Embed Size (px)
Citation preview

Haemolytic Anaemias

Haemolytic Anaemias Any condition where the shortened
lifespan of RBCs within the circulation leads to the development of anaemia
The severity of any anaemia depends directly on the ability of the marrow to compensate for the shortened survival

Haemolytic Anaemias Marrow compensation depends on
several factors, including:- how short the RBC lifespan is age of patient availability of raw materials
Patient may be in a ‘compensated haemolytic state’ or haemolytic anaemia.

Extravascular haemolysis Normal RBC breakdown
Extravascular RE system
Globin breakdown Globin chains amino acids
Haem breakdown Iron transferrin Protoporphyrin

Protoporphyrin Protoporphyrin bilirubin
unconjugated bilirubinconjugated bilirubin
Unconjugated bilirubin circulates in association with plasma proteins
Conjugated bilirubin excreted into gut in bile Converted to stercobilinogen and stercobilin Some reabsorbed and excreted by the kidney in urine
as urobilinogen and urobilin.

Intravascular haemolysis RBCs broken down within the circulation Free haemoglobin released
Plasma haptoglobin may become saturated Remaining free haemoglobin filtered by the
kidney Excess free haemoglobin may enter urine
haemoglobinuria

Haemoglobinuria

Haemolytic Anaemias May be classified by:-
Site of RBC breakdown Intravascular Extravascular
Genetics Congenital Acquired
Nature of defect Intrinsic Extrinsic

Haemolytic Anaemias Intrinsic HA’s are where the HA is due to an
intrinsic defect of the RBCs themselves. They are usually congenital.
Extrinsic HA’s are where the RBCs themselves are essentially normal, but where their environment is too hostile for survival. They are usually acquired.

Intrinsic Causes Membrane defects, including:-
Hereditary Spherocytosis (HS) Hereditary Elliptocytosis (HE)
Contents defects, including:- Metabolic Defects
G6PD Deficiency PK deficiency
Hb abnormalities HbS

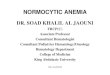
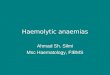
Red cell flexibility
A reticulocyte traversing from the splenic cord to splenic sinus. Note the marked deformation the cell undergoes during its passage through the narrow endothelial slit separating the cord from the sinus. Original magnification ×15 000
British Journal of Haematology Vol. 141, 3 Pages: 367-375

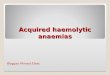
Red cell cytoskeleton

Cytoskeleton Vertical interaction
Band 3 4.2 Ankyrin
Horizontal interaction Spectrin Actin 4.1

Spectrin 2 subunits and co-exist to form a
heterodimer These dimers associate to form tetramers
200nm in length Head units bind head to head fashion Tail units bind to actin via protein 4.1
Actin molecule has a number of binding sites for spectrin

Spectrin / Actin meshwork (Horizontal)
(Winkelmann, JC et al. 1993)
(Swihart et al. 2001)


Intrinsic defects Structural – membrane defects
Abnormality in the membrane-associated cytoskeleton, namely spectrin or other membrane-linking molecules.
Results in membrane instability RBC become more spherical (loss of surface area
relative to volume) Due to inflexibility these cells cannot pass through
spleen, become trapped and phagocytosed by macrophages.
2.1
GPC
Actin
4.1 p554.22.12.1
GPC
ActinActin
4.1 p554.24.2

Abnormal Erythrocytes
Abnormal Shape : Spherocytes / Stomatocytes / Elliptocytes / Echinocyte /Acanthocytes / Pyropoikilocytosis
• Deformabilty reduced, removed from circulation,
• Haemolytic anaemia or non-haemolytic anaemia
• Associated with defects in erythrocyte membrane skeleton

Hereditary Spherocytosis Loss of vertical linkage between cytoskeleton
and membrane. Band 3 and associated molecules essential
for organisation and retention of lipid bilayer. Loss of vertical interaction leads to loss of outer
lipids Decrease SA / Vol ratio Spherocytosis

Hereditary spherocytosis
Membrane defects

Hereditary Elliptocytosis Weakening of lateral linkages between
skeletal proteins.
Spectrin – 4.1 – Actin imparts flexibility Defects in horizontal interaction leads to a loss of
rigidity Elliptocytosis

Clinical signs HS and HE incredibly heterogeneous
disorders Tend to present with anaemia, jaundice and
splenomegaly Treatment
HS patients may benefit from splenectomy Folic acid supplementation

Erythrocyte membrane disorders
HS – loss SA relative to
volume
• Abnormal vertical interactions between lipid bilayer and skeleton e.g HS, band 3, ankyrin, spectrin
• Abnormal Horizontal interactions e.g. HE, spectrin, 4.1R

Extrinsic / Acquired HA Immune
Auto-immune Antibodies produced by patients immune system
against own red cell antigens Allo-immune
Antibodies produced by patients immune system against Foreign red cell antigens Antigens acquired by patients red cells
Non-immune

Extrinsic / Acquired causes Immune
Autoimmune haemolytic anaemias Warm Cold
Alloimune haemolytic anaemias Transfusion of ABO incompatible blood Rhesus disease of the newborn

Cold AIHA Red cells become coated with autoantibody
Usually IgM IgM fixes complement Haemolysis both intravascular and extravascular
Antibody binds optimally at 4 degrees C Peripheral circulation

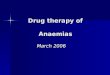
Cold AIHA Chronic haemolytic state aggravated by cold Splenomegaly Jaundice Acrocyanosis in extremities Blood film
Spherocytosis Red cell agglutination (cold)

