Embed Size (px)
Citation preview

FEVER
Dr K Sathiamoorthy
Consultant Paediatrician
Shree Sakthi Hospital

NORMAL
Axillary temperature 36~37 .0 C
Sublingual temperature 36.7~37.7 C
rectal temperature 36.9~37.9 C

CONCEPT
一、 pyrogen set point of the
thermoregulatory center body temperature

TEMPERATURE
sport physiological T pregnancy luteal phase hyperthermia pathological T ( set point ± ) fever

Hyperthermia : thermogenesis thermolysis dysfunction of thermoregulatory center
二、 Causes and pathogenesis of fever
Pyrogen and activator of fever Activator : the substance can activate the cells
that can produce the pyrogen.
pyrogen: the substance can cause fever

ACTIVATORS OF FEVER
microbe: G- LPS, ET G+ peptidoglycan virus: enveloped virus particle: transfuse response 2. internal production immune complexes etiocholanolone
1. Extragenous
pyrogen

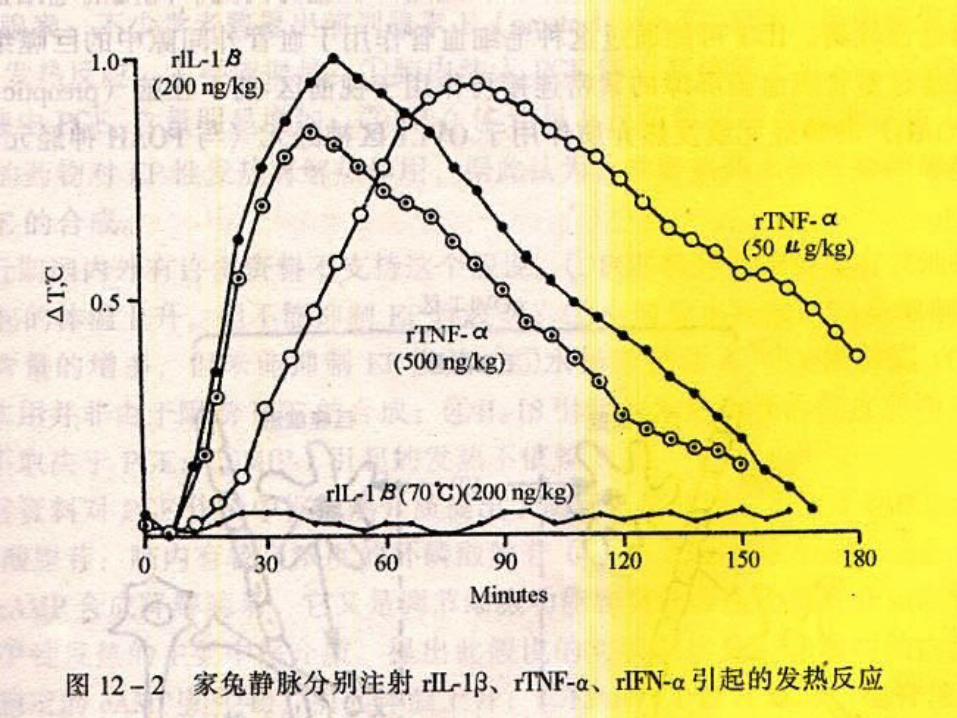
ENDOGENOUS PYROGEN(EP)
interleukin-1(IL-1) :MC,fibroblast IL-6:T,B lymphocyte, tumor cell TNF : TNF Mα φ TNF (lymphotoxin) active T β interferon ( IFN ): T lymphocyte

PRODUCING AND RELEASING OF EP
cell of producing EP
Toll receptor
LPSLPS joint
pro trigger NF-κB
Start transcription ,EP express

LPSLPS joint
pro
sCD14
LPS –sCD14
complexes
T

三、Mechanism : increase of set point1.the pathway: EP entry temperature center

PATHWAYS OF EP SIGNAL TRANSDUCTION TO THE THERMOREGULATION CENTER
a. blood brain barrier
Activator ActivatorActivatorActivatorCell of Producing EP
EP
blood brain barrier
Thermoregulation center
Thermoregulation center
SPSPTT
a.OVLT (organum vasculosum laminace terminalis )

2.The mechanism: increase of set point
a. Warm sensitive neuron: thermolysis
b. Cold sensitive neuron: thermogenesis
Imbalance:Normal:warm sensitive neuron
cold sensitive neuron

THERMOREGULATION MECHANISM OF FEVER
Thermoregulation center1. The positive regulationpreoptic anterior hypothalamus, POAH
2. The negative regulationmedial amygdaloid nucleus, MANventral septal area, VSA

