Embed Size (px)
Citation preview

• Managing an Ageing Patient from
Midlife to Beyond GM Annual
Conference
• 08 October 2014
• Royal Society of Medicine, London

• I am delighted & honoured to be here.
• Have been employed by or had trips from:-
• Internis Bayer MSD
• Servier Merck Aventis
• NovoNordisk Eli Lilly Novartis
• Pfizer Sanofi Takeda
• Schering Sankyo SKB/GSK
• BMS Boehringer Ingelheim
• No conflict, I’ve worked for them all

What are we treating?

DM incidence by Type. Melton LJ et al Diabetes Care 1983, 6, 75-86
0
100
200
300
400
500
600
700
0-9 10-19. 20-29 30-39 40-49 50-59 60-69 70-79 80+
Age (yrs)
Incid
en
ce
(p
er
10
0,0
00
pe
r ye
ar)
T1DM
2ndry
Male T2
Female T2

DM incidence by Type. Melton LJ et al Diabetes Care 1983, 6, 75-86
0
5
10
15
20
25
30
35
40
0-9 10-19. 20-29 30-39 40-49 50-59 60-69 70-79 80+
Age (yrs)
Incid
en
ce
(p
er
10
0,0
00
pe
r ye
ar)
T1DM
2ndry

If skinny, consider:-
- insulin deficient DM,
- malabsorption,
- malignancy,
- thyrotoxicosis.
ie NOT BOG
STANDARD T2DM
Croxson S,
Practical Diabetes International 2000; 17 (7)

Type 1 v Type 2?
• Generally, clinically apparent.
• Urinary C-peptide to creatinine ratio useful
• http://www.diabetesgenes.org/content/urine-
c-peptide-creatinine-ratio
• A cut-off of 0.2 nmol/mmol differentiates
T2DM from T1DM
– 94 % sensitivity, 94% specificity
– ROC AUC 0.94

Important to know what are we
treating? • T2DM might lose weight in future
– Might not need insulin in future.
• Might be ketosis prone T2DM
– ie might just need a short course of insulin
– Umpierrez G, Ann Intern Med. 2006;144:350-357.
• Might be Latent Auto-immune Diabetes of the
Adult
– ie needs insulin long term, not tablets
– Cernea S, Diabetes Care 2009

Patient now diagnosed & treated.
Admitted middle of night:-
•Off legs, weak legs
•Slurred speech
•Confused
Diagnosis?

Δ CVA
FULL ANTI-COAG
+ ASPIRIN
URGENT CT BRAIN
CARRY ON THE
SULPHONYLUREA
Croxson, S. Pract Diab Int 2010 Vol. 27 No. 6
Case like this last seen Tuesday 17th June 2014

Hypoglycaemia Unawareness
• Staff just do not appreciate it – Professional hypoglycaemia unawareness
• Elderly have little difference between:- – Sympathetic threshold
– Neuro-glycopaenic threshold
• And deny them even if noticed: – Heller S BMJ 1995 – 20% patients deny their hypos
• So ask family / carers. • What symptoms, how common?

AJ Jaap, 1998: Commonest symptoms in elderly
• Poor concentration
• Confusion
• Sweating
• Trembling
• Weakness
• Inco-ordination
• Unsteadiness
• Light headedness
• Presents to ED as:-
– Off legs,
– confusion ? Cause
– CVA, TIA
– Fits
• Symptoms may change
over years
• Despite telling, folk
still don’t test during
funny turns.

How common are hypos? Munshi MN 2011
• Continuous Glucose Monitoring (mean 88 hrs)
• 33 diabetic people: 77% -T2DM; 91% -insulin treated.
• Mean age 75.2±4.6 yrs; A1c 9.4±1.3%.
• 20 patients had hypos; 6 had nocturnal hypos
• 10 had an A1c >9%; 6 of these had nocturnal hypo.
• 77 hypos, 73 unrecognized (finger-stick or symptoms).
• All hypo patients had at least 1 unrecognized hypo
• Only 1 of 32 nocturnal hypos recognized by patients.
– Causes confusion, headache low mood next day
– Test at bedtime, & at 3.00am if awake
• ie VERY COMMON, OFTEN NOT APPRECIATED

How common are hypos? Munshi MN 2011
• Or in English:-
– Lots of hypos
– Generally not noticed
– Often at night
– Even in folk with high HbA1c

Hypos
Do they matter?