AIHA (Cold type) Agglutination

Warm AIHA Red cells become coated with autoantibody
IgG RBCs then phagocytosed by macrophages
Phagocytosis may be total or partial Extravascular haemolysis
Red cells become coated with IgG plus complement Complement cascade results in cell lysis
Intravascular haemolysis

Warm AIHA Variable presentation
Gradual onset of anaemia Acute haemolysis
Splenomegaly Jaundice Blood film
Spherocytes Large polychromatic red cells

Alloimmune Haemolytic Anaemias
1) Transfusion of ABO incompatible blood
May be immediate or delayed, intravascular or extravascular
Intravascular ABO
Complement fixing Extravascular
Rhesus Non-complement fixing

2) Haemolytic Disease of the Foetus and Newborn (HDFN) Rh neg mother carrying Rh pos child may
produce antibodies towards this antigen (IgG anti-D) Foetal red cells express paternal / foreign
antigens
IgG causes destruction of foetal red cells in subsequent pregnancies


Prophylactic anti-D Majority of cases of D immunisation can be
prevented by administration of anti-D post partum or post termination / miscarriage
1-2% of D-negative women with D-positive infants will develop anti D prior to delivery
Antenatal administration of anti-D is very effective; and has been endorsed as a policy by the RCOG:
300g of anti-D given at 28 weeks gestation and then standard 300g postpartum dose.
Mechanism of action Rapid removal of fetal red cells before a maternal
immune response can be mounted.

Feto-Maternal traffic of Immunoglobulins Maternal IgG must cross the placenta to reach the
fetus: (Syncytiotrophoblasts and foetal capillary endothelial cells)
Neonatal Fc receptor (FcRn) mediates this process Two-stage transport (1) IgG pinocytosed into acidic endosomes where
IgG-FcRn complex with high avidity (2)IgG-FcRn complexes then shuttled to basolateral
surface of endothelial cells and then released at neutral pH

• FcRN Structure
• Heterodimer, homology with MHC Class I
chain (50 kDa, Blue) + 2--globulin (15 kDa, Green)
• Binds IgG at pH 6.0• Released at pH 7.4• Binds Fc of IgG between
CH2 & CH3 using FcRn domains
• X-ray evidence suggests 2 FcRNs bind 1 IgG

FcRn:IgG
Clark, M (1997), Chemical Immunology 65, 88-110 "IgG Effector Mechanisms

Roitt & Delves, Essential Immunology, 10th edn., p.52.
• In human milk and colostrum IgA provides most protection
FcRN mediated transfer of IgG

Clinical manifestations of Rh D haemolytic disease (1)
Three levels of severity generally described with different clinical manifestations:
(1) Infants at birth with no signs of RBC destruction
may develop mild Jaundice after 1-2 days of life (build up of bilirubin). Treated by phototherapy
(2) In more severely affected infants jaundice may develop more rapidly (icterus gravis neonatorum).
Unless treated rapidly by exchange transfusion may develop Kernicterus where levels of serum bilirubin exceed 20mg/dl. Kernicterus is associated with fetal lethargy, spasticity and irreversible brain damage.

Clinical manifestations of Rh D haemolytic disease
(3) In fetuses with even more severe haemolytic anaemia (Hb levels as low as 4g/dl); Hydrops fetalis can occur.
• ascites (watery fluid gathers in tissues)
• generalised oedema (tissue swelling)
• gross enlargement of fetal liver and spleen
• low serum albumin level (albumin involved in transport of serum fetal bilirubin for destruction)
Foetus requires intrauterine transfusion.

Estimation of Feto-maternal haemorrhage (FMH)(1) Kleihauer-Betke test
Postpartum maternal blood fixed on microscope slide with ethanol
Slides washed, and treated with buffered citric acid, pH3.3. This solution dissolves adult but not fetal haemoglobin.
Slides stained with haematoxylin and erythrosine and examined.
Maternal red cells will appear as “ghosts” whilst fetal cells are heavily stained.
Estimate of foetal leak made (rarely exceeds 30mls).

(2) Flow cytometry
Maternal blood incubated with fluorescently-labelled anti-D (E.g. FITC, fluorescein isothiocyanate); washed and visualised by passing through a flow cytometer.
Standards of known quantities of D-pos/Dneg mixes are used. FMH estimated, and 20g anti-D used per ml of D-pos fetal leak

Drug induced HA’s Antibody directed against a RBC:drug
complex Penicilin, ampicillin (high dose)
Complement attachment to RBC:drug:antibody complex Quinidine, rifampicin
Methyldopa > causes true autoimmune HA via an unclear mechanism
Extravascular haemolysis

Extrinsic Causes Acquired Non-immune HA
Biological agentsInfections Malaria
P.falciparum sp ‘Black water fever’
Bacterial Infections Clostriduim perfringens

Extrinsic Causes Physical agents:-
Heat Burns and Scalds
Compressive forces March haemoglobinuria
Shear stress Mechanical heart valves
“Cheese cutter” effects DIC MAHA

Cell fragments (MAHA)

Paroxysmal nocturnal haemoglobinuria (PNH) Acquired Intrinsic Clonal disorder (mutation) Deficient synthesis of structural protein
Glycosylphosphatidylinositol anchor Attachment of surface proteins
Cells more susceptible to complement attachment and lysis.
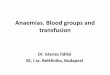
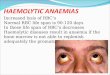
Characterised by haemoglobinuria

Haemoglobinuria PNH
Urine samples during a 12 hour period in a patient with PNH. Note the darker early morning sample.