POSITIVE REGULATION MEDIATORS
1.PGE2: warm sensitive neuron
cold sensitive neuron Effective medicine: Aspirin, ibuprofen
2.CRH(corticotrophin releasing hormone) EP (IL-1 , IL-6 ) CRH media feverβ TNF , IL-1 PGEα α 2 media fever
SP
3. cAMP : SPEP hypothalamus: Na+ /Ca2+ cAMP
SP
4. Na+ /Ca2+ :5. NO:a. Activate metabolism Brown fatb. Inhibit Negative regulation mediatorsc. OVLT POAH T
NEGATIVE REGULATION MEDIATORS
Negative feedback: Febrile ceiling: < 42℃ endogenous cryogens AVP
-MSHα T center T
PERIOD AND METABOLISM OF FEVER
The period of febrile: 1.the fervescence period characteristic: thermogenesis>thermolysis chill brown adipose tissue(scapula
,large vessel of thoracic and
cervical metabolic rate
Thermogenesis

MANIFESTATION:
pale , gooseflesh, chill
warm sensitive neuron (POAH) Chill center
Chill cold sensitive neuron (POAH) cold stimuli Chill center
Chill skin T
Chill
Rubro nucleus
Lateral spinothalamic tract
Rubrospinal tract Reticulospinal tract
anterior motor cells
Up
Down
2.THE PERSISTENT FEBRILE PERIOD
The temperature reaches the new set point ★ Thermogenesis = thermolysis : SP on higher level ★Manifestation: febrile , headache metabolic rate and pulse rate anorexia

3.THE DEFERVESCENCE PERIOD
★ characteristic: Thermogenesis < thermolysis SP is reset to the normal level ★ Manifestation: the skin is warm and flush, sweat
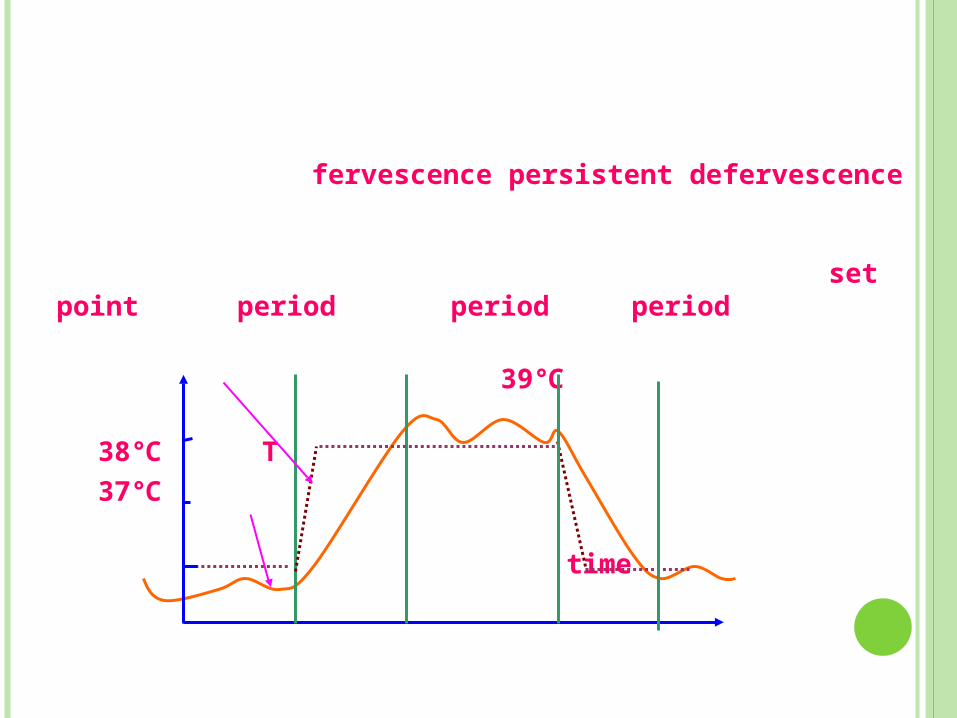
fervescence persistent defervescence set point period period period
39 ℃
38 T℃ 37℃ time

METABOLISM CHANGE OF FEVER
1. Glycometabolism
Glycogenolysis Glycogen storage2. Fat metabolism lipodieresis Fat storage Ketosis3. proteometabolism
Protein catatabolism, negative nitrogen4. water\electrolyte metabolism\vitamin
metabolism T 1 metabolism rate 13%℃ acute phase response WBC
PHYSIOLOGICAL CHANGES:
1.CNS: headache , dizzy,drowsiness, febrile convulsion: 24h inheritance hypoxia discharge
2.immunity system IL-1: activator of lymphocyte IL-6 : differentiation factor IFN: humoral factor TNF: anti-tumor

3.Digestion system Sympathetic digestive juice EP hypothalamus nauseated,vomit abdominal distention constipation

4. circulation system HR 1 HR 18℃ /min CO induce heart failure
5. Respiratory system Tachypnoea

PRINCIPAL OF TREATMENT
1.medicine Inhibit production of pyrogen: glucocorticoid:
inhibit IL-6 and TNFInhibit production of PGs: salicylic
2. physics: brain 1g water 2.5KJ(lose)
50%1~2%

ADVANTAGE AND DISADVANTAGE
1. Disadvantage Side effects
2. Advantage Signal: malariaSerious underlying infectionInflammation