Diabetes & Dementia
• Observational studies → Hypos increase future dementia
– Whitmer RA, JAMA 2009
– Mark Strachan, Diabetic Med 2012
– Feinkohl I et al, D Care 2014
• Yaffe K, JAMA 2013
• 12 year FU of 783 folk with known DM
• Hypo increased risk of future dementia
– HR 2.1
• Dementia increased risk future hypo
– HR 3.1

Results of hypoglycaemia • Falls & fractures associated with low HbA1c
– Nelson, J; JAGS 2007. 55(12): 2041-2044, – Puar T et al JAGS 2012
• Permanent neuro loss – eg cognitive impairment; S Croxson PDI 2001
• Cardiac events
• Death – McCoy RG, Diab Care 2012
• Long stay in hospital, eg Johnston V, Davies M – 2 years of hypo admissions LRI (n=83)
– Age 76 (range 51-92)
– Mean duration stay 18 days
– J Diabetes nursing 2002; 6 (2):

Who will go Hypo?
• Risk factors for hypoglycaemia:-
– Recent change agent, type agent, hospitalisation
– Co-morbidities; any failure
– Elderly single male
– Alcohol
– Cognitive impairment
– Increasing age
• After hospital discharge on insulin / SU
– Ensure someone checks not hypo at 4-6 w
• Ensure adequate diet

Nutrition
Advisory Group
for Elderly
People
(NAGE)
on www.bda.uk.com

Other Language Diet guides @ DUK http://www.diabetes.org.uk/Guide-to-
diabetes/Information-in-different-languages1/ www.diabetes.org.uk/Guide-to-
diabetes/Information-in-different-
languages1/

Factors I consider in hypos • Can keep going hypo 5 days after last gliclazide
• Due to weight loss?
• Due to development of renal impairment?
• Are they on the best treatment?
– Do they need the insulin & is it the best one?
– Do they really need the Sulphonylurea?
– Have steroids just been stopped?
• Injection technique & timing
– Worn out pens
• “Chasing sugars”
– BGM = high, so increase dose
– Then hypo so decrease dose

Factors I consider in hypos • Nocturnal hypos increasing risk day hypos
– Test at 3.00 am
• Hypothyroid
• Addison’s
• ACE inhibitors ↑ risk hypo, ARBs do not
• Alcohol
• Chasing inappropriately low HbA1c target
– High HbA1c and hypos both linked to complications
– Targets often HbA1c based
– Is the HbA1c reliable?
• Clearly no, otherwise I would not be asking

Glucose targets?

Less aggressive control; ADA EASD 2012

HbA1c Reliable? Gallagher, EJ, 2009
• Increased by ageing; 0.1% per decade
– Dubowitz N, D Med 2014
• Raised if RBCs survive longer:-
– B12 & iron deficiency; splenectomy
• Afro-Caribbean HbA1c increased 0.5%
• Decreased if decreased RBC survival:
– Haemolytic anaemia
• HbA1c very variable:
– Significant CKD, variant Haemoglobins
• Is just an average, not reflecting hi’s & lo’s.

What about renal function:
is the eGFR reliable?

Mrs T
89 yr F
Creatinine 137
(1.8 mg / dL) 28Kg

MDRD = 31 mls/min
Cockcroft Gault = 10.5 mls/min
- MDRD eGFR over-estimates renal function
- Cockcroft Gault most accurate Schaeffner ES, Ann Intern Med 2012

Glucose control

Metformin
• Care in impaired renal function – But might be safer than we think
– Florent F Richy, D Care 2014
• May cause weight loss
• Doubles risk vitamin B12 deficiency
• Diarrhoea

Pioglitazone • Pros
– Reduction of vascular events,
– Useful in NAFLD
– No hypos
• Cons
– Ankle oedema
– Weight gain a bother
– Bladder cancer on long term use
• Possibly not a prob
– Interesting - the 3 TZDs had similar structure, but
very different outcomes on liver & blood vessels

