childhood chronic condition• Patient reported asthma symptoms (adults included)
• 1973 – 4.2%• 1988 – 9.1%• 2003 – 15.4%• 2010 – 17%
• Hospital admissions are falling• Risk of asthma rises with:
– positive family history atopy– maternal smoking in pregnancy– early sensitisation to aeroallergens
Burr Thorax 2006, Asthma UK, National statistics
British Thoracic Society (BTS) guideline Oct 2014

16/09/2015
6
Case: High v Low probability of asthma?• 5 year old Josh:
– 4 episodes of wheezingin the past, mostly withURTI
– Improvement insymptoms after startingRx
– Symptoms are worse atnight and in the earlymorning
– Widespread wheezeheard on auscultation
Royal Free OPD
High probability of asthma• More than one of the following symptoms:• Wheeze, cough, difficulty breathing, chest
tightness, particularly if these symptoms:• are frequent and recurrent• are worse at night and in the early morning• occur in response/worse after triggers, such as
exposure to pets, cold or damp air, or with emotions orlaughter
• occur apart from cold• personal/ Family history of atopy or asthma• wheeze heard on auscultation• improvement in symptoms or lung function in response
to adequate therapy
Case: High v Low probability ofasthma?
• 13 year old Jenny:– Isolated cough in the absence of
a wheeze or difficulty breathing– Dizziness, light-headedness and
peripheral tingling– Normal peak expiratory flow
when symptomatic– No response to a trial of asthma
therapy

16/09/2015
7
Low probability of asthma• Symptoms only with colds and with no interval symptoms• Isolated cough in the absence of a wheeze or difficulty
breathing• Prominent dizziness, light-headedness and peripheral tingling• Repeatedly normal physical examination of the chest when
symptomatic• Normal peak expiratory flow (PEF) or spirometry when
symptomatic• No response to a trial of asthma therapy• Clinical features pointing to alternative diagnosis
Clinical features pointing to alternativediagnosis
• Symptoms are present from birth or perinatallung problem
• Isolated upper respiratory tract disease– Stridor, chest deformity and asymmetric signs
• Persistent moist cough• Failure to thrive• Abnormal voice or cry
When should you refer?• Investigations - SPT, PEFR or spirometry
• Escalating dosages above BTS step 2/3• To establish and review definitive diagnosis
• Poor response +/- compliance• Trigger avoidance advice• Education & device technique• Risk assessment – severity and home visits• Management of co-morbidities• Communication with other agencies
• Involved people (doctor, child, family) areunhappy with outcomes

16/09/2015
8
Clinical Gems• Clarify what the family means by wheezing• Isolated dry cough in a community setting is
rarely due to asthma• Preschool wheeze - “episodic viral” or
“multiple trigger”• Pre school wheeze treatment is driven
solely by current symptoms• Prednisolone is not indicated in preschool
children with wheezing attacks• Focus clinical assessment of school wheeze
based on high or low probability of asthma