NICE GUIDELINES:
ASSESSMENT AND INITIAL MANAGEMENT OF FEVERISH ILLNESS IN CHILDREN YOUNGER THAN 5 YEARS
WHY GUIDELINES NEEDED Fever = commonest reason for child to be take to a
doctor Fever = second commonest reason for a child being
admitted to hospital Infection = leading cause of death in children under five
years Fever without apparent source (FWS) particular
diagnostic difficulty Current variable management Difference in mortality and morbidity secondary to
health inequality

EVIDENCE BASE
Best available evidence Consensus technique: Delphi consensus Traffic light system to assess the risk of serious
illness as LOWLOW INTERMEDIATEINTERMEDIATE HIGHHIGH Direct management accordingly
CLINICAL ASSESSMENT
Identify life threatening features ABCD Assess the risk of serious illness using the traffic light
system Measure and record temperature, heart rate,
respiratory rate, and capillary refill time Attempt to identify a focus of infection or features of
specific serious conditions: Meningococcal disease, Meningitis, Herpes simplex
encephalitis, Pneumonia, UTI, Septic arthritis/ osteomyelitis, Kawasaki disease
Guidance on further ix if FWS

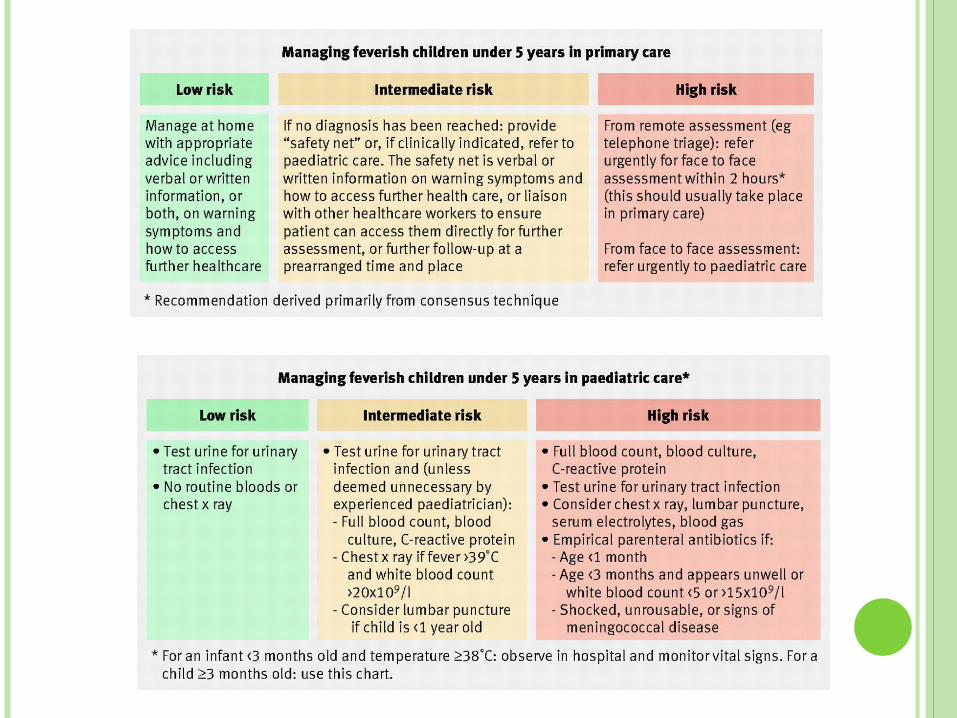
Copyright ©2007 BMJ Publishing Group Ltd.
Assessing the risk of serious illness in feverish children under age 5 years
MANAGEMENT OF CHILDREN < 3MTHS Febrile infants under 3 mths of age should have the
following ix: FBC, Blood cultures, CRP, Urine testing, CXR (if resp signs
present), Stool culture (if diarrhoea) LP (without delay and if poss < abx) if:
< 1 month 1-3 months who appear unwell 1-3 mths with WBC < 5 or >15
RX: 3rd generation cephalosporin + abx active against listeria
DETECTION OF FEVER
< 4 weeks: electronic thermometer, axilla chemical dot
thermometer 4wks-5yrs: electronic thermometer, axilla
chemical dot thermometer,
infra-red tympanic thermometer
Reported parental perception of fever should be taken seriously
Do not routinely use oral and rectal routes in children aged < 5 yrs

ANTIPYRETIC INTERVENTIONS Tepid sponging not recommended Do not under dress OR over wrap Antipyretic agents should not be routinely used
with sole aim to reduce fever in a child who is otherwise well
Paracetamol/Ibuprofen should not be administered at the same time
Paracetamol/Ibuprofen should not be given alternately to children with fever
Antipyretic agents do not prevent febrile convulsions and should not be given specifically for this purpose
OTHER RECOMMENDATIONS Healthcare professionals should not rely on a decrease or
lack of decrease in temp following anti-pyretic administration to differentiate between serious and non-serious illness
Children with symptoms and signs suggesting pneumonia who are not admitted should not routinely have an CXR
Oral antibiotics should not be prescribed to children with fever without apparent source

QUESTIONS