Gliptins • Buying:-
– Likely HbA1c drop 0.6%
• same as 150 mls white wine, Merlot
• Wine dose ranging, LFT safety & durability studies?
– Presumed safety
– No hypos
– No weight gain
– Main SE = nausea, pharyngitis on SPC
– Skin rash in my practice
– Ongoing safety review by EMEA and FDA, with GLP-1 RAs

Meta-Analysis of DPP-4 Inhibitors
on CVS Risk. Monami M. Diab Obes Metab, 2013; 15; 112-120
• 70 RCTs; 41,959 folk on DPP4 inhibitor.
• Mean duration of therapy – 44.1 weeks.
• With DPP-4 inhibitor OR (95% CI):-
– MACE 0.71 [0.59 - 0.86],
– Myocardial infarction 0.64 [0.44 - 0.94],
– Stroke 0.77 [0.48 - 1.24]
– Mortality 0.60 [0.41 - 0.88]
• But recent Saxa & Alo trials not confirmed this
– Short eg 2 year trials, but big numbers eg SAVOR

Metformin plus SU or Gliptin? C. Ll. Morgan, C. J. Currie, DOM 2014
Mortality
MACE

Do gliptins decrease hypos with
insulin or SUs? Not sure.
Safety & efficacy of linagliptin plus basal insulin combination therapy in a vulnerable
population of elderly patients (age= 70 years) with T2DM.
HJ Woerle, D Neubacher, S Patel et al, Poster EASD 2012

Gliptin added to Insulin Frandsen CSS, Madsbad S D Med 2014
• Adding gliptin drops HbA1c 0.6 % (6.6 mM/M)
• No increased risk hypo

Use of gliptins
• Converging licensed indications
• Different molecules with very different
excretion
• So wait 10 years to see full SE profile

Anyone do particularly well on DPP-4 Inhibitor?
• Probably elderly
– ? More hyperglucagonaemia than young
– Risks of hypo with SU
– Risks of oedema with TZDs
– May not wish such great HbA1c drops
• Anyone at risk of hypos – Had them before
– Ramadan fasting
• Anyone for whom hypos not great idea – eg taxi driver

SGLT-2 inhibitors Sodium Glucose CoTransporter 2 inhibitors
eg dapaglflozin, canagliflozin, empagliflozin

SGLT-2 inhibitors
• Inhibit glucose
resorption from
glomerular filtrate
• HbA1c reduction like
other OHAs eg 0.6%
• Croxson et al, GM2
2013; 43 (Sept); 27-31

SGLT-2 inhibitors
• Lose as much weight as GLP-1 RA eg 3-5 kg
• Drop BP 5 mmHg systolic
• No hypos from them per se
• Not mega-expensive for new drug
• BUT
• Need eGFR > 50-60 to work
• Might dehydrate if on loop diuretic or D&V
• 1 episode genital thrush per year
• License for T2DM, but probably OK for T1 & 2ndry

SGLT-2 inhibitors use.
• Limited by eGFR & diuretic use
• T2DM:-
– On insulin, weight probs not helped by liraglutide,
try SGLT-2i
– On tablets, thinking of liraglutide, try SGLT-2i
• Insulin treated with brittle control, could
decrease insulin dose to lose hypos & add
SGLT-2i to lose peaks – novel

T2DM Failing
Oral Hypoglycaemic Agents.
Insulin or GLP-1 RA?

Failing Oral Hypoglycaemic
Agents: Insulin or GLP-1 RA? • If skinny or losing weight, probably insulin
deficient, ie need insulin.
• If tend to vomit easily, GLP-1 RA will make
sure, eg with gastroparesis.
• Significant renal impairment is a contra-
indication to GLP-1 RA,
– This might change for liraglutide shortly
– GLP-1 RA vomiting worsens eGFR dramatically
• Previous pancreatitis = avoid GLP-1 RA

Key GLP-1 RA Injection Message
• They make folk throw up.
• But very useful agents with daily or weekly jabs
• Gliptin & GLP-1 RA safety
– Ongoing review by FDA and EMEA
– As safe if not safer than any other drug

Failing on oral agents,
and adding insulin.
What does one do with the
tablets?
• Stop Pio – weight gain & oedema
• Others – review safety & continue

Choice of regime; do what you like. • OD Glargine
– Fritsche A, Ann Intern Med. 2003
• OD Levemir
– Hermansen K, Diabetes Care 2006
– Garber AJ, JAGS 2007 (elderly pooled analysis)
• Novomix 123 regime
– Garber AJ, DOM 2005
• Stepwise Lyspro Mix 50 – Nakashima E, Endocrinology 2013
• BD novomix 30
– Holman R (4T) NEJM 2009
• OD Neulente
– Tindall, H, 1988 62 different insulins / presentations (4 makers)

Insulin
• One can find evidence to do whatever one wishes
• Fasting hypoglycaemia major problem with once daily long acting basal insulin
• Using insulin in elderly:-
– What does the patient eat?
– What is one trying to achieve?
– Who will give?
– Who will monitor?
– Bedtime snack / meal
– No fixed ideas

What do they eat?
• Meals regularly through day.
– Probably try morning basal insulin
• One meal per day
– Probably try mealtime biphasic
– eg Humalog Mix 25, Novomix 30
• Ill in hospital
– Probably basal bolus
– 0.5 units / Kg, half lantus, half prandial
– And elderly often happy to continue at home – Long acting to quick acting ratio same as Humalog Mix 50

Which basal? • NPH
– Economical
– But less predictable and need to shake
• Lantus and levemir
– More expensive
– But more predictable & no need to shake
– Levemir for the frail LOD who only needs a small
dose; Rosenstock J et al Diabetologia 2008

Which basal? • Degludec
• Much more expensive
• Use as last resort for :-
– variable control with hypos
– insulin timing haphazard eg dementia, or just
haphazard

On basal and failing? • Pushed basal, fasting levels OK, HbA1c > target of whatever
• Usually add rapid acting to meal that raises
glucose, either breakfast or biggest meal of day
• Add liraglutide or I Aspart? C Mathieu; Abs 1027; EASD 2013
• Hence IDegLira, S Gough, Lancet 2014
+ Lira +Aspart P
↓ HbA1c 0.74 0.39 0.002
Hypo / year 1.0 8.15 <0.0001
Δ weight -2.8 +0.9 <0.0001

Das Ende La Fin
El Fin The End
Questions?
Sorry - English

Blood Pressure

Blood Pressure
• Jan 2012 Target from ADA
–Under 140 systolic
• Benefit of very tight control
–eg ADVANCE, ACCORD
–Marginal
–But drug side effects increased

Use whatever you like, but:
• Avoid β blockers – do not stop CVAs
• Do not mix ACEi and ARBs
• Indapamide preferred to bendrofluazide
• Moxonidine well tolerated, but no evidence
it stops CVAs

Cholesterol

Cholesterol treatment • Use in Free Range
– Not in nursing home folk
• Targets unchanged
• Which statin?
– Atorvostatin eg 10 mg
• Generic
• Any time of day
• Any eGFR
• Safer with grapefruit
• Ezetimibe?
– IMPROVE-IT reports very soon

Diabetes
and
dementia.

Xu W et al Diabetes 2009 • Swedish twin registry data (13,693 aged 65+)
• Diabetes associated with dementia
adjusted Odds Ratio (95% CI):-
– 1.89 (1.51–2.38) for dementia,
– 1.69 (1.16–2.36) for Alzheimer's disease,
– 2.17 (1.36–3.47) for vascular dementia.
• Risk by onset of DM (Odds R with 95% CI):-
– Mid-life onset DM 2.41 (1.05–5.51)
– Late-life life onset DM, 0.68 (0.30–1.53)

MCI to dementia; quicker decline with DM,
3.2 years quicker. Xu W, Diabetes 2010

Confusion • Dementia x 2-3 more common in DM
• Undoubtedly vascular
• Probably increased Alzheimer’s Disease
• Probably impaired cognition deteriorates more
quickly in DM.
• Alcohol → chronic pancreatitis & dementia
• Obesity = independent risk factor for dementia
• Strong links between DM & Psyche Illness.
– Multiple directions of causality

DM & Dementia
• AVOID
– Avoid hypos
– BP control
• SPOT
– Mini-COG
• MANAGE
– Safe relaxed targets
– Avoid hypo inducing Rx if pos
– So need to know type of DM

End stage dementia needing
insulin. • Low dose basal insulin probably in morning
– If basal at different times, Degludec
• Rapid acting eg Humalog at the end of meal if
they have eaten the whole meal.
– Zero if they do not eat the whole meal
• Monitoring may be difficult to do & justify
– But should not die hypo.

The End Questions,
or sneak out the back
to get some coffee?

Das Ende La Fin
El Fin The End
Questions?
Sorry - English

Avoid

Confusion; Avoidance.
• BP control probably helpful
– Syst-Eur, Forette F, Arch Intern Med 2002
– PROGRESS Collaborative Arch Inter Med 2003
– Observational data - Hassing LB, Age Ageing 2004
• Dementia occurred if BP not controlled
– But takes 5 years to work, Peila R, Stroke 2006
• Current ADA target is under 140 systolic
• Evidence hypoglycaemia harmful:
• Whitmer, R: Strachan, M.

Spot


Confusion: Glycaemic Management Change from tight control to safe control
• If insulin treated, what type of DM?
• T1DM = Needs insulin
• DM 2ndry to pancreatitis = needs insulin
• DM 2ndry to steroids = may not need insulin
• T2DM = may not need insulin
– Particularly as they lose weight

Gadgets • Pens:-
– Novo ECHO pens – size last dose
– Timesulin pen tops – time since last jab
• http://timesulin.com/
• Reminder devices
– Pendant
• www.alrt.com
– Reminder & Alert watch
• www.cadexwatch.com/
• There are others, but these are the ones we
have come across.

Relax glycaemic targets
• Avoid hypos
• But some folk’s behaviour seems to get very
disturbed if BGM high teens
• Avoid side effects of drugs
• Eg :-
– HBGM 5-15 mM
– HbA1c 8-9% or 65–75 mM/M
– Sinclair AJ
– European Diabetes Working Party for Older People 2011
clinical guidelines for T2DM.
– Diabetes Metab. 2011;37 Suppl 3:S27-38.

Confusion: finding it.
• Generally when sudden loss of control
– Classic = forget taken insulin, so take again
• Sometimes when spouse dies
– was covering up problem
• Finding is recommended
– Value is debated for many subjects
– But pre-empts glycaemic problems in diabetes.
• Annual memory test aged 75+
– Screen with quick test eg MiniCOG
– If abnormal, fancy test eg MoCA

Puar T et al JAGS 2012
• Case control study of DM folk with fractures
• vs age, gender, race, duration DM, comorbidity control:
• Versus HbA1c > 8.0%:-
• HbA1c < 6.0% = 3.01 x fractures
• HbA1c 6.1-7.0% = 2.64 x fractures
• HbA1c 7.1-8.0% = NS
• SU & insulin linked to fractures
• But we are probably going for safe control in these
folk already.

Factors increasing mortality.
McCoy RG, Diab Care 2012
• Assessed for severe hypo, 5 yr FU
• Direction of causality will always be a problem

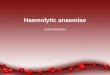
Types of DM incidence Melton LJ et al Diabetes Care 1983, 6, 75-86
0
100
200
300
400
500
600
700
0-9 10-19. 20-29 30-39 40-49 50-59 60-69 70-79 80+
Age (yrs)
Incid
en
ce
(p
er
10
0,0
00
pe
r ye
ar)
T1DM
2ndry
Male T2
Female T2

Types of DM incidence Melton LJ et al Diabetes Care 1983, 6, 75-86
0
5
10
15
20
25
30
35
40
0-9 10-19. 20-29 30-39 40-49 50-59 60-69 70-79 80+
Age (yrs)
Incid
en
ce
(p
er
10
0,0
00
pe
r ye
ar)
T1DM
2ndry

Hypos vs HbA1c; Lipska KJ, 2013
X X

The Talk. • The fasting plasma glucose and HbA1c levels can miss undiagnosed
diabetes in the elderly.
• Having diagnosed diabetes, ascertain the type; it may be useful to clarify
the beta cell function by urinary C-peptide to creatinine ratio.
• The HbA1c and eGFR (MDRD formula) can be misleading in the elderly.
• Hypoglycaemia is common, poorly recognised and associated with
adverse health outcomes.
• One must know the wide choice of drugs and injectable therapy
• Glycaemic targets must be individualised
• Blood pressure targets are now under 140 systolic, ie more relaxed.
• Cholesterol targets remain under 4.0 mmol/L total.
• Dementia is more common in diabetic folk and finding it is useful eg Mini-
Cog

Use of Fasting Plasma Glucose?
Bristol Data, Croxson & Mostafa, PDI, 2008
Aged 60+ 151 (of 265 tested) diabetic subjects, • 21 (14%) - FPG <6.1 mmol/L 110 mg% • 17 (11%) - FPG 6.1 to 6.9 mmol/L
inclusive. • ie 25% FPG < 7.0 mM, 126 mg%
Aged under 60 121 (of 334 tested) diabetic subjects, • 3 (2%) - FPG <6.1 mmol/L, 110 mg% • 8 (7%) - FPG 6.1 to 6.9 mmol/L
inclusive. • ie 9% FPG < 7.0 mM, 126 mg% Diabetic care home residents • 18% Diabetics had raised FPG
FPG >6.9
FPG 6.1-6.9
FPG <6.1


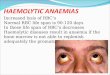
Matyka K, Diabetes Care. 1997 Altered responses against hypoglycemia in aging.
Young Elderly
Autonomic
Symptoms
<3.6 mM
<65 mg%
<3.0 mM
<54 mg%
Accuracy
Reaction
<2.8 mM
<50 mg%
<2.8 mM
<50 mg%
Reaction
Time
<3.0 mM
<54 mg%
<3.0 mM
<54 mg%
Symptoms less pronounced in elderly

Hypoglycaemia & Dementia
• Whitmer RA, JAMA 2009
• Kaiser Permanante subjects of North California
• Examined subjects 1980-2002 – any hypos?
– Hospitalisation, or ED attendance
• Examined 2003 – 2007 – developed dementia?
– Not known dementia at start of observation
– Mean age 65 at start of dementia observation

Just having to attend ED hypo
• 1 hypo - x 1.26 risk
– ED hypo – 1.42 risk
• 2 hypos – x 1.80 risk
– ED hypo – x 2.36 risk
• 3+ hypos – x 1.94 risk
• Mark Strachan, Diabetic Med 2012
• Feinkohl I et al, D Care 2014
• Severe hypo & late‐life cognitive ability in older people
with T2DM: the Edinburgh T2DM Study

So why lower plasma
glucose?

Benefits of glycaemic control
• Avoid microvascular disease
– RCTs with insulin, but middle aged
– Eg UKPDS, Kumamoto
• Avoid macrovscular disease
– UKPDS, Stettler meta analysis, ie middle aged
• Preserve cognition & well being
– RCTs; middle aged with insulin, elderly with OHAs
• Muscle strength with lower HbA1c
– Observational in elderly; FRAILTY
• Avoid infection with lower HbA1c
– Observational, all ages

Sinclair, AJ et al, European Diabetes Working Party for Older People 2011
Diabetes & Metabolism 2011; 37: S27-S38 Cf Brown AF et al. Guidelines for improving care of the older person with DM. JAGS. 2003; 51(5 Suppl):S265-80
• Non-Frail:
• HbA1c 7.0 - 7.5%
– Evidence level 1+, grade of recommendation A
• Fasting glucose 6.5 - 7.5
– Evidence level 2++, grade of recommendation B
• Frail:
• HbA1c 7.6 - 8.5%
– Evidence level 1+, grade of recommendation A
• Fasting glucose 7.6 - 9.0
– Evidence level 2+, grade of recommendation C
•

Trog, Pio, Rosiglitazone
Liver: Bad Good Good
Vessels: ? Good Bad Very similar chemicals have very different results

SU + Vilda / placebo; Garber AJ 2008
• Vilda vs placebo in elderly DW Strain Lancet 2013
• Investigator determined target
HbA1c attained:-
– 27% on placebo
– 53% on Vilda
• 0.6% placebo subtracted ↓ HbA1c
• Worked as well over 75 as under
75 years
– Mean age was 75 years, (70 - 97)
• SE same on vilda & placebo

So when?
• After metformin
• Before Insulin
• Probably before Pio
• If worried about hypo on SU
• Within 1% of HbA1c target,
– And ongoing review of glycaemic achievement

Major CVS events in HOT. Note benefit, even tho’ not to target (<80 DBP)

Cholesterol
• Starting treatment beneficial up to age 82
– HPS up to age 80
– PROSPER subjects aged 70-82 yrs
• Target:-
– Total cholesterol under 4.0 mmol/l, 156 mg%
– LDL cholesterol under 2.0 mmol/l, 78 mg%
• Statin +/- ezetimibe
• But stop when enter nursing home care

Which statin?
• Atorvostatin eg 10 mg
– Generic
– Any time of day
– Any eGFR
– Safer with grapefruit

Insulin:
Easy to
give,
sometimes.

Insulin
• One can find evidence to do whatever one wishes
• Fasting hypoglycaemia major problem with once daily long acting basal insulin
• Using insulin in elderly:-
– What does the patient eat?
– What is one trying to achieve?
– Who will give?
– Who will monitor?
– Bedtime snack / meal
– No fixed ideas

Tablets with insulin • Metformin
– Adjust dose for eGFR, & continue
• Sulphonylurea
– Continue,
– Might switch to amaryl 3-4 mg – less tablets
• Pioglitazone
– Stop – ankle oedema & weight gain with insulin
• Gliptin
– Continue

Tindall H, Diabet Med 1988
• 66 pts failing OHA at home
• Assessed in hospital for 2 weeks.
• Only 22 patients still failing.
• Ensuring compliance with OHA important
• And the older insulin was better than the newer! • Randomised to Humulin-Zn (12 patients) or Neulente insulin (10 patients) for 6 m.
• Sig (p < 0.05) improvement occurred in HbA1c from a median (range) of 13.2(9.8-
16.4)% & 13.1(10.5-16.2)% to 10.6(8-14.2)% & 11.2(8.7-13.5)% in patients given
Humulin-Zn & Neulente, respectively.
• 46 hypos on Humulin-Zn, (36 between 0300 and 0600 h).
• 4 hypos on Neulente
• 6 on Humulin-Zn, 1 on Neulente needed short-acting insulin.

Diagnosis.

Diabetic or not?
• FPG > 7.0 mM
– 75% sensitivity
• HbA1c
– 50% sensitivity, specificity
• Urinalysis
– 50% sensitivity
• So,
– If these tests positive, subject probably has
diabetes,
– If negative, may still have diabetes

Gold Standard
• Wait 10 years & look for retinopathy
• GTT is a surrogate for this
• MOGTT (just the two hour glucose level) is just
as good
• But for whom?
• Post prandial or admission plasma glucose
– 8.0 mM or more
• Croxson S; Chapter 3: Screening. In Sinclair A, (Ed) Diabetes
in Old Age (3rd edition) John Wiley & Sons.

HbA1c, survival, Currie C, Lancet 2010, similar elderly data from K Permanante, Huang 2011
on SU & on Insulin.

Hypos
• Whitmer RA, JAMA 2009
• Mark Strachan, Diabetic Med 2012
• Feinkohl I et al, D Care 2014
• Observational studies
• Hypos increase risk future dementia

Tablets with insulin • Metformin
– Adjust dose for eGFR, & continue • Douek I et al D Med 2005
– Perhaps too cautious with metformin & eGFR
• Richy FF, D Care 2014
– Some elderly get B12 deficient or anorexic on it
• Sulphonylurea
– Continue, ? switch to amaryl 3-4 mg – less tablets
• Pioglitazone
– Stop – ankle oedema & weight gain with insulin
• Gliptin
– Continue

The Talk.
• What are we treating?
• Value of HbA1c and eGFR
• Hypoglycaemia.
• Wide choice of drugs and injectable therapy
• Glycaemic targets must be individualised
• Not enough time to cover all I desire.